
Abstract
Background
These updated guidelines aimed to provide appropriate and convenient guidelines for the treatment of various types of juvenile idiopathic arthritis (JIA).
Using the Delphi technique, this study was conducted to reach expert consensus on a treat-to-target management strategy for JIA. According to the PICO (patient/population, intervention, comparison, and outcomes) approach, the preliminary scientific committee identified a total of 17 key clinical questions. To assemble evidence on the advantages and dangers associated with JIA treatments, an evidence-based, systematic literature review was conducted. Researchers and clinicians with experience in JIA management were identified by the core leadership team. To establish a consensus on the management suggestions for JIA patients, a Delphi approach (2 rounds) was used.
Results
An online survey was applied to the expert panel (n = 27), and 26 of them completed both rounds. At the conclusion of round 2, a total of eighteen (18) recommendation items were gathered, which were divided into four sections to address the four key JIA categories. The percentage of those who agreed with the recommendations (ranks 7–9) ranged from 83.2 to 100% (average 86.8%). The phrasing of all 18 clinical standards identified by the scientific committee was agreed upon (i.e. 75% of respondents strongly agreed or agreed). Algorithms have been proposed for the management of JIA polyarthritis, oligoarthritis, and systemic JIA.
Conclusion
A wide and representative panel of experts initiated a consensus about the management of JIA. The created guidelines give a complete approach to the management of JIA for all healthcare professionals involved in its management, as well as a means of monitoring and evaluating these guidelines on a regular basis.
Similar content being viewed by others


Background
Juvenile idiopathic arthritis (JIA) is one of the most frequent chronic illnesses in children. JIA is predicted to affect one out of every 1000 children [1,2,3]. JIA is a heterogeneous set of arthritis types characterized by long-term joint inflammation that begins before the age of 16 and lasts longer than 6 weeks [4]. Its aetiology is unknown. The condition can affect one or more joints, and it can also cause additional systemic symptoms like fever or rash, as well as extra-articular inflammatory signs like uveitis.
With recent advancements in therapeutic approaches and the availability of a large number of treatment options for JIA, quick commencement of proper medical therapy has become critical in preventing lasting joint and organ damage. Furthermore, these advancements in JIA management have increased the chance of beneficial outcomes for children, such as better illness control. As a result, the treating healthcare practitioner is free to set even higher treatment goals, such as complete remission [5]. As a result, future therapy guidelines may contain an overarching aim of clinical remission or, at the very least, low disease activity [6].
At this time, there is a compelling argument about the impact of early diagnosis and expanded treatment options on standard paediatric rheumatology practice and whether it has made therapeutic medical decision-making more difficult for treating healthcare professionals, caregivers, and patients [7, 8]. Treatment recommendations are created to assist healthcare providers in a variety of ways, including encouraging the adoption of a consistent approach to care delivery, supporting the proper and effective use of available resources, and reducing the risk of inappropriate care [9].
Overall, the most significant potential advantage is an improvement in the patient’s quality of treatment and improved health outcomes.
While controlling disease activity is certainly the primary goal, attention should also be paid to the patients’ overall health, emotional well-being, and their functional, educational, social, and economic status. In 2018, the first recommendations for JIA in Egypt were released [10]. However, recommendations were made to update the methodology approach to ease the adoption of the treat-to-target (T2T) management strategy and make the decision-making process more transparent. Furthermore, considering that Egypt is a low- and middle-income country (LMIC), there is a significant difficulty in terms of limited resources and disparities in the management of this chronic condition. This was the main motive behind developing guidelines specific for Egyptian children living with JIA. By ensuring the optimum standards of care, all children with JIA would have the right to equitable access to the highest quality of clinical care, based on current evidence and delivered by appropriately resourced and experienced multidisciplinary teams. These standards of care are designed to help and support children and young people with JIA and their families, the treating healthcare professional teams, and the health authorities.
This work was carried out aiming at providing updated evidence-based management guidelines for children and adolescents with JIA in its various forms, adopting treat-to-target approach and incorporating recently published data. Recommendations for the treatment of chronic and acute JIA-associated uveitis were developed concomitantly and are included in these guidelines.
Method
Design
This was a multistep approach that followed the protocol for the “clinical, evidence-based, guidelines” (CEG) initiative (ethical approval code: 34842/8/21) to create an actionable clinical gold standard for treat-to-target management of inflammatory arthritic diseases. The process of developing the updated guidelines for treat-to-target JIA management had evolved through a pathway starting with the conduction of a scientific literature review and the involvement of experts’ opinions using a Delphi technique until the development of consensus regarding treatment options and desired outcome throughout the journey of this chronic disease.
The study design and procedures were developed using a qualitative synthesis of scientific evidence and consensus based on clinical experience and current scientific information. The Egyptian College of Pediatric Rheumatology spearheaded the campaign.
Study teams
Core team
Four experts with experience in paediatric rheumatology and one expert in uveitis make up the group. The team was in charge of overseeing and coordinating the project, helping to define the project’s scope and initial patient/population, intervention, comparison, and outcomes (PICO) questions and nominating the expert panel and authoring the book.
Literature review team
An experienced literature review consultant is in charge. The team finished the literature search, data abstraction, and evidence quality assessment.
Expert panel
The core leadership team nominated 27 participants. The criteria for their selection included professional knowledge and experience (at least 8 years of experience) in the field of paediatric rheumatology, its management and practice in the Egyptian health system, and active participation in scientific research on paediatric rheumatic diseases.
Scientific literature review
In concordance with the scientific team’s previous guidelines [10], it was agreed to set the current guidelines on broad clinical phenotypes rather than ILAR categories. The patient populations addressed in this guideline included (1) polyarticular JIA; these are children with JIA and nonsystemic polyarthritis (≥ 5 joints ever involved), whether rheumatoid factor positive or negative, psoriatic arthritis, and undifferentiated arthritis; (2) oligoarticular and extended oligoarticular JIA; (3) systemic JIA; and (4) enthesitis/spondylitis-related JIA (Supplement 1).
Inclusion criteria
Systematic reviews, randomized controlled trials (RCTs), uncontrolled trials, and observational studies such as cohort, case-control, and cross-sectional studies were among the articles included.
Exclusion criteria
Editorials, commentaries, conference abstracts, and narrative/personal reviews that were not based on evidence were excluded.
Formulation of PICOs
Using the PICO (population, intervention, comparator, outcome) structure [11], a preliminary scientific committee (5 members) has undertaken the task of identifying the key clinical topics, aiming at (1) defining the research questions and (2) developing criteria for selection of studies to be reviewed by the expert panel in the development of clinical and therapeutic recommendations for the children and adolescents living with JIA. The PICO framework aided in the identification of a precise definition of a group of participants (population), clear reporting of drug exposures (intervention) (Supplement 2) and control group interventions (comparator), and well-defined and clearly specified effect (outcomes) (Supplement 3) of the intervention under consideration. The scientific committee developed this guideline by formulating seventeen PICO research topics (Table 1).
A systematic search including a series of literature searches in the database MEDLINE/PubMed and the Cochrane Library for human studies published in English focusing on JIA management until the present was conducted on 1st January 2021. For each PICO question, the review was undertaken to accumulate evidence for the benefits and harms associated with treatments. All of the studies found were read in their entirety. Papers that were not related to the main theme (e.g. for a sickness or medicine) were not accepted.
Critical appraisal of identified studies
The degree of evidence in each of the included studies was determined using Oxford standards for evidence-based levels of evidence [12]. The levels of evidence that were employed in the analyses are indicated in the table below (Supplement 4). In terms of confidence and study design, evidence levels are a good indicator of quality. The experts’ assessment of the clinical conclusions of the studies was combined with the definition of the evidence levels in defining the recommendations.
Consensus process
Two Delphi rounds were carried out to establish consensus regarding the T2T strategy in JIA. Once the main aspects of this strategy were identified, a discussion group has defined the aspects to be included in the questionnaire with the scientific committee. The structured Delphi approach ensures that the opinions of participants are equally considered, and it is particularly conforming to geographically diverse centres as in Egypt. The Delphi process was conducted through online questionnaires.
Delphi process
The Delphi method is an organized way for gathering vital information about a certain issue that is extensively used. It is based on the main assumption that group projections are often more accurate than individual forecasts. The Delphi method’s goal is to build consensus forecasts from a group of experts in a structured iterative manner. Its methodology is based on the completion of a series of questionnaires or “rounds” directed at experts.
The Delphi approach is usually divided into the following stages:
-
(1)
A panel of specialists is assembled.
-
(2)
Forecasting jobs and problems are distributed among professionals.
-
(3)
Preliminary projections and arguments are provided by experts. In order to provide input, the core team compiles and summarises them.
-
(4)
Experts receive feedback and utilize it to alter their projections in light of it. This approach can be repeated until an acceptable level of consensus is reached.
-
(5)
The expert forecasts are combined to form the final forecasts. This technique has two significant advantages: participant anonymity and regulated feedback [13,14,15].
Chronogram of Delphi rounds
The first round took place between 5th and 8th March 2021 (3 days). Aspects on which there was no agreement in the first round were amended in light of the feedback and incorporated in the second round. The second round took place 1 week after the first and lasted 3 days, from March 11 to March 13, 2021.
Voting process
Live online voting was conducted in two rounds, each with a strict time limit. All members of the expert panel were invited to take part and were given advance notice of the start and end times of each round of voting. Anonymous votes were gathered and evaluated, and unique access links were sent out. At the same time as the voting procedure, comments on rephrasing, potential ambiguity, and unidentified overlaps were received for each statement. The statements could only be voted on by members of the expert panel.
Rating
Each statement was scored on a scale of 1 to 9, with 1 representing “total disagreement” and 9 representing “complete agreement”. Disagreement, uncertainty, and agreement are represented by the numbers 1–3, 4–6, and 7–9.
If a comment is outside of a member’s area of expertise, they should refrain from speaking. As a result, a vote of “uncertainty” shows “dissatisfaction with the recommendation’s truthfulness”. All statements allow for comments, which are reviewed by the core team after each round of voting. In the second round of voting, members were also urged to submit plausibility comments wherever they voted a disagreement. This will allow the panel to notice a misinterpretation of a statement and invalidate the vote on that remark.
Definition of consensus
Prior to data analysis, a definition of consensus was defined. It was determined that if at least 75% of participants attained agreement (scoring 7–9) or disagreement (score 1–3), consensus would be achieved [16,17,18,19]. If a statement received a mean vote of less than 4 or a “poor” degree of agreement, it was retired. In view of the feedback, statements with an uncertainty score of (4–6) were changed. The levels of agreement on each statement of suggestion were considered as “high” if all votes on a statement fell into the agreement bracket following the second round of voting [15, 20, 21].
Ethical aspects
This study was performed in accordance with the Helsinki Declaration. According to national regulations, ethics approval was not required. All participants in the study were required to give verbal informed consent in accordance with Egyptian national ethical committee requirements. In accordance with data protection standards, all participants were separated from the results and kept anonymous.
Results
Literature research and evidence selection
The study selection process revealed that 6843 potentially relevant studies were identified by the search strategy. By reviewing the titles and abstracts, 6597 were ruled out (studies did not examine population or intervention of interest, did not match study design of interest, or did not report outcome measures of interest). As a result, the comprehensive article review included 246 relevant articles. One-hundred fifty-seven studies were eliminated because the citations did not fit the PICO. In a re-evaluation of the literature, two more studies were discovered. As a result, this research contained 91 studies.
Expert panel characteristics
The Delphi form was sent to expert panel (n = 27), of whom 26 (96.3%) participated in the two rounds. Respondents were drawn from different governorates and health centres across Egypt: Cairo University (25.9%), Ain Shams University (15.4%), Tanta University (7.4%), Benha University (3.7%), Alexandria University (7.4%), Suez Canal University (7.4%), Zagazig University (7.4%), Minia University (3.7%), Mansoura University (3.7%), Fayoum University (3.7%), Assiut University (3.7%), Menoufia University (3.7%), and Sohag University (3.7%).
Delphi round 1
The response rate for round 1 was 100% (27/27). The consensus was reached on the inclusion of clinical standards on 82.6% of the items (i.e. ≥ 75% of respondents strongly agreed or agreed). There were comments raised regarding the wording of some of the recommendations. Comments (excluding minor editing suggestions) were more frequent for general principles, polyarthritis section especially usage of corticosteroids, cDMARDs, and biologics. Diversity of opinion was greatest for the item “using sulfasalazine in some cases of polyarticular JIA”. Three statements were retired, one on the use of anti-TNFs as initial therapy in polyarticular JIA and 2 statements for similarities to other statements. Following round 1, the following statements were added: 7, 3, 4, 1, and 7 statements in polyarticular, oligoarticular, enthesitis/spondylitis-related JIA, systemic JIA, and uveitis sections, respectively. Several statements were revised after round 1, most edited statements were in polyarticular JIA section (7 statements), only one statement was edited in uveitis section, and 4 statements were edited in each other sections (oligoarticular, enthesitis/spondylitis-related JIA and systemic JIA).
Delphi round 2
The response rate for round 2 was 96.3% (26/27). The percentage of high-rank recommendations (ranks 7–9) ranged from 83.2 to 100%. One statement was removed because it was too similar to another. On all of the clinical standards, there was agreement (i.e. 75% of respondents strongly agreed or agreed). Table 2 also shows the level of evidence assigned to each statement, in accordance with the Oxford Centre for Evidence-Based Medicine (CEBM) criteria as well as mean ± standard deviation and level of agreement. Agreement was unanimous (> 80% agreement) for the wording of the statements.
Recommendations for the initial and subsequent treatment of children and adolescents with JIA
At the end of round 2, a total of eighteen (18) recommendation items were gathered, which were divided into four sections to address the four key JIA categories. A breakdown is presented in Table 2.
Application of the primary recommendations to clinical practice guidelines
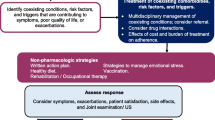
Figure 1 shows a summary of primary recommendations for the initial and follow-up therapy of children with juvenile idiopathic arthritis (JIA) and active polyarthritis (1), whereas Fig. 2 shows the management pathway (algorithm) for oligoarthritis JIA, and Fig. 3 shows a suggested treat-to-target approach for systemic JIA. Figure 4 is the treat-to-target management algorithm for systemic JIA, whereas Fig. 5 is the treatment algorithm for chronic anterior uveitis associated with juvenile idiopathic arthritis.

Flow chart for the study selection process

A summary of primary recommendations for the treat-to-target management of children with juvenile idiopathic arthritis (JIA) and active polyarthritis

Showing the treat-to-target management algorithm for oligoarthritis JIA

Showing a suggested treat-to-target management algorithm for systemic JIA

a Algorithm for screening, referral, and monitoring of chronic anterior uveitis in children and adolescents with JIA
Discussion
Juvenile idiopathic arthritis (JIA for short) is an umbrella term for arthritis of an unknown cause in children under the age of 16. JIA not only causes joint pain, swelling, and stiffness in one or more joints but also decreased health-related quality of life and risk of permanent joint damage. Furthermore, the condition can last well into adulthood, resulting in severe morbidity and poor quality of life [16, 17, 22]. For most individuals with JIA, recent therapy advancements have made remission a realistic goal. JIA has also been the subject of a lot of recent research, with a greater understanding of the underlying biology and more treatments available [5, 18]; hence, it was important to update the treatment guidelines to implement treat-to-target approach into standard practice and accommodate new lines of management.
This guideline defined patient populations based on their clinical phenotypes rather than ILAR categories. This decision was taken in view of the data reporting that the current JIA categories may not accurately reflect the underlying biology and anticipated treatment responses in patients with juvenile arthritis. Similar approach was adopted in the 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Treatment of Juvenile Idiopathic Arthritis [19]. This also aligns with the ongoing effort to standardise as many criteria as feasible for disorders that affect both children and adults, whether for use in clinical trials, research, or in regular clinical practice [23,24,25,26,27].
This guideline was developed based on a structured PICO process. This is in agreement with recent publications that provide recommendations for JIA treatment [4, 19]. The PICO framework is intended to assist researchers in formulating relevant and precise questions that can be answered in a systematic review structure, as well as to improve the specificity and conceptual clarity of clinical questions by breaking them down into smaller, more manageable components that are easier to identify during the literature search process [28].
The Delphi technique is a reliable tool for establishing new concepts and determining the direction of future-oriented research [29]. The technique enlists the help of a group of experts to assess the degree of agreement and settle disagreement on a topic [30]. There was broad agreement among the experts when asked about the feasibility of accomplishing a well-defined objective in osteoporosis. Almost everyone who contributed agreed that the treat-to-target technique may be used in JIA clinical practice. Consensus is reached in Delphi methodology when the percentage of people who agree or disagree is between 50 and 80% [31]. The agreement in our study varied from 83.4 to 100%, demonstrating a strong trend among Egyptian healthcare providers to use a T2T strategy for JIA management. The results of the American College of Rheumatology Guideline for the Treatment of Juvenile Idiopathic Arthritis support these findings [19], the international task force [5], and the German consensus-based strategies in diagnosing and managing systemic juvenile idiopathic arthritis [32] which revealed similar agreement on the treat to target policy.
Although the literature analysis did not reveal trials that compared a treat-to-target method to another or no strategy, it did provide indirect evidence of a better approach to therapy, which aided in the formation of recommendations. In 2018, an international task force issued recommendations for treating JIA with the goal of achieving [5]. The task force discussed particular treatment goals and the T2T technique for achieving them. Their recommendations were meant to provide professional advice on broad treatment options in order to improve patient care in normal clinical practice. This study went above and beyond by presenting a T2T approach to the various JIA categories. According to the task force, there are several goals for treating patients with JIA to target. These include the following: “to control signs and symptoms; to prevent structural damage; to avoid comorbid conditions and drug toxicities; and to optimise function, growth and development, quality of life, and social participation” [5]. The essential premise of a T2T strategy is that a treatment that is aggressively directed at the target will have “domino effects” on all other objectives [33,34,35].
In the absence of joints with overt active illness, treating to target in JIA necessitates a multimodal treatment plan that may include physiotherapy and early pain/fatigue coping strategies administered by a multidisciplinary team for children with tiredness or chronic pain [8, 36, 37]. Furthermore, while these treatment guidelines are meant to improve the quality of clinical decision-making, each individual case is unique, and this should be taken into account in everyday practice. The guidelines given indicated T2T-based algorithms for the management of JIA patients. Clinicians require information that is simple to understand and use. The treatment suggestions should spell out the right lines of management, how to keep track of the patient, and how to deal with refractory instances. Nonsteroidal anti-inflammatory medicines, disease-modifying antirheumatic therapies, biologics, and intra-articular and oral glucocorticoids are among the medications recommended in this guideline. There are additional suggestions for using physical and occupational therapy. Treatment algorithms were created to outline the implementation of treatment methods targeted at establishing and maintaining tight disease control in routine paediatric rheumatology practice.
This work is the first to include imaging as one of the critical outcomes assessed. Whilst MRI is an approved tool for assessment of sacroiliitis, the role of musculoskeletal ultrasonography remains debatable. For JIA patients, musculoskeletal ultrasonography (MSUS) offers significant benefits, in comparison with other imaging modalities, including safety, non-invasiveness, repeatability, rapid performance, relatively low cost, and high acceptability even among very young patients. In addition, MSUS can detect subclinical synovitis, improve the classification of subtypes, and capture early articular damage, as well as help clinicians monitor treatment response and guide intra-articular injections [38]. Moreover, across a majority of studies, many researchers have agreed that MSUS is superior to clinical examination in detecting synovial hypertrophy and synovial effusion [39]. In addition, ultrasonography has other useful applications, including educating young patients by showing them the appearance of both healthy and damaged joints. This exposure, as a pilot study [40] revealed, led to a 25% increase in young patients’ adherence to prescriptions for both disease-modifying antirheumatic drugs and injectable antitumour necrosis factor drugs.
This guideline addressed some of the challenges that face JIA treatment in Egypt. The guidelines endorsed the use of combination therapy for patients with moderate disease activity without poor prognostic factors. In addition, the guidelines highlighted the important role of the biologic therapies: anakinra and canakinumab in the management of systemic JIA. This is in agreement with all the previously published guidelines including the 2013 American College of Rheumatology treatment recommendations for systemic JIA [41], the British recommendations regarding therapies for the treatment of juvenile idiopathic arthritis [42], and the German consensus-based strategies in diagnosing and managing systemic JIA [43]. Unfortunately, both biologic therapy agents are not available in Egypt. Therefore, a copy of this guidelines should be forwarded to the decision-makers in the biologic therapy section in the Ministry of Health to facilitate the presence of these 2 medications. High-dose glucocorticoids are commonly used to treat systemic JIA, but they have serious adverse effects including growth failure and osteoporosis [44]. TNF inhibitors and disease-modifying antirheumatic medications (DMARDs) show poor efficacy in sJIA [45, 46]. The discovery of the critical function of the proinflammatory cytokines interleukin 1 (IL-1) and interleukin 6 (IL-6) led to the creation of specific therapy techniques [47,48,49,50] that are very effective in the near term and may lead to a considerable shift in the disease’s natural history.
We are in agreement with 2021 ACR Guideline for the Treatment of Juvenile Idiopathic Arthritis [51] in almost all lines of treatment in all categories of JIA, but we consider T2T strategy, and ACR 2021 consider temporomandibular joint in separate section and separate algorithm. And we in these recommendations added a separate section for uveitis management in JIA.
In our study, we depend on PICO manoeuvre and also consensus-based recommendations. We consider the treat-to-target strategy which differs than other previous recommendations; also, we had two steps recommendations: the first step was drug-dependent and then the second step was JIA subgroup-dependent; although these steps had more details, but it gives more clarifications.
The study’s key strengths include the participants’ variety as well as their experience, the high levels of consensus reached, and agreement with the most recently published JIA treatment recommendations. Though the treatment recommendations included in this guideline are in agreement with all the recently published guidelines [4, 5, 19, 41,42,43, 52], the study’s main limitation remains the study’s scope, which was conducted in Egypt, and the results may not be applicable to other nations.
In conclusion, Clinicians’ treatment techniques can differ, and these advice notes offer a way to establish best practice based on current evidence or expert consensus. They will also help to improve practice consistency and promote the highest levels of care. The necessity of early and successful treatment for children and adolescents with JIA in its various manifestations is highlighted in this guideline and treatment recommendations. They also endorse a strict disease control strategy based on the treat-to-target method, with the goal of inactive illness. Because children with JIA are typically asymptomatic, it is critical that they be checked for poor prognostic markers and have routine ophthalmology screenings to detect uveitis early.
Availability of data and materials
The data will be available upon reasonable request.
Change history
13 June 2022
A Correction to this paper has been published: https://doi.org/10.1186/s43166-022-00134-0
Abbreviations
- ANA:
-
Antinuclear antibodies
- CEBM:
-
Centre for Evidence-Based Medicine
- DMARDs:
-
Disease-modifying antirheumatic drugs
- EDTA:
-
Ethylenediaminetetraacetic acid
- H:
-
High level of agreement
- HRQoL:
-
Health-related quality of life
- IL:
-
Interleukin
- JADAS:
-
Juvenile arthritis disease activity score
- JIA:
-
Juvenile idiopathic arthritis
- JSpADA:
-
Juvenile spondyloarthritis disease activity
- LE:
-
Level of evidence according to the Oxford Centre for Evidence-Based Medicine (CEBM) criteria
- LMIC:
-
Low- and middle-income countries
- MAS:
-
Macrophage activation syndrome
- MSUS:
-
Musculoskeletal ultrasonography
- MTX:
-
Methotrexate
- NSAIDs:
-
Nonsteroidal anti-inflammatory drugs
- PICO:
-
Population, intervention, comparator, and outcome
- RCTs:
-
Randomized controlled trials
- sJIA:
-
Systemic juvenile idiopathic arthritis
- T2T:
-
Treat to target
- TNF:
-
Tumour necrosis factor
References
Mielants H, Veys EM, Maertens M, Goemaere S, De Clercq L, Castro S et al (1993) Prevalence of inflammatory rheumatic diseases in an adolescent urban student population, age 12 to 18, in Belgium. Clin Exp Rheumatol 11:563–567
Danner S, Sordet C, Terzic J, Donato L, Velten M, Fischbach M et al (2006) Epidemiology of juvenile idiopathic arthritis in Alsace, France. J Rheumatol 33:1377–1381
Hanova P, Pavelka K, Dostal C, Holcatova I, Pikhart H (2006) Epidemiology of rheumatoid arthritis, juvenile idiopathic arthritis and gout in two regions of the Czech Republic in a descriptive population-based survey in 2002-2003. Clin Exp Rheumatol 24:499–507
Ferrara G, Mastrangelo G, Barone P, La Torre F, Martino S, Pappagallo G, Ravelli A, Taddio A, Zulian F, Cimaz R, Rheumatology Italian Study Group (2018) Methotrexate in juvenile idiopathic arthritis: advice and recommendations from the MARAJIA expert consensus meeting. Pediatr Rheumatol Online J 16(1):46
Ravelli A, Consolaro A, Horneff G et al (2018) Treating juvenile idiopathic arthritis to target: recommendations of an international task force. Ann Rheum Dis 77:819–828
Consolaro A, Giancane G, Schiappapietra B et al (2016) Clinical outcome measures in juvenile idiopathic arthritis. Pediatr Rheumatol 14:23
Bromberg MH, Connelly M, Anthony KK, Gil KM, Schanberg LE (2014) Self-reported pain and disease symptoms persist in juvenile idiopathic arthritis despite treatment advances: an electronic diary study. Arthritis Rheum 66:462–469
Nijhof LN, Nap-van der Vlist MM, van de Putte EM, van Royen-Kerkhof A, Nijhof SL (2018) Non-pharmacological options for managing chronic musculoskeletal pain in children with pediatric rheumatic disease: a systematic review. Rheumatol Int 38:2015–2025
Lipstein EA, Brinkman WB, Sage J, Lannon CM, Morgan Dewitt E (2013) Understanding treatment decision making in juvenile idiopathic arthritis: a qualitative assessment. Pediatr Rheumatol Online J 11(1):34
Atef Y, Lotfy H, El Aroussy N, Mekkawy D, Hassan W, Nasef SI et al (2018) THU0555 guidelines for juvenile idiopathic arthritis management: is there a room for combined methotrexate and leflunomide therapy in the treatment recommendations. Ann Rheum Dis 77:480. https://doi.org/10.1136/annrheumdis-2018-eular.2788
Higgins JPT, Green S (eds) (2011) Cochrane handbook for systematic reviews of interventions version 5.1.0 [updated March 2011]. The Cochrane Collaboration Available from: https://training.cochrane.org/handbook
OCEBM Levels of Evidence Working Group (2011) The Oxford levels of evidence 2. Oxford Centre for Evidence-Based Medicine, Oxford
Niederberger M, Spranger J (2020) Delphi technique in health sciences: a map. Front Public Health 8:457. https://doi.org/10.3389/fpubh.2020.00457
Diamond IR, Grant RC, Feldman BM, Pencharz PB, Ling SC, Moore AM, Wales PW (2014) Defining consensus: a systematic review recommends methodologic criteria for reporting of Delphi studies. J Clin Epidemiol 67(4):401–409
Von der Gracht H (2012) Consensus measurement in Delphi studies: review and implications for future quality assurance. Technol Forecast Soc 79(8):1525–1536
Ringold S, Wallace CA, Rivara FP (2009) Health-related quality of life, physical function, fatigue, and disease activity in children with established polyarticular juvenile idiopathic arthritis. J Rheumatol 36:1330–1336
Ringold S, Ward TM, Wallace CA (2013) Disease activity and fatigue in juvenile idiopathic arthritis. Arthritis Care Res (Hoboken) 65:391–397
van Suijlekom-Smit L (2020) Evaluating the past might enlighten the future. Lancet 2(4):E197–E198. https://doi.org/10.1016/S2665-9913(20)30058-8
Ringold S, Angeles-Han ST, Beukelman T, Lovell D, Cuello CA, Becker ML et al (2019) 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Treatment of Juvenile Idiopathic Arthritis: therapeutic approaches for non-systemic polyarthritis, sacroiliitis, and enthesitis. Arthritis Care Res (Hoboken) 71(6):717–734
Hansen MP, Bjerrum L, Gahrn-Hansen B, Jarbol DE (2010) Quality indicators for diagnosis and treatment of respiratory tract infections in general practice: a modified Delphi study. Scand J Prim Health Care 28(1):4–11. https://doi.org/10.3109/02813431003602724
Lai L, Flower A, Moore M, Lewith G (2015) Developing clinical practice guidelines for Chinese herbal treatment of polycystic ovary syndrome: a mixed-methods modified Delphi study. Complement Ther Med 23(3):430–438. https://doi.org/10.1016/j.ctim.2015.03.003
Seid M, Opipari L, Huang B, Brunner HI, Lovell DJ (2009) Disease control and health-related quality of life in juvenile idiopathic arthritis. Arthritis Rheum 61:393–399
Nigrovic PA, Raychaudhuri S, Thompson SD (2018) Review: genetics and the classification of arthritis in adults and children. Arthritis Rheumatol 70:7–17
Eng SW, Duong TT, Rosenberg AM, Morris Q, Yeung RS, REACCH OUT and BBOP Research Consortia (2014) The biologic basis of clinical heterogeneity in juvenile idiopathic arthritis. Arthritis Rheumatol 66:3463–3475
Ombrello MJ, Remmers EF, Tachmazidou I, Grom A, Foell D, Haas JP, International Childhood Arthritis Genetics (INCHARGE) consortium et al (2015) HLA-DRB1*11 and variants of the MHC class II locus are strong risk factors for systemic juvenile idiopathic arthritis. Proc Natl Acad Sci USA 112:15970–15975
Ombrello MJ, Arthur VL, Remmers EF, Hinks A, Tachmazidou I, Grom AA et al (2017) Genetic architecture distinguishes systemic juvenile idiopathic arthritis from other forms of juvenile idiopathic arthritis: clinical and therapeutic implications. Ann Rheum Dis 76:906–913
Martini A, Ravelli A, Avcin T, Beresford MW, Burgos-Vargas R, Cuttica R, Pediatric Rheumatology International Trials Organization (PRINTO) et al (2019) Toward new classification criteria for juvenile idiopathic arthritis: first steps, Pediatric Rheumatology International Trials Organization International Consensus. J Rheumatol 46(2):190–197
Eriksen MB, Frandsen TF (2018) The impact of patient, intervention, comparison, outcome (PICO) as a search strategy tool on literature search quality: a systematic review. J Med Library Assoc 106(4):420–431
Rowe G, Wright G (1999) The Delphi technique as a forecasting tool: issues and analysis. Int J Forecast 15:353–375
Jones J, Hunter D (1995) Consensus methods for medical and health services research. BMJ 311:376–380
Rayens MK, Hahn EJ (2000) Building consensus using the policy Delphi method. Policy Polit Nurs Pract 1(4):308–315
Hinze CH, Holzinger D, Lainka E et al (2018) Practice and consensus-based strategies in diagnosing and managing systemic juvenile idiopathic arthritis in Germany. Pediatr Rheumatol 16:7–12
Smolen JS, Aletaha D, Bijlsma JW, Breedveld FC, Boumpas D, Burmester G et al (2010) Treating rheumatoid arthritis to target: recommendations of an international task force. Ann Rheum Dis 69:631–637
Schipper LG, van Hulst LT, Grol R, van Riel PL, Hulscher ME, Fransen J (2010) Meta-analysis of tight control strategies in rheumatoid arthritis: protocolized treatment has additional value with respect to the clinical outcome. Rheumatology (Oxford) 49:2154–2164
Woo P (2009) Theoretical and practical basis for early aggressive therapy in paediatric autoimmune disorders. Curr Opin Rheumatol 21:552–557
Shoop-Worrall SJW, Verstappen SMM, McDonagh JE, Baildam E, Chieng A, Davidson J et al (2018) Long-term outcomes following achievement of clinically inactive disease in juvenile idiopathic arthritis: the importance of definition. Arthritis Rheum 70:1519–1529
Bromberg MH, Schechter NL, Nurko S, Zempsky WT, Schanberg LE (2014) Persistent pain in chronically ill children without detectable disease activity. Pain Manag 4:211–219
Song H (2020) Keeping up with the progress in the diagnosis and management of pediatric rheumatic diseases. World J Pediatr 16(1):1–4
Caporali R, Smolen JS (2018) Back to the future: forget ultrasound and focus on clinical assessment in rheumatoid arthritis management. Ann Rheum Dis 77(1):18
Favier LA, Ting TV, Modi AC (2018) Feasibility of a musculoskeletal ultrasound intervention to improve adherence in juvenile idiopathic arthritis: a proof-of concept trial. Ped Rheum 16(1):75
Ringold S, Weiss PF, Beukelman T, Dewitt EM, Ilowite NT, Kimura Y, American College of Rheumatology (2013) 2013 update of the 2011 American College of Rheumatology recommendations for the treatment of juvenile idiopathic arthritis: recommendations for the medical therapy of children with systemic juvenile idiopathic arthritis and tuberculosis screening among children receiving biologic medications. Arthritis Care Res 65(10):1551–1563
Clinical Commissioning Policy Statement: biologic therapies for the treatment of juvenile idiopathic arthritis (JIA). NHS England. 2015. Accessed from: https://www.england.nhs.uk/wp-content/uploads/2018/08/Biologic-therapies-for-the-treatment-of-juvenile-idiopathic-arthritis.pdf. Accessed 13 Mar 2021.
Hinze CH, Holzinger D, Lainka E, Haas JP, Speth F, Kallinich T, PRO-KIND SJIA project collaborators et al (2018) Practice and consensus-based strategies in diagnosing and managing systemic juvenile idiopathic arthritis in Germany. Pediatr Rheumatol Online J 16(1):7
Pardeo M, Marafon DP, Insalaco A, Bracaglia C et al (2015) Anakinra in systemic juvenile idiopathic arthritis: a single-center experience. J Rheum 42(8):1523–1527
Bowyer SL, Roettcher PA, Higgins GC, Adams B, Myers LK, Wallace C et al (2003) Health status of patients with juvenile rheumatoid arthritis at 1 and 5 years after diagnosis. J Rheumatol 30:394–400
Woo P, Southwood TR, Prieur AM, Dorè CJ, Grainger J, David J et al (2000) Randomized, placebo-controlled, crossover trial of low-dose oral methotrexate in children with extended oligoarticular or systemic arthritis. Arthritis Rheum 43:1849–1857
Quartier P, Taupin P, Bourdeaut F, Lemelle I, Pillet P, Bost M et al (2003) Efficacy of etanercept for the treatment of juvenile idiopathic arthritis according to the onset type. Arthritis Rheum 48:1093–1101
Quartier P, Allantaz F, Cimaz R, Pillet P, Messiaen C, Bardin C et al (2011) A multicentre, randomised, double-blind, placebo-controlled trial with the interleukin-1 receptor antagonist anakinra in patients with systemic-onset juvenile idiopathic arthritis (ANAJIS trial). Ann Rheum Dis 70:747–754
De Benedetti F, Brunner HI, Ruperto N, Kenwright A, Wright S, Calvo I et al (2012) Randomized trial of tocilizumab in systemic juvenile idiopathic arthritis. N Engl J Med 367:2385–2395
Ruperto N, Brunner HI, Quartier P, Constantin T, Wulffraat N, Horneff G, PRINTO, PRCSG et al (2012) Two randomized trials of canakinumab in systemic juvenile idiopathic arthritis. N Engl J Med 367:2396–2406
Onel KB, Horton DB, Lovell DJ, Shenoi S, Cuello CA, Angeles-Han ST et al (2022) 2021 American College of Rheumatology Guideline for the Treatment of Juvenile Idiopathic Arthritis: therapeutic approaches for oligoarthritis, temporomandibular joint arthritis, and systemic juvenile idiopathic arthritis. Arthritis Care Res (Hoboken) 74(4):521–537
Constantin T, Foeldvari I, Anton J, de Boer J, Czitrom-Guillaume S, Edelsten C, Gepstein R et al (2018) Consensus-based recommendations for the management of uveitis associated with juvenile idiopathic arthritis: the SHARE initiative. Ann Rheum Dis 77(8):1107–1117
Acknowledgements
Not applicable.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author information
Authors and Affiliations
Contributions
Conceptualization and design, YEM and MHAZ; acquisition of data, YEM, MHAZ, and SN; formal analysis, MEG; investigation, SS and HL; methodology, all authors; writing — original draft, YEM, MHAZ, and ST; final approval of the version to be submitted, all authors.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was performed in accordance with the Helsinki Declaration. This was a multistep process which followed the “clinical, evidence-based, guidelines” (CEG) initiative protocol (ethical approval code: 34842/8/21, ethical board Tanta University) aiming at setting up an actionable clinical gold standard for treat-to-target management of rheumatic and bone diseases. As per the Egyptian national ethical committee regulations, verbal informed consent was required from all the participants included in the study. All the participants included in the study gave their verbal informed consent. All the participants were kept anonymous, in compliance with data protection regulations.
Consent for publication
Not applicable.
Competing interests
The authors declare that the corresponding author Dr. Mohammed Hassan Abu-Zaid is Associate Editor in the Egyptian Rheumatology and Rehabilitation. Co-authors Dr. Mohammed Mortada and Yasser El Miedany are among the Editorial Board of the journal.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original online version of this article was revised to update the "Competing interests" section.
Supplementary Information
Additional file 1: Supplement 1.
Population included. Supplement 2. Interventions included in the literature review. Supplement 3. The critical outcomes, as chosen by the Core Team. They varied among the different subgroups of pediatric patients with JIA (polyarthritis, oligoarthritis, systemic juvenile arthritis, sacroiilitis/enthesitis) and/or uveitis. Supplement 4. Levels of evidence [12].
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visithttp://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
El Miedany, Y., Salah, S., Lotfy, H. et al. Updated clinical practice treat-to-target guidelines for JIA management: the Egyptian College of Pediatric Rheumatology initiative. Egypt Rheumatol Rehabil 49, 27 (2022). https://doi.org/10.1186/s43166-022-00125-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43166-022-00125-1