
Abstract
Background
S100A14 is a novel significant individual from S100 proteins family. Its significance is because of its part in tumorigenesis and metastasis process. Elevated level of S100A14 was associated with poor tumor differentiation. A relatively high dose of S100A14 was capable to induce cell injuries. It was discovered that S100A14 is seen at the extracellular medium. S100A14 induces the activation of apoptotic mediators and cell apoptosis. The aim of this study is to assess the clinical response of S100A14 in the detection the stages of liver fibrosis in patients of chronic HCV. ELISA was used to detect the levels of serum S100A14 in both different stages of fibrosis of the liver and control groups, and then, they were noticed together with the results of fibroscan. Other noninvasive markers of fibrosis were calculated such as APRI, AAR, and FIB-4 score.
Results
Protein expression level of S100A14 was positive correlated significantly with stages of fibrosis.
Conclusion
Measurement of serum level of S100A14 is a useful non-invasive marker for detection of the stages of liver fibrosis in patients of chronic HCV. Combinations of measuring S100A14 level to FIB-4 or S100A14 to APRI give a sensitive tool for diagnosing significant fibrosis.
Similar content being viewed by others

Background
Worldwide, morbidity and mortality are caused most likely by hepatic fibrogenesis due to obesity-related disease of the fatty liver and chronic viral hepatitis. The activation of hepatic stellate cell is the inevitable essential event in fibrosis, and they become the primary source of extracellular matrix (ECM) in the liver after injury [1]. Liver diseases with many types lead to liver fibrosis by means of signaling networks integrated that control the sedimentation of extracellular matrix. This cascade of responses drives the activation of hepatic stellate cells (HSCs) into a myofibroblast-like phenotype which is contractile, proliferative, and fibrogenic. Components of ECM including collagen are precipitated as the liver creates an injury-encapsulating a response for wound-healing. Sustained fibrogenesis contributes to cirrhosis, characterized by hepatic parenchyma distortion and vascular architecture. The conception of the complex mechanisms attached to liver fibrogenesis is essential to evolve targeted therapies with anti-fibrotic ability which can enhance the recovery of chronic liver disease patients [2]. The hazard of promote cirrhosis depends on the stages of fibrosis in the liver [3]. Fibroscan is a noninvasive test that replaces liver biopsy [4]. Fibrosis biomarkers can only be direct or indirect markers. Both types of markers can be individually used or in combination which is frequently happening to increase the diagnostic reliability [5, 6]. There are multiple biological processes that the protein family of S100 has been reported to participate, such as cell motility, growth, transcription, signal transduction, apoptosis, and cell survival, which were correlated to tumorigenesis and normal development [7]. Small calcium binding proteins which are great subgroup of the EF-hand protein family were noticed to be the S100 proteins which have a wide range of extracellular and intracellular functions [8]. The proteins S100 belong to a great subgroup of 25 acidic, small proteins that are described by distinctive homo-or hetero-dimeric architecture and EF hand Ca2+-binding motifs, and which were expressed in a various types of cells [9]. An epic individual from S100 protein is S100A14. In new HCC tissues with and without vascular intrusion, the mRNA and protein levels of S100A4 were found to connect with different tumor hubs and vascular attack. Moreover, S100A14 revelation related with both abbreviated illness free endurance and in general endurance in HCC patients, thus proving its potential as prognostic factor. The part of S100A14 in continuing HCC multiplication, movement, and attack was affirmed in HCC cell culture and in vivo (mice) investigation, hence supporting the function of S100A14 in supporting HCC metastasis [10]. S100A14 is also an objective for p53 and could alter p53 stability and transactivity and by controlling the transcription of matrix metalloproteinase (MMP) 2, and the invasiveness of the cell can be affected by S100A14 in a p53-dependent manner [11]. Higher levels of S100A14 are measured in several types of cancer, including lung, ovarian, cervical, breast, and uterine cancer [8]. We were aiming in this study to discover the clinical efficiency of the level of S100A14 as a marker for detection of the liver fibrosis stages in Egyptian patients.
Methods
This study is a descriptive cross-sectional one had been carried out in the National Hepatology and Tropical Medicine Research Institute (NHTMRI) in the period between April 2019 till December 2019, on ninety person classified into two groups: (I) control group: twenty healthy individuals aged 20–60 years with mean ± SD of 29.85 + 8.57 years without any evidence of liver diseases (by normal excretory and synthetic liver function tests, negative HCV PCR, negative HBS Ag, and with ultrasonography that show no hepatic focal lesion , no fatty liver, no ascites, normal liver parenchyma, and normal portal vein diameter); (II) fibrosis group, chronic HCV groups with different stages of fibrosis as inclusion criteria: seventy patients aged 25–60 years with mean ± SD for 49.97 + 8.13 years. The subjects in the patients group were selected from in and out patients of NHTMRI, and the healthy relatives of patients were selected as the control group. Fibroscan test detected fibrotic liver patients, and chronic HCV patients were diagnosed by positive HCV antibody by ELISA and positive PCR. Fibrosis stages from (F0–F6) were chosen to be our categories for HCV patients. The non-invasive markers of fibrosis, involving AAR, APRI, and FIB-4 score were measured. Other former studies have announced other noninvasive markers for predicting hepatic fibrosis, including AAR [12], APRI [13], and FIB-4 [14]. The quantitative determination of Human S100A14 concentrations were detected by ELISA Kit of Glory Science Company, Ltd., USA [15]. The exclusion criteria were patients affected by any clinically significant diseases. The sample was taken from both patients and controls with 3 mL of the peripheral blood. For measuring serum S100A14 levels, all the blood samples were centrifuged and stored at 20 °C.
Statistics analysis
The data were statistically analyzed by the IBM SPSS version 20.The chi-squared test was used to compare between two groups with qualitative data. The independent t test was used to compare between two groups with quantitative data and parametric distribution. Mann-Whitney test was used to compare between two groups with quantitative data and non-parametric distribution. ANOVA test was used to compare between more than two groups with quantitative data and parametric distribution and Kruskall-Wallis test was used to compare between more than two groups with quantitative data and non-parametric distribution. ROC curve was used to give diagnostic accuracy. The level of probability p value indicated the significant levels where P < 0.01: highly significant (HS), P < 0.05: significant (S) and P > 0.05: non-significant (NS).
Results
In the comparison between the fibrosis group ( according to fibroscan) and control group as regards demographic data with age shows a highly statistically significant in the fibrosis group than in the control group, but with sex, there is no statistically significant as regards studied groups. As shown in Table 1.
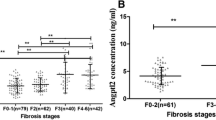
All basically prepared clinical and biochemical data of patients were collected. Platelets with mean and SD of 111.71 + 71.43, AST with 38.14 + 20.93, ALT with 38.03 + 24.757, and albumin with 2.4 + 0.61. Statistically, there is a high significant increase in fibrosis group compared to the control group which can be noticed at Table 2 and Fig. 1 upon the comparison between the fibrosis group and control group as regards S100A14.

The error bar graph of S100A14
Both Table 3 and Fig. 2 present the following: the specificity and sensitivity of S100A14 are 88.57% and 100.0%, respectively, at the cutoff point of > 0.38 ng/ml with AUC of 0.964.

Receiver operating characteristics analysis for AAR, APRI, FIB-4, and S100A14
In the relation between S100A14 as regards sex and the stages of fibrosis, in the fibrosis group shows that S100A14 has no significant correlation between males and females and has positive correlation with stages of fibrosis as shown in Table 4.
Table 5 presents the comparison between all non-invasive markers in different fibrosis stages. Overall, there is a positive association between S100A14 and AAR, APRI and FIB-4 in the patient group of fibrosis as shown in Table 5.
APRI is the best performance in our study to differentiate significant fibrosis, with an AUROC of 88%, in comparison to existed models, AAR and FIB-4 with AUROCs of 68% and 81%, respectively, as shown in Fig. 2. Compared to the existing non-invasive assessments, S100A14 is superior to AAR which (AUC = 68%), for predicting significant fibrosis (F ≥ 2). At the ROC-derived optimum cutoffs, the sensitivity for APRI (> 0.5) is 74% and the specificity is 97% (AUROC, 88%); for AAR (> 0.9), the sensitivity is 72% and the specificity 64% (AUROC, 68%); and for FIB-4 (> 1.6), the sensitivity is 66% and specificity is 94% (AUROC, 81%) as shown in Table 3. S100A14 is performing as the first for detecting the significant fibrosis with AUROC (96.4%), APRI is the second with AUROC (88%), and FIB-4 is the third with AUROC (81%), but after the combination, their diagnostic performance for significant fibrosis enhances with AUROC (98.5%) for S100A14 and APRI and with AUROC (97.5%) for S100A14 and FIB-4 to be higher than AUROC of either one of them alone. AUC of Combination S100A14 and AAR (with AUROC (87.5%)) is lower than combination (S100A14 and APRI) or combination (S100A14 and FIB-4) as shown in Table 6.
Discussion
Amassing proof has indicated that S100 proteins have been ensnared in tumorigenesis and metastasis [16]. Expanding proof demonstrated the significance of S100 family in cell movement, attack, and malignant growth metastasis [17]. In the extracellular medium, many members of S100 family are found with multiple extracellular roles [18, 19]. High dose of S100A14 triggers apoptosis, and the production of ROS was increased. Therefore, exogenous S100A14 induces apoptosis or catalyze cell proliferation at various concentrations via RAGE ligation [20]. A multiligand receptor of the superfamily of immunoglobulin (RAGE) is constitutively secreted during embryonic growth, but its expression in physiological states is downregulated in life of adult [21]. Multiple families of ligands are bond to RAGE, such as amphoterin, S100s, and advanced glycation end products (AGEs), and play a key role in cancer, inflammation, and diabetes [22, 23]. High expression of S100A14 also causes displaying a PARP, cell apoptosis, and caspase-9 cleavage, as well as a decrease in the potential of the mitochondrial membrane. Nac(N-acetyl cysteine) is a ROS inhibitor, inhibited high dose of S100A14 induced injuries, point that S100A14-induced apoptosis was likely dependent on accumulation of intracellular ROS [20]. The current work shows that in the patients of liver fibrosis, S100A14 exerts a significant increase than normal people and a significant increase with stages of liver fibrosis. We have explained that S100A14 can react with RAGE, whereas high doses of S100A14 stimulated apoptosis in a RAGE-mediated and oxidant-dependent manner. Liver biopsy is still the gold standard for evaluating liver fibrosis and diagnosing cirrhosis, but being such invasive model with particular unavoidable risks, poor repetitiveness are considered disadvantages, which limit its clinical applications for patients with end-stage liver diseases [24]. Recent years, many methods and models designed for diagnosing liver fibrosis have brought the diagnosis of liver fibrosis into a non-invasive period. Although these diagnosis techniques were not replaced by liver biopsy, they have non-trauma, convenience, and good repetition advantages; moreover, these techniques have high accuracy rate of diagnosis on hepatic fibrosis to prevent some patients from receiving liver biopsy [5, 25]. Between consequent fibrosis stage, we found the mean values of APRI and FIB-4 were significantly higher (P < 0.05). For each stage of fibrosis, no differences for AAR were detected (P > 0.05, except for S1 VS S2-4, P = 0.037). We found a significant correlation between S100A14 and AAR and a positive correlation between S100A14 in different fibrosis stages and APRI, FIB- 4[26]. In order to increase the diagnostic effectiveness of non-invasive tests, combined models using two or more tests for liver biopsy have been performed [27].
Conclusion
The study revealed the importance of S100A14 expression protein level as a sensitive tool in detection the stages of liver fibrosis. Combination of S100A14 and APRI or S100A14 and FIB-4 offered a simple potency to diagnose significant fibrosis, and its performance was specific and sensitive tool in comparison to the existing scores AAR, APRI, and FIB-4.
Limitation of study
In our study, there is a limitation relatively small sample sizes of the control group comparing to disease group. Finally, if the number of the control group were at least equal to the diseased group, it would have been more fitting.
Recommendation
To confirm this finding, large sample sizes are recommended.
Availability of data and materials
All data generated or analyzed during this study are included in this published article [and its supplementary information files].
Abbreviations
- FIB-4:
-
Fibrosis-4
- APRI:
-
AST/platelet ratio index
- AAR:
-
Aspartate amino transferase/alanine amino transferase ratio
References
Virginia H, Scott L (2011) Pathogenesis of liver fibrosis. Annu Rev Pathol Mech Dis 6:425–456. https://doi.org/10.1146/annurev-pathol-011110-130246 PMID: 21073339
Ursula E, Scott L (2011) Mechanisms of hepatic fibrogenesis. Best Pract Res Clin Gastroenterol 25(2):195–206. https://doi.org/10.1016/j.bpg.2011.02.005 PMID: 21497738 PMCID: PMC3079877
Chengzhao L, Fuchu H, Haijian W, Jie L, Jiyao W et al (2010) Peroxiredoxin 2: a potential biomarker for early diagnosis of hepatitis B virus related liver fibrosis identified by proteomic analysis of the plasma. BMC Gastroenterol 10:115. https://doi.org/10.1186/1471-230X-10-115 PMID: 20939925 PMCID: PMC2959091
Nezam H (2012) Fibroscan (transient elastography) for the measurement of liver fibrosis. Gastroenterol Hepatol (N Y) 8(9):605–607 PMCID: PMC3594956; PMID: 23483859
Baranova A, Lal P, Birerdinc A, Younossi ZM (2011) Non-invasive markers for hepatic fibrosis. BMC Gastroenterol 11:91. https://doi.org/10.1186/1471-230X-11-91 [PMC free article] [PubMed] [Google Scholar]. PMCID: PMC3176189; PMID: 21849046
Ruseva A, Pencheva B, Stoeva D, Mihaylov R (2017) Non-invasive diagnostics of liver fibrosis. Acta Medica Bulgarica 44(1):50–56 https://doi.org/10.1515/amb-2017-0009
Min Z, Hongyi W, Jiantao C, Wenmei L, Guo A et al (2017) Calcium-binding protein S100A14 induces differentiation and suppresses metastasis in gastric cancer. Cell Death Dis 8:e2938. https://doi.org/10.1038/cddis.2017.297 PMID: 28726786 PMCID: PMC5550849
Wang X, Yang J, Qian J, Liu Z, Chen H, Cui Z (2015) S100A14, a mediator of epithelial-mesenchymal transition, regulates proliferation, migration and invasion of human cervical cancer cells. Am J Cancer Res 5:1484–1495 PMID: 26101712 PMCID: PMC4473325
Mizuko T, Naoki I, Namiko S, Keisuke N, Tomiko M et al (2015) Co-expression of S100A14 and S100A16 correlates with a poor prognosis in human breast cancer and promotes cancer cell invasion. BMC Cancer 15:53. https://doi.org/10.1186/s12885-015-1059-6 PMID: 25884418; PMCID: PMC4348405
Zhao FT, Jia ZS, Yang Q, Song L, Jiang XJ (2013) S100A14 promotes the growth and metastasis of hepatocellular carcinoma. Asian Pac J Cancer Prev 14:3831–3836. https://doi.org/10.7314/apjcp.2013.14.6.3831 [PubMed] [Google Scholar]
Yang Z, Feng Y, Weifeng T, Haiyong G, Heng Z (2017) S100A14 rs11548103 G>A polymorphism is associated with a decreased risk of oesophageal cancer in a Chinese population. Oncotarget 8(49):86917–86923. https://doi.org/10.18632/oncotarget.20868 PMID: 29156846 PMCID: PMC5689736
Williams AL, Hoofnagle JH (1988) Ratio of serum aspartate to alanine aminotransferase in chronic hepatitis. Relationship to cirrhosis. Gastroenterology 95:734–739. https://doi.org/10.1016/S0016-5085(88)80022-2 [PubMed] [CrossRef] [Google Scholar]PMID: 3135226
Wai CT, Greenson JK, Fontana RJ, Kalbfleisch JD, Marrero JA, Conjeevaram HS (2003) A simple noninvasive index can predict both significant fibrosis and cirrhosis in patients with chronic hepatitis C. Hepatology 38:518–526. https://doi.org/10.1053/jhep.2003.50346
Sterling RK, Sulkowski M, Torriani FJ, Dieterich DT, Thomas DL et al (2006) Development of a simple noninvasive index to predict significant fibrosis in patients with HIV/HCV co-infection. Hepatology 43:1317–1325. https://doi.org/10.1002/hep.21178 [PubMed] [CrossRef] [Google Scholar]
Pietas A, Schlüns K, Marenholz I, Schäfer BW, Heizmann CW, Petersen I (2002) Molecular cloning and characterization of the human S100A14 gene encoding a novel member of the S100 family. Genomics. 79(4):513–522
Lukanidin E, Sleeman JP (2012) Building the niche: the role of the S100 proteins in metastatic growth. Semin Cancer Biol 22:216–225. https://doi.org/10.1016/j.semcancer.2012.006
Boye K, Maelandsmo GM (2010) S100A4 and metastasis: a small actor playing many roles. Am J Pathol 176:528–535. https://doi.org/10.2353/ajpath.2010.090526
Sparvero SLLJ, Asafu-Adjei D, Kang R, Tang D, Amin N et al (2009) RAGE (Receptor for Advanced Glycation Endproducts), RAGE ligands, and their role in cancer and inflammation. J Transl Med 7:1479–1499. https://doi.org/10.1186/1479-5876-7-17 PMID: 19292913 PMCID: PMC2666642
Leclerc E, Fritz G, Vetter S, Heizmann C (2009) Binding of S100 proteins to RAGE: an update. Biochim Biophys Acta 1793:993–1007. https://doi.org/10.1016/j.bbamcr.2008.11.016 PMID: 19121341
Jin Q, Chen H, Luo A, Ding F, Liu Z (2011) S100A14 stimulates cell proliferation and induces cell apoptosis at different concentrations via receptor for advanced glycation end products (RAGE). PLoS One 6(4):e19375. https://doi.org/10.1371/journal.pone.0019375 PMCID: PMC3084824; PMID: 21559403
Bierhaus A, Humpert P, Morcos M, Wendt T, Chavakis T et al (2005) Understanding RAGE, the receptor for advanced glycation end products. J Mol Med 83:876–886. https://doi.org/10.1007/s00109-005-0688-7 PMID: 16133426
Heizmann C, Ackermann G, Galichet A (2007) Pathologies involving the S100 proteins and RAGE. Subcell Biochem 45:93–138. https://doi.org/10.1007/978-1-4020-6191-2_5 PMID: 18193636
Logsdon C, Fuentes M, Huang E, Arumugam T (2007) RAGE and RAGE ligands in cancer. Curr Mol Med 7:777–789. https://doi.org/10.2174/156652407783220697 PMID:18331236
Jung MK, Cho HJ, Lee HC, Park KS, Seo EH et al (2008) Comparison of transient elastography and hepatic fibrosis assessed by histology in chronic liver disease. Korean J Gastroenterol 51:241–247 [PubMed] [Google Scholar].PMID: 18516003
Anca T, Cojocariu C, Sfarti C, Singeap AM, Stanciu C (2012) Non-invasive evaluation of liver fibrosis in chronic hepatitis C. Rev Med Chir Soc Med Nat Iasi 116:135–138. https://doi.org/10.3748/wjg.v20.i40.14568 PubMed] [Google Scholar]; PMCID: PMC4209524; PMID: 25356021
Zhang Z, Wang G, Kang K, Wu G, Wang P (2016) The diagnostic accuracy and clinical utility of three noninvasive models for predicting liver fibrosis in patients with HBV infection. PLoS One 11(4):e0152757. https://doi.org/10.1371/journal.pone.0152757 PMCID: PMC4822783; PMID: 27050531
Lederkremer GZ, Webb M, Cytter-Kuint R, Shteingart S, Lurie Y (2015) Non-invasive diagnosis of liver fibrosis and cirrhosis. World J Gastroenterol 21(41):11567–11583. https://doi.org/10.3748/wjg.v21.i41.11567 PMCID: PMC4631961; PMID: 26556987
Acknowledgements
Great confession for all physicians in NHTMRI for their cooperation
Funding
Funding information is not available.
Author information
Authors and Affiliations
Contributions
WS was responsible for the practical part, data analyzing, and wrote the manuscript. BE was responsible for sample collection and classification and revision of the manuscript. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
From all study participants, the informed consent was obtained in writing and confirmed under the Ethical Committee of the research of the National Hepatology and Tropical Medicine Research Institute with number 11/2019.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Serag, W.M., Elsayed, B.E. Detection of liver fibrosis stages in patients with hepatitis C virus infection by non-invasive tool. Egypt Liver Journal 11, 9 (2021). https://doi.org/10.1186/s43066-021-00076-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43066-021-00076-w