
Abstract
Background
Renal cell carcinoma (RCC) is known for its ability to metastasize synchronously or metachronously to various anatomic sites. Distinguishing histologic subtypes of metastatic RCC has become increasingly important, as prognosis and therapy can differ dramatically between subtypes. We propose a combination of immunohistochemistry (IHC) and molecular cytogenetics for subtyping metastatic RCC in light of these potential therapeutic implications.
Results
Specimens from 103 cases of metastatic RCC were retrieved, including 32 cases originally diagnosed as metastatic clear cell renal cell carcinoma (CCRCC), 8 as metastatic papillary renal cell carcinoma (PRCC), and 63 metastatic RCC without a specific subtype. Immunohistochemistry was performed with antibodies against cytokeratin 7 (CK7) and alpha-methylacyl-CoA racemase (AMACR). Dual color interphase fluorescence in situ hybridization was utilized to assess for deletion of chromosome 3p and trisomy of chromosomes 7 and 17 in all tumors. Chromosome 3p deletion was detected in 41% of all metastatic RCC specimens, and trisomy of chromosomes 7 and/or 17 was detected in 16%. Of metastatic CCRCC, chromosome 3p deletion was detected in 63%. Of metastatic PRCC, 75% showed trisomy of chromosomes 7 and/or 17. Of the tumors not previously classified, 6% were positive for CK7, and 64% were positive for AMACR; 35% showed chromosome 3p deletion, and 16% showed trisomy of chromosomes 7 and/or 17. Combined analysis of immunohistochemistry and cytogenetics enabled reclassification of 52% of these metastatic tumors not previously classified.
Conclusion
Our findings support the utility of immunohistochemistry and cytogenetics for subtyping metastatic RCC.
Similar content being viewed by others


Introduction
Renal cell carcinoma (RCC) comprises a heterogeneous group of epithelial neoplasms with diverse biologic behaviors and variable clinical outcomes. RCC is the most lethal of the urologic malignancies. Between 20% and 30% of patients with RCC have metastatic disease at the time of diagnosis, and another 30% subsequently develop metastasis after resection[1–3]. The majority of tumors are of the clear cell (CCRCC) subtype (70%-75%), characteristically harboring abnormalities of the von Hippel-Lindau (VHL) gene, located at chromosome 3p25[3–9]. Defects in VHL expression result in constitutive activation of the hypoxia-inducible factor (HIF) pathway and overexpression of vascular endothelial growth factor (VEGF), platelet-derived growth factor (PDGF), and other products. Inactivation of the VHL gene also enhances tumor cell growth though the mammalian target of rapamycin (mTOR) pathway[8, 10–12]. In contrast, papillary renal cell carcinoma (PRCC) is the most common non-clear cell subtype of RCC, accounting for 10%-15% of tumors. PRCC is associated with activation of the MET pathway in a subset of tumors, resulting in a cascade of intracellular signaling leading to tumor cell growth, angiogenesis, migration and invasion[6, 13, 14].
Knowledge of these gene pathways has enabled novel approaches to the management of metastatic RCC[15–17]. Currently, clinical trials with targeted therapeutic strategies for both metastatic CCRCC and PRCC have been intensively planned and carried out[6, 13, 18–26]. Although recent advances have improved patient outcomes[20, 27–29], these targeted agents are not without toxic effects[30, 31]. Optimizing the clinical outcome and knowing when to persist with these therapies highlight the need for accurate RCC subtyping.
Histopathologic examination of a completely resected primary tumor is often sufficient for tumor subtyping, as a component with prototypical morphologic features can usually be readily appreciated. However, in the metastatic setting, it is often challenging to discriminate between subtypes of RCC based on morphology alone, particularly since metastatic foci are often sampled only by core needle biopsy and are often preferentially composed of high-grade tumor. Immunohistochemical analysis is valuable to identify the histogenetic origin of metastatic malignancy[32]. Nevertheless, its use for discriminating different histologic subtypes is limited and rarely applied in prospective treatment outcome studies. A cytogenetic hallmark of CCRCC is loss of chromosome 3p, which distinguishes it from other RCC subtypes[7, 8, 33]. PRCC frequently exhibits chromosomal polysomies, of which trisomy of chromosomes 7 and/or 17 are the most consistent and characteristic[7, 8, 34]. Because CCRCC and PRCC show different immunophenotypes and different characteristic cytogenetic abnormalities, we sought to combine these two ancillary tests in an effort to reduce ambiguity in subtyping of metastatic RCC. Immunophenotypes of 103 cases of metastatic RCC were analyzed in conjunction with cytogenetic characteristics as determined by fluorescence in situ hybridization (FISH), in order to improve classification of these neoplasms.
Patients and methods
Patients
One hundred three cases of metastatic RCC diagnosed between 2007 and 2013 were retrieved from the archives of the Department of Pathology of the Indiana University School of Medicine. The histologic type was established, when possible, according to the 2004 WHO classification[3]. The hematoxylin and eosin slides of these cases were reviewed, and appropriate tumor blocks from metastatic sites were selected for immunohistochemical and cytogenetic studies. This research was approved by the Indiana University Institutional Review Board.
Immunohistochemical staining
Immunohistochemistry was performed with the following antibodies: cytokeratin 7 (CK7; monoclonal mouse anti-human CK7 antibody, OV-TL 12/30, prediluted; Dako Corp.) and alpha-methylacyl-CoA-racemase (AMACR/P504S, polyclonal rabbit anti-human antibody, 13H4 clone, prediluted; Dako Corp.). Diaminobenzidine (3, 3-diaminobenzidine) was used as the chromogen. Immunostaining was performed on the DAKO Autostainer Plus. Positive and negative controls were stained concurrently and showed appropriate immunostaining. The extent of immunohistochemical staining was evaluated microscopically. Labeling for CK7 and AMACR was considered positive when moderate to strong staining was present in greater than 20% of tumor cells.
Fluorescence in situ hybridization
Fluorescence in situ hybridization (FISH) analysis was performed as described previously[5, 7, 34–37]. Briefly, multiple 4 μm sections were obtained from formalin-fixed paraffin-embedded tissue blocks containing neoplastic tissue. A hematoxylin and eosin-stained slide from each block was examined to identify areas of neoplastic tissue for FISH analysis. The slides were deparaffinized with 2 washes of xylene, 15 minutes each, and subsequently washed twice with absolute ethanol, 10 minutes each, and then air-dried in a fume hood. Next, the slides were treated with 0.1 mM citric acid (pH 6.0) (Zymed, South San Francisco, CA) at 95°C for 10 minutes, rinsed in distilled water for 3 minutes, followed by a wash of 2x standard saline citrate for 5 minutes. Digestion was performed by applying 0.4 mL of pepsin (5 mg/mL in 0.1 N HCl/0.9 NaCl) (Sigma, St Louis, MO) at 37°C for 40 minutes. The slides were rinsed with distilled water for 3 minutes, washed with 2x standard saline citrate for 5 minutes and air-dried. The chromosomal probe directed against 3p25 (RP11-572 M14) was obtained from Empire Genomics (Empire Genomics, Buffalo, New York). Chromosome enumeration probes (CEP) for chromosomes 3, 7, and 17 were obtained from Vysis (Abbott, Downers Grove, IL).
Deletion of chromosome 3p was assessed using a probe cocktail containing BAC clone probe to chromosome 3p25 (RP11-572 M14, Green) and CEP3 (Orange). Chromosome 7 and 17 alterations were assessed using a probe cocktail containing probe CEP7 (Green) and CEP17 (Orange). The 3p25/CEP3 probe set and the CEP7/CEP17 probe set were diluted with tDenHyb2 (Insitus, Albuquerque, NM) in ratios of 1:50 and 1:100, respectively.
Analysis was performed in a manner similar to that previously described[5, 7, 34–37]. In brief, for each slide 100 to 150 nuclei from tumor tissue were scored for probe signals under the fluorescence microscope with x1000 magnification. The method of analysis for 3p25 deletion was based on previous studies of chromosome deletions at 1p and 19q in oligodendrogliomas[38, 39]. The cutoff value for 3p deletion was defined as a 3p25/CEP3 ratio of ≤0.7. Definitions of chromosomal trisomy for chromosomes 7 and 17 were based on the Gaussian model and were related to the nonneoplastic renal cortex control cell signals. The cutoff values were set for each probe at the mean plus 3 standard deviations of the control values. Chromosome 3p deletion was considered to be characteristic of CCRCC, whereas trisomy of chromosomes 7 and/or 17 was considered characteristic of PRCC[7].
Results
Clinicopathologic characteristics
A total of 103 metastatic RCC specimens were included in the study. Of these, 32 tumors were originally classified as metastatic CCRCC, and 8 were originally classified as metastatic PRCC, based on a constellation of typical morphologic features and known histologic classification of the primary tumor. In the remaining 63 cases of metastatic RCC, the tumor histologic subtype was unknown or uncertain, based on lack of availability of tissue material from the primary tumor for comparison (including primary tumors that were not resected or those diagnosed an another institution) and equivocal morphologic features in the metastatic lesion. Seventy-five patients were male and 28 were female. The patients’ ages ranged from 28 to 87 years (median 63 years). The metastatic sites included: bone (n = 27), lung (n = 19), abdominal sites (n = 17), liver (n = 7), pleura (n = 7), soft tissue (n = 7), pancreas (n = 3), gastrointestinal tract (n = 3), mediastinum (n = 3), gallbladder (n = 2), thyroid (n = 2), and other organs or tissues (n = 6).
Immunohistochemistry
Overall, 7% (7/103) of all metastatic RCC showed positive immunohistochemical staining for CK7, and 57% (59/103) showed immunoreactivity for AMACR (Table 1, Figures 1 and2). Of the tumors originally classified as metastatic CCRCC, none were positive for CK7 and 34% (11/32) were positive for AMACR. Of the tumors originally classified as metastatic PRCC, 38% (3/8) were positive for CK7, and 100% (8/8) were positive for AMACR. Of the RCCs with an uncertain or unknown histologic subtype, 6% (4/63) were positive for CK7, and 64% (40/63) were positive for AMACR (Table 1). Of the CK7-positive tumors, 86% (6/7) also demonstrated trisomy of chromosomes 7 and/or 17 by FISH.

Metastatic clear cell renal cell carcinoma. A metastatic tumor nodule in the lung (A) was composed of solid, nested, and tubular arrangements of cells with clear cytoplasm (B). The tumor cells showed negative immunoreactivity for CK7 (C) but strong reactivity for AMACR (D). Dual-color fluorescence in situ hybridization demonstrated chromosome 3p deletion, as indicated by the presence of a single 3p25 signal (green) with two chromosome 3 centromere signals (red) per cell (E). Tumor nuclei showed two green signals for chromosome 7 and two red signals for chromosome 17 (F), disomic patterns.

Metastatic papillary renal cell carcinoma. A metastatic tumor nodule in the liver exhibited characteristic papillary architecture (A), composed of fibrovascular cores lined by cells with eosinophilic cytoplasm (B). The tumor cells labeled strongly with antibodies to CK7 (C) and AMACR (D). Dual-color fluorescence in situ hybridization revealed intact chromosome 3p, as indicated by two green signals (3p25) and two chromosome 3 centromeric red signals (CEP3) (E). Dual-color fluorescence in situ hybridization demonstrated trisomy of chromosomes 7 and 17, as evident by three green signals (CEP7) and three red signals (CEP17) in each tumor cell nucleus (F), supporting the classification of papillary renal cell carcinoma.
Cytogenetics
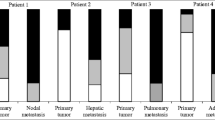
Chromosome 3p deletion was detected in 41% (42/103) of all metastatic RCC cases, and trisomy of chromosomes 7 and/or 17 was detected in 16% (16/103), of which 14 exhibited trisomy of chromosome 7 and 12 exhibited trisomy of chromosome 17 (Table 1). Of the tumors originally classified as metastatic CCRCC, chromosome 3p deletion was detected in 63% (20/32). Of the tumors originally classified as metastatic PRCC, 75% (6/8) showed trisomy of chromosome 7 and/or 17. Deletions of chromosome 3p and trisomy of chromosomes 7 and/or 17 were mutually exclusive findings in these metastatic CCRCC and PRCC cases. Of the RCCs not previously classified, 35% (22/63) were found to have chromosome 3p deletion, and 16% (10/63) were found to have trisomy of chromosome 7 and/or 17 (Table 1). Therefore 51% (32/63) of the metastatic RCCs that were previously not classified could be subtyped based on cytogenetic alterations: The tumors with chromosome 3p deletion (35%, 22/63) were reclassified as metastatic CCRCC, and the tumors with trisomy 7 and/or 17 (16%, 10/63) were reclassified as metastatic PRCC (Table 1, Figure 3).

Metastatic renal cell carcinomas not previously classified. A metastatic tumor nodule involving a lymph node (A) exhibited a nested to sheet-like architecture (B). Although morphologic features supported a diagnosis of metastatic renal cell carcinoma, the precise tumor subtype was not initially apparent. The tumor cells did not label for CK7 (C), but demonstrated moderately strong granular cytoplasmic reactivity for AMACR (D). Dual-color fluorescence in situ hybridization revealed intact chromosome 3p (E) as indicated by two green signals (3p25) and two red chromosome 3 centromeric signals (CEP3). FISH demonstrated trisomy of chromosomes 7 and 17, as indicated by three green signals (CEP7) and three red signals (CEP17) per nucleus (F), supporting reclassification of this tumor as papillary renal cell carcinoma. Another metastatic renal cell carcinoma involving the lung showed architectural and cytologic features not initially recognizable as those of a particular renal cell carcinoma subtype (G). The tumor exhibited a mixture of solid, trabecular, and tubulopapillary growth, lined by cells with eosinophilic cytoplasm (H). Dual-color fluorescence in situ hybridization demonstrated a characteristic 3p25 deletion as indicated by one green signal (3p25) and two chromosome 3 centromere red signals (CEP3) per cell (I), supporting subtyping as high-grade manifestation of clear cell renal cell carcinoma. A third metastatic lesion involving bone (J) contained cells with clear cytoplasm and prominent nucleoli, dispersed in a hemorrhagic and fibrinous (K) background. These morphologic findings raised the possibility of metastatic clear cell renal cell carcinoma. However, FISH revealed trisomy of chromosomes 7 and 17 (L), as demonstrated by three green signals (CEP7) and three red signals (CEP17) per nucleus. These findings were in line with the patient’s history of papillary renal cell carcinoma resected via radical nephrectomy many years prior, despite the morphologic appearance raising the possibility of clear cell renal cell carcinoma.
Of the 22 tumors reclassified based on FISH results as metastatic CCRCC, none were positive for CK7, and 46% (10/22) were positive for AMACR. Of the 10 cases reclassified as metastatic PRCC, 30% (3/10) were positive for CK7, and 100% (10/10) were positive for AMACR. One tumor was positive for CK7 but lacked any cytogenetic abnormality detected by these methods. If this tumor is regarded as PRCC based on positivity for CK7, then 52% (33/63) of the metastatic RCCs that were not previously subtyped could be reclassified based on a combination of FISH and immunohistochemistry.
Discussion
RCC is known for its ability to metastasize either synchronously or metachronously to a variety of anatomic sites. In current practice, distinguishing histologic subtypes of metastatic RCC has become increasingly important, as different subtypes portend divergent prognoses and are managed with disparate treatment algorithms. Histologic features enable accurate classification of most primary tumors. However, overlapping morphologic findings between some categories of renal neoplasms can make subclassification difficult, particularly in the metastatic setting, in which biopsy material may be limited and high-grade morphology may obscure prototypical histopathologic architectural and cytologic features. Additionally, recent molecular insights into the clonal evolution of metastatic RCC have revealed substantial heterogeneity in genetic alterations in different regions of metastatic deposits and within different regions of the primary tumor[40]. In the era of targeted therapies, different histologic subtypes of metastatic RCC have relevance in selecting patients for enrollment in clinical trials and in evaluation for salvage therapy[1, 8, 41]. Currently, pivotal studies using targeted drugs have largely focused on patients with clear cell RCC. Patients with tumors of other non-clear cell histologic subtypes have been less extensively studied[27]. In the present study, we evaluated the immunophenotypes of 103 metastatic RCCs, and correlated with the tumors’ cytogenetic characteristics using FISH. Combined analysis of immunohistochemistry and cytogenetics enabled reclassification of 52% (33/63) of metastatic RCCs for which the histologic subtype was originally unknown or uncertain. Our study establishes the utility of immunohistochemistry and cytogenetics for subtyping metastatic RCC, which may be of particular help toward selecting appropriate targeted therapies.
RCC is not a single disease; it is composed of a number of subtypes, each with unique histologic features, genetic alterations, clinical behavior, and response to therapy[1, 7, 8, 42]. Nonetheless, histologic subtyping of RCC can be particularly problematic in the metastatic setting for a number of reasons: For one, tissue diagnosis of metastatic RCC is sometimes established prior to or in the absence of sampling the primary tumor. Conversely, identification of metastatic RCC sometimes follows resection of the primary tumor by a long intervening period. Further, metastatic RCC may preferentially exhibit high-grade morphology, lacking the characteristic cytologic and architectural features that are often admixed with higher-grade components in the primary tumor. Therefore, some metastatic RCCs present as a tumor of unknown origin, with a prior history of RCC unknown to treating oncologists or pathologists. In the metastatic context, core needle biopsies and fine needle aspiration specimens from metastatic RCC may be particularly challenging due to limited material for evaluation[43].
Advances in biologic and genetic understanding of RCC have led to specifically targeted treatments for metastatic RCC. For example, inhibition of targets in the HIF pathway has resulted in significant clinical responses in CCRCC[44, 45]. Loss of activity of the Krebs cycle enzyme fumarase hydratase (FH) in some cases of papillary type II RCC may also result in HIF upregulation[46], potentially providing an avenue for utilization of similar treatments in patients with PRCC. Activation of the c-MET oncogene is characteristic of papillary RCC type I, particularly in the hereditary PRCC syndrome and a subset of sporadic PRCC[8]. This finding offers a clear opportunity to test newly developed inhibitors of this tyrosine kinase in this subset of RCC[44, 47]. Although these effective biologic agents may be used in a more individualized approach to metastatic RCC therapy, their novelty infers a paucity of clinical data about their toxic effects or management of their therapy-limiting complications in the setting of metastatic RCC[30]. Therefore, histological subtyping of metastatic RCC significantly impact clinical decision making and therapeutic outcomes in these patients.
CK7 and AMACR have been proposed as markers to help distinguish PRCC from other RCC types, especially CCRCC[34, 36, 48–51]. Immunostaining for CK7 in CCRCC is usually negative or only focally positive, contrasting with more diffuse labeling for this protein in many PRCCs[50–53], particularly type I PRCC. Diffuse, strong AMACR expression is typical of PRCC (70-100%); however, reactivity has also been observed to a variable extent in 4-68% of CCRCC[49, 50, 54–58], sometimes less diffusely or associated with higher-grade tumor components. When evaluating these two markers for RCC, focus has been predominantly directed at primary tumors. We performed immunohistochemical staining for CK7 and AMACR in this series of 103 nonprimary cases to confirm their expression in metastatic RCC. None of the metastatic CCRCC met the study threshold for positive CK7 staining. Only 38% (3/8) of the metastatic PRCC and 6% (4/63) of the RCCs that were previously not classified were positive for CK7, suggesting that expression of this marker may be attenuated in metastatic RCC. CK7 was relatively specific for metastatic PRCC, although not as sensitive as AMACR, perhaps due to its expression in predominantly type I rather than type II tumors[59]. AMACR was detected in 23 of 28 metastatic CCRCC (82%) in one study[60], and 6 of 6 metastatic PRCC (100%) in another study[61]. In our study, AMACR was expressed by 57% (59/103) of all metastatic RCC, including 11 cases of metastatic CCRCC (34%, 11/32), all metastatic PRCCs (100%, 8/8), and 40 cases of RCC not previously classified (63%, 40/63). AMACR was relatively sensitive for metastatic PRCC, but its specificity was not high. Therefore, the value of CK7 and AMACR immunostaining alone is limited for accurately subtyping metastatic RCC.
Other immunohistochemical antibodies with emerging utility in the subclassification of RCC include those directed against carbonic anhydrase IX[62–64]. Since this enzyme is a downstream target of the VHL-HIF pathway[64–66], it is reported to exhibit diffuse, strong membranous reactivity by immunohistochemistry in CCRCC, in contrast to other subtypes of renal tumors, which typically exhibit focal or multifocal reactivity[63], sometimes juxtaposed to areas of ischemia or necrosis. However, other investigators have found intratumoral heterogeneity using this marker, particularly in high-grade or sarcomatoid tumors, such as those that might be encountered at a metastatic site[67]. Since tissue sampling of a metastatic tumor is also likely to be limited, the significance of positive reactivity for carbonic anhydrase IX may be uncertain compared to large samples from a completely resected tumor, in which extent of reactivity can be more readily assessed.
Interphase cytogenetic analysis has emerged as a powerful tool for diagnosis and classification of RCC[34, 68–72]. The cytogenetic hallmark of CCRCC is loss of chromosome 3p, the chromosomal site of the VHL gene and other important loci involved in CCRCC tumorigenesis[8, 33]. FISH analysis shows the characteristic chromosome 3p deletion in 60-90% of CCRCC cases[33, 73]. In contrast, PRCC frequently exhibits chromosomal polysomies, of which trisomy of chromosomes 7 and/or 17 are the most consistent and characteristic[34]. The current study provides cytogenetic data for metastatic RCC involving a variety of anatomic sites. Chromosome 3p deletion was detected in 41% (42/103) of all metastatic RCC cases, and in 63% (20/32) of tumors originally diagnosed as metastatic CCRCC. Of tumors originally diagnosed as metastatic PRCC, 75% (6/8) showed trisomy of chromosomes 7 or 17. Of the metastatic RCCs that were not originally classified, 35% (22/63) additionally exhibited chromosome 3p deletion, facilitating reclassification as metastatic CCRCC. An additional 16% of these tumors (10/63) were found to have trisomy of chromosomes 7 and/or 17, supporting reclassification as metastatic PRCC. In this study, we found chromosome 3p deletion and trisomy 7 or 17 to be mutually exclusive in metastatic RCCs; however, other investigators have occasionally found chromosome 3p deletion to coexist with trisomy 7 or 17 in PRCC, such as in some type II PRCC, and some CCRCC[8, 69, 72, 74]. Therefore, when both of these alterations are present in the same tumor, the findings should be interpreted with caution in supporting the diagnosis of a particular RCC subtype. One additional tumor was found to have no cytogenetic abnormality by FISH but positive expression of CK7 by immunohistochemistry. If this tumor is also considered to be PRCC based on this immunoreactivity pattern, 52% (33/63) of the metastatic RCCs that were previously not classified could be subtyped based on the combination of immunohistochemistry and FISH. A limitation of this study is that we assessed primarily only the two most common RCC subtypes, CCRCC and PRCC. However, a number of other RCC subtypes are now increasingly recognized[75], such as those associated with translocations involving MITF family genes[1, 7, 8, 76–79]. Such neoplasms often exhibit overlapping morphologic features of CCRCC and PRCC, yet they are characterized by unique clinicopathologic, immunohistochemical and genetic alterations. In contrast to the 3p deletions and trisomy of chromosomes 7 and 17 in CCRCC and PRCC, respectively, FISH analysis has assumed a key role in confirming rearrangements involving the TFE3 gene in such tumors[1, 78, 79] and to a lesser extent, the TFEB gene[80].
In summary, subtyping of metastatic RCC has become increasingly important with the emergence of novel therapies for specific tumor subtypes. Our data support the utility of a combined approach of immunohistochemistry and cytogenetics for subtyping metastatic RCC. Our findings may have important diagnostic and clinical implications in the era of personalized medicine, with the advent of target-specific therapeutics.
References
MacLennan GT, Cheng L: Neoplasms of the kidney. Urologic Surgical Pathology. Edited by: Bostwick DG, Cheng L. 2014, 74-156. Philadelphia: Mosby/Elsevier, 3
Siegel R, Naishadham D, Jemal A: Cancer statistics, 2013. CA Cancer J Clin. 2013, 63: 11-30. 10.3322/caac.21166
Eble JN, Sauter G, Epstein JI, Sesterhenn IAE: World Health Organization: Pathology and Genetics of Tumours of the Urinary System and Male Genital Organs. 2004, Lyon: IARC Press
Kaelin WG: Kidney cancer: now available in a new flavor. Cancer Cell. 2008, 14: 423-424. 10.1016/j.ccr.2008.11.005
Cheng L, MacLennan GT, Zhang S, Wang M, Zhou M, Tan PH, Foster S, Lopez-Beltran A, Montironi R: Evidence for polyclonal origin of multifocal clear cell renal cell carcinoma. Clin Cancer Res. 2008, 14: 8087-8093. 10.1158/1078-0432.CCR-08-1494
Choueiri TK, Vaishampayan U, Rosenberg JE, Logan TF, Harzstark AL, Bukowski RM, Rini BI, Srinivas S, Stein MN, Adams LM, Ottesen LH, Laubscher KH, Sherman L, McDermott DF, Haas NB, Flaherty KT, Ross R, Eisenberg P, Meltzer PS, Merino MJ, Bottaro DP, Linehan WM, Srinivasan R: Phase II and biomarker study of the dual MET/VEGFR2 inhibitor foretinib in patients with papillary renal cell carcinoma. J Clin Oncol. 2013, 31: 181-186. 10.1200/JCO.2012.43.3383
Cheng L, Zhang S, MacLennan GT, Lopez-Beltran A, Montironi R: Molecular and cytogenetic insights into the pathogenesis, classification, differential diagnosis, and prognosis of renal epithelial neoplasms. Hum Pathol. 2009, 40: 10-29. 10.1016/j.humpath.2008.09.009
Cheng L, Williamson SR, Zhang S, Maclennan GT, Montironi R, Lopez-Beltran A: Understanding the molecular genetics of renal cell neoplasia: implications for diagnosis, prognosis and therapy. Expert Rev Anticancer Ther. 2010, 10: 843-864. 10.1586/era.10.72
Oosterwijk E, Rathmell WK, Junker K, Brannon AR, Pouliot F, Finley DS, Mulders PF, Kirkali Z, Uemura H, Belldegrun A: Basic research in kidney cancer. Eur Urol. 2011, 60: 622-633. 10.1016/j.eururo.2011.06.048
Linehan WM, Bratslavsky G, Pinto PA, Schmidt LS, Neckers L, Bottaro DP, Srinivasan R: Molecular diagnosis and therapy of kidney cancer. Annu Rev Med. 2010, 61: 329-343. 10.1146/annurev.med.042808.171650
Linehan WM: The genetic basis of kidney cancer: implications for management and use of targeted therapeutic approaches. Eur Urol. 2012, 61: 896-898. 10.1016/j.eururo.2012.02.022
Lopez-Beltran A, Kirkali Z, Cheng L, Egevad L, Regueiro JC, Blanca A, Montironi R: Targeted therapies and biological modifiers in urologic tumors: pathobiology and clinical implications. Semin Diagn Pathol. 2008, 25: 232-244. 10.1053/j.semdp.2008.07.006
Tannir NM, Plimack E, Ng C, Tamboli P, Bekele NB, Xiao L, Smith L, Lim Z, Pagliaro L, Araujo J, Aparicio A, Matin S, Wood CG, Jonasch E: A phase 2 trial of sunitinib in patients with advanced non-clear cell renal cell carcinoma. Eur Urol. 2012, 62: 1013-1019. 10.1016/j.eururo.2012.06.043
Eder JP: Vande Woude GF, Boerner SA, LoRusso PM: Novel therapeutic inhibitors of the c-Met signaling pathway in cancer. Clin Cancer Res. 2009, 15: 2207-2214. 10.1158/1078-0432.CCR-08-1306
de Reijke TM, Bellmunt J, van Poppel H, Marreaud S, Aapro M: EORTC-GU group expert opinion on metastatic renal cell cancer. Eur J Cancer. 2009, 45: 765-773. 10.1016/j.ejca.2008.12.010
Escudier B, Eisen T, Porta C, Patard JJ, Khoo V, Algaba F, Mulders P, Kataja V: Renal cell carcinoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2012, 23 (Suppl 7): vii65-71.
Rini BI: New strategies in kidney cancer: therapeutic advances through understanding the molecular basis of response and resistance. Clin Cancer Res. 2010, 16: 1348-1354. 10.1158/1078-0432.CCR-09-2273
Lee JL, Ahn JH, Lim HY, Park SH, Lee SH, Kim TM, Lee DH, Cho YM, Song C, Hong JH, Kim CS, Ahn H: Multicenter phase II study of sunitinib in patients with non-clear cell renal cell carcinoma. Ann Oncol. 2012, 23: 2108-2114. 10.1093/annonc/mdr586
Eder JP, Shapiro GI, Appleman LJ, Zhu AX, Miles D, Keer H, Cancilla B, Chu F, Hitchcock-Bryan S, Sherman L, McCallum S, Heath EI, Boerner SA, LoRusso PM: A phase I study of foretinib, a multi-targeted inhibitor of c-Met and vascular endothelial growth factor receptor 2. Clin Cancer Res. 2010, 16: 3507-3516. 10.1158/1078-0432.CCR-10-0574
Motzer RJ, Nosov D, Eisen T, Bondarenko I, Lesovoy V, Lipatov O, Tomczak P, Lyulko O, Alyasova A, Harza M, Kogan M, Alekseev BY, Sternberg CN, Szczylik C, Cella D, Ivanescu C, Krivoshik A, Strahs A, Esteves B, Berkenblit A, Hutson TE: Tivozanib versus sorafenib as initial targeted therapy for patients with metastatic renal cell carcinoma: results from a phase III trial. J Clin Oncol. 2013, 31: 3791-3799. 10.1200/JCO.2012.47.4940
Bellmunt J, Trigo JM, Calvo E, Carles J, Perez-Gracia JL, Rubio J, Virizuela JA, Lopez R, Lazaro M, Albanell J: Activity of a multitargeted chemo-switch regimen (sorafenib, gemcitabine, and metronomic capecitabine) in metastatic renal-cell carcinoma: a phase 2 study (SOGUG-02-06). Lancet Oncol. 2010, 11: 350-357. 10.1016/S1470-2045(09)70383-3
Coppin C, Kollmannsberger C, Le L, Porzsolt F, Wilt TJ: Targeted therapy for advanced renal cell cancer (RCC): a Cochrane systematic review of published randomised trials. BJU Int. 2011, 108: 1556-1563. 10.1111/j.1464-410X.2011.10629.x
Eisen T, Joensuu H, Nathan PD, Harper PG, Wojtukiewicz MZ, Nicholson S, Bahl A, Tomczak P, Pyrhonen S, Fife K, Bono P, Boxall J, Wagner A, Jeffers M, Lin T, Quinn DI: Regorafenib for patients with previously untreated metastatic or unresectable renal-cell carcinoma: a single-group phase 2 trial. Lancet Oncol. 2012, 13: 1055-1062. 10.1016/S1470-2045(12)70364-9
Heng DY, Xie W, Regan MM, Harshman LC, Bjarnason GA, Vaishampayan UN, Mackenzie M, Wood L, Donskov F, Tan MH, Rha SY, Agarwal N, Kollmannsberger C, Rini BI, Choueiri TK: External validation and comparison with other models of the International Metastatic Renal-Cell Carcinoma Database Consortium prognostic model: a population-based study. Lancet Oncol. 2013, 14: 141-148. 10.1016/S1470-2045(12)70559-4
Motzer RJ, Hutson TE, Cella D, Reeves J, Hawkins R, Guo J, Nathan P, Staehler M, de Souza P, Merchan JR, Boleti E, Fife K, Jin J, Jones R, Uemura H, De Giorgi U, Harmenberg U, Wang J, Sternberg CN, Deen K, McCann L, Hackshaw MD, Crescenzo R, Pandite LN, Choueiri TK: Pazopanib versus sunitinib in metastatic renal-cell carcinoma. N Engl J Med. 2013, 369: 722-731. 10.1056/NEJMoa1303989
Rini BI, Halabi S, Rosenberg JE, Stadler WM, Vaena DA, Archer L, Atkins JN, Picus J, Czaykowski P, Dutcher J, Small EJ: Phase III trial of bevacizumab plus interferon alfa versus interferon alfa monotherapy in patients with metastatic renal cell carcinoma: final results of CALGB 90206. J Clin Oncol. 2010, 28: 2137-2143. 10.1200/JCO.2009.26.5561
Choueiri TK, Plantade A, Elson P, Negrier S, Ravaud A, Oudard S, Zhou M, Rini BI, Bukowski RM, Escudier B: Efficacy of sunitinib and sorafenib in metastatic papillary and chromophobe renal cell carcinoma. J Clin Oncol. 2008, 26: 127-131. 10.1200/JCO.2007.13.3223
Abel EJ, Culp SH, Tannir NM, Matin SF, Tamboli P, Jonasch E, Wood CG: Primary tumor response to targeted agents in patients with metastatic renal cell carcinoma. Eur Urol. 2011, 59: 10-15. 10.1016/j.eururo.2010.09.034
Vogelzang NJ: Another step toward the cure of metastatic renal cell carcinoma?. J Clin Oncol. 2010, 28: 5017-5019. 10.1200/JCO.2010.31.5044
Di Lorenzo G, Porta C, Bellmunt J, Sternberg C, Kirkali Z, Staehler M, Joniau S, Montorsi F, Buonerba C: Toxicities of targeted therapy and their management in kidney cancer. Eur Urol. 2011, 59: 526-540. 10.1016/j.eururo.2011.01.002
Karam JA, Wood CG: The dark side of targeted therapy. Eur Urol. 2011, 59: 541-542. 10.1016/j.eururo.2011.01.041
Horlings HM, van Laar RK, Kerst JM, Helgason HH, Wesseling J, van der Hoeven JJ, Warmoes MO, Floore A, Witteveen A, Lahti-Domenici J, Glas AM, Van't Veer LJ, de Jong D: Gene expression profiling to identify the histogenetic origin of metastatic adenocarcinomas of unknown primary. J Clin Oncol. 2008, 26: 4435-4441. 10.1200/JCO.2007.14.6969
Klatte T, Rao PN, de Martino M, LaRochelle J, Shuch B, Zomorodian N, Said J, Kabbinavar FF, Belldegrun AS, Pantuck AJ: Cytogenetic profile predicts prognosis of patients with clear cell renal cell carcinoma. J Clin Oncol. 2009, 27: 746-753. 10.1200/JCO.2007.15.8345
Gobbo S, Eble JN, MacLennan GT, Grignon DJ, Shah RB, Zhang S, Martignoni G, Brunelli M, Cheng L: Renal cell carcinomas with papillary architecture and clear cell components: the utility of immunohistochemical and cytogenetical analyses in differential diagnosis. Am J Surg Pathol. 2008, 32: 1780-1786. 10.1097/PAS.0b013e31818649ed
Jones TD, Eble JN, Wang M, MacLennan GT, Delahunt B, Brunelli M, Martignoni G, Lopez-Beltran A, Bonsib SM, Ulbright TM, Zhang S, Nigro K, Cheng L: Molecular genetic evidence for the independent origin of multifocal papillary tumors in patients with papillary renal cell carcinomas. Clin Cancer Res. 2005, 11: 7226-7233. 10.1158/1078-0432.CCR-04-2597
Williamson SR, Zhang S, Eble JN, Grignon DJ, Martignoni G, Brunelli M, Wang M, Gobbo S, Baldridge LA, Cheng L: Clear cell papillary renal cell carcinoma-like tumors in patients with von Hippel-Lindau disease are unrelated to sproadic clear cell papillary renal cell carcinoma. Am J Surg Path. 2013, 37: 1131-1139. 10.1097/PAS.0b013e318282dab8
Halat S, Eble JN, Grignon DJ, Lopez-Beltran A, Montironi R, Tan PH, Wang M, Zhang S, MacLennan GT, Cheng L: Multilocular cystic renal cell carcinoma is a subtype of clear cell renal cell carcinoma. Mod Pathol. 2010, 23: 931-936. 10.1038/modpathol.2010.78
Weller M, Berger H, Hartmann C, Schramm J, Westphal M, Simon M, Goldbrunner R, Krex D, Steinbach JP, Ostertag CB, Loeffler M, Pietsch T, von Deimling A: Combined 1p/19q loss in oligodendroglial tumors: predictive or prognostic biomarker?. Clin Cancer Res. 2007, 13: 6933-6937.
Wiens AL, Cheng L, Bertsch EC, Johnson KA, Zhang S, Hattab EM: Polysomy of chromosomes 1 and/or 19 is common and associated with less favorable clinical outcome in oligodendrogliomas: fluorescent in situ hybridization analysis of 84 consecutive cases. J Neuropathol Exp Neurol. 2012, 71: 618-624. 10.1097/NEN.0b013e31825b5f7a
Gerlinger M, Rowan AJ, Horswell S, Larkin J, Endesfelder D, Gronroos E, Martinez P, Matthews N, Stewart A, Tarpey P, Varela I, Phillimore B, Begum S, McDonald NQ, Butler A, Jones D, Raine K, Latimer C, Santos CR, Nohadani M, Eklund AC, Spencer-Dene B, Clark G, Pickering L, Stamp G, Gore M, Szallasi Z, Downward J, Futreal PA, Swanton C: Intratumor heterogeneity and branched evolution revealed by multiregion sequencing. N Engl J Med. 2012, 366: 883-892. 10.1056/NEJMoa1113205
Ficarra V, Brunelli M, Cheng L, Kirkali Z, Lopez-Beltran A, Martignoni G, Montironi R, Novara G, Van Poppel H: Prognostic and therapeutic impact of the histopathologic definition of parenchymal epithelial renal tumors. Eur Urol. 2010, 58: 655-668. 10.1016/j.eururo.2010.08.001
Montironi R, Mazzucchelli R, Scarpelli M, Lopez-Beltran A, Cheng L: Update on selected renal cell tumors with clear cell features. With emphasis on multilocular cystic clear cell renal cell carcinoma. Histol Histopathol. 2013, 28: 1555-1566.
Shen SS, Truong LD, Scarpelli M, Lopez-Beltran A: Role of immunohistochemistry in diagnosing renal neoplasms: when is it really useful?. Arch Pathol Lab Med. 2012, 136: 410-417. 10.5858/arpa.2011-0472-RA
Iliopoulos O: Molecular biology of renal cell cancer and the identification of therapeutic targets. J Clin Oncol. 2006, 24: 5593-5600. 10.1200/JCO.2006.08.8948
Motzer RJ, Rini BI, Bukowski RM, Curti BD, George DJ, Hudes GR, Redman BG, Margolin KA, Merchan JR, Wilding G, Ginsberg MS, Bacik J, Kim ST, Baum CM, Michaelson MD: Sunitinib in patients with metastatic renal cell carcinoma. JAMA. 2006, 295: 2516-2524. 10.1001/jama.295.21.2516
Tomlinson IP, Alam NA, Rowan AJ, Barclay E, Jaeger EE, Kelsell D, Leigh I, Gorman P, Lamlum H, Rahman S, Roylance RR, Olpin S, Bevan S, Barker K, Hearle N, Houlston RS, Kiuru M, Lehtonen R, Karhu A, Vilkki S, Laiho P, Eklund C, Vierimaa O, Aittomaki K, Hietala M, Sistonen P, Paetau A, Salovaara R, Herva R, Launonen V: Germline mutations in FH predispose to dominantly inherited uterine fibroids, skin leiomyomata and papillary renal cell cancer. Nat Genet. 2002, 30: 406-410. 10.1038/ng849
Motzer RJ, Bukowski RM: Targeted therapy for metastatic renal cell carcinoma. J Clin Oncol. 2006, 24: 5601-5608. 10.1200/JCO.2006.08.5415
Gobbo S, Eble JN, Grignon DJ, Martignoni G, MacLennan GT, Shah RB, Zhang S, Brunelli M, Cheng L: Clear cell papillary renal cell carcinoma: a distinct histopathologic and molecular genetic entity. Am J Surg Pathol. 2008, 32: 1239-1245. 10.1097/PAS.0b013e318164bcbb
Al-Ahmadie HA, Alden D, Fine SW, Gopalan A, Touijer KA, Russo P, Reuter VE, Tickoo SK: Role of immunohistochemistry in the evaluation of needle core biopsies in adult renal cortical tumors: an ex vivo study. Am J Surg Pathol. 2011, 35: 949-961. 10.1097/PAS.0b013e31821e25cd
Williamson SR, Halat S, Eble JN, Grignon DJ, Lopez-Beltran A, Montironi R, Tan PH, Wang M, Zhang S, Maclennan GT, Baldridge LA, Cheng L: Multilocular cystic renal cell carcinoma: similarities and differences in immunoprofile compared with clear cell renal cell carcinoma. Am J Surg Pathol. 2012, 36: 1425-1433. 10.1097/PAS.0b013e31825b37f0
Williamson SR, Eble JN, Cheng L, Grignon DJ: Clear cell papillary renal cell carcinoma: differential diagnosis and extended immunohistochemical profile. Mod Pathol. 2013, 26: 697-708. 10.1038/modpathol.2012.204
Skinnider BF, Folpe AL, Hennigar RA, Lim SD, Cohen C, Tamboli P, Young A, de Peralta-Venturina M, Amin MB: Distribution of cytokeratins and vimentin in adult renal neoplasms and normal renal tissue: potential utility of a cytokeratin antibody panel in the differential diagnosis of renal tumors. Am J Surg Pathol. 2005, 29: 747-754. 10.1097/01.pas.0000163362.78475.63
Allory Y, Bazille C, Vieillefond A, Molinie V, Cochand-Priollet B, Cussenot O, Callard P, Sibony M: Profiling and classification tree applied to renal epithelial tumours. Histopathology. 2008, 52: 158-166.
Truong LD, Shen SS: Immunohistochemical diagnosis of renal neoplasms. Arch Pathol Lab Med. 2011, 135: 92-109.
Paner GP, Srigley JR, Radhakrishnan A, Cohen C, Skinnider BF, Tickoo SK, Young AN, Amin MB: Immunohistochemical analysis of mucinous tubular and spindle cell carcinoma and papillary renal cell carcinoma of the kidney: significant immunophenotypic overlap warrants diagnostic caution. Am J Surg Pathol. 2006, 30: 13-19. 10.1097/01.pas.0000180443.94645.50
Went PT, Sauter G, Oberholzer M, Bubendorf L: Abundant expression of AMACR in many distinct tumour types. Pathology. 2006, 38: 426-432. 10.1080/00313020600922470
Kobayashi N, Matsuzaki O, Shirai S, Aoki I, Yao M, Nagashima Y: Collecting duct carcinoma of the kidney: an immunohistochemical evaluation of the use of antibodies for differential diagnosis. Hum Pathol. 2008, 39: 1350-1359. 10.1016/j.humpath.2007.11.020
Molinie V, Balaton A, Rotman S, Mansouri D, De Pinieux I, Homsi T, Guillou L: Alpha-methyl CoA racemase expression in renal cell carcinomas. Hum Pathol. 2006, 37: 698-703. 10.1016/j.humpath.2006.01.012
Delahunt B, Eble JN: Papillary renal cell carcinoma: a clinicopathologic and immunohistochemical study of 105 tumors. Mod Pathol. 1997, 10: 537-544.
Lin F, Brown RE, Shen T, Yang XJ, Schuerch C: Immunohistochemical detection of P504S in primary and metastatic renal cell carcinomas. Appl Immunohistochem Mol Morphol. 2004, 12: 153-159.
Tretiakova MS, Sahoo S, Takahashi M, Turkyilmaz M, Vogelzang NJ, Lin F, Krausz T, Teh BT, Yang XJ: Expression of alpha-methylacyl-CoA racemase in papillary renal cell carcinoma. Am J Surg Pathol. 2004, 28: 69-76. 10.1097/00000478-200401000-00007
Al-Ahmadie HA, Alden D, Qin LX, Olgac S, Fine SW, Gopalan A, Russo P, Motzer RJ, Reuter VE, Tickoo SK: Carbonic anhydrase IX expression in clear cell renal cell carcinoma: an immunohistochemical study comparing 2 antibodies. Am J Surg Pathol. 2008, 32: 377-382. 10.1097/PAS.0b013e3181570343
Gupta R, Balzer B, Picken M, Osunkoya AO, Shet T, Alsabeh R, Luthringer D, Paner GP, Amin MB: Diagnostic implications of transcription factor Pax 2 protein and transmembrane enzyme complex carbonic anhydrase IX immunoreactivity in adult renal epithelial neoplasms. Am J Surg Pathol. 2009, 33: 241-247. 10.1097/PAS.0b013e318181b828
Tan PH, Cheng L, Rioux-Leclercq N, Merino MJ, Netto G, Reuter VE, Shen SS, Grignon DJ, Montironi R, Egevad L, Srigley JR, Delahunt B, Moch H, Panel IRT: Renal tumors: diagnostic and prognostic biomarkers. Am J Surg Pathol. 2013, 37: 1518-1531. 10.1097/PAS.0b013e318299f12e
Klatte T, Seligson DB, Riggs SB, Leppert JT, Berkman MK, Kleid MD, Yu H, Kabbinavar FF, Pantuck AJ, Belldegrun AS: Hypoxia-inducible factor 1 alpha in clear cell renal cell carcinoma. Clin Cancer Res. 2007, 13: 7388-7393. 10.1158/1078-0432.CCR-07-0411
Stillebroer AB, Mulders PF, Boerman OC, Oyen WJ, Oosterwijk E: Carbonic anhydrase IX in renal cell carcinoma: implications for prognosis, diagnosis, and therapy. Eur Urol. 2010, 58: 75-83. 10.1016/j.eururo.2010.03.015
Genega EM, Ghebremichael M, Najarian R, Fu Y, Wang Y, Argani P, Grisanzio C, Signoretti S: Carbonic anhydrase IX expression in renal neoplasms: correlation with tumor type and grade. Am J Clin Pathol. 2010, 134: 873-879. 10.1309/AJCPPPR57HNJMSLZ
Corless CL, Aburatani H, Fletcher JA, Housman DE, Amin MB, Weinberg DS: Papillary renal cell carcinoma: quantitation of chromosomes 7 and 17 by FISH, analysis of chromosome 3p for LOH, and DNA ploidy. Diagn Mol Pathol. 1996, 5: 53-64. 10.1097/00019606-199603000-00009
Haudebourg J, Hoch B, Fabas T, Cardot-Leccia N, Burel-Vandenbos F, Vieillefond A, Amiel J, Michiels JF, Pedeutour F: Strength of molecular cytogenetic analyses for adjusting the diagnosis of renal cell carcinomas with both clear cells and papillary features: a study of three cases. Virchows Arch. 2010, 457: 397-404. 10.1007/s00428-010-0937-1
Kunju LP, Wojno K, Wolf JS, Cheng L, Shah RB: Papillary renal cell carcinoma with oncocytic cells and nonoverlapping low grade nuclei: expanding the morphologic spectrum with emphasis on clinicopathologic, immunohistochemical and molecular features. Hum Pathol. 2008, 39: 96-101. 10.1016/j.humpath.2007.05.016
Cossu-Rocca P, Eble JN, Zhang S, Martignoni G, Brunelli M, Cheng L: Acquired cystic disease-associated renal tumors: an immunohistochemical and fluorescence in situ hybridization study. Mod Pathol. 2006, 19: 780-787.
Reid-Nicholson MD, Motiwala N, Drury SC, Peiper SC, Terris MK, Waller JL, Ramalingam P: Chromosomal abnormalities in renal cell carcinoma variants detected by Urovysion fluorescence in situ hybridization on paraffin-embedded tissue. Ann Diagn Pathol. 2011, 15: 37-45. 10.1016/j.anndiagpath.2010.07.011
Cohen HT, McGovern FJ: Renal-cell carcinoma. N Engl J Med. 2005, 353: 2477-2490. 10.1056/NEJMra043172
Klatte T, Pantuck AJ, Said JW, Seligson DB, Rao NP, LaRochelle JC, Shuch B, Zisman A, Kabbinavar FF, Belldegrun AS: Cytogenetic and molecular tumor profiling for type 1 and type 2 papillary renal cell carcinoma. Clin Cancer Res. 2009, 15: 1162-1169. 10.1158/1078-0432.CCR-08-1229
Srigley JR, Delahunt B, Eble JN, Egevad L, Epstein JI, Grignon D, Hes O, Moch H, Montironi R, Tickoo SK, Zhou M, Argani P, Panel IRT: The International Society of Urological Pathology (ISUP) Vancouver Classification of Renal Neoplasia. Am J Surg Pathol. 2013, 37: 1469-1489. 10.1097/PAS.0b013e318299f2d1
Wu A, Kunju LP, Cheng L, Shah RB: Renal cell carcinoma in children and young adults: analysis of clinicopathological, immunohistochemical and molecular characteristics with an emphasis on the spectrum of Xp11.2 translocation-associated and unusual clear cell subtypes. Histopathology. 2008, 53: 533-544. 10.1111/j.1365-2559.2008.03151.x
Argani P, Hicks J, De Marzo AM, Albadine R, Illei PB, Ladanyi M, Reuter VE, Netto GJ: Xp11 translocation renal cell carcinoma (RCC): extended immunohistochemical profile emphasizing novel RCC markers. Am J Surg Pathol. 2010, 34: 1295-1303. 10.1097/PAS.0b013e3181e8ce5b
Rao Q, Williamson SR, Zhang S, Eble JN, Grignon DJ, Wang M, Zhou XJ, Huang W, Tan PH, Maclennan GT, Cheng L: TFE3 break-apart FISH has a higher sensitivity for Xp11.2 translocation-associated renal cell carcinoma compared with TFE3 or cathepsin K immunohistochemical staining alone: expanding the morphologic spectrum. Am J Surg Pathol. 2013, 37: 804-815. 10.1097/PAS.0b013e31827e17cb
Green WM, Yonescu R, Morsberger L, Morris K, Netto GJ, Epstein JI, Illei PB, Allaf M, Ladanyi M, Griffin CA, Argani P: Utilization of a TFE3 break-apart FISH assay in a renal tumor consultation service. Am J Surg Pathol. 2013, 37: 1150-1163. 10.1097/PAS.0b013e31828a69ae
Rao Q, Liu B, Cheng L, Zhu Y, Shi QL, Wu B, Jiang SJ, Wang Y, Wang X, Yu B, Zhang RS, Ma HH, Lu ZF, Tu P, Wang JD, Zhou XJ: Renal cell carcinomas with t(6;11)(p21;q12): A clinicopathologic study emphasizing unusual morphology, novel alpha-TFEB gene fusion point, immunobiomarkers, and ultrastructural features, as well as detection of the gene fusion by fluorescence in situ hybridization. Am J Surg Pathol. 2012, 36: 1327-1338. 10.1097/PAS.0b013e31825aafb5
Acknowledgement
This work was supported by the grant from the Science and Technology Commission of Shanghai Municipality (No.10DJ1400501).
Author information
Authors and Affiliations
Corresponding authors
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
LW is responsible for the execution, data interpretation, data analyses and drafting of the manuscript. LAB performed immunostaining for the study. SRW, MW, DDD, SZ, XD, and LC contributed to conception and design of study, data preparation and analysis, manuscript drafting and revisions. All authors read and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
{kind=link}
{kind=link}
{kind=link}
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article
Cite this article
Wang, L., Williamson, S.R., Wang, M. et al. Molecular subtyping of metastatic renal cell carcinoma: implications for targeted therapy. Mol Cancer 13, 39 (2014). https://doi.org/10.1186/1476-4598-13-39
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1476-4598-13-39