
Abstract
Background
Insulin resistance is an important cause of cardiovascular events and cerebral infarction development. We aimed to investigate the association of the triglyceride glucose (TyG) index with atherosclerotic burden and plaques in coronary, intra- and extracranial arteries in participants with non-diabetes, and compared the results with that of the homeostasis model assessment of insulin resistance (HOMA-IR).
Methods
Participants without diabetes in the PolyvasculaR Evaluation for Cognitive Impairment and vaScular Events (PRECISE) study were included. We categorized participants by tertiles of the TyG index and the concordance/discordance of the TyG index and HOMA-IR. Discordance was defined as a TyG index equal to or greater than the median and HOMA-IR less than the median, or vice versa. The atherosclerosis plaques and burden in coronary, intra- and extracranial arteries were evaluated. The association of HOMA-IR and TyG index with the presence of atherosclerotic plaques and atherosclerotic burden was assessed by binary and ordinal logistic regression models, respectively.
Results
Among 2,719 included participants, the average age was 60.9 (± 6.6) years, and 53.0% were female. Both TyG index and HOMA-IR were associated with increased odds of coronary/intra- and extracranial atherosclerotic plaques and burden after adjustment for age, sex, currenting smoking and drinking (all P < 0.05). However, the association between HOMA-IR and intracranial atherosclerosis was not statistically significant after adjustment for all potential confounders. Discordantly high TyG index with HOMA-IR had a higher odd of extracranial plaque (odds ratio [OR]: 1.34, 95% confidence interval [CI]: 1.04–1.71), extracranial atherosclerotic burden (common odds ratio [cOR]: 1.35, 95% CI 1.06–1.71), coronary plaque (OR: 1.30, 95% CI 1.01–1.68) and segment stenosis score (cOR: 1.39, 95% CI 1.09–1.78) as compared with concordantly low TyG index with HOMA-IR. The TyG index had a better net reclassification improvement ability than HOMA-IR for atherosclerotic plaques when adding to baseline model.
Conclusion
Elevated TyG index was associated with increased odds of atherosclerosis in coronary/intra- and extracranial arteries. Compared with HOMA-IR, the TyG index was more strongly associated with intracranial atherosclerosis. Moreover, discordantly high TyG index with HOMA-IR was also important for atherosclerosis identification.
Similar content being viewed by others
Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Background
Insulin resistance, as a risk factor for metabolic diseases, was involved in the development of cardiovascular disease [1] and associated with increased stroke risk [2]. Previous studies have reported an association between insulin resistance and early arteriosclerotic lesions [3], the development of which is the main pathological cause of cardiovascular artery disease and stroke [4, 5]. Among biomarkers of insulin resistance, the homeostasis model assessment of insulin resistance (HOMA-IR) index is the most common method for measuring insulin resistance [6]. Recently, the triglyceride glucose (TyG) index, a noninsulin-based and inexpensive approach index to evaluate insulin resistance, has been developed. The TyG index is calculated by fasting glucose and triglyceride, and proposed as a useful surrogate marker of insulin resistance [7]. Some studies have shown that the TyG index had a better value for assessing insulin resistance [8,9,10] and was more closely related to coronary artery stenosis and calcification than HOMA-IR [8, 9]. However, few studies have focused on comparison of relationship of insulin resistance indexes with comprehensive evaluation of atherosclerotic burden and plaques, especially in intra- and extracranial arteries.
We therefore aimed to investigate the association of the TyG index with comprehensive atherosclerotic burden and plaques in coronary, intra- and extracranial arteries in nondiabetic community-dwelling adults and compared the results with that of HOMA-IR.
Methods
Participants
The PolyvasculaR Evaluation for Cognitive Impairment and vaScular Events (PRECISE) study recruited 3067 participants aged 50 to 75 from a cluster sample of 6 villages and 4 communities in Lishui city between May 2017 and September 2019. Details of the study have been published elsewhere[11]. Participants with contraindications to computed tomography angiography (CTA) and magnetic resonance imaging (MRI), mental illness, and life expectancy of less than 4 years were excluded. All participants were comprehensively evaluated for stenosis and plaques in coronary, intra- and extracranial arteries with advanced vascular imaging techniques. The Ethics Committee approved the study protocol of Beijing Tiantan Hospital (IRB Approval No. Ky2017-010-01) and Lishui Hospital (IRB Approval No. 2016-42), and all participants have signed informed consents before enrollment. Participants with self-reported diabetes previously diagnosed by a physician or using of glucose-lowering or insulin medications were excluded from this analysis. Non-diabetic participants who underwent CTA examination, MRI examination, and blood sampling were included in the analysis.
Anthropometric, clinical and socio‑demographic parameters
All anthropometric, clinical and socio-demographic data were collected face to face by trained interviewers following the standard protocols, which included age, sex, education level, body mass index (BMI), smoking, drinking, relevant medical history, and self-reported medication use. BMI was calculated as weighted (kg) divided by the square of height (m2) [6]. Hypertension was defined as hypertension previously diagnosed by physicians or current use of antihypertensive agents or systolic blood pressure ≥ 140 mmHg or diastolic blood pressure ≥ 90 mmHg [12]. History of dyslipidemia was determined by self-reported dyslipidemia previously diagnosed by a physician usually according to Chinese guidelines for the prevention and treatment of adult dyslipidemia[13] or current use of lipid-lowering drugs (e.g., statins, fibrates).
Biological measurements
Venous blood samples were collected in the morning after fasting for at least 8 h at night and transported to Tiantan Hospital biobank for preservation by the cold chain. Biological measurements, including fasting glucose, fasting insulin and triglyceride, were validated and measured in the Central Laboratory of Beijing Tiantan Hospital under strict quality control standards. Insulin resistance was assessed by using HOMA-IR model and the TyG index. The TyG index was determined as ln (fasting triglycerides [mg/dL] × fasting glucose [mg/dL]/2)] [8] and the HOMA-IR was calculated as (fasting insulin [µU/ mL] × fasting glucose [mmol/L])/22.5 [6]. Participants were categorized into 4 concordance/discordance groups: high TyG index/ high HOMA-IR, high TyG index/ low HOMA-IR, low TyG index/ high HOMA-IR, low TyG index/ low HOMA-IR [14]. A TyG index equal to or greater than the median and less than the median were defined as high TyG index and low TyG index, respectively, and similar definition was applied to HOMA-IR. The high TyG index /low HOMA-IR and high HOMA-IR/ low TyG index groups were considered as discordance.
Measurements of coronary atherosclerosis
The CTA was performed on a dual-source CT scanner (SOMATOM Force, Siemens Healthineers, Forchheim, Germany) to examine coronary atherosclerosis burden. The presence of coronary plaque was defined as a structure > 1mm2 within and/or adjacent to the coronary artery lumen, which could be clearly distinguished from the vessel lumen and the surrounding pericardial/myocardial tissue [15]. The evaluated coronary artery segments included the left main trunk, anterior descending branch, diagonal branch, circumflex branch, obtuse margin branch, middle branch, right coronary artery, posterior descending branch and posterior lateral branch. Coronary stenosis was quantified by visual estimation, and each artery segments graded as following: score 0, minimal (< 30%); score 1, mild (30–49%); score 2, moderate (50–69%); score 3, severe (> 70%) [16]. The segment stenosis score (SSS) was calculated as a measure of the overall coronary artery plaque burden, and was graded and summed for each coronary segment as none to severe plaque (0–3) based on the extent of obstruction (total score ranging: 0 to 27) [15]. The SSS was further categorized into three grades (grade 0, 0 score; grade 1, 1–3 scores; grade 2, ≥ 4 scores). We calculated the Cohens κ to evaluated interobserver agreement for the presence of plaque and artery stenosis (Cohen κ = 0.96 and 0.92).
Measurements of intra- and extracranial atherosclerosis
The 3.0T scanner (Ingenia 3.0T, Philips, Best, The Netherlands) was used to detect intra-/extra-cranial atherosclerotic plaques and stenosis. The imaging sequences included three-dimensional time-of-flight magnetic resonance angiography (3D-TOF-MRA) and three-dimensional isotropic high-resolution black-blood T1w vessel wall imaging (3D T1w VWI). The presence of intra- and extracranial atherosclerosis plaques was defined as eccentric wall thickening with or without luminal stenosis identified on the 3D T1w VWI images in comparison to the corresponding location on the 3D TOF MR angiogram at MR angiography [17, 18]. The evaluated intracranial arterial segments included the bilateral internal carotid, anterior cerebral arteries (A1, A2), the middle cerebral artery (M1, M2), posterior cerebral arteries (P1, P2), and basal vertebral arteries (V4). The extracranial arterial segments included the common carotid, proximal internal carotid artery, and vertebral artery (V1, V2, V3) [17]. The Warfarin-Aspirin Symptomatic Intracranial Disease Trial (WASIDT) [19] was used to assess the luminal stenosis in the intracranial arteries, and the North American Symptomatic Carotid Endarterectomy Trial (NASCET) [20] was used to measure the luminal stenosis in the extracranial arteries. According to the degree of atherosclerotic plaques and stenosis, semi-quantitative score was used to evaluate atherosclerotic conditions (0, no atherosclerotic plaque; 1 atherosclerotic plaque without evident lumen stenosis or stenosis < 50%; 2, stenosis 50-69%; 3, stenosis 70-99%; 4, occlusion) [21]. The intracranial atherosclerotic burden was calculated through summing the intracranial atherosclerotic scores of intracranial arterial segments, which were categorized into four grades of 0, 1, 2–3, and ≥ 4 scores [21]. Similarly, the extracranial atherosclerotic burden was counted through extracranial arterial segments, and categorized into four grades of 0, 1, 2–3, and ≥ 4 scores[21]. We calculated the Cohens κ to assess the interrater reliability for the presence of plaques and artery stenosis ≥ 50% in intra- and extracranial artery (Cohen κ = 0.97 and 0.79 for intracranial artery and Cohen κ = 0.94 and 0.86 for extracranial artery).
Statistical methods
The characteristics of the participants were displayed according to the tertiles of insulin resistance index. Data are presented as mean ± standard deviation (SD) or median [interquartile range (IQR)] for continuous variables and as the frequency (%) for categorical variables. We used ANOVA or Kruskal-Wallis test for continuous variables and χ2 test or Fisher’s exact for categorical variables. The association of TyG index or HOMA-IR with the presence of atherosclerotic plaques was analyzed by binary logistic regressions and with the atherosclerotic burden by ordinal logistic regression models. The odds ratio (OR) or common odds ratio (cOR) with 95% confidence intervals (CI) were estimated. Logistic regression models were also applied to estimate odds for atherosclerosis associated with concordance/discordance groups. We used 2 models: model 1, unadjusted; model 2, adjusted for age, sex, current smoking, current drinking, BMI, estimated glomerular filtration rate, low-density lipoprotein levels, medical history of transient ischemic attack, stroke, coronary artery disease, hypertension, dyslipidemia, and use of antihypertensive and antiplatelet medications. Restricted cubic splines with 5 knots were constructed to model a non-linear relationship between HOMA-IR or TyG and the presence of atherosclerotic plaques. The area under the receiver operating characteristic curve (AUC), the integrated discrimination improvement (IDI), and the net reclassification improvement (NRI) were determined to assess the predictive performance of insulin resistance index [7].
Two-tailed P value < 0.05 was considered statistically significant, and all analyses were performed using SAS version 9.4 (SAS Institute Inc, Cary, NC).
Results
Baseline characteristics
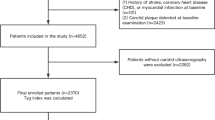
Among the 3,067 enrolled participants, 307 participants with diabetes, 4 with missing fasting glucose, fasting insulin or triglyceride, and 37 without CTA or MRI examinations were excluded, and a total of 2,719 participants were available for final analysis (Fig. 1). The demographic and clinical characteristics of the included participants are shown according to the tertiles of TyG index in Table 1. Among the included participants, the average age was 60.9 (± 6.6) years, and 53.0% were women. Participants with higher TyG had more frequent dyslipidemia and hypertension, and higher levels of BMI, fasting glucose, fasting insulin, and triglyceride (P < 0.05). Baseline characteristics compared across the 4 concordance/discordance groups and different HOMA-IR tertiles are shown in Additional file 1: Table S1-S2.

Flowchart of the included participants. PRECISE, PolyvasculaR Evaluation for Cognitive Impairment and vaScular Events; CTA, computed tomography angiography; MRI, magnetic resonance imaging
Association of insulin resistance and atherosclerosis
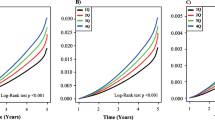
Of the 2,719 nondiabetic participants, 432(15.89%) had intracranial plaques, 975(35.86%) had extracranial plaques and 1160(42.66%) had coronary plaques. Compared with the first tertile, the third tertile of TyG was associated with increased odds of the presence of intracranial plaques (OR,1.45; 95%CI, 1.09–1.92, P = 0.01), intracranial atherosclerotic burden (cOR,1.40; 95%CI, 1.06–1.85, P = 0.02), the presence of extracranial plaques (OR,1.25; 95%CI, 1.01–1.55, P = 0.04), extracranial atherosclerotic burden (cOR: 1.28, 95% CI, 1.04–1.58, P = 0.02), the presence of coronary plaques (OR: 1.42, 95% CI, 1.14–1.76, P = 0.002) and segment stenosis score (cOR: 1.40, 95% CI, 1.14–1.73, P = 0.002) after adjusting for potential covariates (Table 2). Similar results were observed for the HOMA-IR in model1, but the association between HOMA-IR and the presence of intra- and extracranial atherosclerotic plaques, and intracranial atherosclerotic burden was not significant after adjustment for all confounders (all P > 0.05). In Fig. 2, multivariable-adjusted spline regression models showed a positive relationship between TyG index or HOMA-IR and the presence of coronary, intra- and extracranial plaques.

Association of insulin resistance with the presence of coronary, intracranial and extracranial arteries plaque. Multivariable-adjusted ORs for the presence of intracranial(A), extracranial (B) and coronary (C) plaques based on restricted cubic spines with 5 knots (5th, 25th, 50th, 75th, and 95th percentiles) of TyG index. Multivariable-adjusted ORs for the presence of intracranial(D), extracranial (E) and coronary (F) plaques based on restricted cubic spines with 5 knots (5th, 25th, 50th, 75th, and 95th percentiles) of HOMA-IR.
HOMA-IR, homeostasis model assessment insulin resistance; TyG, the triglyceride glucose index
All models adjusted for age, sex, current smoking, current drinking, BMI, estimated glomerular filtration rate, low-density lipoprotein levels, medical history of TIA, stroke, coronary disease, hypertension and dyslipidemia, using of antihypertensive and antiplatelet medications
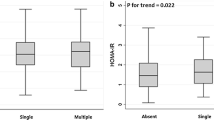
Figure 3 shows the different proportions of participants with coronary, intra- and extracranial atherosclerotic burden in 4 concordance/discordance groups. In the concordance/discordance analysis (Table 3), discordantly high TyG index with HOMA-IR had a greater odd of extracranial plaque (OR: 1.34, 95% CI 1.04–1.71), extracranial atherosclerotic burden (cOR: 1.35, 95% CI 1.06–1.71), coronary plaque (OR: 1.30, 95% CI 1.01–1.68) and segment stenosis score (cOR: 1.39, 95% CI 1.09–1.78) as compared with concordantly low TyG index with HOMA-IR. For the outcome of the presence of atherosclerotic plaques, we found the TyG index had a better net reclassification improvement ability than HOMA-IR when adding to baseline models (NRI, 9.57 -18.01%, all P < 0.05) (Additional file 1: Table S3).

Bar charts of atherosclerotic burden of concordance/discordance groups
Distribution of intracranial atherosclerotic burden(A), extracranial atherosclerotic burden(B), and Segment stenosis score(C) in accordance and discordance groups
HOMA-IR, homeostasis model assessment insulin resistance; TyG, the triglyceride glucose index
The intracranial atherosclerosis burden was graded according to the sum of intracranial atherosclerosis scores, including 0, 1, 2–3 and ≥ 4 scores
The extracranial atherosclerosis burden was graded according to the sum of extracranial atherosclerosis scores, including 0, 1, 2–3 and ≥ 4 scores
Segment stenosis score, the total number of segments with any plaque was graded: 0, 1–3, and ≥ 4 scores
Discussion
This cross-sectional study showed significant associations between the TyG index and intra- and extracranial, and coronary atherosclerosis after adjustment for confounders. The TyG index was more strongly associated with increased odds for the presence of intracranial atherosclerotic plaques and burden than HOMA-IR after adjustment for potential covariates. Moreover, the TyG index for atherosclerotic plaques had a better improvement ability than HOMA-IR, and the concordance/discordance analysis also reveal extra clinical value of the TyG index.
Several studies suggested that TyG index was recognized as a risk factor for cardiovascular disease [1, 22, 23]. Ki-Bum Won et al. [22] demonstrated the TyG index was associated with an increased risk of severe coronary artery disease in patients with near-normal renal function, and Kahui Park et al. [1] showed elevated TyG index level was significantly associated with the progression of coronary artery calcification regardless of other conventional risk factors. In addition, The TyG index was more independently associated with coronary artery atherosclerosis than HOMA-IR in healthy Korean adults [9]. Similarly, the Asan Medical Center [24] demonstrated the TyG index rather than HOMA-IR had an independent association with the presence of coronary artery disease in non-diabetic patients. Although there was a difference in outcome measures, our study arrived at a similar conclusion that the TyG index but not HOMA-IR was strongly associated with coronary atherosclerosis from the perspective of the presence of coronary atherosclerosis plaques and burden.
Moreover, previous studies have also reported the association between insulin resistance and intra- and extra-cranial arterial disease [25, 26]. There was very little literature linking insulin resistance with extracranial atherosclerosis, but some literature showed that insulin resistance could cause intracranial atherosclerosis by affecting arterial dilation [26, 27]. The Kongcun Town Study [28] demonstrated that the insulin resistance was related to asymptomatic intracranial arterial stenosis. Similarly, the AsIA cohort study [29] suggested insulin resistance and related metabolic abnormalities emerged as an important mechanism involved in the development of intracranial atherosclerotic disease. On the contrary, based on Transcranial Doppler Ultrasonography examination, the APAC study [25] showed elevated TyG index was associated with a significantly higher risk of extracranial artery stenosis, but not with intracranial artery stenosis. Compared with previous studies, our study used a high-resolution black-blood T1w vessel wall imaging technique to evaluate intra- and external stenosis, and provided additional evidence for significant correlation between the TyG index and intra- and external burden and plaques. Meanwhile, we further demonstrated that the TyG index had a better value in identifying intra- and external atherosclerosis plaques than HOMA-IR.
Although the mechanisms of TyG index had superior association than HOMA-IR with atherosclerosis have not yet been fully elucidated, two possible explanations have been proposed. First, the two insulin resistance indexes may reflect different aspects of insulin resistance. The TyG index was thought to reflect the insulin resistance of both the hepatic and peripheral tissues[9], whereas HOMA-IR only reflects insulin resistance of hepatic tissues [10]. The peripheral insulin resistance was a useful marker of atherosclerosis risk [30]. Thus, the TyG index showed a significantly association with atherosclerosis. Second, one important mechanism between insulin resistance and atherosclerosis might be hyperglycemic damage [22]. Besides, when triglyceride levels are very high, the triglyceride-rich chyle particles are too large to cross the endothelial barrier into the intima, and then also cause atherosclerosis [31]. The TyG index takes into account the effects of fasting glucose and triglyceride, and mirrors the physiological condition of glucose and lipid at the same time [32]. Evaluated by two common clinical indicators (fasting glucose and triglyceride), the TyG index also have a potential clinical advantage that it was noninsulin-based and less costly than HOMA-IR [8]. This may suggest that the TyG index could be a more appropriate indicator for identifying high-risk atherosclerosis patients in clinical practice.
Strengths and limitations
Our study has several strengths. First, with advanced high-resolution imaging techniques, our study comprehensively assessed the intra-/extra-cranial atherosclerotic plaques and stenosis, and calculated atherosclerosis burden. Second, the concordance/discordance analysis helped us further understood the extra clinical value of the TyG index via the disagreements between the TyG index and HOMA-IR.
Some potential limitations also require careful consideration in the present study. First, the cross-sectional data limits the exploration of causality. The longitudinal study of atherosclerosis may better indicate the association between TyG index and progression of atherosclerosis diseases. Second, this study only includes the Chinese population and restricts the generalization of the results. Third, our study population comes from the same neighborhoods, and the inherent selection bias may influence our results to some extent. Despite these limitations, this study provides evidence for the correlation between TyG index and coronary, intracranial or extracranial atherosclerosis. These results need to be further validated in other large-scale populations.
Conclusion
Elevated TyG index was associated with increased odds of atherosclerosis in coronary, intra- and extracranial arteries. Compared with HOMA-IR, the TyG index was more strongly associated with intracranial atherosclerosis. Besides, the TyG index could be a more appropriate predictor to identify high-risk atherosclerosis patients.
Data availability
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- TyG index:
-
the triglyceride glucose index
- HOMA-IR:
-
the homeostasis model assessment of insulin resistance
- the PRECISE study:
-
the PolyvasculaR Evaluation for Cognitive Impairment and vaScular Events study
- OR:
-
odds ratio
- CI:
-
confidence interval
- cOR:
-
common odds ratio
- CTA:
-
contraindications to computed tomography angiography
- MRI:
-
magnetic resonance imaging
- BMI:
-
body mass index
- WASIDT:
-
the Warfarin-Aspirin Symptomatic Intracranial Disease Trial
- NASCET:
-
the North American Symptomatic Carotid Endarterectomy Trial
- IQR:
-
interquartile range
- AUC:
-
the receiver operating characteristic curve
- IDI:
-
the integrated discrimination improvement
- NRI:
-
the net reclassification improvement
References
Park K, Ahn CW, Lee SB, Kang S, Nam JS, Lee BK, et al. Elevated TyG index predicts progression of coronary artery calcification. Diabetes Care. 2019;42:1569–73.
Zhao Y, Sun H, Zhang W, Xi Y, Shi X, Yang Y, et al. Elevated triglyceride-glucose index predicts risk of incident ischaemic stroke: The Rural Chinese cohort study. Diabetes Metab. 2021;47:101246.
Liang CP, Han S, Senokuchi T, Tall AR. The macrophage at the crossroads of insulin resistance and atherosclerosis. Circ Res. 2007;100:1546–55.
Farhan S, Redfors B, Maehara A, McAndrew T, Ben-Yehuda O, De Bruyne B, et al. Relationship between insulin resistance, coronary plaque, and clinical outcomes in patients with acute coronary syndromes: an analysis from the PROSPECT study. Cardiovasc Diabetol. 2021;20:10.
Bonora E, Kiechl S, Willeit J, Oberhollenzer F, Egger G, Meigs JB, et al. Insulin resistance as estimated by homeostasis model assessment predicts incident symptomatic cardiovascular disease in caucasian subjects from the general population: the Bruneck study. Diabetes Care. 2007;30:318–24.
Wang S, Shi J, Peng Y, Fang Q, Mu Q, Gu W, et al. Stronger association of triglyceride glucose index than the HOMA-IR with arterial stiffness in patients with type 2 diabetes: a real-world single-centre study. Cardiovasc Diabetol. 2021;20:82.
Zhang Y, Ding X, Hua B, Liu Q, Gao H, Chen H, et al. Predictive effect of triglycerideglucose index on clinical events in patients with type 2 diabetes mellitus and acute myocardial infarction: results from an observational cohort study in China. Cardiovasc Diabetol. 2021;20:43.
Lee EY, Yang HK, Lee J, Kang B, Yang Y, Lee SH, et al. Triglyceride glucose index, a marker of insulin resistance, is associated with coronary artery stenosis in asymptomatic subjects with type 2 diabetes. Lipids Health Dis. 2016;15:155.
Kim MK, Ahn CW, Kang S, Nam JS, Kim KR, Park JS. Relationship between the triglyceride glucose index and coronary artery calcification in Korean adults. Cardiovasc Diabetol. 2017;16:108.
Lee SB, Ahn CW, Lee BK, Kang S, Nam JS, You JH, et al. Association between triglyceride glucose index and arterial stiffness in Korean adults. Cardiovasc Diabetol. 2018;17:41.
Pan Y, Jing J, Cai X, Wang Y, Wang S, Meng X, et al. PolyvasculaR Evaluation for Cognitive Impairment and vaScular Events (PRECISE)-a population-based prospective cohort study: rationale, design and baseline participant characteristics. Stroke Vasc Neurol. 2021;6:145–51.
Wang Z, Chen Z, Zhang L, Wang X, Hao G, Zhang Z, et al Status of Hypertension in China: Results From the China Hypertension Survey, 2012–2015. Circulation. 2018 137: 2344–2356.
Joint Committee on the Revision of Guidelines for Prevention and Treatment of Adult Dyslipidemia in China. Guidelines for the prevention and treatment of adult dyslipidemia in China (revised in 2016) (in Chinese). Chin Circulation J. 2016;31:937–53.
Hu C, Zhang J, Liu J, Liu Y, Gao A, Zhu Y, et al. Discordance between the triglyceride glucose index and fasting plasma glucose or HbA1C in patients with acute coronary syndrome undergoing percutaneous coronary intervention predicts cardiovascular events: a cohort study from China. Cardiovasc Diabetol. 2020;19:116.
Rana JS, Dunning A, Achenbach S, Al-Mallah M, Budoff MJ, Cademartiri F, et al. Differences in prevalence, extent, severity, and prognosis of coronary artery disease among patients with and without diabetes undergoing coronary computed tomography angiography: results from 10,110 individuals from the CONFIRM (COronary CT Angiography EvaluatioN For Clinical Outcomes): an InteRnational Multicenter Registry. Diabetes Care. 2012;35:1787–94.
Min JK, Shaw LJ, Devereux RB, Okin PM, Weinsaft JW, Russo DJ, et al. Prognostic value of multidetector coronary computed tomographic angiography for prediction of all-cause mortality. J Am Coll Cardiol. 2007;50:1161–70.
Ye Qiao EG, Fareed K, Suri L, Liu Y, Zhang Z, Anwar S, Mirbagheri, YuanYuan Joyce Xie, Nariman Nezami, Jarunee Intrapiromkul, Shuqian Zhang, Alvaro Alonso, Haitao Chu, David Couper, Bruce A, Wasserman. MR imaging Measures of intracranial atherosclerosis in a Population-based study. Radiology. 2016.
Ye Qiao PSRZ, PhD Saeedeh Mirbagheri MD, Richard Leigh MD, Victor Urrutia MD, Robert Wityk MD, Bruce MD. A. Wasserman, MD. Intracranial Plaque enhancement in Patients with cerebrovascular events on highspatial-resolution Mr images. Radiology. 2014;271:2.
Owen B. Samuels GJJ, Lynn MJ, Smith HA, Marc I. Chimowitz. A standardized method for measuring intracranial arterial stenosis. American Society of Neuroradiology. 2000: 643–646.
Allan J. Fox M. FRCPC How to measure carotid stenosis. Radiology. 1993.
Kong Q, Ma X, Wang C, Du X, Ren Y, Wan Y. Total Atherosclerosis burden of baroreceptor-resident arteries independently predicts blood pressure dipping in patients with ischemic stroke. Hypertension. 2020;75:1505–12.
Won KB, Kim YS, Lee BK, Heo R, Han D, Lee JH, et al. The relationship of insulin resistance estimated by triglyceride glucose index and coronary plaque characteristics. Med (Baltim). 2018;97:e10726.
Thai PV, Tien HA, Van Minh H, Valensi P. Triglyceride glucose index for the detection of asymptomatic coronary artery stenosis in patients with type 2 diabetes. Cardiovasc Diabetol. 2020;19:137.
Cho YR, Ann SH, Won KB, Park GM, Kim YG, Yang DH, et al. Association between insulin resistance, hyperglycemia, and coronary artery disease according to the presence of diabetes. Sci Rep. 2019;9:6129.
Wang A, Tian X, Zuo Y, Chen S, Zhang X, Guo J, et al. Association of triglyceride-glucose index with intra- and extra-cranial arterial stenosis: a combined cross-sectional and longitudinal analysis. Endocrine. 2021;74:308–17.
Bang OY. Intracranial Atherosclerotic Stroke: Specific Focus on the Metabolic Syndrome and Inflammation. 2006 8: 330–336.
V Salomaa WR, Kark JD, Nardo C, Folsom AR. Non-insulin-dependent diabetes mellitus and fasting glucose and insulin concentrations are associated with arterial stiffness indexes. The ARIC Study. Atherosclerosis Risk in Communities Study. Circulation. 1995;91:1432–43.
Wang Q, Zhao Y, Wang X, Ji X, Sang S, Shao S, et al Association between asymptomatic intracranial arterial stenosis and insulin resistance or diabetes mellitus: a cross-sectional study in rural Shandong, China. BMJ Open Diabetes Res Care. 2020 8.
Lopez-Cancio E, Galan A, Dorado L, Jimenez M, Hernandez M, Millan M, et al. Biological signatures of asymptomatic extra- and intracranial atherosclerosis: the Barcelona-AsIA (Asymptomatic Intracranial Atherosclerosis) study. Stroke. 2012;43:2712–9.
Irace C, Carallo C, Scavelli FB, De Franceschi MS, Esposito T, Tripolino C, et al. Markers of insulin resistance and carotid atherosclerosis. A comparison of the homeostasis model assessment and triglyceride glucose index. Int J Clin Pract. 2013;67:665–72.
Sascau R, Clement A, Radu R, Prisacariu C, Statescu C. Triglyceride-Rich lipoproteins and their remnants as silent promoters of atherosclerotic cardiovascular disease and other metabolic disorders: A review. Nutrients. 2021;13:1774.
GARY F. LEWIS, AC, KHOSROW ADELI, AND ADRIA GIACCA. Disordered fat storage and mobilization in the pathogenesis of insulin resistance and type 2 diabetes. Endocr Rev. 2002;23(2):201–29.
Acknowledgements
We would like to thank the staff and participants of the PolyvasculaR Evaluation for Cognitive Impairment and vaScular Events study for their contributions.
Funding
This study is supported by grants from the Beijing Hospitals Authority Youth Programme (QML20190501), National Natural Science Foundation of China (81971091, 81870905, U20A20358, 82111530203), Outstanding Young Talents Project of Capital Medical University (A2105), Chinese Academy of Medical Sciences Innovation Fund for Medical Sciences (2019-I2M-5-029), Key Science & Technologies R&D Program of Lishui City (2019ZDYF18), Zhejiang provincial program for the Cultivation of High-level Innovative Health talents and grants from AstraZeneca Investment (China) Co., Ltd.
Author information
Authors and Affiliations
Contributions
MXW and LRM contributed equally to the manuscript. MXW and LRM made substantial contributions to study design, data analysis and manuscript writing. AMJ made substantial contributions to data analysis. XLC, JJ, SYW, XM, SL and TMW made contributions to data collection. YJW and YSP made substantial contributions to study design and intellectual direction and revised the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participants
The study protocol was approved by the Ethics Committee of the Beijing Tiantan Hospital (IRB Approval No. Ky2017-010-01) and Lishui Hospital (IRB Approval No. 2016-42). All participants or their representatives provided the written informed consent before participating in the study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Wang, M., Mei, L., Jin, A. et al. Association between triglyceride glucose index and atherosclerotic plaques and Burden: findings from a community-based study. Cardiovasc Diabetol 21, 204 (2022). https://doi.org/10.1186/s12933-022-01638-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12933-022-01638-x