
Abstract
Background
Menopause is an inevitable stage affecting every middle-aged woman. China has a large and increasing group of post-menopausal women. Most post-menopausal women suffer from increased risks for cardiovascular diseases (CVD) and sleep problems. Previous studies have demonstrated the associations between sleep disorders and increased CVD risks in general population. The current study is to examine the relationship between sleep quality and CVD risks among Chinese post-menopausal women.
Methods
This study was a sub-study nested in a cross-sectional study that investigated the sleep quality of community-dwelling adults in Xian, Shaanxi Province, China. The Chinese version of the Pittsburgh Sleep Quality Index (PSQI) and the Framingham 10-year risk score (FRS) were used to measure sleep quality and CVD risk among 154 Chinese post-menopausal women. Multivariate regression and logistic regression were used to determine the association between sleep quality and CVD risk.
Results
The participants (age: 63.65 ± 4.47 years) experienced poor sleep quality (mean score of global PSQI = 8.58) and a 10-year risk of CVD of 12.54%. The CVD risk was significantly associated with sleep duration (β = − 0.18, p = 0.04) and sleep disturbance (β = 0.33, p < 0.001). Women with good sleep quality (PSQI ≤5) were less likely to be at high risk for CVD (FRS > 10%) (odds ratio = 0.51, p = 0.04).
Conclusions
Poor sleep quality might increase the CVD risk in post-menopausal women. Interventions to promote the cardiovascular health of Chinese post-menopausal women may need to include sleep promotion strategies.
Similar content being viewed by others


Background
Menopause is a natural and an inevitable stage leading to old age that affects every middle-aged woman. Every day, about 6000 American women reach menopause [1]. In China, 120 million women, accounting for around 23% of the world’s menopausal population, are experiencing the transition to menopause [2]. With the ageing population and rise in life expectancy worldwide, the stages of menopause and post-menopause will account for about one third of women’s lives [1]. Moreover, the number of post-menopausal women is also expected to increase. It is estimated that there will be 1.1 billion post-menopausal women in the world by 2025 [1]. Therefore, the health of this large population group is of high importance to public health.
Menopause is often accompanied by an increased risk for cardiovascular diseases (CVD) and sleep problems [3,4,5]. During the normal physiological process of menopause, the reduction in ovarian follicular function often leads to the depletion of estrogen, contributing to the development of a series of cardio-metabolic risks. These risks include central obesity, reduced glucose tolerance, increased blood pressure, abnormal levels of plasma lipids, and vascular inflammation [6], and as a consequence, substantially increasing the CVD risk and mortality in this group of women [7]. The hormonal changes that occur during menopause have also been reported to be correlated with various sleep problems [8]. The common complaints among post-menopausal women include difficulty in sleep onset, short sleep duration, and poor sleep quality [9]. It was reported that around 53.3% to 65.8% of post-menopausal women suffered from sleeplessness during their menopausal transition [10].
Numerous studies have demonstrated the associations between sleep disorders and increased CVD risk in general population [11]. An increased risk for CVD and coronary heart disease (CHD) incidents was found in individuals who had short sleep duration (≤ 6 h) and poor sleep quality [11]. Furthermore, in those who had sleep-disordered breathing (e.g., apnea and hypopnea), the relative risk for heart failure and stroke was 2.38 and 1.58, respectively [12]. However, limited studies examined the relationship of these health-related aspects particularly among post-menopausal women, and even fewer studies were conducted among Chinese post-menopausal women, the largest population group of this type in the world.
Previous studies among general populations usually assessed sleep quality by a single item, such as “How often is your sleep satisfactory?”, “How many hours of sleep do you usually get?” or “How often do you experience insomnia?” [11]. Moreover, limited evidence was obtained from a comprehensive and validated assessment of sleep quality. Thus, the present study aimed to investigate sleep quality using a comprehensive and validated tool and to examine the relationship between sleep quality and the CVD risk among Chinese post-menopausal women.
Methods
Study design and participants
This study was a secondary data analysis of a cross-sectional study conducted in Xi’an, Shaanxi Province, China. The original cohort consisted of 404 community-dwelling adults, whose sleep quality and its associated factors were examined [13]. The present study focused on the data of 154 post-menopausal women from the original cohort to evaluate their sleep quality and CVD risk. Post-menopause was defined as amenorrhea not attributable to other causes for at least 12 months [14]. The eligibility of the participants was assessed by their self-reported menstrual history.
Measures
Data were collected by a structured questionnaire that included the Pittsburgh Sleep Quality Index (PSQI), items on cardiovascular parameters, and socio-demographic information. All questionnaires were administered by one researcher through face-to-face interviews.
Pittsburgh sleep quality index
Sleep quality was assessed by the Chinese-version of the PSQI (PSQI-C) [15]. The PSQI-C consists of 19 self-rated items related to sleep quality in the past month, of which seven component scores are summed to give a global score. The seven components include subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleep medication, and daytime dysfunction. Each component score ranges from 0 to 3, and a score > 1 indicates problems in that aspect of sleep quality. The global score of sleep quality ranges from 0 to 21 with a higher score indicating poorer quality of sleep, whereas a cutoff score of ≤5 indicates good sleep quality [16]. The original PSQI had received extensive support to confirm its good psychometric properties and high correlation with actual sleep log data [17, 18]. Good reliability of the PSQI-C was also demonstrated among 793 Chinese adults, with a Cronbach’s alpha = 0.84 and a 2-week test-retest reliability of 0.81 [15].
Ten-year risk of CVD
Anthropometric measurements
Anthropometric measurements were administered in the same manner for all participants. Body weight and height were measured without shoes. Body mass index (BMI) was calculated as weight divided by the square of height (kg/m2). Systolic blood pressure (SBP) and diastolic blood pressure (DBP) were measured by a mercury sphygmomanometer after at least 15 min of rest.
Framingham 10-year risk score
The CVD risk in the participants was estimated by the office-based prediction model of the Framingham 10-year risk score (FRS) [19]. The predictors of the model include age, BMI, SBP, use of antihypertensive medication, medical history of diabetes, and current smoking status. This model revealed good performance in model discrimination and calibration, with a discrimination statistic of 0.785 [95% confidence interval (CI), 0.764–0.806] and a calibration Chi-square of 10.24 [19]. The sensitivity and specificity of this model for CVD events in follow-up studies were 0.58 and 0.83, respectively [19]. According to the American Heart Association guidelines for women’ health, a FRS ≥ 10% is regarded as being at high risk for CVD [7].
Socio-demographic variables included age, marital status, education level, employment status, medical history, and drinking and smoking status, which were collected based on self-report information. The participants’ physical exercise habit was evaluated by a single item: “How often do you do physical exercise?” A frequency of three times per week or above was regarded as a regular physical exercise habit [7].
Statistical analysis
Descriptive statistics were used to describe the socio-demographic characteristics, cardiovascular parameters, and sleep quality of the participants. The normality of each continuous variable was tested through skewness and kurtosis statistics.
Multivariate regression and logistic regression were used to determine the association between sleep quality, socio-demographic variables, and CVD risk. To identify potential predicting variables encoded in the regression models, bivariate analyses between participants’ characteristics, sleep quality and FRS were conducted through independent t-test and Pearson correlation analyses as appropriate. As the FRS was calculated based on variables of age, gender, BMI, SBP, and smoking status [19], those variables were not examined in the bivariate analyses. A liberal significance level of 0.2 was applied to identify potential predictors, which would reduce the probability of excluding important variables from the model [20]. To reduce over-parameterization of the model, potential predictors with high co-variability (r > 0.7) and lowest correlation coefficient with the outcome variables were excluded from the model [20]. The two-sided level of significance was set at 0.05. Statistical analysis was performed by the IBM SPSS version 21.0 [21].
Results
This study comprised of 154 Chinese post-menopausal women with a mean age of 63.65 (standard deviation, SD = 4.47) years. Table 1 summarizes the socio-demographic characteristics and cardiovascular parameters of the post-menopausal women. A majority of participants were married (81.8%) and had an education level of secondary or above (78.5%). For those who were still in employment (10.4%), most were employed as manual labourers, which required a high level of physically activity. The majority of the women (72.1%) had regular physical exercise. Hypertension was the most prevalent chronic illness (66, 43%), followed by diabetes (13%) and hypercholesterolemia (4%). Among those with hypertension, only 25 (37.9%) were taking antihypertensive medications. Only 1.3% of the participants were current smokers and 5.1% were drinkers. Their mean BMI was 24.41 (SD = 3.64) kg/m2, and 67.6% of the women were overweight or obese. The mean values for SBP and DBP were 126.20 (SD = 15.10) and 78.41 (SD = 7.92) mmHg, respectively. The participants had a mean 10-year risk of CVD of 12.54%, and half of them (51.3%) were at high risk for CVD (FRS ≥ 10%) [22, 23].
Findings from the PSQI showed that the sleep duration of the participants ranged from 1 to 9 (mean = 6.09, SD = 1.52) hours, with 25.0% of the women having less than 5 h sleep. Time spent in bed ranged from 5 to 13 (mean = 7.77, SD = 1.11) hours. The mean sleep efficiency, calculated by actual sleep duration / time spent in bed, was 78.35% (range: 7.69–100%). Table 2 presents the participants’ sleep quality, with regard to the seven component scores and the global score of PSQI. The global PSQI score was 8.58 ± 4.37. Six components, except for use of sleep medication, were scored >1. The component of sleep latency had the highest score (2.32), followed by sleep disturbance (1.51) and subjective sleep quality (1.26). Of the 154 participants, 136 (88.3%) reported “had to get up to use the bathroom” at least once per week as the most common cause of sleep disturbance, followed by “cannot get to sleep within 30 minutes” (n = 110, 71.4%), and “waking up in the middle of the night or early morning” (n = 97, 63.0%).
In the multivariate regression, the FRS was analyzed as the dependent variable. Bi-variate analyses were conducted to identify potential predicting variables of CVD risks. As presented in Table 3, five variables with a significance level < 0.2 in the bi-variate analyses with FRS, including subjective sleep quality (r = 0.138, p = 0.087), sleep duration (r = 0.106, p = 0.191), sleep disturbance (r = 0.264, p = 0.001), global PSQI score (r = 0.124, p = 0.126), and employment status (t = 6.414, p = 0.012). Given that global PSQI score was calculated based on all the seven component scores [15], to better understand the influences of specific sleep quality components on CVD risks, the variables of subjective sleep quality, sleep duration, and sleep disturbance, together with employment status were included as independent variables in the regression model. Moreover, physical exercise habit was also adjusted in the regression model, for its significant influence on CVD risk observed in the previous study [11]. The multivariate regression model (Table 4) identified three variables that influenced the CVD risk: employment status (p = 0.016), sleep duration (p = 0.04), and sleep disturbance (p < 0.001).
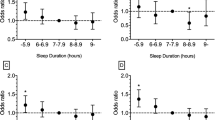
Logistic regression analysis was also conducted to explore the relationship between sleep quality and CVD risk. The dependent variable is CVD risk, including a high-risk group (FRS ≥ 10%) and a low-risk group (FRS < 10%) [22, 23]. As indicated in the bivariate analysis with CVD risk, five variables (subjective sleep quality, sleep duration, sleep disturbance, global PSQI score, and employment status) revealed p values less than 0.2. As the global PSQI score has considered the scores on subjective sleep quality, sleep duration, and sleep disturbance. The independent variables in the logistic regress model included employment status and the sleep quality (including a good sleep quality group with PSQI ≤5 and a poor sleep quality group with PSQI >5). Given the significant influence on CVD risk [11], physical exercise habit was also adjusted in the logistic regression model. The results demonstrated that women with good sleep quality were less likely to be at high risk for CVD, with an odds ratio (OR) of 0.51 (95% CI: 0.26–0.97, p = 0.04).
Discussion
The Chinese post-menopausal women had poor sleep quality and increased CVD risks. The current study also identified a significant relationship between sleep quality and CVD risk, which provided valuable clues for developing interventions to improve the sleep quality and to reduce the CVD risks in post-menopausal women.
The socio-demographic characteristics of the study sample were consistent with those in previous studies among Chinese post-menopausal women [24, 25]. The mean FRS in the study sample was 12.54%, indicating a high risk for CVD (> 10%) among the Chinese post-menopausal women. Previous studies have also reported an increased CVD risk among post-menopausal women, which may be related to the reduced protective effects of estrogen on cardiovascular health [8, 26].
The participants reported a poor sleep quality, with a mean global PSQI score of 8.58 (> 6). Their sleep quality was much poorer than that of other age groups of Chinese women in other studies [13, 24]. Particularly, poor sleep quality had been consistently reported in previous studies among post-menopausal women [10, 25]. These findings suggest that poor sleep quality is common among post-menopausal women in both western and Chinese populations.
On average, the participants spent 7.77 h in bed per night, but only had 6.09 h of sleep. The more than 1-h of awake in bed reflected a severe problem with sleep latency (mean score = 2.32) and may also have influenced their subjective perception of sleep quality [13]. Moreover, 71.4% of the participants reported “cannot get to sleep within 30 minutes” at least once per week. These findings are consistent with the high prevalence of insomnia reported in post-menopausal women in Asia [10, 24].
Most participants reported “have to get up to use bathroom,” “cannot get to sleep within 30 minutes,” and “waking up in the middle of the night or early morning.” as the most common causes of sleep disturbance. These sleep problems may be due to the aging changes of their urinary system, or to menopausal symptoms such as hot flashes and night sweats [13, 27]. Similar sleep problems were reported in the Wisconsin Sleep Cohort Study, in which post-menopausal women experienced more problems in initiating sleep (OR = 2.77) and repeated episodes of waking up (OR = 1.58) when compared with those of premenopausal women [27].
Sleep quality greatly affects the women’s quality of life and role functioning in work places and family [28]. The poor sleep quality observed among Chinese post-menopausal women indicates the urgent need for interventions to improve their sleep quality, and in particularly to address the long sleep latency and severe sleep disturbances.
The present study also identified that among the post-menopausal women, there was a significant relationship between the CVD risks and sleep quality, particularly in sleep duration and sleep disturbance. Women who slept longer (with a lower component score in sleep duration) were at higher risks for CVD. Previous studies reported a U-shaped relationship between sleep duration and health, suggesting that too little or too much sleep correlates with adverse health outcomes [29]. A meta-analysis of 15 prospective studies also reported that when compared to participants with normal sleep duration, those with longer sleep duration (> 8 h per night) had greater risks for total CVD incidents, CHD, and stroke [30]. The participants in the present study slept on average 6.09 h per night, and most (81.8%) had normal sleep duration with 5–8 h of sleep per night [30]. The present study added evidence that among the post-menopausal women with normal sleep duration, longer sleep duration was associated with higher CVD risks.
The participants who experienced more sleep disturbances had higher CVD risks. However, the relationship between sleep disturbance and CVD risk has received limited attention in previous studies. The sleep disturbances as measured by the PSQI included “cannot get to sleep within 30 minutes,” “waking up in the middle of the night or early morning,” “had to get up to use bathroom,” “cannot breathe comfortably,” “cough or snore loudly,” “feel too cold or hot,” “having bad dreams,” “pain,” and other problems. All these reported sleep disturbances may reflect the severity of some menopausal symptoms, such as urinary frequency, anxiety, and hot flashes. Moreover, the latter symptoms were significantly associated with increased CVD risks [5, 6, 31]. In addition, these sleep disturbances may have interrupted the physiological recovery function of sleep and therefore led to poorer cardiovascular health [11]. Future studies should attempt to develop CVD prevention strategies by addressing the sleep disturbances experienced by post-menopausal women.
Interestingly, women who were still working were at lower risk for CVD (β = −0.19, p = 0.016). Some women might stop working due to the comorbidity of hypertension, diabetes, or poor sleep quality. These health problems would contribute to an increased CVD risk. On the other hand, the majority of the women in the working group were manual labourers, who are likely to have higher levels of physical activity compared with those in the non-working group. Moreover, the working women were significantly younger than the non-working women (57.8 vs. 64.3 years, p < 0.001). Because age is a significant predictor in the algorithm of the FRS [19], the correlation between working status and CVD risk should be interpreted with caution. Future studies should pay attention to promote the cardiovascular health among post-menopausal women who are not working, such as improving their physical activity levels.
The CVD risk was found to be reduced by half in women who had better sleep quality than those who had poor sleep quality (OR = 0.51, p = 0.04). This finding was consistent with the results of previous studies. Good sleep quality has been recognized as a beneficial factor for cardiovascular health, and may prevent the development of CVD [9]. One study in the Netherlands reported that short-duration sleepers with poor sleep quality had a 63% increased risk for CVD, and a 79% higher risk for CHD when compared to normal-duration sleepers who had good sleep quality [11]. This evidence further strengthens the need to include sleep quality as an important indicator when assessing CVD risk among Chinese post-menopausal women.
Considering the critical contribution of SBP and use of anti-hypertensive medication on CVD risks and the close relationship between sleep quality and CVD risks in the current study participants, further analysis was conducted to explore the relationship between sleep quality and BP control. The Eighth Joint National Committee recommended that for those <60 years, the control target is SBP < 140 mmHg and DBP < 90 mmHg; and for those ≥60 years, the control target is SBP < 150 mmHg and DBP < 90 mmHg [32]. Accordingly, the participants were divided into three groups: those with hypertension and controlled BP; those with hypertension but uncontrolled BP; and a group without hypertension. However, the one way analysis of variance did not revealed statistically significant difference in sleep quality among the groups (F = 3.055, p = 0.050054).
To the best of our knowledge, this is the first study to examine the relationship between sleep quality and CVD risk among Chinese post-menopausal women. Nonetheless, this study had some limitations. First, this was a cross-sectional study with an internal limitation in confirming the cause-and-effect relationships. Future study should use a prospective study design with long-term follow-up to further explore the relationship between sleep quality and CVD risk. Secondly, sleep quality was measured by the self-reported PSQI. Previous studies had extensively used such a self-report system, even through a single item to assess sleep duration or sleep quality. Anyway, the PSQI is a comprehensive assessment of sleep quality and has revealed good performance in psychometric properties [27, 30]. To eliminate the possibility of self-reporting bias, future studies should employ a more objective approach to measure sleep quality, such as polysomnography and actigraphy. Moreover, the medical history of hypertension, diabetes, and hypercholesterolemia was also collected based on participants’ self-report information. To get more accurate information, future studies could conduct blood tests or retrieve data from participants’ medical records.
Conclusions
In conclusion, this study identified that Chinese post-menopausal women had poor sleep quality and increased CVD risk. Special attention should be paid to improve the sleep quality and cardiovascular health in these women. As indicted by the significant relationship between sleep quality and CVD risk, poor sleep quality might increase the CVD risk in post-menopausal women. To improve their cardiovascular health, future interventions should target towards strategies for improving sleep quality and for addressing sleep disturbances.
Abbreviations
- BMI:
-
Body mass index
- CHD:
-
Coronary heart disease
- CI:
-
Confidence interval
- CVD:
-
Cardiovascular disease
- DBP:
-
Diastolic blood pressure
- FRS:
-
Framingham 10-year risk score
- OR:
-
Odds ratio
- PSQI:
-
Pittsburgh sleep quality index
- SBP:
-
Systolic blood pressure
- SD:
-
Standard deviation
References
Feng JJ. Worries about the sexual health of Chinese women during menopause, Implies from the Euro-Asia study on health of menopause women. Beijing: People’s Daily; 2006. Vol. 14.
Shifren JL, Gass ML. NAMS recommendations for clinical Care of Midlife Women Working Group: the North American Menopause Society recommendations for clinical care of midlife women. Menopause. 2014;21(10):1038–62.
He L, Tang X, Li N, Wu Y, Wang J, Li J, Zhang Z, Dou H, Liu J, Yu L. Menopause with cardiovascular disease and its risk factors among rural Chinese women in Beijing: a population-based study. Maturitas. 2012;72(2):132–8.
Colditz GA, Willett WC, Stampfer MJ, Rosner B, Speizer FE, Hennekens CH. Menopause and the risk of coronary heart disease in women. N Engl J Med. 1987;316(18):1105–10.
Van der Schouw Y, van der Graaf Y, Steyerberg E, Eijkemans M, Banga J. Age at menopause as a risk factor for cardiovascular mortality. Lancet. 1996;347(9003):714–8.
Rosano G, Vitale C, Marazzi G, Volterrani M. Menopause and cardiovascular disease: the evidence. Climacteric. 2007;10(sup1):19–24.
Mosca L, Benjamin EJ, Berra K, Bezanson JL, Dolor RJ, Lloyd-Jones DM, Newby LK, Pina IL, Roger VL, Shaw LJ. Effectiveness-based guidelines for the prevention of cardiovascular disease in women-2011 update: a guideline from the American Heart Association. J Am Coll Cardiol. 2011;57(12):1404–23.
Polo-Kantola P, Saaresranta T, Polo O. Aetiology and treatment of sleep disturbances during perimenopause and postmenopause. CNS drugs. 2001;15(6):445–52.
Chung KF, Tang MK. Subjective sleep disturbance and its correlates in middle-aged Hong Kong Chinese women. Maturitas. 2006;53(4):396–404.
Huang K, Xu L, Nasri N, Jaisamrarn U. The Asian menopause survey: knowledge, perceptions, hormone treatment and sexual function. Maturitas. 2010;65(3):276–83.
Hoevenaar-Blom MP, Spijkerman AM, Kromhout D, van den Berg JF, Verschuren WM. Sleep duration and sleep quality in relation to 12-year cardiovascular disease incidence: the MORGEN study. Sleep. 2011;34(11):1487–92.
Shahar E, Whitney CW, REdline S, Lee ET, Newman AB, Javier Nieto F, O'Connor GT, Boland LL, Schwartz JE, Samet JM. Sleep-disordered breathing and cardiovascular disease: cross-sectional results of the sleep heart health study. Am J Respir Crit Care Med. 2001;163(1):19–25.
Wang Q, Li X. Study on sleep quality of elderly in communities in Xi'an city and its influencing factors. Chin Nurs Res. 2012;7:591–4.
Harlow SD, Gass M, Hall JE, Lobo R, Maki P, Rebar RW, Sherman S, Sluss PM, De Villiers TJ. Executive summary of the stages of reproductive aging workshop 10: addressing the unfinished agenda of staging reproductive aging. Climacteric. 2012;15(2):105–14.
Liu X, Tang M, Hu L. Reliability and validity of the Pittsburgh sleep quality index. Chinese Journal of Psychiatry. 1996;29:103–7.
Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh sleep quality index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213.
Backhaus J, Junghanns K, Broocks A, Riemann D, Hohagen F. Test–retest reliability and validity of the Pittsburgh sleep quality index in primary insomnia. J Psychosom Res. 2002;53(3):737–40.
Mollayeva T, Thurairajah P, Burton K, Mollayeva S, Shapiro C, Colantonio A. The Pittsburgh sleep quality index as a screening tool for sleep dysfunction in clinical and non-clinical samples: a systematic review and meta-analysis. Sleep Med Rev. 2015;25:52–73.
D'Agostino RBS, Vasan RS, Pencina MJ, Wolf PA, Cobain M, Massaro JM, Kannel WB. General cardiovascular risk profile for use in primary care: the Framingham heart study. Circulation. 2008;117(6):743–53.
Tabachnick BG. In: Tabachnick BG, Fidel LS, editors. Using multivariate statistics /. 6th ed. Boston: Boston: Pearson Education; 2013.
Corp I: IBM SPSS statistics for Windows, version 21.0. 2012.
Lloyd LJ, Langley-Evans SC, McMullen S. Childhood obesity and risk of the adult metabolic syndrome: a systematic review. Int J Obes. 2012;36(1):1–11.
Grundy SM, Cleeman JI, Merz CNB, Brewer HB, Clark LT, Hunninghake DB, Pasternak RC, Smith SC, Stone NJ. Implications of recent clinical trials for the national cholesterol education program adult treatment panel III guidelines. J Am Coll Cardiol. 2004;44(3):720–32.
Chen H, Liu J, Zhang X. Association between sleep quality and psychosomatic symptoms in menopause women in community. Medical Journal of Chinese People's Health. 2008;20(3):200–3.
Lin Y, Li F, Zhang J, Wang L. Investigation and analysis on health status in climacteric women of Xi'an City. Journal of Xi'an Jiaotong University (Medical Sciences). 2008;1:110–4.
Kannel WB, Hjortland MC, McNamara PM, Gordon T. Menopause and risk of cardiovascular disease: the Framingham study. Ann Intern Med. 1976;85(4):447–52.
Young T, Rabago D, Zgierska A, Austin D, Laurel F. Objective and subjective sleep quality in premenopausal, perimenopausal, and postmenopausal women in the Wisconsin sleep cohort study. Sleep. 2003;26(6):667–72.
Lee KA, Kryger MH. Women and sleep. J Women's Health. 2008;17(7):1189–90.
Knutson KL, Turek FW. The U-shaped association between sleep and health: the 2 peaks do not mean the same thing. Sleep. 2006;29(7):878–9.
Cappuccio FP, Cooper D, D'Elia L, Strazzullo P, Miller MA. Sleep duration predicts cardiovascular outcomes: a systematic review and meta-analysis of prospective studies. Eur Heart J. 2011;32(12):1484–92.
Szmuilowicz ED, Manson JE, Rossouw JE, Howard BV, Margolis KL, Greep NC, Brzyski RG, Stefanick ML, O'Sullivan MJ, Wu C, Allison M, Grobbee DE, Johnson KC, Ockene JK, Rodriguez BL, Sarto GE, Vitolins MZ, Seely EW. Vasomotor symptoms and cardiovascular events in postmenopausal women. Menopause. 2011;18(6):603–10.
James PA, Oparil S, Carter BL, Cushman WC, Dennison-Himmelfarb C, Handler J, Lackland DT, LeFevre ML, MacKenzie TD, Ogedegbe O, Smith SC. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the eighth joint National Committee (JNC 8). JAMA. 2014;311(5):507–20.
Acknowledgements
The authors would like to thank all the participants of the study.
Funding
Nil.
Availability of the data and materials
Data were available upon request from the corresponding author.
Author information
Authors and Affiliations
Contributions
SYC, QW, and XML were involved in the study design and coordination. QW and XML conducted the data collection. QW, HYC and SWL completed the data analysis. SYC, QW, HYC and SWL drafted the manuscript. XML, EMW and JWS revised the manuscript for quality, consistency and accuracy. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Ethical Committee of the Xian Jiaotong University [13]. Each participant received detailed explanation about the study and provided written informed consent before participating in the study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Chair, S.Y., Wang, Q., Cheng, H.Y. et al. Relationship between sleep quality and cardiovascular disease risk in Chinese post-menopausal women. BMC Women's Health 17, 79 (2017). https://doi.org/10.1186/s12905-017-0436-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12905-017-0436-5