
Abstract
We report the case of a 64 year old woman who presented with symptomatology of gallstone disease but was radiologically shown to have a polyp within the gallbladder. Upon resection this was shown to be a metastasis from renal cell carcinoma for which she had had a nephrectomy six years previously.
Similar content being viewed by others

Case presentation
A 64 year old Caucasian female presented with recurrent right upper quadrant pain that radiated through to her back, often associated with ingestion of fatty foods. She also complained of unrelated episodes of regurgitation and vomiting. Of note, she had previously been diagnosed with a renal cell carcinoma and undergone a left nephrectomy, approximately six years ago. At the time, a follow-up ultrasound scan of her abdomen had revealed incidental gallstones. Abdominal examination revealed a soft abdomen with no localised tenderness or palpable masses. A working diagnosis of cholecystitis was made.
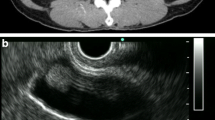
A repeat ultrasound scan confirmed the presence of gallstones, but also noted a 3 cm polyp within the gall-bladder. This appeared to be benign but a CT scan was carried out for further evaluation. This showed an irregular polyp centred within the gall-bladder with a tiny accompanying nodule on its medial surface.
The patient underwent a laparoscopic cholecystectomy without complication. At surgery, there was no evidence of metastatic disease. The gall-bladder was found to contain numerous small calculi and a polyp as demonstrated by previous imaging. The polyp was entirely within the gall-bladder and not extending into the liver (Figure 1, 2).

Intraoperative photograph showing gallbladder dissection and no infiltration into liver.

Macroscopic image of resected specimen with polyp visible.
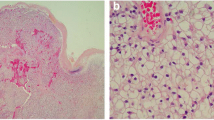
Histological examination revealed that the polyp was in fact a clear cell carcinoma consistent with metastatic renal cell carcinoma, which was morphologically similar to the renal tumour excised in 2001. She made an uneventful recovery and was discharged with planned follow-up by way of interval surveillance CT imaging.
Discussion
Metastases to the gall-bladder are very rare and and in most cases, the primary tumour is a malignant melanoma [1, 2]. Renal cell carcinomas account for approximately 3% of all adult malignancies and have the potential to metastasise to almost any site in the body [3]. The commonest sites are lung, soft tissue, bone, liver, skin and the central nervous system [4, 5]. Metastases to the gall-bladder are extremely uncommon and usually detected only at autopsy. Clinically, patients present with symptoms and signs typically associated with gallstone disease. This can occur many years after the initial nephrectomy. The nature of polypoidal masses within a gall-bladder can be difficult to elucidate [6]. Limani et al [2] stated that preoperative imaging was futile in differentiating between primary and secondary tumours of the gall-bladder. They reported that primary tumours often coexisted with gallstones whilst metastatic disease was associated with an acalculus gall-bladder. The latter are often associated with hypervascularity on diagnostic imaging [7].
Metastatic gall-bladder involvement is associated with a poorer prognosis. 23 cases of metastatic renal cell carcinoma of the gall-bladder have been reported - of these 9 remained free of recurrent disease post cholecystectomy, with the longest follow up interval being 6 years [8]. Although metastases are a bad prognostic factor, it seems that patients with solitary metastases such as in the gallbladder have an improvement in survival after resection of the lesion [4], usually by way of a laparoscopic cholecystectomy.
Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Abbreviations
- CT:
-
Computed tomography.
References
Sparwasser C, Krupenski M, Radomsky J, Pust RA: Gallbladder metastasis of renal cell carcinoma. A case report and review of the literature. Urol Int. 1997, 58 (4): 257-258.
Limani K, Matos C, Hut F, Gelin M, Closset J: Metastatic carcinoma of the gallbladder after a renal cell carcinoma. Acta Chir Belg. 2003, 103 (2): 233-234.
Park JS, Chae YS, Hong SJ, Shin DH, Choi JS, Kim BR: Metastatic renal cell carcinoma of the gallbladder. Yonsei Med J. 2003, 44 (2): 355-358.
Pandey D, Kane SV, Shukla PJ, Shrikhande SV, Tongaonkar HB: Isolated gall bladder metastasis from renal cell carcinoma. Indian J Gastroenterol. 2006, 25 (3): 161-162.
Finkelstein LH, Coffman LM: Acute cholecystitis or metastatic renal cell carcinoma? a diagnostic dilemma. J Am Osteopath Assoc. 1996, 96 (5): 314-315.
Celebi I, Guezelsoy M, Yorukoglu K, Kirkali Z: Renal cell carcinoma with gallbladder metastasis. Int J Urol. 1998, 5 (3): 288-290. 10.1111/j.1442-2042.1998.tb00605.x.
Aoki T, Inoue K, Tsuchida A, Aoki T, Kasuya K, Kitamaru K, Koyanagi Y, Shimizu T: Gallbladder metastasis of renal cell carcinoma: report of two cases. Surg Today. 2002, 32 (1): 89-92. 10.1007/s595-002-8123-6.
Ishizawa T, Okuda T, Kawanishi T, Kitagawa T, Sekikawa T, Yakumaru K: Metastatic renal cell carcinoma of the gallbladder. Asian J Surg. 2006, 29 (3): 145-148.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
BZ and NP wrote the paper, SP and SG edited and revised the paper, KS and TL performed the surgery, JG interpreted the specimen. All authors have read and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
{kind=link}
{kind=link}
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Patel, S., Zebian, B., Gurjar, S. et al. An unusual gall-bladder polyp - site of metastatic renal cell carcinoma: a case report. Cases Journal 2, 172 (2009). https://doi.org/10.1186/1757-1626-2-172
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1757-1626-2-172