
Abstract
Background
The role of Accredited Social Health Activist (ASHA) in the health care delivery services at the periphery level is crucial for achieving disease prevention, control and elimination goals. The objective of the study was to assess the knowledge, attitude, practices, priorities and capability of ASHA related to malaria diagnosis and treatment as part of the Malaria Elimination Demonstration Project in 1233 villages of district Mandla, Madhya Pradesh.
Methods
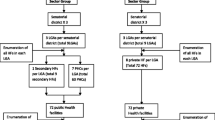
A cross sectional study was conducted using a fully structured, pre-tested interview schedule during June and July 2017 (before the field operations of MEDP were started). Two hundred twenty (17%) of the total ASHAs were selected for the interview from the 9 developmental blocks of Mandla district.
Results
Knowledge, Attitude and Practices (KAP) study revealed that most ASHAs knew that mosquitoes are the main agent for spread of malaria (97.7%). They mostly used Rapid Diagnostic Test (RDT) for diagnosis (91.8%). The majority (87.3%) correctly identified negative RDT result while only 15% and 10.5%, respectively, identified Plasmodium vivax and Plasmodium falciparum positive cases correctly. Further analysis showed that 85% ASHAs used chloroquine, 44.5% used artemisinin-based combination therapy (ACT), and 55.5% used primaquine for treatment of malaria. It was also found that only 38.2% ASHA gave PQ for 14 days in cases of P. vivax. At the time of the interview, 19.1% ASHAs did not have any RDTs for diagnosis and 47.7% reported not having ACT for treatment of P. falciparum malaria.
Conclusions
This study has revealed that ASHAs in the test district were not adequately trained or stocked for malaria parasite species identification and treatment, which are the major components of malaria elimination programme. This study has, therefore, revealed a need for training ASHAs on testing by RDT and proper treatment regimen for P. vivax and P. falciparum.
Similar content being viewed by others


Background
Malaria is a major public health problem in India, especially in rural/tribal areas of the country. India contributes ~ 80% of malaria cases in South East Asia Regional (SEAR) countries [1] and has the highest number of deaths outside the African continent, with approximately 1.2 billion at risk, including 183.5 million at high risk [1]. National Vector Borne Disease Control Programme (NVBDCP) has launched a national framework to eliminate malaria by 2030 [2]. The World Health Organization (WHO) and Roll Back Malaria (RBM) have also prepared materials and strategies for a malaria-free world by 2030 [3].
The National Health Mission (NHM) has focused specially on eight states that have limited infrastructure and low public health indicators. These eight Empowered Action Group (EAG) states are Bihar, Jharkhand, Madhya Pradesh, Chhattisgarh, Uttar Pradesh, Uttaranchal, Odisha and Rajasthan. One of the key components of the NHM is to provide one Accredited Social Health Activist (ASHA) who is a trained female community health activist for every 1000 population, which roughly translates to one ASHA for each village. The ASHA is selected from the village itself and accountable to it and she is trained to work as an interface between the community and the public health system.
ASHAs also act as health educators and promoters in their communities and they undergo series of modular training to acquire the necessary knowledge, skills and confidence for performing their spelled-out roles related to Maternal and Child Health (MCH), immunization, family planning, malaria and tuberculosis. Considering their reach and availability, they are also involved in diagnosis and treatment of malaria cases on a day-to-day basis. ASHA is supposed to screen suspected malaria cases, using Rapid Diagnostic Test (RDT) kits and blood slides and administer complete treatment as per the national drug policy [4, 5].
Malaria Elimination Demonstration Project (MEDP) is a first-of-its-kind public-private-partnership between the Indian Council of Medical Research (ICMR) through the National Institute of Research in Tribal Health (NIRTH), Government of Madhya Pradesh (GoMP), and the Foundation for Disease Elimination and Control of India (FDEC-India, established by Sun Pharmaceutical Industries Ltd. as a not-for-profit entity). The goal of MEDP is to demonstrate successful elimination of malaria from 1233 villages of Mandla district and use the lessons learnt for eliminating malaria from rest of Madhya Pradesh and the country.
The goal of MEDP is to demonstrate successful elimination of malaria from 1233 villages of Mandla district and use the lessons learnt for eliminating malaria from rest of Madhya Pradesh and the country. As a part of the Malaria Elimination Demonstration Project (MEDP), all ASHAs in project areas are engaged in malaria control strategies, like carrying out mass awareness, diagnosis and treatment of malaria cases.
A needs assessment on malaria for the Accredited Social Health Activists (ASHAs) of Mandla district was done to ensure that these village-based health care workers are informed and trained for malaria-specific community-based interventions, and to determine any training needs that would allow ASHAs to conduct their malaria elimination work in a reproducible and reliable manner.
Methods
Study setting
This study was carried out as part of the longitudinal Malaria Elimination Demonstration Project [6]. The district has an area of 8771 km², and is divided into nine development blocks, and 1233 villages. According to the 2011 census Mandla has a population of 1,053,522. Schedule Tribe (ST) is about 58% of total enumerated population and Gonds are primarily dominated tribe in the district.
Study design
A cross sectional survey was conducted using a fully structured, pre-tested interview schedule. The ICMR guidelines 2017 for vulnerable groups were followed as Mandla district is predominantly tribal in nature [7]. The interview schedule was designed around: (1) Diagnosis and treatment; (2) Knowledge, Attitude, and Practices; (3) Vector control; (4) Incentives; and (5) Overall health literacy, and shared for review by the experts of the Malaria Elimination Advisory Group of MEDP Mandla [6]. Following their inputs, a pilot test run was conducted and the responses were analysed for consistency, validity, and measurability. To avoid bias, the subjects were chosen using random sampling, the tool had neutrally worded questions, and was structured in different sections to avoid overlapping of information. The schedule (Additional file 1) was administered by scientists and technical staff of ICMR-NIRTH Jabalpur and MEDP Mandla. The training done in May 2017 and involved a comprehensive review of the study-design followed by mock-interviews. The survey was done in the months of June and July 2017.
Sampling technique and sample size
Out of the total 1300 ASHAs of Mandla district, 220 were selected for the interview. The sample size was estimated assuming: (1) 95% confidence; (2) 50% ASHAs had correct knowledge of malaria diagnosis and treatment; (3) 10% error; (4) design effect 2 and; (5) further inflated 15% non-response. Mandla consists of nine development blocks, namely Mandla, Narayanganj, Bijadandi, Ghughri, Mawai, Niwas, Mohgaon, Bicchia and Nainpur. The samples were drawn proportionally to number of ASHA working in a block, and within the block the ASHA were selected randomly using lottery method from the list of ASHAs provided by district health authorities.
Ethical clearance
This study was part of the Malaria Elimination Demonstration Project, which has been cleared by the Institutional Ethical Clearance (IEC) Committee of ICMR—National Institute of Research in Tribal Health (NIRTH) on 16th March 2017 (reference no. 201701/10). An informed written consent was obtained from all participants.
Data management and analysis
The data was entered in data entry software designed on CS-Pro 7.0 platform, and logical expressions and conditional statements were used to minimize the errors in data entry. The data analysis was done with Statistical Package for Social Sciences (SPSS) v25.0 (IBM SPSS Statistics, Armonk, NY: IBM Corp.) package. Univariate and bivariate analyses were performed. Means were compared using student ‘t’ test and p < 0.05 was considered for statistical significance.
Overall health literacy of ASHAs for malaria was assessed based on their awareness and perception on malaria’s sign and symptoms, mode of transmission, prevention, diagnosis and treatment. The health literacy was evaluated based on the following items: (i) how a person can get malaria, (ii) breeding sites of mosquitoes, (iii) who are at high risk of malaria, (iv) how one can avoid getting malaria, (v) common symptoms of malaria, (vi) how to diagnose malaria, (vii) minimum time limit for RDT kit to give correct result, (viii) correct identification of results from different RDTs pictures, (ix) correct identification of colour of ACT packs for different age groups, (x) identification of anti-malarial drugs, (xi) awareness about Insecticide-Treated Net (ITN)/Long-Lasting Insecticidal Net (LLIN), and (xii) number of days of administration of primaquine for treatment in case of Plasmodium falciparum and Plasmodium vivax.
Some of the questions had multiple correct answers, so overall these twelve questions had 35 correct responses. All correct responses were scored one (1) and for incorrect/ don’t know responses as zero (0). Scores for responses were added together to generate a literacy score, which varied from 4 to 29. These scores were converted to percentages ranging from minimum 11% to maximum of 83%. The percentage was categorized into three grades, namely low, medium and high, using cut-off values of < 40, 41–60 and > 60, respectively. The same technique was used for computing health literacy by Tobin et al. [8] and Muniyandi et al. [9].
Results
Socio‐demographic characteristics of respondents
ASHAs were recruited from all the nine blocks of Mandla for this study and to maintain uniformity and obtain generalizability of results, equitable distribution of samples was obtained from all the blocks. The sampled ASHAs ranged between 13 in Mohgaon block to 33 in Bichhiya block of the district. The mean age of the ASHAs was 33.3 ± 5 years. About 98% of ASHAs were married and the mean number of children per ASHA was 2.3 ± 1.0. Majority of ASHAs belonged to Scheduled Tribes (ST) (66.8%) Other Backward Castes (OBC), Scheduled Castes (SC) and General categories at 25%, 6.4% and 1.8%, respectively. Regarding the education status, 47.7% ASHAs studied up-to middle school, 23.6% to high school, 12.3% to intermediate or higher, 12.7% to primary and 3.6% to grades lesser than Primary.
As per the guidelines by the National Health Mission, minimum educational qualification for recruitment of an ASHA is tenth grade or high school. This educational condition gets relaxed in situation where suitable person with prescribed qualification is not available in the village [10]. More than half of the ASHAs (59.2%) had worked for more than 10 years in this job, 20.6% for 5–9 years and 20.2% for less than 5 years.
Training
ASHAs receive regular training for various components of their duties on a periodic basis. These trainings act as refreshers for the existing health programmes and inductive for the new ones. Almost all the ASHAs (99.5%) had received trainings on Maternal Health, but nearly half 54.9% on malaria. It was mentioned by the ASHAs that maternal care is their top priority service and malaria comes as number five out of seven priority areas (Fig. 1). ASHAs were trained by the state government on malaria tasks, which included preparing blood slide, rapid diagnostic test, and for prevention and treatment of malaria.

Percentage ASHAs received training and average ranking for activities. The green bars indicate the amount of training received in the respective area and the red line indicates the average priority given by ASHAs to the respective areas pertaining to various public health domains
Knowledge, Attitude and Practices (KAP) related to malaria
KAP assessment related to malaria was conducted for all the interviewed ASHAs. This assessment was crucial to identify the needs of ASHAs when it comes to diagnosis, treatment and prevention of malaria in the community. Most of the ASHAs knew about mosquitoes being the main agent for spread of malaria (97.7%). However, about 30% believed that malaria also spread by drinking bad water and various other misinformation for the spread of malaria (5.9%) (Fig. 2).

KAP related to Malaria: Spread of Malaria. The bar chart represents percentage of different reasons attributed to spread of Malaria by the 220 ASHAs interviewed
The majority of ASHAs (83.6%) knew that mosquitoes breed in stagnant water, however, about 12% reported fresh or running water as the site for breeding, while 3.2% informed garbage and 0.5% said dark and humid places. When asked about the method of diagnosing malaria, 91.8% ASHAs reported use of Rapid Diagnostic Test (RDT) kits, 85.9% also used blood slides, 8.2% mentioned diagnosed based on symptoms and 1.4% did not know how to diagnose it. Time limit to interpret results from the RDTs was told as 5 min by 41.4%, 15 min by 46.8%, 30 min by 8.6%, and 3.2% ASHAs did not know the answer to this question.
When ASHAs were asked to interpret various test results of the bivalent P. falciparum/P. vivax malaria RDT, except one, none could identify all the possible results correctly. Most (87.3%) correctly identified ‘negative’ result. P. vivax positive case was correctly recognized by only 15% ASHAs correctly and P. falciparum by 11%. About 60% could identify ‘mixed’ infections correctly and ‘invalid’ test results could be identified correctly by only 51.4% and 33.2% of the respondents (Fig. 3).

KAP related to Malaria: Interpretation of RDT result. The first column represents various scenarios of an RDT, the second column indicates percentage of ASHAs who correctly diagnosed the given scenario. Following these two columns, there are additional responses given by the participants. The ones highlighted in green and red are correct and incorrect/ undesirable, respectively - to the given scenario in column one
As per NVBDCP guidelines, chloroquine (CQ), primaquine (PQ) and artemisinin-based combination therapy (ACT) are the mainline recommended drugs for treatment of malaria. The study showed that 85% ASHAs used chloroquine, 44.5% ACT, 55.5% primaquine and 10% used other drugs for treatment of malaria. For the treatment of P. falciparum, PQ is given for one day only (2nd day) and for the treatment of P. vivax, PQ is given for 14 days. According to the responses received during the assessment, 52.7% and 41.8% did not dispense PQ in cases of P. falciparum and P. vivax, respectively. Whereas, 31.8% and 19.5% dispensed it for 13 days in cases of P. falciparum and P. vivax, respectively. 15% ASHAs gave PQ for 14 days in P. falciparum, which should have been given only once, and only 38.2% gave PQ for 14 days in cases of P. vivax.
Artemisinin-based combination is given for the treatment of uncomplicated P. falciparum malaria. It comes in different coloured packs for different age groups. The ASHAs were asked to identify these colored packs as recommended for specific age groups. The values highlighted in ‘yellow’ are the percentage of respondents who answered correctly. Nearly 25% ASHAs could recognize one correct ACT pack colour corresponding to the age group (Table 1). For age group 1–4 years and 15 + years, colour packs were commonly identified by the ASHAs. However, for other age groups very few could correctly identify.
Fever cases attended to by ASHAs
Fever surveillance is the primary strategy to track, test and treat malaria cases in the community. On an average, maximum fever patients were covered by ASHA from Mohgaon block (31.3 in the last 3 months) and lowest of Mawai (8.9). and Mandla (5.1). It should be noted that Mawai is the block with highest number of cases of malaria. Preceding the survey, total average number of fever cases catered by each ASHA of entire Mandla district was observed to be 2.6, 6.3 and 13.4 in last week, last month and last 3 months, respectively (Table 2).
Stock verification
A spot verification of stocks available with ASHAs was done. It was observed that 19.1% ASHAs did not have any RDTs with them. ACT packs for treatment of P. falciparum malaria were absent with almost half of the ASHAs (47.7%) and primaquine was also absent with almost half of ASHAs (46.4%) (Table 3).
Incentives
Out of the 220 ASHAs interviewed, 94% (207) said that they received monetary incentives during the last year preceding the survey. Out of which, 67% (138) mentioned that they have received it on-time. The receipt of highest incentive during the year preceding the survey and 3 months before the survey was reported highest in the block Narayanganj (19,529 INR/year and 4647 INR/3 months), while the incentive was least received at Nainpur block (5670 INR/year and 4095 INR/3 months). The average total incentive received by an ASHA of Mandla district was found to be 12,421 INR for last year and 3634 INR for last week.
Overall health literacy on malaria
Twelve questions with 35 correct responses were used to assess the level of literacy on malaria. Overall, the health literacy score varied from 4 to 29. Of the 220 ASHAs, 28.6% scored less than 40%, 53.2% scored between 41% and 60%, and only 18.2% scored more than 60%. The average health literacy scores according to respondent’s background characteristics are given in Table 4. The average health literacy score was significantly higher among older (40 or above years) ASHAs as compared to younger (less than 30 years) (18.8 vs. 15.4, p = 0.000). Similarly, middle and high school passed ASHAs had higher scores compared to illiterate/primary educated ASHAs. About 67% of interviewed ASHAs belonged to Scheduled Tribe (ST) communities, and by and large, they achieved considerably lower scores compared to Scheduled Castes (SC) and other castes.
No specific trend was observed between malaria literacy scores and primary occupation of the ASHAs. Number of trainings had substantial positive impact on the health literacy scores compared to those received less training. ASHAs who had received more than 4 rounds of training had significantly higher malaria literacy scores. ASHAs received training on malaria had considerable higher scores (16.5 vs. 11.6, p = 0.000) compared to those who had not received training. The study shows that ASHA’s age, education, caste, and training had significant impact on their health literacy scores.
Discussion
This study was performed to determine the needs-assessment of malaria diagnosis and treatment the ASHA workers of Mandla district. The findings of the study were grouped into various socio-demographic, training, incentives, knowledge, attitude, and practices (KAP) related to malaria, stock status, and overall health literacy indicators.
In this study, the mean age of the ASHAs complimented the mean ages of ASHAs in the other Indian states of Karnataka [11], Bihar (Samastipur) [12] and Odisha [13]. As per the guidelines of the National Health Mission, ASHA should be a literate woman with due preference in selection to those who are qualified up to 10th standard [5]. In the current study, 83.6% of ASHAs had completed at-least 8 years of schooling. In Karnataka, it was 90%, 82.6% in Bihar, and 85.75% in Odisha [12, 13]. The highest percentage observed in Karnataka may be due to the better literacy scores of the state [14].
Regarding the prioritization of different health programmes, the results of this study were supported by a study done by Fathima et al. in Karnataka [11], where more than 80% of the ASHAs reported MCH related work as their key activities and only 32% reported malaria as one of their important activities. However, a significantly higher readiness was observed in Odisha with 89% ASHAs trained in malaria diagnosis and treatment [13].
In this study, while majority of the ASHAs knew the method of diagnosis of malaria, the translation of this knowledge into practice was poor. Only 10% and 15% of the ASHAs could interpret the P. falciparum and P. vivax results on RDTs, respectively. These findings were contrary to a study done in Odisha, where the ability to interpret an RDT correctly was 86.8% [13], however, the unavailability of stock acted as an impediment in delivering services. In Wardha district of Maharashtra state, it was revealed that none of the ASHAs were taught about the diagnosis of malaria [15]. Another evaluation of three high endemic districts of Assam revealed that none of the ASHAs were involved in anti-malarial programme owing to lack of training and no supply of logistics [16]. In Mandla, the paradoxical combination of high-level awareness about malaria and lack of knowledge about the correct anti-malarial may be explained by a poor supply chain management system, where the ASHAs dispense the only available anti-malarial with them. The authors have demonstrated and discussed the makings of a sound supply chain management system used in the same district for malaria elimination [6].
ASHAs could not recognize correctly the age group-wise color packs of ACTs. However, with only 25% of ASHAs who could identify Yellow (1–4 years) ACT packs correctly. It was noticed that all ASHAs could not correctly identify the age-group of the colour-coded ACT combo-packs. Additionally, all ASHAs did not have adequate literacy levels to read the age-groups on the packs. It is recommended by the authors that along with the colour of packaging, the age-group may also be mentioned in the regional language on the packaging. It is also suggested that periodical assessments and refresher trainings of the ASHAs should be done similar to the methodology explained in a training study for malaria elimination in the same district [17].
Conclusions
This study has revealed that ASHAs of Mandla district are not fully trained on malaria diagnosis and treatment. In the study district, most of ASHAs reported diagnosis of malaria through RDTs and blood slides, but only 10–15% could recognize P. vivax and P. falciparum RDTs correctly. ASHA’s awareness to ACT colour packs for different age group was also poor and PQ doses were not properly administered in case of P. vivax and P. falciparum malaria cases. Lack of stock in abundance could also be a major barrier in diagnosing and administration of wrong type of anti-malarial to the patients. There is strong need for fresh and continuous training of ASHAs on RDTs and treatment regimen for P. vivax and P. falciparum, failing which, the goal of malaria elimination in India could be threatened.
Availability of data and materials
We have reported all the findings in this manuscript. The hardcopy data is stored at MEDP Office in Mandla, Madhya Pradesh and Indian Council of Medical Research-National Institute of Research in Tribal Health (ICMR-NIRTH), Jabalpur, Madhya Pradesh. Softcopy data is available on the project server of MEDP hosted by Microsoft Azure. If anyone wants to review or use the data, they should contact: Dr. Altaf A. Lal. Project Director – Malaria Elimination Demonstration Project, Mandla. Foundation for Disease Elimination and Control of India, Mumbai, India 482003. E mail: altaf.lal@sunpharma.com.
Abbreviations
- ACT:
-
Artemisinin-based Combination Therapy
- ASHA:
-
Accredited Social Health Activist
- CQ:
-
Chloroquine
- EAG:
-
Empowered Action Group
- FDEC:
-
Foundation for Disease Elimination and Control of India
- GoMP:
-
Government of Madhya Pradesh
- ICMR:
-
Indian Council of Medical Research
- IEC:
-
Institutional Ethical Committee
- KAP:
-
Knowledge, Attitude and Practices
- MCH:
-
Maternal and Child Health
- MEDP:
-
Malaria Elimination Demonstration Project
- NHM:
-
National Health Mission
- NIRTH:
-
National Institute of Research in Tribal Health
- NVBDCP:
-
National Vector Borne Disease Control Programme
- OBC:
-
Other Backward Caste
- PQ:
-
Primaquine
- RBM:
-
Roll Back Malaria partnership to end malaria
- RDT:
-
Rapid Diagnostic Test
- SC:
-
Scheduled Caste
- SEAR:
-
South East Asia Regional
- SPSS:
-
Statistical Package for Social Sciences
- ST:
-
Scheduled Tribe
- WHO:
-
World Health Organization
References
WHO. World Malaria Report. Geneva: World Health Organization; 2018. https://www.who.int/malaria/publications/world-malaria-report-2018/report/en/. Accessed 28 Jan 2021.
National Framework. for Elimination of Malaria in India 2016-30. NVBDCP.
Action RBM. Investment to defeat Malaria 2016–2030 (AIM)—for a malaria-free world. Geneva: World Health Organization; 2015.
Guidelines for Involvement of ASHAs in VBDs. NVBDCP. https://nvbdcp.gov.in/WriteReadData/l892s/Guidelines-Involvement-ASHAs.pdf. Accessed 28 Jan 2021.
MoH&FW. About accredited social health activist (ASHA): national health mission; 2014. http://nhm.gov.in/communitisation/asha/about-asha.html. Accessed 28 Jan 2021.
Rajvanshi H, Bharti PK, Nisar S, Jain Y, Jayswar H, Mishra AK, et al. Study design and operational framework for a community based Malaria Elimination Demonstration Project in 1233 villages of district Mandla, Madhya Pradesh. Malar J. 2020;19:410.
Behera SK, Das S, Xavier AS, Selvarajan S, Anandabaskar N. Indian Council of Medical Research’s National Ethical Guidelines for biomedical and health research involving human participants: the way forward from 2006 to 2017. Perspect Clin Res. 2019;10:108–14.
Tobin EA, Okojie P-W, Isah EC. Community knowledge and attitude to pulmonary tuberculosis in rural Edo state, Nigeria. Ann Afr Med. 2013;12:148.
Muniyandi M, Rao V, Bhat J, Yadav R, Sharma R, Bhondeley M. Health literacy on tuberculosis amongst vulnerable segment of population: special reference to Saharia tribe in central India. Indian J Med Res. 2015;141:640.
About Accredited Social Health Activist (ASHA)—National Health Mission: Ministry of Health and Family Welfare, Government of India; 2014. http://nhm.gov.in/communitisation/asha/about-asha.html.
Fathima FN, Raju M, Varadharajan KS, Krishnamurthy A, Ananthkumar S, Mony PK. Assessment of ‘accredited social health activists’—a national community health volunteer scheme in Karnataka State, India. J Health Popul Nutr. 2015;33:137–45.
Swadhin Kumar J. Assessment of accredited social health activist on postnatal care service, Samastipur district, Bihar. SCTIMST, 2017.
Hussain MA, Dandona L, Schellenberg D. Public health system readiness to treat malaria in Odisha State of India. Malar J. 2013;12:351.
Census. 2011, Chapt. 6 (State of Literacy). https://censusindia.gov.in/2011-prov-results/data_files/india/Final_PPT_2011_chapter6.pdf. Accessed 28 Jan 2021.
Gosavi S, Raut A, Deshmukh P, Mehendale A, Garg B. ASHAs awareness and perceptions about their roles and responsibilities: a study from rural Wardha. J Mahatma Gandhi Inst Med Sci. 2011;16:1–8.
Prasad H. Evaluation of malaria control programme in three selected districts of Assam, India. J Vector Borne Dis. 2009;46:280.
Rajvanshi H, Nisar S, Bharti PK, Jayswar H, Mishra AK, Sharma RK, et al. Significance of training, monitoring and assessment of malaria workers in achieving malaria elimination goal of Malaria Elimination Demonstration Project. Malar J. 2021;20:27.
Acknowledgements
We dedicate this paper to late Dr. Neeru Singh, past Director of ICMR- National Institute of Research in Tribal Health (ICMR-NIRTH), Jabalpur, who was the leading force in establishing this Malaria Elimination Demonstration Project. We are thankful to Director NVBDCP Dr. Neeraj Dhingra for his leadership and insights. We are thankful to the former Director General of ICMR and Secretary Department of Health Research, Dr. Soumya Swaminathan and present DG ICMR and Secretary Department of Health Research. Dr. Balram Bhargava for their support, insights and guidance. We are also thankful to the former Principal Secretary Health Mrs. Gauri Singh. the present Principal Secretary Health Dr. Pallavi Govil, and Health Commissioner Mr. Prateek Hajela, for their constant support for conduct of work in Mandla. We are also thankful to the District Magistrate of Mandla, Chief Medical and Health Officer Mandla, Police Superintendent of Mandla, CEO Zila Panchayat, Panchayat heads, ASHAs, ANMs for their encouragement and support in daily activities of MEDP. We would also like to thank District Malaria Officer and DVBD Consultant for attending training meetings and providing RDTs and ACTs for the project. The project could not have achieved its results without the support from Board of Sun Pharmaceuticals, FDEC India, core team of MEDP, community members, and media of Mandla district. The manuscript has been approved by the Publication Screening Committee of ICMR - NIRTH Jabalpur and assigned with reference number ICMR-NIRTH/PSC/13/2020.
Funding
This study is part of the Malaria Elimination Demonstration Project, which is a public-private-partnership between Government of Madhya Pradesh, India, Indian Council of Medical Research, New Delhi, India and Foundation for Disease Elimination and Control of India. All three parties have supported the work.
Author information
Authors and Affiliations
Contributions
KBS, PKB, AAL conceptualized the study; KBS, RKS, PKB designed the study protocol; SN, MMS, AV, NS carried out the data collection; RKS, HR analysed the data; HR drafted the manuscript; PKB, RKS, AKM, MMS, KBS, AD, HJ, SLW, HK, AAL critically reviewed the manuscript. All authors reviewed and approved the final manuscript.
Corresponding author
Ethics declarations
Consent for publication
All authors have given their consent for publication.
Competing interests
The authors declare that they have no competing interests.
Disclaimer
The views represented by the author—Suman L. Wattal are solely in her personal capacity and do not necessarily reflect the views of NVBDCP, New Delhi.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
ASHA needs-assessment tool for malaria elimination used in the study.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Rajvanshi, H., Saha, K.B., Shukla, M.M. et al. Assessment of ASHA for knowledge, diagnosis and treatment on malaria in Mandla district of Madhya Pradesh as part of the malaria elimination demonstration project. Malar J 20, 78 (2021). https://doi.org/10.1186/s12936-021-03610-8
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12936-021-03610-8