
Abstract
Background
The Dermatology Life Quality Index (DLQI) is the most commonly used instrument for clinical evaluation of the impact on health-related quality of life (HRQOL) in dermatological research protocols. The DLQI’s classical psychometric properties have been considered adequate in validation studies from several countries. However, the structure of the DLQI is a matter of discussion, especially concerning the dimensionality and informative properties of its questions according to the item response theory (IRT).
Methods
Pooled data from studies in Brazil that utilized the DLQI to assess HRQOL in 14 dermatoses were reanalyzed. Classical psychometrical analysis, dimensionality assessment through parallel analysis and IRT (Samejima’s ordinal model) analysis were performed.
Results
The sample consisted of 1286 patients with a mean age of 47 years (SD = 16), and the proportion of women was 59% (765). The DLQI scores ranged from 0 to 29, with a median (p25–p75) of 5 (2–11). All items indicated significant correlations with the total DLQI score (rho > 0.54). The Cronbach’s alpha result was 0.90 (CI 95% 0.89–0.91). Parallel analysis indicated a unidimensional factor structure. According to IRT analysis, items q6 (sports) and q7 (work/study) exhibited insufficient fit to the model (p < 0.01), while the items that indicated the best discrimination and information functions were q2 (embarrassment), q3 (shopping/gardening), q4 (clothing) and q5 (social/leisure). The ordination of the scores was confirmed for all items. Most items revealed non-uniform behavior according to sex, age and type of disease.
Conclusions
The DLQI exhibits adequate psychometric reliability and a unidimensional structure for assessing HRQOL in Brazilian dermatological patients. The DLQI’s performance varies in the assessment of HRQOL in heterogeneous samples.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Most dermatologic diseases are not life-threatening or extremely symptomatic; however, they affect an individual’s social, affective and emotional functioning. Thus, patient-oriented outcomes are important in measuring disease burden and substantiating therapeutic efficacy and decisions on treatment. The appropriateness of the instruments assessing health-related quality of life (HRQOL) rest on their validity, consistency, reliability, dimensionality and invariance through subgroups [1]. The Dermatology Life Quality Index (DLQI) is the most commonly used instrument for the HRQOL evaluation and follow-up of patients with dermatological diseases under research protocols; it is also part of the decision-making algorithm for several treatment guidelines. Nevertheless, there are concerns regarding its performance, which we examine [2,3,4].
The DLQI is a short HRQOL questionnaire on general dermatological diseases. It was published in 1994 by Finlay and Khan [5], and it has been translated into more than 90 languages and applied to research on more than 40 dermatoses. It is a practical and straightforward instrument that has performed well in several studies [6,7,8,9,10]. In 2004, Martins et al. validated the DLQI for the Portuguese language in Brazil (DLQI-BRA) [11, 12].
The DLQI was developed from interviews with 120 patients with different dermatological diseases, in which the patients highlighted aspects that affected their daily lives. From this qualitative approach, the 10 most important aspects were selected. To validate the adequacy of the psychometric properties, 200 dermatological patients and 100 controls were assessed [5]. Theoretically, the DLQI is a scale developed as a unidimensional reflexive instrument to assess dermatologic diseases’ effects on HRQOL.
The final version of the DLQI consists of 10 items arranged in six categories: symptoms and feelings (questions 1 and 2), daily activity (3 and 4), leisure (5 and 6), work or study (7), interpersonal relationships (8 and 9) and treatment (10). The questions evaluate an individual’s perception of the disease over the past week. The possible answers for each item are “very much,” “a lot,” “a little,” “not at all” and “not relevant,” with a respective ordinal grade of 0 to 3. Item 7 is divided into two stages: the first stage questions whether skin disease prevents the individual from working; if the answer is no, the next step asks how much the disease interferes with his or her work [13]. The total score can vary from 0 (no impact on HRQOL) to 30 (maximum impact on HRQOL) [5, 10]. Conventionally, DLQI scores are interpreted from the sum of the indices of the 10 items evaluated, such as “no impairment of HRQOL” (0–1), “mild impairment” (2–5), “moderate” (6–10), “severe” (11–20) or “very severe impairment” (21–30) [14].
The psychometric properties regarding classical test theory have been considered appropriate for evaluating HRQOL in patients with dermatological diseases in studies in several countries. However, the structure of the DLQI is currently a matter of discussion, especially regarding the informative properties of its items according to the item response theory (IRT) [15,16,17].
Recent studies have not recognized the unidimensionality of the DLQI. Moreover, differential item functioning (DIF) analysis reveals that the same item presents different behavior according to age, sex and the type of dermatological disease [13, 18,19,20].
The content validity of the DLQI has been questioned due to the instrument’s insufficient evaluation of emotional and psychological aspects, which are fundamental in dermatology, especially in asymptomatic but stigmatizing diseases, such as vitiligo, congenital nevus, melasma and alopecia [1, 21,22,23,24]. Furthermore, the plurality of dermatological diseases affects different dimensions of HRQOL. The DLQI’s unidimensional proposal may not capture all the nuances in different dermatoses.
This study aims to investigate the DLQI’s internal consistency, dimensionality, discrimination and performance in a subgroup analysis of a Brazilian population sample.
Methods
We performed a reanalysis of pooled data from cross-sectional studies in Brazil that utilized the DLQI-BRA to assess the HRQOL impact of 14 dermatoses on 1286 patients [25,26,27,28,29,30,31,32,33]. Furthermore, sex, age, educational status and physical and psychological dimensions of the skin disorders were evaluated. The authors of these original studies provided permission to reanalyze the data, and all these projects were approved by their institutional review boards.
The dermatoses were classified (by author consensus) according to characteristic physical symptoms and psychological or social domains (Table 1) to test the performance of the DLQI items and scores in different types of skin disorders. This classification was chosen based on the dimensions of another validated HRQOL multidimensional scale (Skindex-17) [34].
As the score of the DLQI results from the sum of its 10 items, the assurance of unidimensionality is crucial. The DLQI dimensionality was assessed by Horn’s parallel analysis method, using a random matrix (sphericity calculated after a Monte Carlo simulation method with 99% reliability). Additionally, the unidimensional congruence (UniCo), explained common variance (ECV) and mean of item residual absolute loadings (MIREAL) were assessed, and the Hull method was performed [35,36,37,38,39,40]. The internal consistency of the DLQI was estimated by Cronbach’s alpha and its 95% confidence interval (CI 95%). Furthermore, McDonald’s ordinal omega and the greatest lower bound to reliability were assessed [41,42,43]. Inter-item and item-total correlations were measured by polychoric correlations and Spearman’s rho coefficients [44,45,46].
The normality of the data distribution was assessed by the Kolmogorov-Smirnov (Lilliefors) test. Quantitative variables are expressed as means (standard deviation) or medians and quartiles (p25-p75) [47].
To analyze the informativity of each item, the DLQI was evaluated according to the IRT through a graded response (Samejima’s) model [48]. The adjustment of the model was assessed by the Akaike information criterion (AIC), the Bayesian information criterion (BIC), the comparative fit index (CFI), the root mean square error of approximation (RMSEA) and X2. The coefficients for each item were then extracted.
Another important issue to assess is related to invariance in the measurement of people with equivalent abilities. The item invariability was assessed through DIF analysis by ordinal logistic regression for each item according to sex, age group (< 30, 30–60 and > 60 years old) and the characteristics of the disease [13, 49]. The total DLQI score was tested regarding these covariates by a generalized linear model (gamma regression).
The sample was a result of pooled data from 14 cross-sectional studies in Brazil that utilized the DLQI-BRA to assess HRQOL [25,26,27,28,29,30,31,32,33]. The sample size (n = 1286) was assumed to be sufficient in the IRT parameter estimation, dimensionality assessment and DIF and generalized linear model analyses, adjusted for up to eight dummy variables [50,51,52]. All data was related to completely filled questionnaires; there was no available information regarding the number of distributed questionnaires or the percentage of incomplete questionnaires in each original study.
Data were analyzed with IBM SPSS 25.0; Factor [53] and R (mirt package) [54]. Significance was set as two-tailed p < 0.05.
Results
The main clinical and demographic data from the sample are displayed in Table 2. The DLQI scores ranged from 0 to 29, with a median of 5 (p25 = 2; p75 = 11) (Fig. 1). According to the predefined categories of HRQOL impairment, 310 (24%) participants were classified as having no impairment, 383 (30%) were classified as having a mild impairment, 247 (19%) as having a moderate impairment, 248 (19%) as having a severe impairment and 98 (8%) as having a very severe impairment.

Histogram of DLQI-BRA scores (n = 1286)
Inter-item correlations were indicated for all items (> 0.3), and correlations between items and DLQI scores were found (Table 3). Sexual difficulties (q9) indicated the lowest item-total correlation (rho = 0.54), while shopping/home activities and social/leisure (q3 and q5) revealed the highest correlations (rho = 0.82).
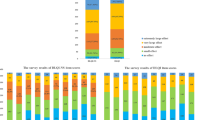
The distribution of item grades was asymmetrical for most items (Fig. 2), as was that of the total DLQI scores (Fig. 1). In more than 67% of cases, the rating of items q6 through q10 was “no” or “not at all.”

Distribution of item grades of the sample (n = 1286)
Horn’s parallel analysis and the scree plot pattern indicated unidimensionality for the DLQI (Fig. 3). The UniCo result was 0.99 (CI 95% 0.98–0.99), ECV was 0.91 (CI 95% 0.90–0.93) and MIREAL was 0.19 (CI 95% 0.16–0.21). Hull analysis also corroborated the unidimensional structure (data not shown). Moreover, when a second factor was extracted, the total explained variation increased from 63 to 71%.

Diagram of the eigenvalues versus the number of factors, showing only one factor to the point of inflection and stabilization of the curve: analysis of scree plot; and before the crossing of the parallel analysis with a random spherical matrix: Horn’s parallel analysis (n = 1286; Kaiser-Meyer-Olkin test = 0.92; Bartlett’s statistic = 6219.9, df = 45; p < 0.01)
The internal consistency of the DLQI (Cronbach’s alpha) was 0.90 (CI 95% 0.89–0.91), which varied from 0.72 to 0.91 according to the dermatoses (Table 2). If any item was excluded, Cronbach’s alpha for the total sample ranged from 0.87 to 0.89 (data not shown). Internal consistency was also greater than 0.8, as assessed by McDonald’s ordinal omega (0.90) and the greatest lower bound to reliability (0.91).
The DLQI was tested according to the ordinal IRT for four models: Samejima’s graded response model, the generalized partial credit model (GPCM), the graded ratings scale model (GRSM) and the Rasch rating scale model (RSM). Samejima’s graded response model produced the best adjustment (AIC = 22.157; CFI = 0.98; RMSEA = 0.05; X2 = 318.9; p = 0.22).
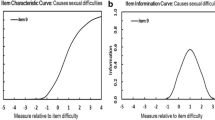
The coefficients from the items and the item-fit parameters are listed in Table 4. Items q6 and q7 exhibited unsatisfactory fit to the model (p < 0.01). All items demonstrated good discrimination (a > 0.8), and the items that disclosed the best discrimination (a > 2) and information functions were q2, q3, q4 and q5. The difficulty of the items followed a suitable ordination according to Samejima’s graded response model; however, the RSM and GRSM models revealed irregularities in the ordination of the response categories (data not shown). Items q1 and q2 (symptoms and feelings) identified subjects with lower levels of HRQOL impact (b1 < − 0.2), though item q9 (sexual life) identified only higher levels of HRQOL impact (b1 > 1.0).
Items were submitted to the analysis of invariance (DIF) according to sex, age group (< 30, 30–60 and > 60 years old) and type of disease (symptomatic or psychosocial). Several items disclosed non-uniform behavior according to sex, age and disease type (Table 5) after multivariate adjustment.
Discussion
The DLQI proved to be a suitable instrument with which to evaluate HRQOL in a Brazilian population; however, there were psychometric concerns regarding the DLQI’s validity for different patterns of disease and its item composition.
The dermatological diseases studied in this work are among the most prevalent in Brazil, according to a recent survey [55]. The DLQI produced a wide variation in HRQOL scores, with a predominance of mild and moderate HRQOL impairment (49% of scores were between 2 and 10). This is characteristic of general dermatological diseases that have little impact on HRQOL [11, 13, 16, 23,24,25,26, 29,30,31,32,33, 56,57,58,59,60]. As such, highly discriminative instruments are required in this range of mild diseases. To date, this is the largest South American study on DLQI psychometrics.
The diseases with the highest DLQI score were urticaria, bullous dermatoses and hidradenitis. These are diseases whose physical symptoms are highly evident, demonstrating that the DLQI adequately assesses concrete discomforts [1]. Asymptomatic diseases, such as vitiligo, alopecia and melasma, can manifest as a different structural pattern of DLQI items. Some authors have found that the DLQI is unable to adequately measure the impact of mild diseases on patients’ HRQOL, which may, for example, present as lower responsiveness [16, 31]. In our study, five items presented a “ground” effect, which may have exacerbated this problem.
In 8 of the 10 questions, response options include “not at all” and “not relevant,” both of which are graded zero. Though these options contribute identically to the final score, they represent different meanings. Moreover, some items, such as q6 (sports) and q9 (sexual life), may elicit different response patterns based on the questioning period, since the instrument evaluates only the last 7 days [13, 16, 24, 61]. A recent proposal to adjust the total DLQI score of the questionnaire for the number of “not relevant” responses (DLQI-R) has the potential to improve the discriminatory power of the instrument, though a systematic psychometric study on item performance has not been performed [61, 62].
The correlation between item grades and the total score was adequate, except for item q9 (sexual life). Previous studies have found this item problematic [20, 61]. In a Chinese study that evaluated the DLQI among patients with neurodermatitis, q9 did not fit the model. The authors hypothesized that such a problem could be explained by the cultural difficulty of discussing this matter within the population [20]. Another possible explanation for this item’s performance is that the survey was conducted among adolescents or the elderly, for whom sexual activity is not a highly present element in daily life [61]. Moreover, IRT analysis indicates that q9 is most affected with severe HRQOL impact.
Due to the inter-item correlation, q9 must be carefully evaluated in different populations, since its exclusion from the questionnaire would make comparisons with other studies unfeasible. A practical proposal to address this would be the inclusion of a pre-assessment of the relevance of sexual activity in the participants’ lives, allowing the separation of groups on this issue, as occurs with item q7, related to work and study activities. Another proposal is the adaptation of the questionnaire scores (DLQI-R) that resizes the weight of all items marked “not relevant” [61, 62].
The current literature questions the dimensionality of the instrument [13, 18]. Our results evidence unidimensionality using the Horn parallel analysis and additional methods, which confirm the dimensionality of the original structure, as proposed by the author [5, 35,36,37]. The proper use of exploratory factor analysis for ordinal data (using polychoric correlations), rather than continuous data, can justify this previous divergence in comparison to some more robust methods [63].
The IRT analysis more accurately evaluated the HRQOL assessment questionnaires than the classical test theory psychometrics. The analysis of the DLQI by Rasch models among patients with psoriasis, atopic dermatitis and neurodermatitis revealed the lack of adjustability of some items, even though studies on the classical theory of the tests have indicated their adequacy [16, 20]. The Rasch-based analysis for ordinal data does not consider the independence of the discrimination (a-parameter) for each item, reducing the flexibility of the model.
In our study, Samejima’s graded response model produced the best performance in the IRT analysis and evidenced insufficient adjustment for items q6 (sports) and q7 (working/studying). The other studies that used Rasch models did not describe them in detail, from which it can be inferred that the differences in the fit of the items may be due to the underlying model [13, 16, 19, 20]. Additionally, when our data were analyzed according to other poorly fitting models (e.g., RSM and GRSM), the ordination of all items was not verified (data not shown). The practice of sports (q6) and work (q7) among the patients – especially those who were older and retired – was less likely to affect HRQOL. These particularities of different dermatosis and different population groups should be considered when using the DLQI for the assessment of HRQOL in specific circumstances.
Items q2 (embarrassment), q3 (shopping/gardening), q4 (clothing) and q5 (social/leisure activities) presented the best performance, suggesting that they address the fundamental elements of the different dermatoses studied. These items refer to activities and situations in which, in most cases, there is a certain degree of skin exposure, which could explain the discomfort experienced by patients with skin diseases. In this sample, symptoms (q1) and feelings (q2) were the first HRQOL aspects affected by skin diseases, while sexual life (q9) was the last.
The presence of DIF is a recurrent finding in recent literature on the DLQI. In a study that evaluated patients with psoriasis and atopic dermatitis, DIF was found for age, gender and type of disease [16]. In this study, several items exhibited DIF, which suggests that the DLQI does not adequately assess HRQOL in individuals with specific characteristics. Moreover, some characteristics that affect HRQOL are directly associated with groups of patients and diseases, justifying the behavior of DIF when analyzed as a single disorder. These elements indicate that caution should be exercised in the comparative evaluation of HRQOL in different population subgroups (e.g., men vs. women) and diseases with different characteristics (e.g., with predominantly physical complaints vs. psychological impact) [64].
The DIF verified between the elderly and the youth could also be explained by the difference in the range of diseases that affect each age group or the type of physical activity performed. In a study on hand eczema, DIF was found for age in q7 (influence of dermatosis at work), which could be explained by the older population being retired [19]. In this study, DIF was also evidenced for gender in q5 (influence in sports practice), which may demonstrate male predominance in sports practice in that population [19].
A Chinese study on neurodermatitis found that people who are younger than 35 years experienced less impact on HRQOL than those over 35 [20]. In another Chinese study with 9845 patients, Rasch’s analysis showed DIF for disease (q1, q2 and q5) and geographic location (q7, work/study), suggesting that the comparison between patients with different diseases can be limited [13].
Another study comparing the performance of the DLQI between different populations revealed DIF among cultures, despite using a questionnaire validated for the local language. Disease was found to present differently in interpretations of HRQOL among different cultures [17].
The ordering of the responses (grades within items) has also been questioned by other investigators. This may influence clinical decisions because some therapeutic protocols adopt the DLQI score, for which linearity is fundamental. Our results indicate a high correlation between the items and the total score. Furthermore, the ordering was adequate by IRT analysis, probably due to the use of Samejima’s model that disclosed greater adjustment to the data, which had not been used by previous studies (e.g., the Rasch-based model).
As the main contribution, this study confirms the DLQI is suitable for use in the Brazilian population. However, despite its unidimensionality, most items revealed non-uniform behavior according to sex, age and type of disease. Cautious interpretation is required to interpret a final score, especially if assessing or comparing heterogeneous samples. Under those conditions, the difference in HRQOL measures can be influenced by population characteristics rather than the disease burden. In practice, the best performance of the DLQI is achieved in assessing one kind of disease in samples with low variability in age and, preferably, of the same sex.
The strength of this study relies on the substantial sample and the diversity of dermatological diseases assessed, representing the most prevalent dermatoses among the Brazilian population [55]. Limitations are related to the unknown percentage of incomplete data or refusal to participate in the original studies, as well as which and how many items were marked “not at all” and “not relevant,” as it was a reanalysis of pooled data.
Further psychometric comparison of the DLQI with other multidimensional generic dermatological HRQOL questionnaires (e.g., Skindex-16), as well as testing of the DLQI’s responsiveness, temporal stability and exploration of its network structure (network analysis), are needed. Furthermore, the importance of the “not relevant” and “not at all” grades to the DLQI’s overall performance should be further assessed.
Conclusions
The DLQI exhibits adequate reliability and a unidimensional structure for assessing HRQOL in Brazilian dermatological patients. Item performance varies according to sex, age and type of dermatosis, suggesting that these factors can result in different indications in the HRQOL assessment of patients. Researchers should be aware of these points when using the DLQI for evaluating HRQOL. Therefore, it is important to consider not only the numerical result of the DLQI in clinical decisions but also or the context of the patient’s responses that may affect the final score.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- AIC:
-
Akaike information criterion
- BIC:
-
Bayesian information criterion
- CFI:
-
Comparative fit index
- DIF:
-
Differential item functioning
- DLQI:
-
Dermatology Life Quality Index
- DLQI-BRA:
-
DLQI for the Portuguese language in Brazil
- ECV:
-
Explained Common Variance
- GPCM:
-
Generalized partial credit model
- GRSM:
-
Graded ratings scale model
- HRQOL:
-
Health-related quality of life
- IRT:
-
Item response theory
- MIREAL:
-
Mean of Item Residual Absolute Loadings
- RMSEA:
-
Root mean square error of approximation
- RSM:
-
Rasch rating scale model
- UniCo:
-
Unidimensional Congruence
References
Nijsten T. Dermatology life quality index: time to move forward. J Invest Dermatol. 2012;132:11–3.
Sanchez J, Zakzuk J, Cardona R. Evaluation of a guidelines-based approach to the treatment of chronic spontaneous Urticaria. J Allergy Clin Immunol Pract. 2018;6:177–82 e1.
Baker C, Mack A, Cooper A, et al. Treatment goals for moderate to severe psoriasis: an Australian consensus. Australas J Dermatol. 2013;54:148–54.
Chernyshov PV, Tomas-Aragones L, Manolache L, et al. Which acne treatment has the best influence on health-related quality of life? Literature review by the European academy of dermatology and venereology task force on quality of life and patient oriented outcomes. J Eur Acad Dermatol Venereol. 2018;32:1410–9.
Finlay AY, Khan GK. Dermatology life quality index (DLQI)--a simple practical measure for routine clinical use. Clin Exp Dermatol. 1994;19:210–6.
He Z, Lu C, Basra MK, et al. Psychometric properties of the Chinese version of dermatology life quality index (DLQI) in 851 Chinese patients with psoriasis. J Eur Acad Dermatol Venereol. 2013;27:109–15.
Mork C, Wahl A, Moum T. The Norwegian version of the dermatology life quality index: a study of validity and reliability in psoriatics. Acta Derm Venereol. 2002;82:347–51.
Ozturkcan S, Ermertcan AT, Eser E, et al. Cross validation of the Turkish version of dermatology life quality index. Int J Dermatol. 2006;45:1300–7.
Takahashi N, Suzukamo Y, Nakamura M, et al. Japanese version of the dermatology life quality index: validity and reliability in patients with acne. Health Qual Life Outcomes. 2006;4:46.
Lewis V, Finlay AY. 10 years experience of the dermatology life quality index (DLQI). J Investig Dermatol Symp Proc. 2004;9:169–80.
Ferraz LB, Almeida FA, Vasconcellos MR, et al. The impact of lupus erythematosus cutaneous on the quality of life: the Brazilian-Portuguese version of DLQI. Qual Life Res. 2006;15:565–70.
Martins GA, Arruda L, Mugnaini ASB. Validation of life quality questionnaires for psoriasis patients. An Bras Dermatol. 2004;79:521–35.
He Z, Lo Martire R, Lu C, et al. Rasch analysis of the dermatology life quality index reveals limited application to Chinese patients with skin disease. Acta Derm Venereol. 2018;98:59–64.
Hongbo Y, Thomas CL, Harrison MA, et al. Translating the science of quality of life into practice: what do dermatology life quality index scores mean? J Invest Dermatol. 2005;125:659–64.
Poor AK, Brodszky V, Pentek M, et al. Is the DLQI appropriate for medical decision-making in psoriasis patients? Arch Dermatol Res. 2018;310:47–55.
Twiss J, Meads DM, Preston EP, et al. Can we rely on the dermatology life quality index as a measure of the impact of psoriasis or atopic dermatitis? J Invest Dermatol. 2012;132:76–84.
Nijsten T, Meads DM, de Korte J, et al. Cross-cultural inequivalence of dermatology-specific health-related quality of life instruments in psoriasis patients. J Invest Dermatol. 2007;127:2315–22.
Nijsten T, Meads DM, McKenna SP. Dimensionality of the dermatology life quality index (DLQI): a commentary. Acta Derm Venereol. 2006;86:284–5.
Ofenloch RF, Diepgen TL, Weisshaar E, et al. Assessing health-related quality of life in hand eczema patients: how to overcome psychometric faults when using the dermatology life quality index. Acta Derm Venereol. 2014;94:658–62.
Liu Y, Li T, An J, et al. Rasch analysis holds no brief for the use of the dermatology life quality index (DLQI) in Chinese neurodermatitis patients. Health Qual Life Outcomes. 2016;14:17.
Chren MM, Lasek RJ, Quinn LM, et al. Convergent and discriminant validity of a generic and a disease-specific instrument to measure quality of life in patients with skin disease. J Invest Dermatol. 1997;108:103–7.
Chren MM, Lasek RJ, Quinn LM, et al. Skindex, a quality-of-life measure for patients with skin disease: reliability, validity, and responsiveness. J Invest Dermatol. 1996;107:707–13.
Maranzatto CF, Miot HA, Miot LD, et al. Psychometrican analysis and dimensional structure of the Brazilian version of melasma quality of life scale (MELASQoL-BP). An Bras Dermatol. 2016;91:422–8.
Pollo CF, Miot LDB, Meneguin S, et al. Factors associated with quality of life in facial melasma: a cross-sectional study. Int J Cosmet Sci. 2018;40:313–6.
Penha MA, Farat JG, Miot HA, et al. Quality of life index in autoimmune bullous dermatosis patients. An Bras Dermatol. 2015;90:190–4.
Silvares MR, Fortes MR, Miot HA. Quality of life in chronic urticaria: a survey at a public university outpatient clinic, Botucatu (Brazil). Rev Assoc Med Bras (1992). 2011;57:577–82.
Boza JC, Kundu RV, Fabbrin A, et al. Translation, cross-cultural adaptation and validation of the vitiligo-specific health-related quality of life instrument (VitiQoL) into Brazilian Portuguese. An Bras Dermatol. 2015;90:358–62.
Nunes DH, Frode TS. Quality of life in basal cell carcinoma patients in Brazil: a pilot cross sectional study. Dermatol Surg. 2013;39:620–6.
Camargo CC, D'Elia MPB, Miot HA. Quality of life in men diagnosed with anogenital warts. An Bras Dermatol. 2017;92:427–9.
Borges APP, Pelafsky VPC, Miot LDB, et al. Quality of life with ingrown toenails: a cross-sectional study. Dermatol Surg. 2017;43:751–3.
Shimizu GKM, Wedy GF, Schaefer LV, et al. Translation into Portuguese language (Brazil), transcultural adaptation and validation of the quality of life questionnaire in female pattern hair loss (WAA-QoL-BP). An Bras Dermatol. 2018;93:701–6.
Ianhez M, Pinto SA, Miot HA, et al. A randomized, open, controlled trial of tretinoin 0.05% cream vs. low-dose oral isotretinoin for the treatment of field cancerization. Int J Dermatol. 2019;58:365–73.
Gobo-Oliveira M, Pigari VG, Ogata MS, et al. Gabapentin versus dexchlorpheniramine as treatment for uremic pruritus: a randomised controlled trial. Eur J Dermatol. 2018;28:488–95.
Nijsten TE, Sampogna F, Chren MM, et al. Testing and reducing skindex-29 using Rasch analysis: Skindex-17. J Invest Dermatol. 2006;126:1244–50.
Horn JL. A rationale and test for the number of factors in factor analysis. Psychometrika. 1965;30:179–85.
O'Connor BP. SPSS and SAS programs for determining the number of components using parallel analysis and velicer's MAP test. Behav Res Methods Instrum Comput. 2000;32:396–402.
Lorenzo-Seva U, Timmerman ME, Kiers HA. The Hull method for selecting the number of common factors. Multivar Behav Res. 2011;46:340–64.
Timmerman ME, Lorenzo-Seva U. Dimensionality assessment of ordered polytomous items with parallel analysis. Psychol Methods. 2011;16:209–20.
Calderon Garrido C, Navarro Gonzalez D, Lorenzo Seva U, et al. Multidimensional or essentially unidimensional? A multi-faceted factor-analytic approach for assessing the dimensionality of tests and items. Psicothema. 2019;31:450–7.
Ferrando PJ, Lorenzo-Seva U. Program FACTOR at 10: origins, development and future directions. Psicothema. 2017;29:236–40.
Sheng Y, Sheng Z. Is coefficient alpha robust to non-normal data? Front Psychol. 2012;3:34.
Deng L, Chan W. Testing the difference between reliability coefficients alpha and omega. Educ Psychol Meas. 2017;77:185–203.
Trizano-Hermosilla I, Alvarado JM. Best alternatives to Cronbach's alpha reliability in realistic conditions: congeneric and asymmetrical measurements. Front Psychol. 2016;7:769.
Sijtsma K. On the use, the misuse, and the very limited usefulness of Cronbach's alpha. Psychometrika. 2009;74:107–20.
Jin S, Yang-Wallentin F. Asymptotic robustness study of the Polychoric correlation estimation. Psychometrika. 2017;82:67–85.
Miot HA. Correlation analysis in clinical and experimental studies. J Vasc Bras. 2018;17:275–9.
Miot H. Assessing normality of data in clinical and experimental trials. J Vasc Bras. 2017;16:88–91.
Kuo TC, Sheng Y. A comparison of estimation methods for a multi-unidimensional graded response IRT model. Front Psychol. 2016;7:880.
Crane PK, Gibbons LE, Jolley L, et al. Differential item functioning analysis with ordinal logistic regression techniques. DIFdetect and difwithpar. Med Care. 2006;44:S115–23.
Kutscher T, Eid M, Crayen C. Sample size requirements for applying mixed Polytomous item response models: results of a Monte Carlo simulation study. Front Psychol. 2019;10:2494.
Jiang S, Wang C, Weiss DJ. Sample size requirements for estimation of item parameters in the multidimensional graded response model. Front Psychol. 2016;7:109.
Miot HA. Sample size in clinical and experimental studies. J Vasc Bras. 2011;10:275–8.
Lorenzo-Seva U, Ferrando PJ. FACTOR: a computer program to fit the exploratory factor analysis model. Behav Res Methods. 2006;38:88–91.
Chalmers RP. Mirt: a multidimensional item response theory package for the R environment. J Stat Softw. 2012;48:1–29.
Miot HA, Penna GO, Ramos AMC, et al. Profile of dermatological consultations in Brazil (2018). An Bras Dermatol. 2018;93:916–28.
Carcano CBM, de Oliveira CZ, Paiva BSR, et al. The Brazilian version of Skindex-16 is a valid and reliable instrument to assess the health-related quality of life of patients with skin diseases. PLoS One. 2018;13:e0194492.
Guimenes Albuquerque R, Grudtner Buratto G, Hirotsu C, et al. Comparison of quality of life evaluated by SF-36 and DLQI in multibacillary and paucibacillary leprosy patients from Sao Paulo, Brazil. Int J Dermatol. 2019;58:1415–22.
Silva MF, Fortes MR, Miot LD, et al. Psoriasis: correlation between severity index (PASI) and quality of life index (DLQI) in patients assessed before and after systemic treatment. An Bras Dermatol. 2013;88:760–3.
Tavora IG, Bissoli GC, Miot HA, et al. Clinical manifestations and quality of life in hidradenitis suppurativa patients: survey of participants from an internet support group. An Bras Dermatol. 2019;94:298–303.
Scotton MF, Miot HA, Abbade LP. Factors that influence healing of chronic venous leg ulcers: a retrospective cohort. An Bras Dermatol. 2014;89:414–22.
Rencz F, Poor AK, Pentek M, et al. A detailed analysis of 'not relevant' responses on the DLQI in psoriasis: potential biases in treatment decisions. J Eur Acad Dermatol Venereol. 2018;32:783–90.
Rencz F, Gulacsi L, Pentek M, et al. DLQI-R scoring improves the discriminatory power of the dermatology life quality index in patients with psoriasis, pemphigus and morphea. Br J Dermatol. 2020;182:1167–75.
Garrido LE, Abad FJ, Ponsoda V. A new look at Horn's parallel analysis with ordinal variables. Psychol Methods. 2013;18:454–74.
Twiss J, McKenna SP. Comparing the impact of psoriasis and atopic dermatitis on quality of life: co-calibration of the PSORIQoL and QoLIAD. Qual Life Res. 2015;24:105–13.
Acknowledgements
Not applicable.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
All authors contributed to the conception and designed of this paper and collected the data. M.F.S.J and H.A.M. wrote the paper; H.A.M. performed the analysis. All authors revised critically the work and reviewed the final version of the article. All authors agree to be accountable for all aspects of this study. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
We performed a reanalysis of data from cross-sectional studies in Brazil. All studies were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. All studies were approved by their respective IRBs. Informed consent was obtained from all individual participants included in the study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Jorge, M.F.S., Sousa, T.D., Pollo, C.F. et al. Dimensionality and psychometric analysis of DLQI in a Brazilian population. Health Qual Life Outcomes 18, 268 (2020). https://doi.org/10.1186/s12955-020-01523-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12955-020-01523-9