
Abstract
Objectives
The aim of the study was to evaluate the correlation between cardiopulmonary exercise testing (CPET) parameters and right ventricular echocardiographic parameters for pulmonary arterial hypertension screening in a cohort of systemic sclerosis (SSc) patients. Methods forty SSc patients were examined using CPET and resting transthoracic echocardiography. CPET parameters analyzed were minute ventilation/carbon dioxide production (VE/VCO2) slope and maximum oxygen uptake (VO2 max); echocardiographic parameters were systolic pulmonary artery pressure (sPAP), tricuspid annular plane systolic excursion (TAPSE), and TAPSE/sPAP ratio. Results a positive correlation was observed between VE/VCO2 slope and age (r = 0.415, p < 0.01) and sPAP (r = 0.461, p < 0.01), conversely, a negative correlation was found between VE/VCO2 slope and TASPE/sPAP ratio (r = − 0.521, p = 0.001). VO2 max showed an inverse correlation with age (r = − 0.367, p < 0.05) and sPAP (r = − 0.387, p < 0.05) and a positive correlation with TAPSE/sPAP ratio (r = 0.521, p < 0.01). On stepwise linear regression analysis, VE/VCO2 slope was significantly correlated with TAPSE/sPAP ratio (β coefficient = − 0.570; p < 0.0001), as well as VO2 max was significantly correlated with TAPSE/sPAP ratio (β coefficient = 0.518; p = 0.001). Conclusion in SSc patients, TAPSE/sPAP ratio is the echocardiographic parameter of RV function which showed the best correlation with ventilatory efficiency and exercise capacity.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
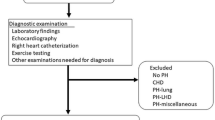
Pulmonary arterial hypertension (PAH) is characterized by progressive pulmonary vascular remodeling resulting in increased pulmonary vascular resistance and pulmonary arterial pressure, eventually leading to right ventricular (RV) failure [1]. PAH is a leading cause of morbidity and mortality in systemic sclerosis (SSc) patients [2]. Early diagnosis and treatment have been associated with improved outcomes [3, 4]. Annual screening with echocardiography, diffusing capacity of the lung for carbon monoxide (DLCO) and natriuretic peptides is recommended by current guidelines. Right heart catheterization (RHC) is required to confirm PAH diagnosis and to assess the severity of haemodynamic impairment [5]. Cardiopulmonary exercise testing (CPET) has been included in PAH diagnostic algorithm in order to reduce unnecessary invasive procedures [6, 7].
CPET is a safe non-invasive, dynamic technique providing an integrative assessment of cardiovascular, respiratory, metabolic, and muscular response to physical effort. Among CPET parameters, maximum oxygen uptake (VO2 max) and minute ventilation/carbon dioxide production (VE/VCO2) slope have been the most widely studied in cardiopulmonary diseases and have proved to be useful not only for PAH detection but also as prognostic markers [8, 9]. A low VO2 max is an index of reduced exercise capacity. A high VE/VCO2 slope reflects reduced ventilatory efficiency and is a hallmark of pulmonary vascular diseases [10].
Pressure overload is the main cause of RV dysfunction and failure in PAH. The RV–pulmonary arterial (PA) coupling describes the continuum of RV adaptation to pulmonary arterial load. The tricuspid annular plane systolic excursion/systolic pulmonary artery pressure (TAPSE/sPAP) ratio is the echocardiographic estimate of RV–PA coupling measured invasively by RHC [11]. A reduced TAPSE/sPAP ratio has been associated with poor outcomes in patients with PAH [12]. TAPSE/sPAP ratio is a powerful predictor of all-cause mortality in patients with moderate or severe tricuspid regurgitation [13]. Moreover, it has recently been demonstrated the potential role of TAPSE/sPAP ratio in SSc-PAH diagnosis [14].
An association between RV function parameters and VE/VCO2 slope and VO2 max has already been reported in heart failure and PAH [15, 16]. No study to date has specifically investigated the relationship between CPET measures and TAPSE/sPAP ratio.
The aim of the study was to evaluate the correlation between CPET parameters and RV echocardiographic parameters for PAH screening in a cohort of SSc patients.
Methods
Subjects
Forty patients meeting the 2013 American College of Rheumatology/European League against Rheumatism classification criteria for SSc [17] were enrolled in the study. Diffuse cutaneous SSc (dcSSc) and limited cutaneous SSc (lcSSc) were classified according to Le Roy et al. [18].
Patients with unstable angina, heart failure, arrhythmias, neurological disorders, valvular heart disease, uncontrolled arterial hypertension, hypertrophic cardiomyopathy, compromised exercise performance, mental or cognitive impairment, peripheral vascular diseases, anaemia, pregnant or breastfeeding women and subjects unable to give written informed consent were excluded. Calcium channel blockers, endotelin-1 receptor antagonist, and phosphodiesterase type 5 inhibitors were interrupted 72 h before CPET examination. CPET was performed 24 h prior to the next infusion of Iloprost.
The subjects’ written consent was obtained according to the declaration of Helsinki and the study was approved by the ethics committee of Sapienza University.
Echocardiography
Resting transthoracic echocardiography was performed in all SSc patients by the same experienced operator with the General Electric Vivid S5 apparatus (GE Medical Systems, Israel Ltd.). Left ventricle (LV) diameter, wall thickness, LV ejection fraction (EF), RV diameter, TAPSE, left and right atrium area were assessed by standard methods [19]. sPAP was calculated from peak tricuspidal jet velocity using the simplified Bernoulli equation and combining this value with an estimate of the right atrium (RA) pressure: sPAP = 4(V)2 + RA pressure, where V is the peak velocity (in meters per second) of the tricuspid valve regurgitant jet, and RA pressure is estimated from inferior vena cava (IVC) diameter and respiratory changes [20].
CPET
An incremental symptom-limited CPET was performed on an electronically braked cycloergometer (Ergoline-800, Mortara, Bologna, Italy), according to our previous study [21]. The subject was connected to the breath-by-breath lung gas exchange system by the use of a mask and breathing through a bidirectional turbine mass flow sensor (Quark PFT, Cosmed, Rome, Italy). The exercise protocol consisted of 3 min of rest and 3 min of unloaded cycling, followed by an incremental work rate to induce voluntary exhaustion in about 10 min, followed by 3 min of recovery. ECG and pulse oximetry were continuously monitored, and blood pressure was measured every two minutes. VO2, VCO2 and the respiratory exchange ratio (VCO2/VO2, RER) were computed and averaged every 10 s. The anaerobic threshold (AT) was determined by the V-slope method. The relation between VE and VCO2 (VE/VCO2 slope) was calculated as the slope of the linear relationship between VE and VCO2 from one minute after the beginning of the loaded exercise to the end of the isocapnic buffering period. A submaximal test is defined by RER ≤ 1.05.
Statistical analysis
All results are expressed as the median and interquartile range (IQR), SPSS version 26.0 software was used for statistical analysis. The Shapiro–Wilk test was used to evaluate the normal distribution of data. Group of comparisons were made by Mann–Whitney test. The Fisher’s exact test was used to compare categorical variables. Spearman coefficient was used to evaluate the linear correlation. Stepwise regression analysis with significant variables in linear correlation was used to evaluate the correlation between the dependent variable (VE/VCO2 slope and VO2 max) and independent variables. P-values < 0.05 were considered significant.
Results
Forty SSc patients [35 females (87.5%); median age 53 (IQR 46–59) years] were enrolled in the study. Twenty-three patients (57.5%) had lcSSc. Clinical, echocardiographic and CPET parameters of SSc patients are reported in Table 1.
VE/VCO2 slope and VO2 max median values were 29.2 (IQR 25.3–32.7) and 19.7 (IQR 17.85–24.21) mL/min/kg, respectively. sPAP and TAPSE/sPAP ratio median value were 28 (25–32) mmHg and 0.87 (IQR 0.75–1.05) mm/mmHg, respectively.
A significant positive correlation was found between VE/VCO2 slope and age (r = 0.415, p < 0.01) and sPAP (r = 0.461, p < 0.01), conversely, a significant negative correlation was observed between VE/VCO2 slope and TAPSE/sPAP ratio (r = − 0.521, p = 0.001) (Fig. 1). No correlation was found between VE/VCO2 slope and TAPSE. By stepwise linear regression analysis, VE/VCO2 slope was significantly correlated with TAPSE/sPAP ratio (β coefficient = − 0.570; p < 0.0001).

A Correlation between minute ventilation/carbon dioxide production (VE/VCO2) slope and tricuspid annular plane systolic excursion/systolic pulmonary artery pressure (TAPSE/sPAP) ratio; B Correlation between maximum oxygen uptake (VO2 max) and TAPSE/sPAP ratio
VO2 max showed a significant negative correlation with age (r = − 0.367, p < 0.05) and sPAP (r = − 0.387, p < 0.05) and a significant positive correlation with TAPSE/sPAP ratio (r = 0.521, p < 0.01) (Fig. 1). No correlation was found between VO2 max and TAPSE. On stepwise regression analysis VO2 max was significantly correlated with TAPSE/sPAP ratio (β coefficient = 0.518; p = 0.001).
Discussion
In this study, VE/VCO2 slope and VO2 max showed a correlation with age, sPAP and TAPSE/sPAP ratio. Therefore, in multiple regression analysis TAPSE/sPAP ratio is the only variable, which shows a significant correlation with exercise capacity (VO2 max) and ventilatory efficiency (VE/VCO2 slope).
Reducing the time to PAH diagnosis can significantly improve patients’ survival. Current guidelines recommend resting echocardiography as a screening test in SSc patients. Although elevated sPAP values are associated with an increased probability of PAH, sPAP estimation may be inaccurate in the individual patient. In the ESC/ERS guidelines, CPET was performed to reduce unnecessary invasive procedures and in PAH risk assessment [5].
In our study, we demonstrated that TAPSE/sPAP ratio is the best echocardiographic parameter of RV function which correlates with VE/VCO2 slope and VO2 max. In clinical practice, sPAP is the most used echocardiograpic parameter to evaluate PAH. In our previous study, we demonstrated that in SSc patients with a DETECT algorithm step 2 total score > 35 TAPSE/sPAP ratio can be used to further select patients requiring RHC to confirm PAH diagnosis [14]. Dumitrescu et al. investigated the role of CPET in early PAH detection in a prospective study of 173 SSc patients, without known PAH, who also underwent RHC. PeakVO2 and VE/VCO2 were the CPET parameters, which showed the highest correlations with pulmonary haemodynamics. PeakVO2 was the most accurate parameter for diagnosis (sensitivity 87.5%, specificity 74.8% at a threshold level of 13.8 mL/min/kg) and a peakVO2 of > 18.7 mL/kg/min excluded PAH (negative predictive value of 1.0). In addition, a nadir VE/VCO2 ratio of > 45.5 showed a positive predictive value of 1.0 [6]. Santaniello et al. demonstrated that CPET is useful, in addition to the DETECT algorithm, to select patients for RHC referral. Among CPET parameters VE/VCO2 slope showed the best performance to predict PAH at RHC [7]. An association between RV function parameters and VE/VCO2 slope and VO2 max has already been reported. In heart failure, higher sPAP and lower RV fractional area change (FAC) were correlated with worse percent predicted VO2 max and higher VE/VCO2 slope [15]. In PAH, resting RV function assessed by FAC or RV longitudinal strain was also associated with the CPET parameters of exercise capacity and ventilatory efficiency [16]. To date, no study has investigated the correlation between TAPSE/sPAP ratio and CPET parameters. We can assume that TAPSE/sPAP ratio could be a useful echocardiographic parameter of RV function to select SSc patients requiring CPET. The main limitations of our study are the small sample size, the lack of a control group, the lack of RHC data and the prospective role of TAPSE/sPAP ratio during the follow-up of SSc patients.
In conclusion, in SSc patients TAPSE/sPAP ratio is the echocardiographic parameter of RV function which showed the best correlation with ventilatory efficiency and exercise capacity. Future larger studies are needed to confirm our preliminary data.
References
Humbert M, Guignabert C, Bonnet S, et al. Pathology and pathobiology of pulmonary hypertension: state of the art and research perspectives. Eur Respir J. 2019;53(1):1801887. https://doi.org/10.1183/13993003.01887-2018.
Elhai M, Meune C, Boubaya M, et al. Mapping and predicting mortality from systemic sclerosis. Ann Rheum Dis. 2017;76(11):1897–905. https://doi.org/10.1136/annrheumdis-2017-211448.
Hughes M, Zanatta E, Sandler RD, Avouac J, Allanore Y. Improvement with time of vascular outcomes in systemic sclerosis: a systematic review and meta-analysis study. Rheumatology (Oxford). 2021. https://doi.org/10.1093/rheumatology/keab850.
Brown Z, Proudman S, Morrisroe K, Stevens W, Hansen D, Nikpour M. Screening for the early detection of pulmonary arterial hypertension in patients with systemic sclerosis: a systematic review and meta-analysis of long-term outcomes. Semin Arthritis Rheum. 2021;51(3):495–512. https://doi.org/10.1016/j.semarthrit.2021.03.011.
Galiè N, Humbert M, Vachiery JL, et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: the joint task force for the diagnosis and treatment of pulmonary hypertension of the European society of cardiology (ESC) and the European respiratory society (ERS): endorsed by: association for European paediatric and congenital cardiology (AEPC), international society for heart and lung transplantation (ISHLT). Eur Heart J. 2016;37(1):67–119. https://doi.org/10.1093/eurheartj/ehv317.
Dumitrescu D, Nagel C, Kovacs G, et al. Cardiopulmonary exercise testing for detecting pulmonary arterial hypertension in systemic sclerosis. Heart. 2017;103(10):774–82. https://doi.org/10.1136/heartjnl-2016-309981.
Santaniello A, Casella R, Vicenzi M, et al. Cardiopulmonary exercise testing in a combined screening approach to individuate pulmonary arterial hypertension in systemic sclerosis. Rheumatology (Oxford). 2020;59(7):1581–6. https://doi.org/10.1093/rheumatology/kez473.
Wensel R, Francis DP, Meyer FJ, et al. Incremental prognostic value of cardiopulmonary exercise testing and resting haemodynamics in pulmonary arterial hypertension. Int J Cardiol. 2013;167(4):1193–8. https://doi.org/10.1016/j.ijcard.2012.03.135.
Ewert R, Ittermann T, Habedank D, et al. Prognostic value of cardiopulmonary exercise testing in patients with systemic sclerosis. BMC Pulm Med. 2019;19(1):230. https://doi.org/10.1186/s12890-019-1003-7.
Weatherald J, Philipenko B, Montani D, Laveneziana P. Ventilatory efficiency in pulmonary vascular diseases. Eur Respir Rev. 2021;30(161): 200214. https://doi.org/10.1183/16000617.0214-2020.
Tello K, Wan J, Dalmer A, et al. Validation of the tricuspid annular plane systolic excursion/systolic pulmonary artery pressure ratio for the assessment of right ventricular–arterial coupling in severe pulmonary hypertension. Circ Cardiovasc Imaging. 2019;12(9): e009047. https://doi.org/10.1161/CIRCIMAGING.119.009047.
Tello K, Axmann J, Ghofrani HA, et al. Relevance of the TAPSE/PASP ratio in pulmonary arterial hypertension. Int J Cardiol. 2018;266:229–35. https://doi.org/10.1016/j.ijcard.2018.01.053.
Saeed S, Smith J, Grigoryan K, et al. The tricuspid annular plane systolic excursion to systolic pulmonary artery pressure index: association with all-cause mortality in patients with moderate or severe tricuspid regurgitation. Int J Cardiol. 2020;317:176–80. https://doi.org/10.1016/j.ijcard.2020.05.093.
Colalillo A, Grimaldi MC, Vaiarello V, et al. In systemic sclerosis TAPSE/sPAP ratio can be used in addition to the DETECT algorithm for pulmonary arterial hypertension diagnosis. Rheumatology (Oxford). 2021. https://doi.org/10.1093/rheumatology/keab748.
Teramoto K, Sengelov M, West E, et al. Association of pulmonary hypertension and right ventricular function with exercise capacity in heart failure. ESC Heart Fail. 2020;7(4):1635–44. https://doi.org/10.1002/ehf2.12717.
Rehman MB, Howard LS, Christiaens LP, Gill D, Gibbs JSR, Nihoyannopoulos P. Resting right ventricular function is associated with exercise performance in PAH, but not in CTEPH. Eur Heart J Cardiovasc Imaging. 2018;19(2):185–92. https://doi.org/10.1093/ehjci/jex002.
van den Hoogen F, Khanna D, Fransen J, et al. 2013 classification criteria for systemic sclerosis: an American college of rheumatology/European league against rheumatism collaborative initiative. Ann Rheum Dis. 2013;72(11):1747–55. https://doi.org/10.1136/annrheumdis-2013-204424.
Lang RM, Bierig M, Devereux RB, et al. Recommendations for chamber quantification: a report from the American society of echocardiography’s guidelines and standards committee and the chamber quantification writing group, developed in conjunction with the European association of echocardiography, a branch of the European society of cardiology. J Am Soc Echocardiogr. 2005;18(12):1440–63. https://doi.org/10.1016/j.echo.2005.10.005.
LeRoy EC, Black C, Fleischmajer R, et al. Scleroderma (systemic sclerosis): classification, subsets and pathogenesis. J Rheumatol. 1988;15(2):202–5.
Rudski LG, Lai WW, Afilalo J, et al. Guidelines for the echocardiographic assessment of the right heart in adults: a report from the American society of echocardiography endorsed by the European association of echocardiography, a registered branch of the European society of cardiology, and the Canadian society of echocardiography. J Am Soc Echocardiogr. 2010;23(7):685–788. https://doi.org/10.1016/j.echo.2010.05.010.
Rosato E, Leodori G, Gigante A, Di Paolo M, Paone G, Palange P. Reduced ventilatory efficiency during exercise predicts major vascular complications and mortality for interstitial lung disease in systemic sclerosis. Clin Exp Rheumatol. 2020;38(Suppl 125):85–91.
Funding
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no relevant financial or non-financial interests to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Colalillo, A., Pellicano, C., Romaniello, A. et al. In systemic sclerosis TAPSE/sPAP ratio is correlated with ventilatory efficiency and exercise capacity assessed by CPET. Clin Exp Med 23, 365–369 (2023). https://doi.org/10.1007/s10238-022-00804-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10238-022-00804-5