
Abstract
Background
Western diet and sedentary life are imputed for non-alcoholic fatty liver disease (NAFLD). Relationship of obesity and bright liver, i.e., the ultrasound hallmarks of fatty liver, evaluated as Bright Liver Score (BLS), with Western diet pattern score (WDS) and with the level of physical exercise, assessed by the Baecke questionnaire, were investigated.
Methods
One hundred fifty (72 females, 78 males) NAFLD non-diabetic patients, 47.89 ± 13.85 years old, were referred to a diagnostic-therapeutic unit with the lone evidence of fatty liver as detected by an ultrasound. WDS, Adherence to Mediterranean Diet Score (AMDS), physical exercise, insulin resistance (HOMA-IR), and BMI were assessed also after 6 months of comprehensive lifestyle intervention.
Results
BLS, BMI, HOMA, and WDS were significantly greater, while AMDS and physical exercise were lower at the greater severity of ultrasound (US)-detected NAFLD. Positive linear correlation of WDS, BMI, and HOMA vs. BLS was present at patients’ referral. After intervention, decrease of liver dimension and of Bright Liver Score concurrent with a reduction of BMI, HOMA-IR, WDS, LDL cholesterol, and triglycerides was observed. A reciprocal increase of AMDS, physical exercise, and HDL cholesterol was also reported.
Conclusions
The assessment of some features of the Western diet is possible; its effect, along with overweight, is associated with a greater severity of fatty liver as evaluated by ultrasound in NAFLD.
Trial registration
NCT02670590. Registered on February 2, 2016.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
Clinical risk assessment is the basis for a tailored clinical risk management. Western diet and sedentary life are imputed for non-alcoholic fatty liver disease (NAFLD) [1,2,3,4,5,6,7]. Worldwide, the prevalence of NAFLD is about 25% with the highest prevalence in the Middle East and South America and the lowest in Africa [2] and a fibrosis progression proportion to steatohepatitis (NASH) of 40.76% [2]. The unfavorable impact of unhealthy dietary pattern on the liver is recognized and confirmed [1]. Several food, nutrients, dietary profiles, and other nutrition-related factors were and are studied, considering their relationship with obesity and other risk factors for degenerative disease. This is an approach reciprocal of the quest for “healthy diets,” investigated by epidemiological, observational, and interventional approaches [8], and it is probably fostered by the impact of non-traditional, industrial foods recently introduced in emerging Countries, which otherwise have historical and robust cultures of traditional healthier diets [2,3,4,5,6,7,8,9]. A special role should be deserved to gastronomy which links food and culture, art of preparing, and serving more or less rich or delicate and appetizing food: overall, it encompasses both style of cooking and science of good eating. Mediterranean diet, besides being a very broad but quite meaningful concept, was developed and is now a well-accepted model of healthy diet. Its feature and benefits were examined by excellent epidemiological investigations and confirmed by clinical intervention studies [9,10,11]. Nutritional counseling, oriented to a Mediterranean diet profile, showed indeed improvement of the lipid profile, positive effects on liver enzymes, insulin resistance and NAFLD [6, 9, 10].
Actually, the concept of unhealthy nutrition and food, by this approach, is mainly a negative concept, i.e., it is defined by a poor adherence to healthy diets [12, 13]. More definite criteria for detecting unhealthy diet profiles and components potentially harmful for the liver and clinical intervention are still mostly warranted [14] than actively pursued; however, some valuable trials have addressed to this scope [15], confirming the concept that unhealthy diet in adolescence increases the risk of fatty liver in youngsters. In this study, however, this association is no longer significant after adjusting for body mass index, so that several possible associated factors should be considered, including the most obvious one, i.e., that fatty liver may be related mainly to an excessive caloric intake or inadequate caloric expenditure, consequent to limited physical activity [16]. We recently reported that beneficial effects on decrease or disappearance of fatty liver can be achieved by the concurrent intervention on dietary changes, in the sense of a greater adherence to the Mediterranean diet and by the increase of physical activity [16]. Physical exercise is an important factor for maintaining normal body weight or reducing obesity [17,18,19,20]. Overall, these combined effects of diet and physical activity are seemingly globally beneficial; actually, also neurological [21,22,23] and psychological [24, 25] improvements are reported. The scope of our study is to investigate the relationship, if any, of food preferences with the severity of bright liver, defined by ultrasound, and assessing concurrently the difference of the level of physical exercise. This clinical research is developed within a frame aimed at a sustainable assessment and change of lifestyle and Western dietary pattern.
Methods
The subjects (30–70 years old) were referred by the out-patient clinic for lifestyle nutritional prescription for overweight (BMI > 25 ≤ 30) and obesity (BMI > 30 ≤ 40) or by the emergency department of the University Hospital Policlinico-Vittorio Emanuele of Catania, for minor ailments, all with the lone evidence of fatty liver detected by BLS. Patients were consecutively studied throughout January 2011–December 2014 also by a comprehensive ultrasound assessment (liver-abdomen, heart, thyroid, and lung), according to our current practice [26, 27]. Patients with the confirmed evidence of fatty liver by ultrasound (US), according to the Bright Liver Score (BLS) [28], and with habitual low alcohol consumption (defined as < 20 g/day of ethanol for both men and women in the last year), were included in the study. The severity of liver steatosis was graded 1–3: grade 0 was the absence of bright liver, i.e., a normal pattern, and previously validated by US-guided FNAB (fine-needle aspirate biopsy by 20 Gauge Menghini’s needles). GE echo color Doppler machines (GE Logiq P7, US machine manufactured by GE Medical Systems, Milwaukee, WI, USA), high-resolution, equipped with real-time convex, phased array and linear scan transducers, were used throughout this study. Routine laboratory tests included hepatitis virus panel (hepatitis A, B, and C viruses, i.e., HAV, HBV, and HCV) and cancer biomarkers (Alpha-fetoprotein, CEA, Ca125, Ca 19-9, and Ca15-3), thyroid hormones (FT3 and FT4), thyroid-stimulating hormone (TSH), aspartate aminotransferase (AST), alanine aminotransferase (ALT), γ-glutamyl transpeptidase (γ-GT), ferritin, total protein, and albumin. Mediterranean Diet Adherence Profile was assessed by the Adherence to Mediterranean Diet Score (AMDS) on the basis of a 1-week recall computerized questionnaire [10, 11]. A pictogram-based method of visualizing dietary intake, descriptive also of the size of the single portion is currently used; pictograms include also items for the quantification of physical activity, which is otherwise quantified by detailed physical activity reports (Baecke questionnaire) [29]. Exclusion criteria were diabetes, renal insufficiency (glomerular filtration rate (GFR) < 90 ml/min), cancer, heart failure (> II NYHA Class), chronic viral hepatitis, and cirrhosis. Insulin resistance was assessed as HOMA-IR [30]. The counseling intervention (6 months), based on cognitive-behavioral strategies, included goal setting, self-monitoring, feedback and reinforcement, self-efficacy enhancement, incentives, modeling, problem solving, relapse prevention, and motivational interviewing [10, 11]. The Western diet pattern (WDP) score included 12 questions and items exploring specific foods use and its weekly frequency. In more detail, the use of critical foods of Western diet was investigated to reach the Western diet pattern score. For each item of the following, a score 1–7, on a weekly basis, was recorded by the patients; a total maximal score of 84 is therefore calculated. The questions were specific and articulated, addressed to the use in one or more days of the week preceding the interview of the following 12 categories of food: (1) take-away foods, (2) red meats, (3) processed meats, (4) full-fat dairy products, (5) fried potatoes (“hot chips” or “French fries”), (6) refined cereals, (7) cakes and biscuits, (8) confectionery, (9) soft drinks, (10) crisps, (11) sauces with cream, and (12) other dressings. A preliminary validation of reliability of the questionnaire was performed in the same group of subjects by the test-retest procedure, 1 day apart, assessing the internal consistency by Cronbach’s alpha analysis; measures of α ≥ 0.9 were found, i.e., an excellent concordance. The study and the manuscript were approved by the Institutional Review Board of the Policlinico-Vittorio Emanuele Project Office. Written informed consent was obtained from each patient prior to the clinical data recording and before the US procedure, allowing the use of information for teaching and clinical research. Details that might disclose the identity of the subjects under study are carefully omitted in any part of the study. This observational study follows the STROBE guidelines, and it is registered at https://clinicaltrials.gov/ct2/show/NCT02670590.
Statistical analysis
Linear correlation of Western diet pattern (WDP) score, Adherence to Mediterranean Diet Score, physical exercise, assessed by Baecke’s tool, insulin resistance assessed by HOMA-IR, and BMI vs. BLS were analyzed and included also in a MLR model using data available at the enrollment of patients. WDP score, Adherence to Mediterranean Diet Score (AMDS), physical exercise, insulin resistance (HOMA-IR), and BMI and the other measures were assessed also after 6 months of comprehensive lifestyle intervention and compared by Student’s t test.
Results
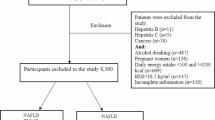
The study, after the initial enrollment of 195 subjects, included at last 150 (72 females, 78 males) non-alcoholic fatty liver disease (NAFLD) non-diabetic patients, aged 47.89 ± 13.85 years: 97 of them were referred by the out-patient clinic and 53 of them by the emergency department; 30/195 patients were excluded due to the lack of preliminary criteria of inclusion and 15/195 dropped from the study before the end of the period of the observation. In Table 1, the characteristics of patients are summarized. After intervention, changes of liver ultrasound features were observed, with a decrease of the longitudinal right liver length from 167.75 ± 18.31 mm to 157.60 ± 39.32 mm (p < 0.001), and a decrease of Bright Liver Score from 1.96 ± 0.68 mm to 1.25 ± 0.81 mm (p < 0.0001).
Concurrent with these morphological changes, significant reductions of BMI, HOMA-IR, Western diet pattern score (WDS from 25.31 ± 8.50 to 21.29 ± 6.82; < 0.0001), LDL cholesterol, and triglycerides were observed (Table 1). Significant increases of the adherence to Mediterranean diet (AMDS from 27.12 ± 3.67 to 34.41 ± 2.53; < 0.0001), physical exercise (assessed by the Baecke questionnaire from 38.56 ± 3.55 to 44.11 ± 4.23; < 0.0001), and HDL cholesterol were also observed.
Considering the features of NAFLD patients (21/150) that responded favorably to the intervention with the total disappearance of ultrasound bright liver, the most remarkable features, at the beginning of the intervention, were minor BMI, lower insulin resistance, greater adherence to Mediterranean diet, less prominent Western diet pattern, and greater physical activity (Table 2).
Positive direct correlation of BMI, insulin resistance (HOMA-IR), and Western diet pattern score vs. fatty liver severity, assessed by the BLS score, and an inverse correlation of the Adherence to Mediterranean Diet, assessed by AMDS, and of the physical activity score assessed by Baecke’s tool are observed only in univariate correlation (Figure 1). By the multiple linear regression model, using data at the beginning of the study, i.e., before intervention (Table 3), weighted by gender and age of the subjects, the severity of fatty liver appearance at US examination was explained significantly only by the greater score of the Western dietary pattern.

Linear regression of BMI, HOMA (insulin resistance), AMDS (Adherence to Mediterranean Diet Score), WDS (Western diet pattern score), and Baecke’s score (physical activity measure) vs. severity of fatty liver assessed by the ultrasound BLS (Bright Liver Score) before dietary and lifestyle intervention
Discussion
The feature of NAFLD and the intervention addressed to therapy and clinical risk management, quite alike for obesity and metabolic syndrome, are not neatly defined [31]. Nonetheless, the intervention on lifestyle, with changes in the sense of healthier diet with a concurrent increase of physical activity is generally granted as fruitful in several patients [32, 33]. Actually, NAFLD is a complex and chronic disease that does not yield to simplistic sounding solutions [34]. Other factors and nutrients can individually interfere, even coffee [35]. Other habits, such as sleep curtailment [36], noise exposure [37], wrong body self-perceptions [38], and even fashion clothing [39], may be associated with behavior prone to obesity and fatty liver. Apart of the possible interference of hepatotropic and adipotropic viruses, which may enhance fatty storage in the liver [40,41,42], the association of fatty liver with cardiovascular disease and arterial hypertension and with acute events can be a topic which encompasses joint risk factors [43,44,45].
Referral for NAFLD is a clinical subset, which may appropriately address, as a comprehensive clue, clinical risk management issues [44, 45]. This is particularly relevant due to the frequent association of fatty liver disease with other hepatic conditions, which can take advantage by an approach tailored and personalized within the NAFLD patients’ context [46, 47]. Many different experiences are available and very specific and sensitive subsets are peri-menopausal women [48,49,50], vitamin D deficiencies [51], and others which share the risk for metabolic syndrome and NAFLD, but, almost equally, for cardiovascular disease [43, 44]. The clinical approach with the target of improving liver imaging and function is often rewarding because the physician indicates to patients a tangible non-invasive goal. Suggestions and advice on individual “healthy” food purchase, storage, and cooking must be given, dealing with details and empowering the patients especially when a reliable feedback and evidence of patients’ adherence cannot be easily obtained using only scheduled dietician’s interviews.
From our results, it is likely that difference of caloric intake, leading to slight reduction of BMI and body weight, and the improvement of the quality of nutrition, as described by the effect of a greater adherence to the Mediterranean diet, are factors suitable for explaining, and conceivably achieving, a reduction or the disappearance of fatty liver in NAFLD. Withdrawal of putative unhealthy food, such as those definite by the Western diet pattern, is strongly associated with a more severe feature of fatty liver by US imaging and was explicitly addressed in our study after a preliminary specific detection and assessment. Nonetheless, this is not a sufficient explaining factor of the improvement that we achieved in our patients. It is more likely that pushing toward healthier food profiles and not only dissuading the patients from Western dietary food is needed to achieve a favorable effect, as we actually did.
Vigorous physical activity ameliorates insulin resistance, maintains weight loss, and improves liver histology [17,18,19,20]. Slight or moderate exercise did not provide any relevant benefit on the occurrence of NAFLD, and an inverse association of vigorous total exercise with the severity of NAFLD is observed [19]. We strongly agree that “there are no universally accepted criteria for the quantity and quality of evidence required to warrant a public policy around a health issue” [24]. The potential and the role of the medical doctors are often neglected in this regard: a proactive counseling addressed to healthy gastronomy can counteract, also in the prescriptions of dietitians and medical doctors, use, promotion, and marketing of unhealthy food.
Our study has the limitations that it is not a randomized trial and this could reduce the power of the results; moreover, the study is based on self-reported data and, for that, can contain several potential sources of bias.
Conclusion
The assessment of some features of the Western diet is possible, and the size of this dietary pattern is associated with a greater severity of fatty liver as detected by an ultrasound in NAFLD. Focusing to these putative detrimental components of a diet, apart from alcohol, should be greatly addressed in the clinical practice with benefits for counteracting obesity and fatty liver disease.
References
Popper H, Schaffner F. Nutritional cirrhosis in man? N Engl J Med. 1971;285:577–8.
Younossi ZM, Koenig AB, Abdelatif D, Fazel Y, Henry L, Wymer M. Global epidemiology of nonalcoholic fatty liver disease-meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology. 2016;64(1):73–84. https://doi.org/10.1002/hep.28431.
Ferreira SR, Lerario DD, Gimeno SG, Sanudo A, Franco LJ, Japanese-Brazilian Diabetes Study Group. Obesity and central adiposity in Japanese immigrants: role of the Western dietary pattern. J Epidemiol. 2002;12:431–8.
Lopez CN, Martinez-Gonzalez MA, Sanchez-Villegas A, et al. Costs of Mediterranean and Western dietary patterns in a Spanish cohort and their relationship with prospective weight change. J Epidemiol Community Health. 2009;63:920–7.
Bouchard-Mercier A, Rudkowska I, Lemieux S, Couture P, Vohl MC. The metabolic signature associated with the Western dietary pattern: a cross-sectional study. Nutr J. 2013;12:158.
Abenavoli L, Greco M, Milic N, Accattato F, Foti D, Gulletta E, Luzza F. Effect of Mediterranean diet and antioxidant formulation in non-alcoholic fatty liver disease: a randomized study. Nutrients. 2017;9(8) https://doi.org/10.3390/nu9080870.
Naja F, Hwalla N, Itani L, Karam S, Sibai AM, Nasreddine L. A Western dietary pattern is associated with overweight and obesity in a national sample of Lebanese adolescents (13–19 years): a cross-sectional study. Br J Nutr. 2015;114:1909–19.
Bonaccio M, Iacoviello L, de Gaetano G, Moli-Sani Investigators. The Mediterranean diet: the reasons for a success. Thromb Res. 2012;129:401–4.
Gelli C, Tarocchi M, Abenavoli L, Di Renzo L, Galli A, De Lorenzo A. Effect of a counseling-supported treatment with the Mediterranean diet and physical activity on the severity of the non-alcoholic fatty liver disease. World J Gastroenterol. 2017;23(17):3150–62. https://doi.org/10.3748/wjg.v23.i17.3150.
Catalano D, Trovato GM, Martines GF, Randazzo M, Tonzuso A. Bright liver, body composition and insulin resistance changes with nutritional intervention: a follow-up study. Liver Int. 2008;28:1280–7.
Trovato FM, Catalano D, Martines GF, Pace P, Trovato GM. Mediterranean diet and non-alcoholic fatty liver disease: the need of extended and comprehensive interventions. Clin Nutr. 2015;34:86–8.
Kontogianni MD, Tileli N, Margariti A, et al. Adherence to the Mediterranean diet is associated with the severity of non-alcoholic fatty liver disease. Clin Nutr. 2014;33:678–83.
Thomas EL, Brynes AE, Hamilton G, et al. Effect of nutritional counseling on hepatic, muscle and adipose tissue fat content and distribution in non-alcoholic fatty liver disease. World J Gastroenterol. 2006;12:5813–9.
Zelber-Sagi S, Salomone F, Mlynarsky L. The Mediterranean dietary pattern as the diet of choice for non-alcoholic fatty liver disease: evidence and plausible mechanisms. Liver Int. 2017;37:936–49.
Oddy WH, Herbison CE, Jacoby P, et al. The Western dietary pattern is prospectively associated with nonalcoholic fatty liver disease in adolescence. Am J Gastroenterol. 2013;108:778–85.
Trovato GM, Catalano D, Martines GF, Pirri C, Trovato FM. Western dietary pattern and sedentary life: independent effects of diet and physical exercise intensity on NAFLD. Am J Gastroenterol. 2013;108:1932–3.
Zelber-Sagi S, Ratziu V, Oren R. Nutrition and physical activity in NAFLD: an overview of the epidemiological evidence. World J Gastroenterol. 2011;17:3377–89.
van Baak MA, van Mil E, Astrup AV, et al. Leisure-time activity is an important determinant of long-term weight maintenance after weight loss in the Sibutramine Trial on Obesity Reduction and Maintenance (STORM trial). Am J Clin Nutr. 2003;78:209–14.
Kistler KD, Brunt EM, Clark JM, Diehl AM, Sallis JF, Schwimmer JB, NASH CRN Research Group. Physical activity recommendations, exercise intensity, and histological severity of nonalcoholic fatty liver disease. Am J Gastroenterol. 2011;106:460–8.
Tolman Asrih M, Jornayvaz FR. Diets and nonalcoholic fatty liver disease: the good and the bad. Clin Nutr. 2014;33(2):186–90.
Catalano D, Trovato GM, Pace P, Martines GF, Trovato FM. Mediterranean diet and physical activity: an intervention study. Does olive oil exercise the body through the mind? Int J Cardiol. 2013;168:4408–9.
Trovato GM, Martines GF, Trovato FM, Catalano D. Relation of the traditional Mediterranean diet to cerebrovascular disease in a Mediterranean population. Am J Epidemiol. 2013;178:661.
Misirli G, Benetou V, Lagiou P, Bamia C, Trichopoulos D, Trichopoulou A. Relation of the traditional Mediterranean diet to cerebrovascular disease in a Mediterranean population. Am J Epidemiol. 2012;176:1185–92.
Catalano D, Trovato FM, Pirri C, Trovato GM. Outpatient diagnosis and therapeutic units linked with ED referrals: a sustainable quality-centered approach. Am J Emerg Med. 2013;31:1612.
Trovato GM, Catalano D, Martines GF, Pace P, Trovato FM. Mediterranean diet: relationship with anxiety and depression. Ann Neurol. 2014;75:613.
Trovato FM, Tognarelli JM, Crossey MM, Catalano D, Taylor-Robinson SD, Trovato GM. Challenges of liver cancer: future emerging tools in imaging and urinary biomarkers. World J Hepatol. 2015;7:2664–75.
Trovato FM, Catalano D, Musumeci G, Trovato GM. 4Ps medicine of the fatty liver: the research model of predictive, preventive, personalized and participatory medicine-recommendations for facing obesity, fatty liver and fibrosis epidemics. EPMA J. 2014;5:21.
Mathiesen UL, Franzén LE, Aselius H, et al. Increased liver echogenicity at ultrasound examination reflects degree of steatosis but not of fibrosis in asymptomatic patients with mild/moderate abnormalities of liver transaminases. Dig Liver Dis. 2002;34:516–22.
Baecke JA, Burema J, Frijters JE. A short questionnaire for the measurement of habitual physical activity in epidemiological studies. Am J Clin Nutr. 1982;36:936–42.
Rutter MK, Wilson PW, Sullivan LM, Fox CS, D' Agostino RB Sr, Meigs JB. Use of alternative thresholds defining insulin resistance to predict incident type 2 diabetes mellitus and cardiovascular disease. Circulation. 2008;117:1003–9.
Musso G, Gambino R, Cassader M, Pagano G. A meta-analysis of randomized trials for the treatment of nonalcoholic fatty liver disease. Hepatology. 2010;52:79–104.
Masuzaki R, Karp SJ, Omata M. NAFLD as a risk factor for HCC: new rules of engagement? Hepatol Int. 2016;10:533–4.
Chalasani N, Younossi Z, Lavine JE, et al. The diagnosis and management of non-alcoholic fatty liver disease: practice guideline by the American Association for the Study of Liver Diseases, American College of Gastroenterology, and the American Gastroenterological Association. Am J Gastroenterol. 2012;107:811–26.
Dhurandhar NV. Health policies for obesity: how to get there. Int J Obes. 2017;41:829–30.
Catalano D, Martines GF, Tonzuso A, Pirri C, Trovato FM, Trovato GM. Protective role of coffee in non-alcoholic fatty liver disease (NAFLD). Dig Dis Sci. 2010;55:3200–6.
Trovato G, Pace P, Martines GF, Brischetto D. Mala-movida: late bed-timing and wake-up induce malnutrition and underweight in youngsters. Chronobiol Int. 2014;31:945–6.
Trovato G, Brischetto D, Martines GF. Teens’ obesity, noise and sleep deprivation: a perverse liaison. Let’s move beyond movida. Obesity (Silver Spring). 2014;22:1209.
Trovato G, Brischetto D, Pace P, Fabio Martines G. Perceived body weight status of youngsters interferes with headache in obese and non-obese subjects. Headache. 2014;54:1062–3.
Trovato FM, Martines GF, Brischetto D, Catalano D, Musumeci G, Trovato GM. Fatty liver disease and lifestyle in youngsters: diet, food intake frequency, exercise, sleep shortage and fashion. Liver Int. 2016;36:427–33.
Trovato FM, Catalano D, Garozzo A, Martines GF, Pirri C, Trovato GM. ADV36 adipogenic adenovirus in human liver disease. World J Gastroenterol. 2014;20:14706–16.
Trovato GM, Martines GF, Pirri C, et al. Obesity-independent association of human adenovirus Ad37 seropositivity with nonalcoholic fatty liver disease. J Clin Gastroenterol. 2012;46:e46–54.
Trovato GM, Martines GF, Garozzo A, et al. Ad36 adipogenic adenovirus in human non-alcoholic fatty liver disease. Liver Int. 2010;30:184–90.
Trovato FM, Martines GF, Catalano D, Musumeci G, Pirri C, Trovato GM. Echocardiography and NAFLD (non-alcoholic fatty liver disease). Int J Cardiol. 2016;221:275–9.
Trovato GM. Clinical research and methodology. The paradigm of fatty liver and atherosclerosis behind the chicken or the egg dilemma. Atherosclerosis. 2016;249:228–9.
Park YM, Steck SE, Fung TT, et al. Mediterranean diet, Dietary Approaches to Stop Hypertension (DASH) style diet, and metabolic health in U.S. adults. Clin Nutr. 2017;36(5):1301–9.
Sobhani V, Ghamar Chehreh ME, Alavian SM, Zaree A. Effect of aerobic and resistance exercise training on liver enzymes and hepatic fat in Iranian men with nonalcoholic fatty liver disease. Hepat Mon. 2015;15:e31434.
Younossi Z, Henry L. Contribution of alcoholic and nonalcoholic fatty liver disease to the burden of liver-related morbidity and mortality. Gastroenterology. 2016;150:1778–85.
Catalano D, Trovato GM, Spadaro D, et al. Insulin resistance in postmenopausal women: concurrent effects of hormone replacement therapy and coffee. Climacteric. 2008;11:373–82.
Hamaguchi M, Kojima T, Ohbora A, Takeda N, Fukui M, Kato T. Aging is a risk factor of nonalcoholic fatty liver disease in premenopausal women. World J Gastroenterol. 2012;18:237–43.
Wang Z, Xu M, Hu Z, Shrestha UK. Prevalence of nonalcoholic fatty liver disease and its metabolic risk factors in women of different ages and body mass index. Menopause. 2015;22:667–73.
Lee SM, Jun DW, Cho YK, Jang KS. Vitamin D deficiency in non-alcoholic fatty liver disease: the chicken or the egg? Clin Nutr. 2017;36:191–7.
Acknowledgements
Authors thank Professor Guglielmo Trovato for his important intellectual contribution in the conception and critical revision of this paper.
Funding
The authors have no funding to report.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on a reasonable request.
Author information
Authors and Affiliations
Contributions
FMT, GFM, and DC contributed to the design and implementation of the research, to the analysis of the results, and to the writing of the manuscript. All authors are in agreement with the manuscript and declare that the content has not been published elsewhere. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study and the manuscript were approved by the Institutional Review Board of the Policlinico’s Project Office.
Consent for publication
Written informed consent was obtained from each patient prior to the clinical data recording and before the US procedure, allowing the use of information for teaching and clinical research.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Trovato, F.M., Martines, G.F. & Catalano, D. Addressing Western dietary pattern in obesity and NAFLD. Nutrire 43, 11 (2018). https://doi.org/10.1186/s41110-018-0067-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41110-018-0067-0