
Abstract
Objective
Childhood is a critical period for brain development. However, it remains unknown whether the behaviors in a typical 24-h day are related to children’s executive function (EF). This study aimed to investigate the relationship between the 24-h movement guidelines and children’s EF.
Method
Children aged 7–12 years (n = 376) were studied in 2017 in China. Physical activity (PA) was accelerometer-derived, while screen time (ST) and sleep duration were self-reported. Meeting the 24-h movement guidelines was defined as: 1) ≥ 60 min/day of moderate-to-vigorous PA; 2) ≤ 2 h/day of recreational ST; 3) 9–11 h/night of sleep. EF was assessed by the Wisconsin Card Sorting Test (WCST). Number of completed categories (CC), shifting efficiency (SE), non-perseverative errors (NPE), and failure to maintain set (FMS) were used to measure four processes of EF, respectively represented global performance, cognitive flexibility, efficiency in rule discovery, and sustained attention. Generalized linear mixed models (GLMM) were completed to explore the associations of meeting the PA, ST, and sleep duration recommendations with four processes of EF.
Results
Statistically significant positive associations were observed between the number of guidelines met, regarded as a continuous variable, with CC [β = 0.343 (95% confidence interval [CI]: 0.125, 0.561)] and SE [β = 4.028 (95% CI: 0.328, 7.727)], while number of guidelines met negatively related to NPE [β = − 4.377 (95% CI:-7.952,-0.802)]. Participants not meeting the two recommendations for PA and sleep duration had lower scores in CC [β = -0.636(95% CI:-1.125,-0.147)] and SE [β = -10.610 (95% CI:-18.794,-2.425)] compared with those meeting the two, suggesting inferior global performance and worse efficiency in rule discovery. However, ST recommendation had no significant association with any processes of EF.
Conclusion
Meeting more recommendations of the 24-h movement guidelines was associated with superior EF in children. Specifically, more PA and healthy sleep duration should be encouraged to promote children’s EF.
Similar content being viewed by others
Background
Executive function (EF) is a multifaceted and multidimensional cognitive domain in which several underlying processes—such as planning, working memory, sustained attention, integration and feedback—coordinate together to perform both current and future goal-directed behaviors [1]. The Wisconsin Card Sorting Test (WCST) is regarded as “the gold standard of EF task” because of a highly sensitive indicator for cognitive flexibility, planning, and set maintenance [2]. Evidence suggests that EF early in life appears to be quite predictive of achievement and health throughout life [3]. For example, Moffitt et al. found that children who at ages 3 to 11 had better EF were more likely as teenagers to still be in school and were less likely to make risky choices in future, such as smoking, drugs use, etc. [3], which shows that the development of EF in childhood deserves more attention. A child’s EF development is affected by cultural and environmental factors including education, diet, environmental exposures, and daily movement behaviors [4, 5]. Among them, daily movement behaviors are considered to be important modifiable factors to promote children’s EF [4].
Achieving high levels of physical activity (PA), low levels of recreational screen time (ST), and enough sleep has been individually positively associated with children’s EF development [6,7,8]. Preadolescent children with higher PA tended to have better EF performance compared to their peers with less PA [6]. Excessive ST were reported independently related to weak inhibitory control, indicating that the more time children spent on screen, the worse their EF [7, 9]. In addition, sleep deprivation led to worse working memory, speed, and accuracy, and negatively affected the brain’s prefrontal cortex, leading to executive dysfunction [10]. However, the fact that PA, ST and sleep duration have been separately from each other is concerning, because research has shown that these three behaviors are codependent and should be considered simultaneously [11].
The 24-h movement guidelines represent a shift from focusing on certain individual movement types to the all-day behavior model. According to the latest data, only between 3 and 10% of children and adolescents from different countries around the world met all three recommendations [12,13,14]. Previous studies looking at the 24-h movement guidelines and health indicators mostly focused on examining associations between the combinations of PA, ST, and sleep duration with physical health outcomes [15,16,17]. To our knowledge, only 10 studies have reported the relationship between 24-h movement guidelines and mental health indicators, and one of the 10 had EF as an outcome variable [18, 19]. However, the above-mentioned study [19] conducted among children aged 9–10 years evaluated EF by using scales instead of the WCST, and it did not consider adjustment for Intelligence Quotient (IQ), which is recognized as a factor closely related to EF and might play a role in the association between the 24-h movement guidelines and EF [20]. In conclusion, little is known about the extent of the gaps in the current literature regarding the 24-h movement guidelines in relation to children’s EF. It is also unclear whether some combinations of PA, ST and sleep duration are more strongly associated with EF.
To address the pending evidence gaps, we examined if meeting the 24-h movement guidelines relate to EF while adjusting for IQ. It was hypothesized that children meeting all three recommendations of the 24-h movement behaviors would have superior EF compared to those who meeting two, one, or none of the recommendations.
Methods
Study design and participants
This study was conducted in 2017 using data from a school-based prospective cohort study’s baseline examination (Registration number: NCT03582709). The study complied with Declaration of Helsinki and was approved by the Ethics and Human Subject Committee of Sun Yat-sen University. Design of this study has been described elsewhere [21]. Briefly, we performed a two-stage cluster sampling strategy to recruit participants. First, we randomly selected five districts including three urban areas (Yuexiu District, Tianhe District, Liwan District) and two suburban areas (Panyu District, Huangpu District) in Guangzhou, a city located in southern China. Second, we randomly selected one primary school within every district. A brief meeting was arranged for school teachers to facilitate the implementation of this project. Informed consent for the study was distributed to each child. Children were advised to discuss with their parents and returned the parents’ signed informed consent to the school if they and their parents were willing to participant. Subsequently, 637 students of five schools with written informed consent were enrolled in this study.
Summary of all the measurements
The 24-h movement guidelines, as exposure variable were synthesized by PA, ST and sleep duration. PA was objectively measured by ActiGraph GT3X accelerometer, ST and sleep duration were collected by questionnaires with good reliability and validity [22]. We assessed EF using the WCST, which is often used to assess EF performance in children [23].
Exposures
Physical activity
PA was measured using ActiGraph GT3X accelerometer (ActiGraph, Pensacola, Florida, USA), one of the most commonly used activity monitors in children [24]. Accelerometers were attached to an elastic belt and worn above the iliac crest on the right side. Meanwhile, children were asked to fill in a PA log with the help of their parents, providing detailed information of PA and sedentary behaviors corresponding to the accelerometer records. All children were instructed to wear the devices during waking hours for 7 consecutive days, except during water-based activities (swimming and bathing). Sampled at 30 Hz, data were collected starting at 6:00 am, and ended at 11:59 pm using the unit of counts per minute (cpm). The accelerometer data files were reintegrated to 30-s epochs for its good sensitivity to detect child's activities, and non-wear periods were identified (and excluded from further analysis) by scanning the data array for periods of at least 60 min of consecutive zeros (allowing for 2 min of non-zero interruptions) [24]. We limited our analyses to participants who wore the device for ≥ 10 h/day for ≥ 4 days (including 3 weekdays and 1 weekend) according to the software (ActiLife V.6.13.3). Prediction equations were used to identify cut-points for classifying activity into sedentary time (< 100 cpm), light-intensity (100-2295 cpm), moderate-intensity (2296-4011 cpm) and vigorous-intensity (≥ 4012 cpm) PA [25]. Moderate-to-vigorous-intensity PA was calculated as the sum of moderate-intensity and vigorous-intensity PA. Total wear time was recorded and averaged per day.
Screen time and sleep duration
Under the assistance of the parent, children were asked to report the average amount of time (h and min) spent daily on various recreational screen-based activities (e.g., watching television or videos, playing video games, using the computer) in the past 7 days. Children’s bedtimes, waketimes, sleep latency, and nap duration over the previous week were recorded separately for weekdays and weekends. Sleep latency was measured by asking “how long it usually takes you to fall asleep after you go to bed?” The sleep duration was calculated as follows: sleep duration (hours) = (waketimes − bedtimes) − sleep latency; weekly sleep duration (hours) = [5 × (weekday sleep duration) + 2 × (weekend sleep duration)]/7. Questionnaires, used to collect ST and sleep duration, have been proven to have a good internal consistency with the coefficient was 0.80 and 0.74 and test–retest reliability with the coefficient was 0.59 and 0.63 in ST and sleep duration, respectively [22].
24-h movement guidelines
Children who reported moderate-to-vigorous-intensity PA ≥ 60 min/day, accumulating ≤ 2 h of daily recreational ST, and sleeping 9–11 h/night were considered to be meeting all three recommendations of the 24-h movement behaviors [26].
Outcomes
Executive function (WCST)
The WCST represents a widely used neuropsychological test for EF assessment [27]. We used 128-cards WCST’s computerized version to examine children’s EF. Participants were asked to sort cards according to one of the three rules (color, shape and number) by mouse clicking [27]. Four WCST indices were used for analysis: number of completed categories (CC), shifting efficiency (SE), non-perseverative errors (NPE), and failure to maintain set (FMS) [28, 29]. CC was the number of sets of 10 consecutive correct responses. NPE comprised all errors except perseverative errors. FMS was the number of incorrect responses after 2–9 consecutive correct responses. SE was calculated as proposed by [29]: SE score = CC*6 + [128 − (the number of cards used)]. This scoring method takes efficiency in achieving CC into account by rewarding unused cards, which helps to detect differences in task performance. The CC measure gives a global performance score, and higher CC score indicates superior global performance. Higher SE score suggests better cognitive flexibility. Lower NPE and FMS score are related to higher efficiency in rule discovery and less difficulty in sustained attention.
Covariates
Children’s birth date, sex, paternal and maternal educational level, and household monthly income were collected by questionnaires filled out by the parents. Height and weight were measured by research assistants. Body mass index (BMI) was calculated by dividing body weight (kg) by height squared (m2). Children’s IQ was initially assessed using the Combined Raven’s Test (second edition). With the advantages of non-verbal and less affected by language and ethnic differences, this test has widely used in China, especially for school-aged children [30]. Through the group test, every child received a booklet and a sheet of answer paper in the quiet classrooms. Under trained research assistants’ guidance, participants had 40 min to complete this test.
Statistical analyses
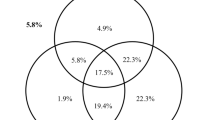
The participants’ descriptive statistics were used to characterize the study population. Mean ± standard deviation (SD) and sample number (percentage) were presented for continuous and categorical variables, respectively. T-tests and chi-squared tests or Kruskal–Wallis tests were used to compare sex differences among continuous and categorical variables. Descriptive statistics for the proportion of participants meeting different combinations of recommendations are presented in Fig. 2.
Analysis of covariance (ANCOVA) was conducted to examine group differences in meeting different number of guidelines with the WCST’s four indices (CC, SE, NPE, FMS). A trend analysis was completed to examine whether there was a gradient of meeting more recommendations with higher or lower scores among EF’s four processes. Generalized linear mixed models (GLMM) were completed to explore the associations of meeting or not meeting different combinations of recommendations with WCST’s indices (CC, SE, NPE, and FMS) after controlling for sex, age, paternal/maternal educational level, household monthly income, BMI, and IQ. Schools were fitted as random effects in models. The results were reported with unstandardized path coefficients (β), and 95% confidence interval (CI). All analyses were conducted using SPSS 21.0 (IBM, Armonk, NY, USA). We defined statistical significance as P < 0.05 for a two-tailed test.
Results
Participants characteristics and adherence to movement behavior recommendations
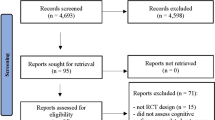
A total of 637 children were enrolled in this study, and 376 of them had valid data and were included in the analyses. Flow diagram of participants selection was showed in Fig. 1. Participants’ demographics and characteristics stratified by sex are summarized in Table 1. Three hundred seventy-six children (195 boys [51.9%] and 181 girls [48.1%]; mean [SD] age, 9.17 [1.61] years) completed the questionnaire information and effective wearing of accelerometer to assess PA, and the WCST. Sample’s average time of moderate-to-vigorous-intensity PA was 42.05 ± 16.79 min/day, and boys did more moderate-to-vigorous-intensity PA than girls per day (49.05 ± 16.22 vs. 34.51 ± 13.92, P < 0.001). On average (mean ± SD), participants reported spending 0.99 ± 1.12 h/day on ST and 9.35 ± 0.71 h/night on sleep. Overall, 15.7%, 82.4%, and 72.1% of participants met the PA, ST, and sleep duration recommendations, respectively (Fig. 2). Only approximately 10% of participants met all three guidelines. (Table 1 and Fig. 2). We also analyzed differences in demographic characteristics of the analyzed subjects and sampling populations. There were no statistically significant differences between the two groups in age, sex, paternal and maternal educational level, household monthly income, BMI, and IQ (P > 0.05), indicating that the included samples were representative of the total sample (Table S1).

Flow diagram of participant selection and assignment

Venn diagram showing the proportion (%) of participants meeting no guidelines, physical activity, screen time, and sleep duration recommendations, and combinations of these recommendations in the full study sample (N = 376)
Associations between meeting the 24-h movement guidelines and executive function
ANCOVAs showed that children meeting more recommendations had higher CC and SE scores and lower NPE scores, indicating superior global performance, better cognitive flexibility, and greater efficiency in rule discovery, respectively (P for trend <0.05). We also compared sex differences in WCST performance across the four groups, and found that the above statistically significant relationship was only observed in boys, but not in girls. However, this trend did not appear in patterns of recommendations and FMS score for both boys and girls (Table 2).
We further performed GLMM to explore the associations between patterns of meeting various movement behavior recommendations and the WCST’s four indices (Table 3). Statistically significant positive associations were observed the number of guidelines met, regarded as a continuous variable, with CC [β = 0.343 (95% confidence interval [CI]: 0.125, 0.561)] and SE [β = 4.028 (95% CI: 0.328, 7.727)], while number of guidelines met negatively related to NPE [β = − 4.377(95% CI:-7.952,-0.802)]. Not meeting any recommendations was associated with significantly lower CC score, lower SE score, and higher NPE score than meeting all three recommendations as a categorical variable, respectively implied inferior global performance, worse cognitive flexibility, and lower efficiency in rule discovery (P < 0.05).
Children not meeting the PA recommendation had a significantly lower CC score [β = − 0.497 (95% CI: − 0.939, − 0.055)] than those meeting them. Moreover, not meeting sleep duration recommendations had detectable associations with inferior global performance score and worse efficiency in rule discovery than meeting sleep duration recommendations (P < 0.05). No significant associations were found between ST recommendation and WCST’s indices. For specific combinations of recommendations, there were significantly lower CC scores in children who did not meet PA + ST [β = − 0.643 (95% CI: − 1.101, − 0.185)], or PA + sleep duration [β = − 0.636 (95% CI: − 1.125, − 0.147)], or ST + sleep duration [β = − 0.411 (95% CI: − 0.741, − 0.080)] than in children meeting those patterns of the above recommendations. A similar association was observed between meeting recommendations of PA + sleep duration and SE score. Compared with those who met the ST + sleep duration recommendations, participants not meeting those two recommendations had worse efficiency in rule discovery [β = 6.198 (95% CI: 0.814,11.582)]. No significant association was observed between any individual or concurrent recommendations and FMS score (P > 0.05).
Discussion
To the best of our knowledge, this is the first study to examine the association of 24-h movement guidelines with EF adjusting the analysis for IQ among children aged 6–12 years. The main finding was that children meeting more 24-h movement guidelines’ recommendations had superior EF regarding global performance, cognitive flexibility, and efficiency in rule discovery. Particularly, this pattern was evident for individual and concurrent associations of PA and sleep duration with children’s EF.
Across CC, SE, and NPE, we found that meeting fewer recommendations was associated with worse global performance, cognitive flexibility, and efficiency in rule discovery in a gradient pattern. Consistent with this study’s findings, Walsh et al. [19] observed that children aged 9–10 years who met fewer 24-h movement guidelines’ recommendations had lower global cognition scores using by scale. Similarly, using a parent-reported Child Behavior Checklist, one Canadian study reported that meeting more recommendations of the 24-h movement guidelines was associated with fewer behavioral and emotional problems at 3 years [31]. Another study also reported that meeting none, one, and two recommendations was related to higher difficulties score compared to meeting all three recommendations [32]. Here, further results from GLMM suggested associations between three of the WCST’s indices (CC, SE, and NPE) and patterns of meeting various movement behavior recommendations after adjusting for sex, age, paternal and maternal educational level, household monthly income, BMI, and even IQ. Moreover, we found sex differences in the relationship between 24-h movement guidelines and children's EF, possibly due to the fact that boys participated in MVPA more time than girls in this study.
In particular, evident individual and combined associations of PA and sleep duration with children’s EF were found. Meeting the PA recommendation (alone or in combination with meeting the sleep duration recommendation) was positively related to CC and/or SE scores, indicating better global performance and/or cognitive flexibility. A recent well-documented meta-analysis also provided evidence of PA’s positive effects on EF, attention, and academic performance children (aged 6–12 years) [6]. Additionally, emerging evidence shows that a single exercise and regular participation in PA benefit EF, including memory, attention, and inhibition [33]. The mechanisms that benefit from PA may include increased cerebral blood flow and metabolism, enhanced functional coupling between the brain networks and the provision of neurotrophins, and better neurotransmitter regulation [34].
Another important finding was that participants not meeting sleep duration recommendation had statistically detectable associations with inferior global performance and efficiency in rule discovery compared to those meeting sleep duration recommendation. These results further support Short, et al.’s study, which showed that sleep plays an important role in brain development and plasticity, and greater sleep quality and quantity were positively associated with cognition in children [35]. Sleep deprivation can result in impairments in the brain structure among children, and further lead to executive dysfunction [10]. Thus, our results are consistent with an increasing body of literature suggesting that meeting the sleep duration recommendation (alone or in combination with meeting the PA or ST recommendations) was favorably associated with some indices of WCST. A randomized controlled trial confirmed that increased PA can improve sleep and mood outcomes [36]. Furthermore, one cross-sectional study also reported that youth who regularly meet sleep duration guideline are more physically active [37]. These results converge with those of our study. Our findings highlight that meeting the recommendations of PA and sleep duration can provide unique benefits to CC and SE compared with not meeting the two.
Interestingly, we found that not meeting the ST recommendation was not significantly associated with any indices of the WCST compared to meeting ST recommendation, consistent with previous studies’ finding [38, 39]. Previous studies showed that the associations between ST and mental health outcomes were very small [38, 39]. On the other hand, in the 2016 PAFCTYS, 63.2% of Chinese children aged 9–17 met the ST recommendation [40], which is far lower than 82.4% in this study. This difference in proportion, in addition to different age composition of samples, also suggested that the level of ST may be underestimated in our study because of not including all types of ST, such as the time spent using mobile phones and iPads, which is also a possible reason for the insignificant relationship between ST and children’s EF in present study.
However, the association between ST and mental health has been controversial. Temperate engagement in ST may not lead to behavioral or emotional problems. For instance, previous research found that ≤ 2 h/day of ST was linked to superior global cognition [19]. In contrast, frequent use of video games was related to conduct problems, and increased television viewing was negatively associated with children’s cognitive development [41]. Growing evidence suggests that screen use may differentially impact EF resulting from screen type, content, and task requirements [7]. Results of an interventional study showed that children were more likely to delay gratification after playing an educational app than after viewing a cartoon, and children’s working memory also improved after playing the educational app [42]. One study even pointed out that the adverse effects of ST on EF may due to the occupation or replacement of other activities (such as PA, reading, etc.) that were beneficial to the development of children's EF [43]. Here, ST + PA or ST + sleep duration, rather than individual ST, had statistical correlation with WCST’s certain indices. We speculate that the concurrent associations of ST + PA or ST + sleep duration with children’s EF were mainly driven by PA or sleep duration. Therefore, understanding the multiple dimensions of screen use and its place in modern life may be critical to envision the role of screen use in children.
This study’s key strengths are PA’s objective measurement, and the EF assessment using WCST. Additionally, models were adjusted for several key potential confounders, including IQ and BMI. Although IQ has been proven to be an important factor closely related to children’s EF [20], few studies have considered it as a confounding factor. However, our study’s limitations need to be noted. First, our results are based on cross-sectional data, which do not allow for tracking the durability and consistency of movement behavior adherence over time, precluding any causal inferences, prospective cohort study or randomized controlled study in the future would be need to establish that causality inference. Second, self-reported exposures on ST and sleep duration, even though they were collected from questionnaires with good reliability and validity [22], make our study susceptible to recall and social desirability biases. Third, assessment of ST in this study is not comprehensive, such as excluding time spent on mobile electronic devices, and future research should take them and other newly emerging electric devices into account. Forth, though we did a sensitivity analysis for missing samples, a large proportion of missing data may still affect the results to some extent. Fifth, small sample size of some groups may limit the power to detect associations, which is also an important reason for limiting our analysis of subgroups by sex.
Conclusions
Meeting more 24-h movement guidelines’ recommendations was associated with superior EF performance in children. As only 10.1% of the sample met all three recommendations, these guidelines’ adoption should be promoted. Additionally, future work should further explore longitudinal data to more concretely decipher these associations’ temporality and intensity.
Availability of data and materials
The data that support the findings of this study are available on request from the corresponding author. The data used during the current study is not publicly available due to privacy or ethical restrictions.
Abbreviations
- EF:
-
Executive function
- PA:
-
Physical activity
- ST:
-
Screen time
- WCST:
-
The Wisconsin Card Sorting Test
- IQ:
-
Intelligence quotient
- CC:
-
Completed categories
- SE:
-
Shifting efficiency
- NPE:
-
Non-perseverative errors
- FMS:
-
Failure to maintain set
- BMI:
-
Body mass index
- SD:
-
Standard deviation
- ANCOVA:
-
Analysis of covariance
- CI:
-
Confidence interval
References
Diamond A. Executive Functions. Annu Rev Psychol. 2013;64:135–68.
Westwood H, Stahl D, Mandy W, Tchanturia K. The set-shifting profiles of anorexia nervosa and autism spectrum disorder using the Wisconsin Card Sorting Test: a systematic review and meta-analysis. Psychol Med. 2016;46(9):1809–27.
Moffitt TE, Arseneault L, Belsky D, Dickson N, Hancox RJ, Harrington H, et al. A gradient of childhood self-control predicts health, wealth, and public safety. Proc Natl Acad Sci. 2011;108:2693–8. https://doi.org/10.1073/pnas.1010076108.
Zelazo, PD, and Carlson, SM. Hot and Cool Executive Function in Childhood and Adolescence Development and Plasticity. Child Dev Perspect. doi:https://doi.org/10.1111/j.1750-8606.2012.00246.x.
Lindenberger U. Lifespan Theories of Cognitive Development. Int Encycl Soc Behav Sci. 2001;8848–54. https://doi.org/10.1016/b0-08-043076-7/01572-2.
De Greeff JW, Bosker RJ, Oosterlaan J, Visscher C, Hartman E. Effects of physical activity on executive functions, attention and academic performance in preadolescent children: a meta-analysis. J Sci Med Sport. 2018;21(5):501–7.
Anderson DR, Subrahmanyam K. Digital Screen Media and Cognitive Development. Pediatrics. 2017;140(Suppl 2):S57–61.
Reynolds CM, Short MA, Gradisar M. Sleep spindles and cognitive performance across adolescence: A meta-analytic review. J Adolescence. 2018;66:55–70.
Uncapher MR, Lin L, Rosen LD, Kirkorian HL, Baron NS, Bailey K, et al. Media Multitasking and Cognitive, Psychological, Neural, and Learning Differences. Pediatrics. 2017;140(Suppl 2):S62–6.
Maski KP, Kothare SV. Sleep deprivation and neurobehavioral functioning in children. Int J Psychophysiol. 2013;89:259–64. https://doi.org/10.1016/j.ijpsycho.2013.06.019.
Feng J, Zheng C, Sit CH, Reilly JJ, Huang WY. Associations between meeting 24-hour movement guidelines and health in the early years: A systematic review and meta-analysis. J Sports Sci. 2021;39(22):2545–57.
Knell G, Durand CP, Kohl HW 3rd, Wu IHC, Pettee GK. Prevalence and likelihood of meeting sleep, physical activity, and screen-time guidelines among US youth. JAMA Pediatr. 2019;173(4):387–9.
Pearson N, Sherar LB, Hamer M. Prevalence and correlates of meeting sleep, screen-time, and physical activity guidelines among adolescents in the United Kingdom. JAMA Pediatr. 2019;173(10):993–4.
Roman-Vinas B, Chaput JP, Katzmarzyk PT, Fogelholm M, Lambert EV, Maher C, et al. Proportion of children meeting recommendations for 24-hour movement guidelines and associations with adiposity in a 12-country study. Int J Behav Nutr Phys Act. 2016;13(1):123 Epub 2016/11/27.
Poitras VJ, Gray CE, Borghese MM, Carson V, Chaput J-P, Janssen I, et al. Systematic review of the relationships between objectively measured physical activity and health indicators in school-aged children and youth. Appl Physiol Nutr Metab. 2016;41(6):S197–239.
Chaput JP, Gray CE, Poitras VJ, Carson V, Gruber R, Olds T, et al. Systematic review of the relationships between sleep duration and health indicators in school-aged children and youth. Appl Physiol Nutr Metab. 2016;41(6 Suppl 3):S266–82.
Carson V, Hunter S, Kuzik N, Gray CE, Poitras VJ, Chaput J-P, et al. Systematic review of sedentary behaviour and health indicators in school-aged children and youth: an update. Appl Physiol Nutr Metab. 2016;41(6):S240–65.
Sampasa-Kanyinga H, Colman I, Goldfield GS, Janssen I, Wang J, Podinic I, et al. Combinations of physical activity, sedentary time, and sleep duration and their associations with depressive symptoms and other mental health problems in children and adolescents: a systematic review. Int J Behav Nutr Phys Act. 2020;17(1):72.
Walsh JJ, Barnes JD, Cameron JD, Goldfield GS, Chaput JP, Gunnell KE, et al. Associations between 24-hour movement behaviours and global cognition in US children: a cross-sectional observational study. Lancet Child Adoles Health. 2018;2:783–91.
Gray S, Green S, Alt M, Hogan TP, Kuo T, Brinkley S, et al. The Structure of Working Memory in Young Children and Its Relation to Intelligence. J Mem Lang. 2017;92:183–201.
Lv Y, Cai L, Gui Z, Zeng X, Tan M, Wan N, et al. Effects of physical activity and sedentary behaviour on cardiometabolic risk factors and cognitive function in children: protocol for a cohort study. BMJ Open. 2019;9: e30322.
Yajie L, Lijuan L, Danling L, Li L, Yanna Z, Chenyang F, et al. Study on the reliability and validity of physical health surveillance system questionnaire for primary school students in Guangzhou. Mat Child Health Care China. 2020;35:1511–6 (Article in Chinese).
Dai M, Lin L, Liang J, Wang Z, Jing J. Gender Difference in the Association Between Executive Function and Autistic Traits in Typically Developing Children. J Autism Dev Disord. 2019;49(3):1182–92.
Troiano RP, Berrigan D, Dodd KW, Mâsse LC, Tilert T, McDowell M. Physical Activity in the United States Measured by Accelerometer. Med Sci Sports Exerc. 2008;40:181–8.
Evenson KR, Catellier DJ, Gill K, Ondrak KS, McMurray RG. Calibration of two objective measures of physical activity for children. J Sports Sci. 2008;26(14):1557–65.
Tremblay MS, Carson V, Chaput JP. Introduction to the Canadian 24-Hour Movement Guidelines for Children and Youth: An Integration of Physical Activity, Sedentary Behaviour, and Sleep. Appl Physiol Nutr Metab. 2016;41:iii–iv.
Mitrushina M, Boone KB, Razani JD, Elia LF. Handbook of Normative Data for Neuropsychological Assessment. 2nd ed. New York, NY, USA: Oxford University Press; 2005.
Sherman E, Tan J, Hrabok M. A Compendium of Neuropsychological Tests. Fundamentals of Neuropsychological Assessment and Test Reviews for Clinical Practice. 4th ed. Oxford, MS, USA: Oxford University Press; 2020.
Cianchetti C, Corona S, Foscoliano M, Scalas F, Sannio-Fancello G. Modified Wisconsin Card Sorting Test: proposal of a supplementary scoring method. Arch Clin Neuropsychol. 2005;20(4):555–8.
Yu X, Chen J, Li Y, Liu H, Hou C, Zeng Q, et al. Threshold effects of moderately excessive fluoride exposure on children’s health: A potential association between dental fluorosis and loss of excellent intelligence. Environ Int. 2018;118:116–24.
Carson V, Ezeugwu VE, Tamana SK, Chikuma J, Lefebvre DL, Azad MB, et al. Associations between meeting the Canadian 24-Hour Movement Guidelines for the Early Years and behavioral and emotional problems among 3-year-olds. J Sci Med Sport. 2019;22(7):797–802.
Carson V, Chaput JP, Janssen I, Tremblay MS. Health associations with meeting new 24-hour movement guidelines for Canadian children and youth. Prev Med. 2017;95:7–13.
Donnelly JE, Hillman CH, Castelli D, Etnier JL, Lee S, Tomporowski P, et al. Physical Activity, Fitness, Cognitive Function, and Academic Achievement in Children. Med Sci Sports Exerc. 2016;48(6):1197–222.
Hillman CH, Erickson KI, Kramer AF. Be smart, exercise your heart exercise effects on brain and cognition. Nat Rev Neurosci. 2008;9:58–65.
Short MA, Blunden S, Rigney G, Matricciani L, Coussens S, M Reynolds C, et al. Cognition and objectively measured sleep duration in children: a systematic review and meta-analysis. Sleep Health. 2018;4(3):292–300.
Hartescu I, Morgan K, Stevinson CD. Increased physical activity improves sleep and mood outcomes in inactive people with insomnia: a randomized controlled trial. J Sleep Res. 2015;24(5):526–34.
Kim Y, Umeda M, Lochbaum M, Stegemeier S. Physical Activity, Screen-Based Sedentary Behavior, and Sleep Duration in Adolescents: Youth Risk Behavior Survey, 2011–2013. Prev Chronic Dis. 2016;13:E131.
Orben A, Przybylski AK. The association between adolescent well-being and digital technology use. Nat Hum Behav. 2019;3(2):173–82.
Ferguson CJ. Everything in Moderation: Moderate Use of Screens Unassociated with Child Behavior Problems. Psychiatr Q. 2017;88:797–805.
Cai Y, Zhu X, Wu X. Overweight, obesity, and screen-time viewing among Chinese school-aged children: National prevalence estimates from the 2016 Physical Activity and Fitness in China-The Youth Study. J Sport Health Sci. 2017;6(4):404–9.
Takeuchi H, Taki Y, Hashizume H, Asano K, Asano M, Sassa Y, et al. The Impact of Television Viewing on Brain Structures: Cross-Sectional and Longitudinal Analyses. Cereb Cortex. 2015;25(5):1188–97.
Huber B, Yeates M, Meyer D, Fleckhammer L, Kaufman J. The effects of screen media content on young children’s executive functioning. J Exp Child Psychol. 2018;170:72–85.
Scarf D, Hinten AE. Television Format and Children’s Executive Function. Pediatrics. 2018;141(3): e20172674.
Acknowledgements
The authors want to thank the students and their guardians for their participation in the survey and the postgraduates for conducting the questionnaire survey and inputting the data.
Funding
This work was supported by National Natural Science Foundation of China (Grant No.81673193) and Guangdong Provincial Engineering Research Center of Public Health Detection and Assessment, Guangdong Pharmaceutical University, Guangzhou, China.
Author information
Authors and Affiliations
Contributions
YC and WY designed the experiments. XZ and WT carried out the experiments. XZ performed the statistical analysis and drafted the manuscript. LC and WH critically revised the manuscript. YC provided suggestions in the statistical analysis and revised manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Ethics and Human Subject Committee of Sun Yat-sen University and complied with Declaration of Helsinki. All the children and their parents voluntarily participated in this study with the parent’s signed informed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no conflicts of interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Table S1.
Demographic characteristics of the analyzed subjects and sampling populations. Table S2. Performance of WCST with or without meeting recommendations for PA, ST, and sleep duration. Table S3. Associations between meeting the physical activity, screen time, and sleep duration recommendations and four dimensions of WCST in boys.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zeng, X., Cai, L., Yang, W. et al. Association between the 24-hour movement guidelines and executive function among Chinese children. BMC Public Health 22, 1017 (2022). https://doi.org/10.1186/s12889-022-13420-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-022-13420-5