
Abstract
Background
Ethiopia has achieved considerable progresses in the prevention and control of malaria in the past decades; hitherto it is a formidable health concern and socio-economic impediment. This study aimed at assessing the magnitude, knowledge, attitudes and practices towards malaria among febrile patients attending Chagni health center, northwest Ethiopia.
Methods
Health facility-based cross-sectional study was conducted to estimate the prevalence of malaria and KAP towards malaria among febrile patients at Chagni health center in Chagni Town during September 2017 to February 2018. In order to determine the magnitude of malaria, finger prick blood samples were collected and thick and thin smears were prepared and microscopically examined for the presence of malaria parasites. A pre-tested structured questionnaire was also applied to assess KAP of suspected malaria patients, attending the health center. Data were analyzed using SPSS version 20.0.
Results
Prevalence of malaria among febrile patients, who visited the sampled health facility, was 7.3%. Of these, Plasmodium falciparum, P. vivax, and mixed infections accounted for 55, 44.3 and 0.7% of the cases, respectively. This study also revealed that 97% of the respondents had ever heard about malaria and recognized it as a serious health problem. Mosquito bite was identified as the main malaria transmission. Taking drug (86.3%), use of mosquito nets (73.3%), drain stagnated water (68%), and house spay with insecticides (66%) were mentioned as the main malaria prevention methods. Mosquito net coverage and utilizations in the prior night were 98 and 75%, respectively. Indoor residual spraying (IRS) coverage was 99%, of which 77.5% of study participants’ houses have been sprayed in the last 6 months.
Conclusions
The current study revealed that prevalence of malaria among febrile illnesses in the study area was relatively low (7.3%) with a high proportion of P. falciparum. Besides, participants had adequate knowledge, encouraging attitudes, and good practices about prevention and control of malaria. However, some misconceptions on malaria disease, its transmission, and prevention have been noted that actually require due attention by the concerned stakeholders. The findings of this study could be used as important inputs for the implementation of effective malaria prevention and control methods, including community health education programs, and scaling up coverage of evidence-based interventions.
Similar content being viewed by others
Background
Malaria is a leading public health problem in Ethiopia where an estimated 68% of the population lives in malarious areas and three quarters of the total land mass is regarded as malarious [1]. Malaria has been one of the main causes of hospitalization and deaths in the country. In 2009/2010, it was the most important cause of outpatient visits and health facility admissions, accounting for 14% of outpatient visits and 9% of admissions in the country in 2009/2010 [2]. Plasmodium falciparum and P. vivax, which are distributed all over the endemic regions of the country, account for about 60 and 40% of malaria cases, respectively [3].
Varying topographical and climatic features contribute to the seasonal and unstable malaria transmission pattern in Ethiopia, which is usually characterized by frequent focal, cyclic, and widespread epidemics [3]. In general, the peak of malaria incidence follows the main rainfall season in July, August and September each year [3]. Previous cross-sectional studies of malaria prevalence in Ethiopia have demonstrated the wide range (2.8 to 39.6%) of malaria prevalence [4,5,6,7,8].
Malaria is one of the major public health problems in Amhara Regional State. In 2012, a total of 1,127,241 cases of malaria were reported in this Region, out of a population of 19,867,817 habitants [9]. West Amhara, constituting five administrative zones accounted for 93.1% of the total malaria burden, of which West Gojjam had the greatest number of cases (404,926) [6]. In Awi zone, malaria counted for 259,009 outpatients, 43,131 in-patients, and 1 death from 2011 to 2020 [10]. Chagni town, which is located in this zone, is among the major malarious areas in the region requiring particular attention.
In the past decade, considerable scale-up and implementation of key malaria interventions, including insecticide-treated nets (ITNs), indoor residual spraying of households with insecticide (IRS), and rapid diagnostic tests (RDTs) of malaria coupled with prompt and effective case management with artemisinin-based combination therapy (ACT) resulted in a significant reduction in the prevalence of the malarial in Ethiopia [11, 12]. However, such achievements have been faced with many challenges, including insecticide resistance of vectors, drug resistance of parasites, under-utilization of intervention, increased number of man-made mosquito breeding sites; gaps in service delivery and health system weaknesses [3, 13,14,15]. Moreover, poor community awareness toward malaria and control intervention practices have also been mentioned [16].
Studies involving community knowledge, attitudes and practices (KAP) have also been carried out in Ethiopia regarding the level of awareness about malaria and associated risk factors to its transmission and control measures [13, 17,18,19,20]. Such reports evidenced the presence of misconceptions about malaria causation, symptom identification, and treatment of malaria among communities, in particular within rural areas. In addition, practices for the control of the disease are inadequate, suggesting the need for health education to raise the community’s awareness about the disease. Considering these issues, fostering community KAP that help to gauge the implementation and effectiveness of proven malaria interventions in a given locality is vital to ensure scale-up of control options to sustainably prevent and control the disease.
The aim of the present study was therefore to determine the current prevalence of malaria infection among febrile patients attending Chagni health center, northwest Ethiopia from September 2017 to February 2018. In addition, the study focused on assessing patient’s knowledge, attitude, and practice of malaria and its control.
Methods
Study area
The study took place in Chagni Town in Amhara Regional State, northwest Ethiopia. Situated in the Awi Zone, the town has a longitude and latitude of 10°57′N 36°30′E, and an elevation of 1583 m above sea level. The town is located 505 km from Addis Ababa. The mean annual temperature and rainfall in the town are 21.6 °C and 1896.6 mill liters, respectively (Ethiopian Meteorology Agency, unpublished data). The town is divided into five kebeles (lowest administrative centers). The town has a total population of 39,292 of whom 19,165 were men and 20,127 women [21]. Two public health institutions (one hospital and one health center) and four medium private clinics are found in the town that provides healthcare service to the society.
Study design
The study followed facility-based cross-sectional design between September 2017 and February 2018.
Inclusion and exclusion criteria
For the prospective malaria prevalence study, malaria suspected individuals who had complains of febrile illness in the health center from September 2017 to February 2018 were included. On the other hand, patients who did not give consent and assent, as well as had been in the Kebeles for less than 6 months were excluded from the study.
For KAP study, febrile patients who were > 18 years and permanent residents in the five kebeles of the town were included. Alternatively, study participants who cannot communicate due to impairment or sever sickness and mentally sick people, those people who did not provide consent and assent, were less than 18 years, and had been in the kebeles for less than 6 months, were excluded.
Sample size and sampling techniques
All of the 4077 malaria suspected patients registered in the health centre from September 2017 to February 2018 were the sample sizes to determine the current prevalence of malaria. In the meantime, the sample size for assessing the KAP of participants was calculated using a single population proportion formula (n = z2p(1-p)/d2 [22]; where n = the sample size, z = 1.96 at 95% confidence interval (CI), d = margin of error at 5%, P = 0.78 (78% proportion of population who had good knowledge towards malaria and its prevention was taken from a study done in Amhara region [1]. After adding 5% non-response rate, the final sample size became 274.
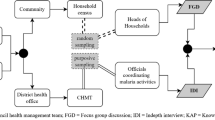
For KAP study, a systematic simple random sampling method was used to enroll the study participants. First, the proposed sample size was proportionately allocated to each kebele. Thereafter, individual participants from each kebele who came to health centre were systematically selected by taking every third attendant from random start on the health centre up to the sample size of the population is reached.
Data collection
Blood film collection and testing
Data was collected from September 2017 to February 2018. Blood slide samples were taken from compliance of febrile patients at Chagni health centre. Blood film collection was carried out by experienced medical laboratory technicians by pricking the finger with disposable blood lancet. Throughout the data collection, microscopy was used for the detection and species identification of Plasmodium parasites by examination of peripheral smears of stained blood films, as per the WHO protocol. Thick and thin blood smears were taken and identification numbers marked on the thin films. The thin films fixed using 100% methanol and all slides were stained with 3% Giemsa solution for 20 min. The staining technique and blood film examination was conducted according to a standard of WHO protocols. Then, parasite positivity was determined from thick smear and species identification was carried out from thin smear slide preparation. Malaria slides were stained with Giemsa and examined under 100x microscopes for the presence of malaria parasites. Parameters such as date of examination, total clinically treated and confirmed cases in months, types of malaria species, and socio-demographic data such as age and sex were collected of patients were collected on patient registration book. All individuals who had fever on physical examination and were positive for malaria parasites during blood film examination were offered anti-malarial treatment as per national guidelines [4].
Measurement of KAP
In order to measure KAP of the study participants about malaria and its prevention and control practices, a structured questionnaire was designed and applied. The questionnaire covered socio-demographic details, knowledge about malaria transmission, treatment and prevention, and risk perception of the disease. It also covered bed net ownership and use, prevention and treatment practices of the respondents. The questionnaire was first developed in English and translated into Amharic (the local language), and then pre-tested in non-selected patients for assessing content validity, appropriateness, and question comprehensibility. It was administered to 274 systematically randomized study participants selected from febrile patients, visiting the health center during September 2017 to February 2018. Two trained laboratory technicians from the health center were selected to collect data. Training was given to the data collectors on how to conduct the interview, content of the questionnaire, data quality, and ways to approach respondents. Data were checked for completeness, and incomplete questionnaires were returned to data collectors for correction by revisiting the concerned interview.
Data analysis
Data were checked for completeness and consistency, entered in to Microsoft Excel data sheets, and exported in to Statistical Package for Social Science (SPSS) version 20 software for data analysis. Descriptive statistics were carried out to measure relative frequencies, percentages, averages, and relative frequencies of the variables. The chi-squared test was used for prospective malaria prevalence data to determine differences between age, sex and seasons and malaria parasite distribution. Statistical significance was defined at P < 0.05. The analyzed data was presented using tables and figures.
Results
Malaria prevalence at health facility survey
In this study, a total of 4077 malaria suspected patients were microscopically diagnosed at Chagni Health Center from September 2017 to February 2018 (Table 1). Of these, 296 (7.3%) were slide positive for malaria with mean monthly malaria cases of 49.3. The mean monthly slide positivity rate was 6.95%, though the number of malaria suspected patients who visited the health center showed fluctuating trend each month. Malaria case distribution by months had significant fluctuating trend (χ2 = 14.194, df = 5, P < 0.05; Table 1). Transmission of malaria from September to November was higher, 194 (65.5%) whilst the dry season of the year from December to February had lower case, 102 (34.5%).
Plasmodium parasite distribution with socio-demographic variables
Plasmodium falciparum and P. vivax were the only species in the study area, where P. falciparum accounted for 163 (55%), P. vivax was 131 (44.3%), and the rest 2 (0.7%) were mixed infections of both species. Of the total patients examined, 2103 were males and 1974 were females (Table 2). The infection rates among males were 164 (55.4%) and females were 132 (44.6%), albeit this association of malaria cases with sex was not statistically significant (χ2 = 1.868, df = 1, P > 0.05).
The distribution of parasite species in relation to age is presented in Fig. 1. Distribution of malaria varied among different age groups, ranging from 4.7 to 8.5% (χ2 = 14.448, d.f. = 2, P = 0.001). Adults (≥15 years) were the most affected group 185 (8.5%), followed by 5–14 and under 5 age categories, with prevalence rates 63 (7.1%) and 48 (4.7%), respectively. P. falciparum species proportion of positive cases were higher in 5–14 age group, followed by ≥15 years, and under 5 age group with a prevalence rate of 57.1% (36/63), 56.2% (104/185) and 47.9% (23/48), respectively (Fig. 1). Similarly, the age group ≥15 was more affected by P. vivax, 79 (42.7%) compared to 5–14, 27 (30.7%) and below 5 year, 25 (52.1%) age categories. There were two mixed cases detected in both male and female individuals of age groups ≥15 years of age.

Prevalence of Plasmodium spp. in different age groups in Chagni Health Centre from September 2017-Feburary 2018
Socio-demographic characteristics for KAP survey
We enrolled a total of 274 individuals with a 100% response rate (Table 3). Out of the total respondents, 154 (56.2%) and 120 (43.8%) were males and females, respectively. The age of the respondents ranged from 18 to 74 years, with the median age of 32.4 years. Most of study participants 128 (46.7%) were married. The majority of respondents [118 (43.1%)] had no formal education. The average family size of the respondents was 3.84. The main economic activities by study respondents were daily labor 95 (34.7%), government employment 64 (23.4%), trading 48 (17.5%), agriculture 33 (12%), and other 34 (12.4%) (Table 3).
Knowledge and attitude of respondents towards malaria and mosquitoes
Malaria related knowledge of the participants is summarized in Table 4. The majority of the respondents [266 (97%)] had ever heard about malaria and the same number of respondents believed that malaria is one of serious and life-threatening diseases of the community. The most common sources of malaria related information were mass media (radio and television) 229 (86.1%), and health facility education 37 (13.9%). One hundred sixty two (60.9%) of the respondents mentioned that malaria is transmittable from person to person, of whom 156 (96.3%) and 6 (3.7%) associated the transmission with the bite of mosquitoes and drinking contaminated water, respectively (Table 4).
Fever, chills and shivering, and headache were the most frequently mentioned malaria symptoms reported by 97, 96.6, and 95.4% of the respondents, respectively (Table 4).
Of the respondents, the majority (97%) stated malaria as a preventable and curable disease, while 2.6% considered the opposite and 0.4% did not know. Taking drug 226 (85%), using mosquito nets 192 (72.2%), draining stagnant water 178 (67%), and IRS 173 (65%) were the most commonly mentioned preventive strategies. Most of the respondents 218 (82%) believed that sleeping under mosquito net protect from mosquito bites (Table 5).
Malaria prevention practices
Regarding treatment seeking behavior, 243 (91.4%) of the respondents had sought treatment within the first 24 h of symptom onset while the rest, 23 (8.8%) had delayed treatment seeking behavior (Table 6). Of the respondents, 243 (91.4%) responded that they sought treatment from health center/clinic, 15 (5.6%) while 8 (3%) of them practice self-medication by procuring drugs from drug stores and using traditional medicines such as garlic and leaf of neem tree, respectively.
The majority (98%) of interviewees reported that they possessed at least one insecticide-treated mosquito net (ITN) in their houses. Out of which, 167 (62%), 81 (30%), and 20 (8%) had two, more than two, and one ITN per household, respectively. The majority (75%) of the ITN owners claimed that they slept under a bed net the previous night while the rest of 25% did not. A similar figure (74%) replied that pregnant mother and children were given priority to sleep under bed net, followed by father and mother (22%), and the remaining family members (4%). It was also indicated that three fourth of the individuals who owned ITN reported that they utilize bed net regularly /every night, whilst 25% of respondents stated they use it during the malaria season. Of those who are not currently using bed net, 192 (77%) mentioned lack of access, 20 (8%), and 37 (15%) mentioned other reasons. The reasons for not using bed net were that fear of burning sensation (64%), and 36% lack of awareness (Table 6).
The study also revealed that IRS is one of the most important malaria prevention methods practiced in the locality with the overall coverage of 99%. Out of the respondents, 77.5 and 22.5% of them stated that their house was sprayed with chemicals in the last 6 and 12 months, respectively (Table 6).
Discussion
In this study, we found that relatively small percentage of febrile patients visiting Chagni health center had microscopically confirmed malaria parasitemia. The overall malaria positivity rate was 7.3%. This figure is comparable with the result of the study done in Kombolcha health facility, north-central Ethiopia that reported a prevalence of 7.52% [23]. Nonetheless, the finding of this study contradicts with previous studies from southern and northern Ethiopia, reported overall malaria positivity rates between 11.5 and 28.1% among patients visited health facilities [5, 24, 25]. Possible factors for observed variations might be differences in the time of studies, microclimate, altitude, community awareness about malaria bed net application, its transmission, and health seeking behavior, and malaria intervention practices.
The dominant Plasmodium species detected in the current study participants was P. falciparum. This finding is congruent with national figures and other similar studies in parts of Ethiopia that reported preponderance of P. falciparum than P. vivax [3, 8, 26, 27]. However, this is incongruity with the previous report from Jimma Town, which reported a higher prevalence of P. vivax than P. falciparum [28]. The reason why P. falciparum dominated over P. vivax in the study area could be related to drug resistance pattern, and gap of program performance.
In the present study, more males (55.4%) were affected by malaria than females (44.6%). This finding is concurrent with studies from several localities in Ethiopia that reported higher malaria burden among males than females [23, 26, 27]. The higher prevalence rate in males might be due to the fact that males are usually engaged in outdoor activities at dusks and dawns, coinciding with the peak biting hours of the exophagic mosquito species. In addition, males often travel as seasonal migrant laborers to different malarious parts of Ethiopia to perform agricultural activities, thereby exposing them to the higher risk of contracting malaria infection. Conversely, this was not similar with a study conducted in Amhara region where the prevalence of malaria was relatively higher among females (60%) than males (40%) [29].
Regarding the age groups, the burden of malaria morbidity was more concentrated in the adults of age 15 and above. Studies elsewhere in Ethiopia have also shown that the risk of malaria infection varied by age with some reporting more susceptibility to malaria infections among males in the age groups > 15 years [7, 26, 27, 30]. The contributing factors for such higher burden of disease among adults might be due to their frequent engagement in different activities like agriculture, trade and other occupational risks that increase the exposure to infective mosquito bites. Lower cases of malaria in children under 5 years of age was detected, which could be linked to their reduced exposure to infected mosquito bite due to good malaria awareness and control and prevention practices by their guardians.
The results revealed that most of the respondents (97%) had ever heard about malaria and similar number of respondents believed that malaria is one of the serious diseases of the community, which is in line with previous reports in Ethiopia and elsewhere [20, 31, 32]. Study subjects also cited that the most common source of information about malaria was mass media (radio and television) (86.1%), followed by health facility education (13.9%), indicating that these communication channels are essential vehicles to deliver malaria-related information to the community. Elements of IVM such as community malaria education using mass media such as radio and TV have been implemented by the National malaria control program since 2006 [33]. This is similar with those previously reported results from Africa, in which over 90% of individuals in malaria endemic areas are aware of malaria and that mass media (television and radio) and health education by health facilities are the most commonly cited source of malaria information sources [34, 35].
Mosquito bite has been identified as the principal malaria transmission as shown in some studies in Ethiopia and elsewhere in Africa [18, 20, 34,35,36,37]. In Ethiopia, regular practice of awareness creation in the communities about health issues through health extension workers and mass media such as radio and television brought remarkable behavioral changes in the control and prevention of communicable diseases [33]. It can be presumed that this factor has contributed to the high level of awareness observed in the study participants regarding the causes and transmission of malaria in the area.
Fever, headache, chills and shivering, loss of appetite and vomiting were mentioned as sign and symptoms of malaria. Similar results were found from different KAP studies in other regions of Ethiopia [18, 20, 36, 38]. Prominently, large majority of subjects linked mosquito biting time during night time and their main breed sites to stagnant water, which is comparable with previous studies in Ethiopia and elsewhere [33, 37, 38]. This correct understanding of mosquito behavior among participants of the present study is encouraging to implement appropriate malaria preventive measures and for the proper utilization of ITNs.
Similar to other studies in Amhara region and other parts of Ethiopia [18,19,20, 39], great majority (97%) of participants believed that malaria is preventable and curable disease. Taking drug, use of mosquito nets, drain stagnated water (mosquito breeding sites), and house spay with insecticides were the main types of malaria preventive measures frequently reported by the present study participants. This is in line with previous reports from Tanzania [35] and Iran [40].
Around 91.4% of participants go to the nearest health service within the 24 h upon the occurrence of the first malaria symptoms. This was further substantiated by the observation that about 91.4% of participants sought treatment at health facilities, suggestive of a good practice of treatment-seeking behavior at health structures. Generally, treatment seeking behavior for malaria diseases showed improvements across the country in recent reports [1]. However, the commitment among few participants to bring people with fever to health facilities within 24 h since the onset of clinical symptoms remains low, and that they rely on the use of self-administered drugs and traditional medicines, which are common practices in parts of Africa [18, 34, 41]. Treatment seeking behavior is important for early case detection and management so that transmission would be reduced. Therefore, promotion of health education to raise awareness is very crucial to direct the wider community to seek timely treatments at the health structures earlier upon the occurrence of malaria symptoms.
This study also demonstrated that around 98% of participants had least one ITN, of which 75% of them claimed that they slept under a bed net the previous night, which is consistent with previous studies elsewhere in Ethiopia [19, 38, 42]. Yet, quarter of the respondents did not use bed net the previous night. It is strongly envisaged that ITN ownership itself will have little impact on the burden of malaria unless people regularly use it. Factors such as lack of access to ITNs, discomfort due to heat, fear of burning sensation, low level of awareness about its benefit, and lack replacement schemes for worn out ones were cited as the reasons for not using ITNs in this study. Scaling up community awareness through health education has proved to be effective and has effectively alleviated misconceptions on malaria disease, its transmission, and prevention practices [33, 43, 44]. The study further showed that most of the communities give priority for pregnant mother and children to sleep under bed net, which is comparable with results reported from other studies elsewhere in Ethiopia [20, 36].
Our data also showed that IRS is one of the most important malaria prevention methods practiced in the locality with the overall coverage of 99%. Houses of more than 77% of the respondents get sprayed during spraying campaign, result that is comparable with the reports from Jiga area and Shewa Robit district of north-western Ethiopia [6, 18]. This result asserts the demand to expand the coverage and frequency of IRS in malaria endemic areas in order to achieve an already targeted plan of 100% spraying of households before and throughout the transmission for effective prevention and control of malaria [45].
Limitations of the study design and the methods of data collection might create some potential for biases in this study. The cross-sectional design of the study with a focus of recruiting participants who sought healthcare might have influenced their knowledge and practices in malaria prevention and treatment. In addition, data collection relied on information given by the interviewees so that practices such as presence and use of ITN or treatment seeking practices could not be verified.
Conclusions
In conclusion, the current study illustrated that prevalence of malaria among febrile illnesses in the study area was relatively low (7.3%) with a dominance of P. falciparum. It has also been indicated that study subjects had adequate knowledge, encouraging attitudes, and good practices on malaria prevention and control. Nonetheless, some misconceptions on malaria disease, its transmission, and prevention persist as reported in this study, essentially require due attention device effective intervention to improve these misconceptions and lack of [proper information. The findings of this study would make inroads into the implementation effective malaria interventions in the area and beyond focusing on enhancing community awareness and scaling up coverage of evidence-based interventions.
Availability of data and materials
All data underlying the findings are available from corresponding author on reasonable request. All relevant data are within the manuscript.
Abbreviations
- KAP:
-
knowledge, attitudes and practices
- IRS:
-
Indoor residual spray
- ITNs:
-
Insecticide-treated nets
- SPSS:
-
Statistical Package for the Social Science
- WHO:
-
World Health Organization
References
Ethiopian Public Health Institute. Ethiopia National Malaria Indicator Survey 2015. Addis Ababa: Ethiopian Public Health Institute; 2016. https://www.ephi.gov.et/images/pictures/download2009/MIS-2015-Final-Report-December-_2016.pdf.
Federal Ministry of Health (FMOH). Health and health-related indicators, 2009/2010. Addis Ababa: Ministry of Health of Ethiopia; 2011.
Federal Ministry of Health (FMOH). National strategic plan for malaria prevention, control and elimination in Ethiopia, 2011–2015. Addis Ababa: Ministry of Health of Ethiopia; 2010.
Gravesa PM, Richardsa FO, Ngondi J, Emerson PM, Shargie EB, Endeshaw T, et al. Individual, household and environmental risk factors for malaria infection in Amhara, Oromia and SNNP regions of Ethiopia. Trans R Soc Trop Med Hyg. 2009;103(12):1211–20. https://doi.org/10.1016/j.trstmh.2008.11.016.
Delil RK, Dileba TK, Habtu YA, Gone TF, Janfa T. Magnitude of malaria and factors among febrile cases in low transmission areas of Hadiya zone, Ethiopia: a facility based cross sectional study. PLoS One. 2016;11(5):e0154277.
Ayalew S, Mamo H, Animut A, Erko B. Assessment of current malaria status in light of the ongoing control interventions, socio-demographic and environmental variables in Jiga Area, Northwest Ethiopia. PLoS One. 2016;11(1):e0146214.
Hawaria D, Getachew H, Zhong G, Demissew A, Habitamu K, Raya B, et al. Ten years malaria trend at Arjo-Didessa sugar development site and its vicinity, Southwest Ethiopia: a retrospective study. Malar J. 2019;18:145.
Alemu A, Muluye D, Mihret M, Adugna M, Gebeyaw M. Ten year trend analysis of malaria prevalence in Kola Diba, North Gondar, Northwest Ethiopia. Parasit Vectors. 2012;5(1):173. https://doi.org/10.1186/1756-3305-5-173.
TTC. Summary proceedings 4th annual malaria control program review Ethiopia and Nigeria march 8, 2013. Atlanta: The Carter Center; 2013. http://www.cartercenter.org/resources/pdfs/news/health_publications/malaria/malaria-summary-proceedings-final-2012.pdf
Yenew C, Mulatu S. Trends of Malaria on Hotspot and Ivermectin Mass-drug Administration Zone of Amhara Regional State, 2020. 16 December, 2020, PREPRINT (Version 1) available at Research Square [https://doi.org/10.21203/rs.3.rs-112470/v1]. https://www.researchsquare.com/article/rs-112470/v1.
Federal Ministry of Health. Malaria diagnosis and treatment guidelines for health Workers in Ethiopia. 2nd ed. Addis Ababa: Federal Ministry of Health; 2004.
Taffese HS, Hemming-Schroeder H, Koepfli C, Tesfaye G, Lee M, Kazura J, et al. Malaria epidemiology and interventions in Ethiopia from 2001 to 2016. Infect Dis Poverty. 2018;7(1):103. https://doi.org/10.1186/s40249-018-0487-3.
Ayele DG, Zewotir TT, Mwambi HG. Prevalence and risk factors of malaria in Ethiopia. Malar J. 2012;11:195.
Messenger JS, Irish SR, Anshebo GY, Tesfaye AG, Ye-Ebiyo Y, Chibsa S, et al. Insecticide resistance in Anopheles arabiensis from Ethiopia (2012–2016): a nationwide study for insecticide resistance monitoring. Malar J. 2017;16:469.
Kibret S, Wilson GG, Ryder D, Tekie H, Petros B. Environmental and meteorological factors linked to malaria transmission around large dams at three ecological settings in Ethiopia. Malar J. 2019;18:54.
Asale A, Kussa D, Girma M, Mbogo C, Mutero MC. Community based integrated vector management for malaria control: lessons from three years’ experience (2016–2018) in Botor-Tolay district, southwestern Ethiopia. BMC Public Health. 2019;19(1):1318. https://doi.org/10.1186/s12889-019-7606-3.
Deressa W, Chibsa S, Olana D. Treatment seeking of malaria patients in east Shewa zone of Oromia. Ethiop J Health Dev. 2003;17(1):9–16.
Abate A, Abraham D, Berhanu E. Community knowledge, attitude and practice about malaria in a low endemic setting of Shewa Robit town, northeastern Ethiopia. BMC Public Health. 2013;13(1):312. https://doi.org/10.1186/1471-2458-13-312.
Alelign A, Petros B. Knowledge, attitudes and practices of malaria transmission and preventive measures in Woreta town, Northwest Ethiopia. BMC Res Notes. 2018;11(1):491. https://doi.org/10.1186/s13104-018-3607-z.
Tesfay K, Yohannes M, Mardu F, Berhe B, Negash H. Assessment of community knowledge, practice, and determinants of malaria case households in the rural area of Raya Azebo district, Northern Ethiopia. PLoS One. 2017;14(10):e0222427.
(CSA). The 2007 National Census report for Ethiopia. Addis Ababa: Central Statistical Agency; 2008.
Daniel W. Biostatistics, A foundation for the analysis in the health sciences. Singapore: Wiley; 2004.
Gebretsadik D, Feleke DG, Fiseha M. Eight-year trend analysis of malaria prevalence in Kombolcha, south Wollo, north-Central Ethiopia: a retrospective study. Parasit Vectors. 2018;11(1):55. https://doi.org/10.1186/s13071-018-2654-6.
Belete EM, Roro AB. Malaria prevalence and its associated risk factors among patients attending Chichu and Wonago health centers, South Ethiopia. J Res Health Sci. 2016;16(4):185–9.
Woday A, Mohammed A, Gebre A, Urmale K. Prevalence and associated factors of malaria among febrile children in Afar region, Ethiopia: a health facility based study. Ethiop J Health Sci. 2019;29(5):613–22. https://doi.org/10.4314/ejhs.v29i5.12.
Shiferaw M, Alemu M, Tedla K, Tadesse D, Bayissa S, Bugssa G. The prevalence of malaria in Tselemti Wereda, North Ethiopia: a retrospective study. Ethiop J Health Sci. 2018;28(5):539–46. https://doi.org/10.4314/ejhs.v28i5.4.
Dabaro D, Birhanu Z, Delenasaw D. Analysis of trends of malaria from 2010 to 2017 in Boricha District, Southern Ethiopia. Malar J. 2020;19:88.
Alemu A, Tsegaye W, Golassa L, Abebe G. Urban malaria and associated risk factors in Jimma town, south-westEthiopia. Malar J. 2011;10:173.
Derbie A, Mekonnen D. Prevalence of malaria: a cross sectional study at Bahir Dar health center, Northwest Ethiopia. J Harmoniz Res Med Health Sci. 2017;4(2):74–9.
Kassie A, Wale M, Fekensa T. Assessment of insecticide treated bed net possession, proper utilization and the prevalence of malaria, in Dejen wereda, east Gojam zone, Ethiopia. J Parasitol Vector Biol. 2014;6(7):92–102.
Amusan VO, Umar YA, Vantsawa PAUYA. Knowledge, attitudes and practices on malaria prevention and control among private security guards within Kaduna. Sci J Pub Health. 2017;5:240–5.
Hlongwana KW, Mabaso ML, Kunene S, Govender D, Maharaj R. Community knowledge, attitudes and practices (KAP) on malaria in Swaziland: a country earmarked for malaria elimination. Malar J. 2009;8(1):29–37. https://doi.org/10.1186/1475-2875-8-29.
Federal Ministry of Health (FMoH). National Five-Year Strategic Plan for Malaria Prevention & Control In Ethiopia 2006–2010. 2016.
DePina AJ, Dia AK, Martins AAS, Ferreira MC, Moreira AL, Leal SV, et al. Knowledge, attitudes and practices about malaria in Cabo Verde: a country in the pre-elimination context. BMC Public Health. 2019;19(1):850. https://doi.org/10.1186/s12889-019-7130-5.
Munisi DZ, Nyundo AA, Mpondo BC. Knowledge, attitude and practice towards malaria among symptomatic patients attending Tumbi Referral Hospital: A cross-sectional study. PLoS One. 2019;14(8):e0220501.
Haile S, Abera S, Muhdin S, Kumalo A, Henok A. Knowledge and Practice towards Prevention and Control of Malaria in Tepi Town, Sheka Zone, Southwestern Ethiopia. Health Sci J. 2015;10(1):9.
Yaya S, Bishwajit G, Ekholuenetale M, Shah V, Kadio B, Udenigwe O. Knowledge of prevention, cause, symptom and practices of malaria among women in Burkina Faso. PLoS One. 2017;2(7):e0180508.
Yimer F, Animut A, Erko B, Mamo H. Past five–year trend, current prevalence and household knowledge, attitude and practice of malaria in Abeshge, South- central Ethiopia. Malar J. 2015;14:230.
Mitiku I, Assefa A. Caregivers perception of malaria and treatment seeking behavior for under five children in Mandura District, West Ethiopia: a Cross sectional study. Malar J. 2017;16:14.
Madani A, Soleimani-Ahmadi M, Davoodi HS, Sanei-Dehkordi A, Jaberhashemi AS, Zare M, et al. Household knowledge and practices concerning malaria and indoor residual spraying in an endemic area earmarked for malaria elimination in Iran. Parasit Vectors. 2017;10(1):600.
Abuya TO, Mutemi W, Karisa B, Ochola SA, Fegan G, Marsh V. Use of over-the-counter malaria medicines in children and adults in three districts in Kenya: implications for private medicine retailer interventions. Malar J. 2007;6:57.
Animut A, Negash Y, Kebede N. Distribution and utilization of vector control strategies in a malarious village of Jabi Tehnan District, North-Western Ethiopia. Malar J. 2014;13(1):356. https://doi.org/10.1186/1475-2875-13-356.
Amoran OE, Fatugase KO, Fatugase OM, Alausa KO. Impact of health education intervention on insecticide treated nets uptake among nursing mothers in rural communities in Nigeria. BMC Res Notes. 2012;5(1):444. https://doi.org/10.1186/1756-0500-5-444.
Kebede Y, Abebe L, Alemayehu G, Sudhakar M, Birhanu Z. School-based social and behavior change communication (SBCC) advances community exposure to malaria messages, acceptance, and preventive practices in Ethiopia: a pre-posttest study. PLoS One. 2020;15(6):e0235189. https://doi.org/10.1371/journal.pone.0235189.
The Federal Democratic Republic of Ethiopia. National malaria program monitoring and evaluation plan 2014–2020. Addis Ababa: The Federal Democratic Republic of Ethiopia Ministry of Health; 2014.
Acknowledgments
The authors would like to thank Chagni health center head for allowing data collection. We also acknowledge Addis Ababa University for sponsoring the study. Our gratitude also goes to the data collectors and study participants.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
BB and TG conceived the study and involved in the data collection. BB, TG and AG were involved in the data analysis, preparation and critically reviewing the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval consideration
Ethical clearance was obtained from the Institutional Review Board of College of Natural and Computational Sciences, Addis Ababa University and Chagni Health Center Administration. A written supportive letter was also secured from the district health bureau before data collection. The aim of the study was explained in details to the respondents and the respondents were assured of the confidentiality of their information at all levels of the study. Only volunteer sample populations with informed consent were included in the present study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Questionnaire used in KAP Study.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Belay, B., Gelana, T. & Gebresilassie, A. Malaria prevalence, knowledge, attitude, and practice among febrile patients attending Chagni health center, Northwest Ethiopia: a cross-sectional study. Trop Dis Travel Med Vaccines 7, 20 (2021). https://doi.org/10.1186/s40794-021-00146-2
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1186/s40794-021-00146-2