
Abstract
Introduction
While non-invasive ventilation aimed at avoiding intubation has become the modality of choice to treat mild to moderate acute respiratory acidosis, many severely acidotic patients (pH <7.20) still need intubation. Extracorporeal veno-venous CO2 removal (ECCO2R) could prove to be an alternative. The present animal study tested in a systematic fashion technical requirements for successful ECCO2R in terms of cannula size, blood and sweep gas flow.
Methods
ECCO2R with a 0.98 m2 surface oxygenator was performed in six acidotic (pH <7.20) pigs using either a 14.5 French (Fr) or a 19Fr catheter, with sweep gas flow rates of 8 and 16 L/minute, respectively. During each experiment the blood flow was incrementally increased to a maximum of 400 mL/minute (14.5Fr catheter) and 1000 mL/minute (19Fr catheter).
Results
Amelioration of severe respiratory acidosis was only feasible when blood flow rates of 750 to 1000 mL/minute (19Fr catheter) were used. Maximal CO2-elimination was 146.1 ± 22.6 mL/minute, while pH increased from 7.13 ± 0.08 to 7.41 ± 0.07 (blood flow of 1000 mL/minute; sweep gas flow 16 L/minute). Accordingly, a sweep gas flow of 8 L/minute resulted in a maximal CO2-elimination rate of 138.0 ± 16.9 mL/minute. The 14.5Fr catheter allowed a maximum CO2 elimination rate of 77.9 mL/minute, which did not result in the normalization of pH.
Conclusions
Veno-venous ECCO2R may serve as a treatment option for severe respiratory acidosis. In this porcine model, ECCO2R was most effective when using blood flow rates ranging between 750 and 1000 mL/minute, while an increase in sweep gas flow from 8 to 16 L/minute had less impact on ECCO2R in this setting.
Similar content being viewed by others

Introduction
Non-invasive ventilation (NIV) has become the modality of choice to treat mild to moderate respiratory acidosis (pH ≥7.20) due to chronic obstructive pulmonary disease (COPD) exacerbation, since it has been shown to avoid intubation and intubation-related complications, resulting in reduced ICU-mortality [1]. However, real-life observations have revealed high rates of both intubation and mortality in patients with COPD exacerbation and severe acute hypercapnic respiratory failure [2–4]. This is related to severe respiratory acidosis, well-established contraindications of NIV, lack of staff training and the presence of co-morbidities hindering the successful application of NIV [5, 6].
This has led to the attempt of extracorporeal carbon dioxide (CO2) removal (ECCO2R) in patients presenting with acute hypercapnic respiratory failure. ECCO2R systems have been successfully used to reduce invasiveness of mechanical ventilation and, therefore, ventilator-induced lung injury in acute respiratory distress syndrome (ARDS) patients [7–12]. Recently, ECCO2R by means of a pumpless, arterio-venous extracorporeal lung-assist has been shown to preclude the need for intubation and invasive mechanical ventilation in a case–control study in COPD patients with acute-on-chronic respiratory failure [13]. In addition, previous research has demonstrated that this technique is capable of eliminating approximately 50% of the calculated CO2 production, with rapid normalization of respiratory acidosis [14]. Importantly, these systems are driven by the arterio-venous pressure gradient; thus, cannulation of arterial vessels (most commonly the femoral artery), coupled with cannulation of the corresponding vein on the contralateral limb, is necessary for driving the system [13–15]. Based on these preconditions, there are clearly defined contraindications and several complications directly related to arterial cannulation, such as bleeding, hematoma or aneurysm at the insertion site, and ischemia and/or compartment syndrome of the lower limb [15, 16].
Interestingly, a recent study reported the successful application of a pump-driven veno-venous system using a 15.5 French (Fr) dual-lumen catheter with a mean blood flow of 431 ml/minute [17]. Even though this was a pilot study testing the feasibility of this new approach, the study showed the potential of these veno-venous systems to improve respiratory acidosis without requiring arterial cannulation. However, patients only had moderate respiratory acidosis, and it remains unclear how these results translate to more severe respiratory acidosis. Accordingly, clinical experience suggests that substantially higher flow rates are needed to correct severe respiratory acidosis (pH <7.2) [18]. In this regard, the physiological relationships between cannula size, blood flow, sweep gas flow and gas transfer capacity, respectively, are still largely unknown. For this reason, more physiological data on these issues are needed before the promising technique of miniaturized veno-venous ECCO2R can be tested in a broader clinical setting. Therefore, we set up an animal study that aimed to elucidate the relationships between cannula size, blood flow and sweep gas flow, respectively, in pigs with experimentally-induced severe respiratory acidosis that mimicked severe acute hypercapnic respiratory failure with pH values between 7.0 and 7.2.
Material and methods
Extracorporeal CO2 removal techniques
For ECCO2R a pump assisted lung protection (PALP) System® (Maquet Cardiopulmonary Care, Rastatt, Germany) based on the Cardiohelp® platform was used. The oxygenator has an area of 0.98 m2 with a poly methylpentene membrane lacking heat exchange fibers. The priming volume of the whole system is 247 ml. The PALP system® was primed with normal saline solution. Heparin (1,000 IE) was added to the running system.
For venous access, a 14.5Fr hemodialysis catheter (Fresenius Medical Care, Bad Homburg Germany) was used during Experiments 1 and 2, while a 19Fr Bicaval Avalon ELITE Dual Lumen Cannula® (Maquet Cardiopulmonary Care, Rastatt, Germany) was implanted for Experiments 3, 4 and 5. Pigs were anticoagulated with heparin during extracorporeal treatment. For all experiments, the sweep gas flow was applied with 100% oxygen by a Flow-i Anesthesia Delivery System (Maquet Critical Care, Solna, Sweden); in a subset of animals the sweep gas flow was provided with room air.
Animal model
The study was approved by the Animal Research Committee of Uppsala University in Sweden (ethical approval number: C265/12). Pigs (body weight = 39.8 ± 2.9 kg) were anesthetized with IV ketamine 25 to 50 mg/kg/hour, midazolam 90 to 180 μg/kg/hour, fentanyl 3 to 6 μg/kg/hour and rocuronium 2.5 to 5.0 mg/kg/hour. The trachea was intubated with a cuffed endotracheal tube (inner diameter, 7 mm). The pigs were ventilated with a Servo-i ventilator (Maquet Critical Care, Solna, Sweden). Body temperature was kept at 37°C throughout the whole study period by the use of a warm blanket. Arterial blood was taken from the left carotid artery. The estimated CO2 production is about 7 ml/kg/minute in pigs [19], that is, a CO2 production of approximately 280 ml/minute, which is comparable to an adult human.
Study design
ECCO2R was performed in six pigs following intubation, mechanical ventilation and induction of respiratory acidosis by increased dead space ventilation. In detail, anatomical dead space was increased by adding a further tube between the endotracheal tube and the ‘Y’ piece of the ventilator circuit. The length of the additional tube was titrated until respiratory acidosis was induced with a pH value of 7.0 to 7.1. Pigs were ventilated in a volume controlled mode with a tidal volume of 360 ml, a positive end expiratory pressure (PEEP) of 6 cm H2O and a breathing frequency of 15/minute. Dead space fractions and CO2 elimination were measured with a NICO monitor (Philips, Wallingford, CT, USA), where airway flow and CO2 signals were monitored by mainstream sensors placed between the endotracheal tube and the ‘Y’ piece of the ventilator circuit. Dead space was computed as PCO2et–PeCO2/PCO2et, where PCO2et represents the end-tidal partial pressure of CO2 and PeCO2 the mixed expired CO2. Dead space fraction was measured in the first pig by the Bohr equation, with a resulting fraction of 0.85. This dead space fraction was subsequently maintained for the entire duration of the experimental period.
Five experiments were performed in each pig in a standardized fashion. First, ECCO2R was performed via a 14.5Fr hemodialysis catheter inserted into the right jugular vein (experiments 1 and 2). Subsequently, ECCO2R was performed via the 19Fr catheter following re-catheterization of the same right jugular vein (experiments 3, 4, and 5). Correct placement of the 19Fr cannula was confirmed by echocardiography. Equal conditions were used across all experiments (lasting at least 60 minutes), with each experiment starting at the pre-determined acidotic conditions.
During experiments 1 to 4, blood flow rates were increased in a stepwise fashion, while sweep gas flow was maintained (Table 1). Each step lasted 15 minutes in order to achieve equilibrium conditions, with all measurements taken at the end of this 15-minute period.
During experiment 5, sweep gas flow was changed by increasing flow in a stepwise approach (Table 1), while blood flow was maintained at a rate of 1,000 ml/min. Each step lasted 15 minutes in order to achieve equilibrium conditions.
CO2 and blood gas measurement
CO2 was measured in the mainstream of the exhaust/sweep-gas outlet of the oxygenator by the Vaisala Carbocap GM 70 (Vaisala, Bonn, Germany). A water trap was integrated into the circuit before CO2 measurement. CO2 removal was calculated by multiplying the sweep gas flow with CO2 in Vol% in the exhaust/sweep-gas outlet. CO2 was measured with 0.04 Vol% in fresh air. Blood gas analysis was performed with an ABL 800, Radiometer, (Copenhagen, Denmark).
Statistics
For statistical analysis, GraphPad Prism 5 for Macintosh computer (La Jolla, CA USA) was used. Data were tested for normality using the Kolmogorov-Smirnov test with a cut-off P value of <0.05. Normally-distributed data are expressed as mean and standard deviation.
Results
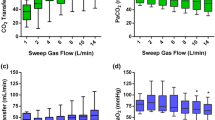
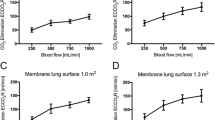
ECCO2R was most effective with the 19Fr catheter at higher blood flow levels (experiments 3 and 4; Figure 1), with no clear difference between different sweep gas flow (8 versus 16 L/minute) conditions. In contrast, ECCO2R was less efficient with the 14.5Fr catheter (experiments 1 and 2; Figure 1). As a consequence, partial pressure of CO2 in arterial blood (PaCO2) progressively decreased with increasing blood flow when the 19Fr catheter, but not the 14.5Fr catheter, was used (Figure 2). Similarly, pH values progressively increased in proportion with blood flow with the 19Fr catheter, but not the 14.5Fr catheter (Figure 3). Of note, non-acidotic blood gas values were only achieved with 19Fr catheters at blood flow rates ranging from 750 to 1,000 ml/minute. Detailed data on CO2 elimination and related blood gas values relative to different blood flow levels at a sweep gas flow of 16 L/minute are provided in Tables 2 and 3 and Additional file 1, respectively. The absolute values of CO2 elimination were normalized to the partial pressure of CO2 in venous blood (PvCO2) and a partial pressure of CO2 (PCO2) value of 45 mmHg according to Wearden et al. [20] and are provided in Figure 4.

Elimination of carbon dioxide (CO 2 ) depending on blood flow. A) 14.5Fr catheter; 8 L/minute sweep gas flow. B) 14.5Fr catheter; 16 L/minute sweep gas flow. C) 19Fr catheter; 8 L/minute sweep gas flow. D) 19Fr catheter; 16 L/minute sweep gas flow. Fr, French.

Partial pressure of arterial carbon dioxide (PaCO 2 ) depending on blood flow. A) 14.5Fr catheter; 8 L/minute sweep gas flow. B) 14.5Fr catheter; 16 L/minute sweep gas flow. C) 19Fr catheter; 8 L/minute sweep gas flow. D) 19Fr catheter; 16 L/minute sweep gas flow. Fr, French.

pH dependence on blood flow. A) 14.5Fr catheter; 8 L/minute sweep gas flow. B) 14.5Fr catheter; 16 L/minute sweep gas flow. C) 19Fr catheter; 8 L/minute sweep gas flow. D) 19Fr catheter; 16 L/minute sweep gas flow. Fr, French.

Normalized elimination of carbon dioxide (CO 2 ) depending on blood flow. A) 14.5Fr catheter; 8 L/minute sweep gas flow. B) 14.5Fr catheter; 16 L/minute sweep gas flow. C) 19Fr catheter; 8 L/minute sweep gas flow. D) 19Fr catheter; 16 L/minute sweep gas flow.
Corresponding data for different sweep gas flows were comparable, where a higher sweep gas flow of 16 L/minute resulted in only a slightly more effective ECCO2R compared to a lower sweep gas flow of 8 L/minute (Tables 2 and 3 and Additional file 1). However, a sweep gas flow below 6 L/minute resulted in less effective ECCO2R when large (19Fr) catheters were used at high blood flow levels (1,000 ml/minute) (Figure 5). The extracorporeal system was more effective with higher PvCO2 and lower blood flow levels and a longer oxygenator contact time, as demonstrated by a lower PCO2 post-oxygenator (Figure 6).

Elimination of carbon dioxide (CO 2 ) in dependence of sweep gas flow under a fixed flood flow of 1,000 ml/minute using a 19Fr catheter. Fr, French.

Partial pressure of arterial (PaCO 2 ) and venous (PvCO 2 ) carbon dioxide depending on blood flow, sweep gas flow and cannula size. A) 14.5Fr catheter; 8 L/minute sweep gas flow. B) 14.5Fr catheter; 16 L/minute sweep gas flow. C) 19Fr catheter; 8 L/minute sweep gas flow. D) 19Fr catheter; 16 L/minute sweep gas flow. Fr, French.
In three pigs, the sweep gas flow was switched from 100% oxygen to room air at the end of experiment 5, with blood flow rates of 1,000 ml/minute. This resulted in a further increase in CO2 removal (150 ± 26.6 versus 159.8 ± 22.6 ml/minute).
Discussion
The present porcine study indicates that pump-driven veno-venous ECCO2R can normalize pH values and reduce PaCO2 in severe, life-threatening respiratory acidosis under constant ventilatory support. In addition, the present study suggests that a blood flow of 750 to 1,000 ml/minute is needed to achieve these results, since pH values remained acidotic at lower blood flow rates.
In particular, the severe respiratory acidosis in the model used in this study could not be sufficiently corrected either by ECCO2R at a blood flow of 200 to 400 ml/minute using the 14.5Fr catheter, or with blood flow rates of 500 ml/minute using the 19Fr cannula. In contrast, severe respiratory acidosis was normalized by veno-venous ECCO2R using the 19Fr catheter and a blood flow rate of 1,000 ml/minute, even though a blood flow of 750 ml/minute was sufficient in 50% of the animals. This finding contrasts with a recent study in human patients, where the application of a pump-driven veno-venous system using a 15.5Fr dual-lumen catheter was successful with a mean blood flow of 431 ml/minute [17]. Importantly, however, the mean pH in that study was around 7.25, thus considerably higher compared to the pH in the present study. Thus, based on the current findings, it remains questionable whether more acidotic pH values could also be successfully corrected by lower blood flow rates, although the 15.5Fr catheter has a more favorable design compared to the 14.5Fr Shaldon catheter. Therefore, using low-diameter catheters and low blood flow rates, pump-driven veno-venous ECCO2R may be primarily feasible in patients with mild to moderate respiratory acidosis. This may be aimed at reducing aggressiveness of invasive ventilation as originally, and also recently, described in patients with ARDS [7, 9, 12, 21, 22].
Interestingly, the ECCO2R capacity of the system used in the present study was in line with previous findings that were also derived from an animal study, where a removal-capacity up to 150 ml CO2/minute could be achieved with a blood flow of 1,000 ml/minute and an 18Fr catheter [23]. In accordance with the present trial, lower blood flow rates resulted in less efficient ECCO2R. In clear contrast, however, the mentioned trial provided evidence that ventilation parameters could be reduced following ECCO2R, but again, animals were not as severely acidotic as those in the present study. Therefore, the current study provides the first evidence that even severe acidosis can be successfully managed by ECCO2R and, in agreement with our clinical experience, this was only feasible with catheters that allowed blood flow rates of 750 to 1,000 ml/minute.
Since intensive care specialists are familiar with 14.5Fr hemodialysis catheters, it would be reasonable to test whether these catheters also qualify for ECCO2R. However, the maximal blood flow through these catheters is physiologically restricted to approximately 400 ml/minute. Furthermore, catheters specifically designed for ECCO2R aim to avoid recirculation [24, 25]; this is particularly evident if the PCO2 of the venous blood, which is directed towards the oxygenator, is lower than arterial PCO2. Of note, recirculation was obvious when hemodialysis catheters were used, even with the lowest blood flow rates, demonstrated by a much lower CO2 before oxygenator than in the arterial blood (Figure 6A and B). In contrast, the specifically designed 19Fr catheter produced no significant recirculation, represented by higher CO2 before oxygenator than in arterial blood (Figure 6C and D). Therefore, (1) blood flow rates and (2) the specific technical design of the catheter that prevents recirculation are the main determinants of successful ECCO2R. Furthermore, CO2 elimination of the oxygenator depends closely on the diffusion gradient of CO2 between venous blood and the sweep gas. Therefore, with a higher CO2 content in venous blood, more CO2 will be eliminated, which has to be taken into consideration at the beginning of the experiments, when PvCO2 is highest. Furthermore, PaCO2 and PvCO2 were slightly higher in the low-flow group with the 19Fr than with the 14.5Fr catheter.
In the 1970’s, Kolobow [26] and Gattinoni [27] indicated that ECCO2R is dependent not only on venous PCO2, blood flow and sweep gas flow, but also on the size of the oxygenator. The currently used oxygenator provides a surface area of 0.98 m2 without heat exchange fibers. The high efficiency of the system is reflected by a very low mean PaCO2 value, leading to alkalotic pH values in the blood that is delivered by the oxygenator at low blood flow rates. This may explain why the previously described linear relationship between sweep gas flow and ECCO2R was not observed [22, 24, 28]. As shown by the present study, sweep gas flow rates of more than 6 L/minute, but not lower flow rates, can sufficiently maintain an optimal ECCO2R when a blood flow rate of 1,000 ml/minute is applied.
Interestingly, ECCO2R tended to be more efficient when 100% oxygen was switched to room air sweep gas. As hypercapnic respiratory failure is not necessarily associated with severe hypoxemia, the use of air as a sweep gas may slightly improve the effectiveness of ECCO2R, but will also reduce the oxygen transfer capacity of the extracorporeal support. On the other hand, the application of oxygen sweep gas was sufficient to improve oxygenation when the ratio of catheter blood flow rate to cardiac output was relatively high, in line with previous results [24].
The current study has some limitations. First, data acquired in animals cannot automatically be transferred into a clinical setting; however, the animals showed CO2 production and cardiac output rates that were similar to those observed in adult humans. Previous studies in humans have already shown the clinical effects of ECCO2R; thus, the present data are likely to be helpful in understanding the physiology of ECCO2R in humans as well. Furthermore, the anatomy of the pig is not comparable to a human adult, and the catheters we used may not be ideal in clinical practice. However, the perfect cannula for CO2 removal still has to be designed. Second, the typical clinical scenario of exacerbated COPD with severe airflow limitation was not simulated, since a rather high dead space ventilation protocol was used to artificially increase PaCO2. Therefore, the interaction between ECCO2R and mechanical ventilation could not be investigated. This, however, is suggested to be of clinical importance, since severe airflow limitation frequently requires the adaptation of ventilator settings. This, in turn, can lead to reduced alveolar ventilation that potentially impacts on acidosis. Third, the present study only applied short-term ECCO2R. In a real-life setting, the long-term effects of blood flow, cannula size and sweep gas flow application need to be elucidated, since CO2 is also stored in the form of HCO3 in slow compartments, and it may take several hours until a steady-state is reached. This is particularly pertinent to patients with acute-on-chronic ventilatory failure who present with respiratory acidosis, hypercapnia and high bicarbonate levels. On the other hand, the time constant for reducing blood CO2 in patients by ventilation is 10 minutes [29]; therefore, 15 minutes at each setting should have been an adequate amount of time to detect any changes in PaCO2. Furthermore, in the present study we did not put the focus on anticoagulation since clotting was no issue in our short-term experiments of 12 hours duration. Further studies have to be done in humans, since low-flow devices may need more anticoagulation in comparison to high-flow extracorporeal membrane oxygenation (ECMO). Finally, only one system for ECCO2R was tested in the present study, and this is suggested to limit the comparison of the current trial with other trials, in which different systems have been used. Nevertheless, the currently used system has shown to be highly effective for ECCO2R represented by a PCO2 lower than 10 mmHg and a PO2 of 600 mmHg after the oxygenator with low blood flows. Although other systems function in a different way, it is physically difficult to further lower PCO2. Thus, we believe that the present study is valid to systematically show changes in physiology during ECCO2R when using different conditions.
Conclusions
In conclusion, this animal study has shown that severe respiratory acidosis can be successfully managed by veno-venous ECCO2R, but only when blood flow rates ranging between 750 and 1,000 ml/minute are applied. For this purpose, the use of specifically-designed catheters with an inner diameter greater than that of the typical hemodialysis catheters are required to establish flow rates ranging between 750 and 1,000 ml/minute and to avoid blood recirculation. In addition, the study has shown that a sweep gas flow rate above 6 L/minute is of minor importance for ECCO2R when using modern, highly-efficient oxygenators with low blood-flow rates. This holds true for the system tested, which is highly effective, represented by a PvCO2 of 10 to 30 mmHg after the oxygenator and, therefore, may be translated to comparable systems. This study also suggests that low-flow veno-venous ECCO2R with modern miniaturized membrane lungs can serve as a treatment option for severe respiratory acidosis associated with acute respiratory failure and severe hypercapnia. Whether these techniques prove to be suitable to avoid endotracheal intubation or to facilitate early extubation in intubated patients needs to be elucidated by future clinical trials.
Key messages
-
Severe respiratory acidosis with pH values of 7.0 to 7.2 can be successfully managed by veno-venous ECCO2R.
-
For this purpose, blood flow rates ranging between 750 and 1,000 ml/minute are mandatory.
-
Specifically-designed catheters aimed at avoiding blood recirculation warranting the target blood flow are required.
-
Sweep gas flow rates above 6 L/minute are sufficient for maximal ECCO2R.
Abbreviations
- ARDS:
-
acute respiratory distress syndrome
- COPD:
-
chronic obstructive pulmonary disease
- ECCO2R:
-
extracorporeal CO2 removal
- ECMO:
-
extracorporeal membrane oxygenation
- Fr:
-
French
- PaCO2:
-
partial pressure of CO2 in arterial blood
- PALP:
-
pump assisted lung protection
- PCO2:
-
partial pressure of CO2
- PEEP:
-
positive end expiratory pressure
- PVCO2:
-
partial pressure of CO2 in venous blood
- NIV:
-
non-invasive ventilation.
References
Lightowler JV, Wedzicha JA, Elliott MW, Ram FS: Non-invasive positive pressure ventilation to treat respiratory failure resulting from exacerbations of chronic obstructive pulmonary disease: Cochrane systematic review and meta-analysis. BMJ 2003, 326: 185.
Chandra D, Stamm JA, Taylor B, Ramos RM, Satterwhite L, Krishnan JA, Mannino D, Sciurba FC, Holguin F: Outcomes of noninvasive ventilation for acute exacerbations of chronic obstructive pulmonary disease in the United States, 1998–2008. Am J Respir Crit Care Med 2012, 185: 152-159.
Hoo GW, Hakimian N, Santiago SM: Hypercapnic respiratory failure in COPD patients: response to therapy. Chest 2000, 117: 169-177.
Quinnell TG, Pilsworth S, Shneerson JM, Smith IE: Prolonged invasive ventilation following acute ventilatory failure in COPD: weaning results, survival, and the role of noninvasive ventilation. Chest 2006, 129: 133-139.
Ambrosino N, Vagheggini G: Noninvasive positive pressure ventilation in the acute care setting: where are we? Eur Respir J 2008, 31: 874-886.
Conti G, Antonelli M, Navalesi P, Rocco M, Bufi M, Spadetta G, Meduri GU: Noninvasive vs. conventional mechanical ventilation in patients with chronic obstructive pulmonary disease after failure of medical treatment in the ward: a randomized trial. Intensive Care Med 2002, 28: 1701-1707.
Gattinoni L, Agostoni A, Pesenti A, Pelizzola A, Rossi GP, Langer M, Vesconi S, Uziel L, Fox U, Longoni F, Kolobow T, Damia G: Treatment of acute respiratory failure with low-frequency positive-pressure ventilation and extracorporeal removal of CO2. Lancet 1980, 2: 292-294.
Gattinoni L, Kolobow T, Tomlinson T, Iapichino G, Samaja M, White D, Pierce J: Low-frequency positive pressure ventilation with extracorporeal carbon dioxide removal (LFPPV-ECCO2R): an experimental study. Anesth Analg 1978, 57: 470-477.
Terragni PP, Del Sorbo L, Mascia L, Urbino R, Martin EL, Birocco A, Faggiano C, Quintel M, Gattinoni L, Ranieri VM: Tidal volume lower than 6 ml/kg enhances lung protection: role of extracorporeal carbon dioxide removal. Anesthesiology 2009, 111: 826-835.
Bein T, Weber-Carstens S, Goldmann A, Muller T, Staudinger T, Brederlau J, Muellenbach R, Dembinski R, Graf BM, Wewalka M, Philipp A, Wernecke KD, Lubnow M, Slutsky AS: Lower tidal volume strategy (approximately 3 ml/kg) combined with extracorporeal CO2 removal versus ‘conventional’ protective ventilation (6 ml/kg) in severe ARDS: the prospective randomized Xtravent-study. Intensive Care Med 2013, 39: 847-856.
Livigni S, Maio M, Ferretti E, Longobardo A, Potenza R, Rivalta L, Selvaggi P, Vergano M, Bertolini G: Efficacy and safety of a low-flow veno-venous carbon dioxide removal device: results of an experimental study in adult sheep. Crit Care 2006, 10: R151.
Batchinsky AI, Jordan BS, Regn D, Necsoiu C, Federspiel WJ, Morris MJ, Cancio LC: Respiratory dialysis: reduction in dependence on mechanical ventilation by venovenous extracorporeal CO2 removal. Crit Care Med 2011, 39: 1382-1387.
Kluge S, Braune SA, Engel M, Nierhaus A, Frings D, Ebelt H, Uhrig A, Metschke M, Wegscheider K, Suttorp N, Rousseau S: Avoiding invasive mechanical ventilation by extracorporeal carbon dioxide removal in patients failing noninvasive ventilation. Intensive Care Med 2012, 38: 1632-1639.
Muller T, Lubnow M, Philipp A, Bein T, Jeron A, Luchner A, Rupprecht L, Reng M, Langgartner J, Wrede CE, Zimmermann M, Birnbaum D, Schmid C, Riegger GA, Pfeifer M: Extracorporeal pumpless interventional lung assist in clinical practice: determinants of efficacy. Eur Respir J 2009, 33: 551-558.
Moerer O, Quintel M: Protective and ultra-protective ventilation: using pumpless interventional lung assist (iLA). Minerva Anestesiol 2011, 77: 537-544.
Bein T, Weber F, Philipp A, Prasser C, Pfeifer M, Schmid FX, Butz B, Birnbaum D, Taeger K, Schlitt HJ: A new pumpless extracorporeal interventional lung assist in critical hypoxemia/hypercapnia. Crit Care Med 2006, 34: 1372-1377.
Burki NK, Mani RK, Herth FJ, Schmidt W, Teschler H, Bonin F, Becker H, Randerath WJ, Stieglitz S, Hagmeyer L, Priegnitz C, Pfeifer M, Blaas SH, Putensen C, Theuerkauf N, Quintel M, Moerer O: A novel extracorporeal CO(2) removal system: results of a pilot study of hypercapnic respiratory failure in patients with COPD. Chest 2013, 143: 678-686.
Abrams DC, Brenner K, Burkart KM, Agerstrand CL, Thomashow BM, Bacchetta M, Brodie D: Pilot study of extracorporeal carbon dioxide removal to facilitate extubation and ambulation in exacerbations of chronic obstructive pulmonary disease. Ann Am Thorac Soc 2013, 10: 307-314.
van Milgen J, Noblet J, Dubois S, Bernier JF: Dynamic aspects of oxygen consumption and carbon dioxide production in swine. Br J Nutr 1997, 78: 397-410.
Wearden PD, Federspiel WJ, Morley SW, Rosenberg M, Bieniek PD, Lund LW, Ochs BD: Respiratory dialysis with an active-mixing extracorporeal carbon dioxide removal system in a chronic sheep study. Intensive Care Med 2012, 38: 1705-1711.
Gattinoni L, Pesenti A, Mascheroni D, Marcolin R, Fumagalli R, Rossi F, Iapichino G, Romagnoli G, Uziel L, Agostoni A, Kolobow T, Giorgio D: Low-frequency positive-pressure ventilation with extracorporeal CO2 removal in severe acute respiratory failure. JAMA 1986, 256: 881-886.
Karagiannidis C, Lubnow M, Philipp A, Riegger GA, Schmid C, Pfeifer M, Mueller T: Autoregulation of ventilation with neurally adjusted ventilatory assist on extracorporeal lung support. Intensive Care Med 2010, 36: 2038-2044.
Cardenas VJ Jr, Miller L, Lynch JE, Anderson MJ, Zwischenberger JB: Percutaneous venovenous CO2 removal with regional anticoagulation in an ovine model. ASAIO J 2006, 52: 467-470.
Schmidt M, Tachon G, Devilliers C, Muller G, Hekimian G, Brechot N, Merceron S, Luyt CE, Trouillet JL, Chastre J, Leprince P, Combes A: Blood oxygenation and decarboxylation determinants during venovenous ECMO for respiratory failure in adults. Intensive Care Med 2013, 39: 838-846.
Korver EP, Ganushchak YM, Simons AP, Donker DW, Maessen JG, Weerwind PW: Quantification of recirculation as an adjuvant to transthoracic echocardiography for optimization of dual-lumen extracorporeal life support. Intensive Care Med 2012, 38: 906-909.
Kolobow T, Gattinoni L, Tomlinson TA, Pierce JE: Control of breathing using an extracorporeal membrane lung. Anesthesiology 1977, 46: 138-141.
Gattinoni L, Kolobow T, Tomlinson T, White D, Pierce J: Control of intermittent positive pressure breathing (IPPB) by extracorporeal removal of carbon dioxide. Br J Anaesth 1978, 50: 753-758.
Park M, Costa EL, Maciel AT, Silva DP, Friedrich N, Barbosa EV, Hirota AS, Schettino G, Azevedo LC: Determinants of oxygen and carbon dioxide transfer during extracorporeal membrane oxygenation in an experimental model of multiple organ dysfunction syndrome. PLoS One 2013, 8: e54954.
Taskar V, John J, Larsson A, Wetterberg T, Jonson B: Dynamics of carbon dioxide elimination following ventilator resetting. Chest 1995, 108: 196-202.
Acknowledgments
The study was financially supported by Maquet, Sweden. This exclusively refers to the materials and the setting being used. The authors state that neither the study design, the results, the interpretation of the findings nor any other subject discussed in the submitted manuscript was dependent on support. Dr. Sandra Dieni is acknowledged for helpful comments on the manuscript prior to submission.
Funding
The PALP system was provided by Maquet, Rastatt, Germany. The laboratory costs were covered by Maquet Critical Care, Solna, Sweden and the Swedish Heart and Lung foundation.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
CK received travel grants and lecture fees from Maquet, Rastatt, Germany. KK, GH and AL have no competing interests. FSS performs consultant services for Maquet Critical Care, Sweden. WW received fees for advisory board meetings and lectures from Maquet, Rastatt, Germany. TM received travel grants from Maquet, Rastatt, Germany. All authors declare that they have no non-financial competing interests.
Authors’ contributions
CK designed the study (together with KA and TM). CK, FS and AL performed the animal experiments and analyzed the physiological data (together with TM and WW). GH designed and supervised the study and the analysis of results. WW and CK designed the concept of the manuscript; all the other authors (CK, KA, FS, AL, GH, TM) contributed to the final drafting of the manuscript. All authors read and approved the final manuscript.
Wolfram Windisch and Thomas Mueller contributed equally to this work.
Electronic supplementary material
13054_2013_2567_MOESM1_ESM.doc
Additional file 1:Absolute values of CO 2 elimination and blood gas analysis with a sweep gas flow of 8 L O 2 /minute depending on blood flow. The table shows the CO2 elimination capacity of the ECCO2R system and the corresponding blood gas analysis with a sweep gas flow of 8 L O2/minute with a hemodialysis catheter (A) and the 19Fr Bicaval Dual Lumen Catheter (B) according to different blood flow levels. It is clearly shown that ECCO2R is less efficient with the 14.5Fr catheter (A) compared to the 19Fr Bicaval Dual Lumen Catheter (B). (DOC 114 KB)
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Karagiannidis, C., Kampe, K.A., Sipmann, F.S. et al. Veno-venous extracorporeal CO2 removal for the treatment of severe respiratory acidosis: pathophysiological and technical considerations. Crit Care 18, R124 (2014). https://doi.org/10.1186/cc13928
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/cc13928