
Abstract
Objective
To investigate the impact of vitamin A (VA), vitamin D (VD), and homocysteine (Hcy) on cardiometabolic multimorbidity (CMM).
Methods
This study is a cross-sectional study conducted in Ningxia Province, China. A total of 5000 participants aged 25–74 were recruited and divided into two groups based on the definition of cardiometabolic multimorbidity: the CMM group and the Non CMM group. Demographic, lifestyle, and laboratory data were collected to investigate the correlation between vitamin A, D, Hcy levels and CMM risk. The association was analyzed using multiple logistic regression and restricted cubic spline method.
Results
CMM incidence increased with age, being higher in females (20.05%) compared to males, Hypertension was present in 96.20% of CMM cases. Reduced VD levels correlated with an elevated CMM risk (OR = 1.799, 95% CI: 1.466–2.238), showing an inverse dose-response relationship, even after adjusting for confounders (OR = 1.553, 95% CI: 1.233–1.956). However, VA and Hcy levels were not significantly associated with CMM risk. The inverse correlation between VD status and CMM risk was more pronounced in males, obese individuals, and those with normal blood lipid profiles (P < 0.05).
Conclusions
The risk of CMM increases with age, especially in women. Inadequate VD status increases vulnerability to CMM, suggesting that optimising VD reduces the risk of CMM.
Similar content being viewed by others

Introduction
It is commonly known that with the aging of the global population and advances in medical technology, more and more diseases are being controlled at a certain level meanwhile the survival time of patients with diseases is prolonged [1]. Accordingly, the increasing number of people suffering from two or more diseases poses a great challenge to the medical and health system [2]. Cardiometabolic Multimorbidity (CMM) is one of the most common and stable common disease gathering models of the metabolic comorbidity defined as the coexistence of two or three cardiometabolic diseases, including diabetes, hypertension, heart disease and stroke [3]. There is no denying that CMM tends to occur in older age groups, which not only increases the risk of depression and disability of the elderly [4,5,6,7], but also increases the risk of death of the elderly by 4 to 8 times [8], resulting in heavy family and social burden. Therefore, it is urgent to find the shared biomarkers of CMM.
Regarding the development of cardiovascular diseases, there have been many studies proving that dyslipidemia, obesity and hypertension have an unshirkable responsibility [9, 10], especially hypercholesterolemia triggering the inflammatory response of macrophages, which is believed to be the basis of atherosclerotic plaque formation [11].
Vitamin D (VD) is one of the main factors affecting bone and calcium metabolism. Its deficiency also increases the risk of diabetes (T2DM), metabolic syndrome (MS), and cardiovascular disease (CVD) [12, 13]. Study [14] showed that vitamin D supplementation can reduce serum total cholesterol (TC), low density lipoprotein (LDL-C) and triglyceride (TG) levels. One meta-analysis showed a 16% reduction in the risk of hypertension as vitamin D levels increased [15]. Mirhosseini [16] also emphasized that supplementing vitamin D can cause a small decrease in systolic and diastolic blood pressure. In summary, much work so far has focused on there is a relationship between vitamin D levels with the development of CMM. Vitamin A (VA) is also a lipid soluble vitamin and an essential nutrient. Its main physiological functions include maintaining vision, promoting embryonic development, influencing cell proliferation and differentiation, maintaining the integrity of epithelial cells, and regulating the immune function of the body [17]. Studies have shown that increased intake of VA can reduce the incidence of cardiovascular disease [18]. Homocysteine (Hcy) is a sulphur-containing amino acid that is an intermediate product of methionine metabolism and plays an important role in the cysteine synthesis pathway. Recent studies have shown that Hcy is associated with a variety of diseases, including diabetes mellitus, neurodegenerative diseases, osteoporosis, and cancer [19, 20]. However, the relationship between Hcy and cardiovascular disease is now considered to be much closer, with many guidelines and literature suggesting that hyperhomocysteinemia (HHcy) is an independent risk factor for cardiovascular disease, and that its mechanisms include inflammatory response and oxidative stress, damage to vascular endothelial cells, prothrombotic, pro-smooth muscle cell proliferation, methylation, and influence on lipid metabolism in vivo [21].
In previous studies, scholars have mostly focused on the risk factors of a single disease, ignoring the current development of a multimorbid disease spectrum or focusing on the impact of different lifestyles and common lipid markers on CMM, and thus comprehensive analyses of the influencing factors are still lacking. Based on the research foundation of vitamin A, D and Hcy in cardiovascular diseases, the present study aims to investigate the relationship between homocysteine and vitamin A, vitamin D and CMM by analyzing the multifaceted influencing factors of CMM, to identify the shared biomarkers of CMM, and to provide a scientific basis for the preventive and therapeutic strategies of CMM in Chinese elderly. In addition, although none of the studies on the factors affecting CMM distinguished between the number of disease types of co-morbidity, two diseases are the initial stage of co-morbidity. The influencing factors of CMM (number of disease types ≥ 2) are of great significance for targeted prevention of CMM.
Methods
Study design and population
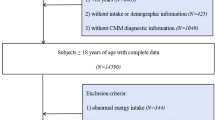
This is a prospective study based on a natural population cohort research project conducted by the National Key Research and Development Programme in rural areas of Ningxia, Northwest China. A baseline survey of people aged 25 and above were recruited as the research participants in rural areas of Qingtongxia and Pingluo counties from March 2018 to July 2020 using randomized whole-cluster sampling. Including those who have no official household registration and have lived in the community for a long time (more than 3 years), and meet the following requirements: (1) Not pregnant; (2) Not lactating; (3) Without mental illness; (4) Without diseases that have a significant impact on the current health status such as car accidents, falls; excluding residents who live temporarily (less than 3 years) and who study or work in other places for a long time but do not live at home. A total of 15,802 individuals completed the questionnaire interview, physical examination, and biological specimen collection in the baseline cross-sectional survey, from which 30% were randomly selected to form a study population of 5,300. A total of 5000 participants were included in the final analyses after excluding 117 with missing data (smoking, alcohol consumption, body mass, blood pressure, and missing lipids) and 183 with abnormal Hcy data. A flow chart of the included studies is presented in Supplementary Figure S1.
Related data collection
Well-trained investigators conducted in-person interviews to obtain data on socioeconomic characteristics, including demographic variables (age, gender, education), lifestyle behaviors (smoking, alcohol consumption, physical activity), medical history, and medication history. Smoking was defined as consumption of at least one cigarette per day for a minimum of six months. Alcohol use status was defined as drinking alcohol at least once daily for a minimum of six months. Physical exercise was operationalized as participation in physical exercise at minimum three times weekly, with each session lasting 30 min or longer. Anthropometric measurements included height, weight, waist circumference (WC), hip circumference (HC), body mass index (BMI) and blood pressure. Height was measured using a ruler. Weight, WC, and HC were measured using a bioelectrical impedance analyzer (Inbody-370s, Seoul, South Korea). BMI was calculated using the standard formula: BMI = Weight (kg)/Height (m)^2. Participants were instructed to remove outer garments, footwear, socks, and metal accessories. They were then instructed to stand motionless with their weight balanced evenly, keep their hands on the analyzer, and remain quiet until completion of the measurements. Systolic blood pressure (SBP) and diastolic blood pressure (DBP) were assessed using an automated sphygmomanometer (OMRON-7124).
Biochemical measurement
In the morning, the physician collected 5 ml of peripheral venous blood from the participants who had fasted 8 h. The blood was collected into a non-anticoagulated tube and 2 ml into an EDTA-anticoagulated tube. Fasting plasma glucose (FPG), total cholesterol, triglycerides, high-density lipoprotein cholesterol, and low-density lipoprotein cholesterol were measured using automated biochemistry analyzers available at local health clinics. Plasma homocysteine was measured using an automated biochemical analyzer [22]. Vitamin A and vitamin D were determined using an Ultra High Performance Liquid Chromatograph (Agilent 1290, Agilent Technologies, USA).
Definition of diseases
Hypertension was defined as a systolic blood pressure measurement of ≥ 140 mmHg or a diastolic blood pressure measurement of ≥ 90 mmHg [23], as documented by a physician’s self-diagnosis of the disease and secondary hospitalization. Diabetes mellitus was defined as a fasting blood glucose level ≥ 7.0 mmol/L [24], as documented by a physician’s self-diagnosis of the disease and secondary hospitalization. Coronary heart disease could be defined as a self-reported disease diagnosed by a physician and secondary inpatient record. Stroke was defined as self-reported disease diagnosed by a physician and secondary hospitalization records [25]. Multimorbidity (MM) has two or more chronic diseases at the same time Cardiometabolic multimorbidity (CMM) is defined as the same individual two or more (including hypertension, diabetes, coronary heart disease and stroke) [26]. BMI: Based on the Working Group on Obesity in China’s criteria, the BMI classifications are as follows: underweight, BMI < 18.5 kg/m2; normal weight, 18.5 ≤ BMI < 24 kg/m2; overweight, 24 ≤ BMI < 28 kg/m2; and obesity, BMI ≥ 28 kg/m2 [27]. Physical exercise: Physical activity, which was rated as low, moderate, or high, was assessed using the International Physical Activity Questionnaire [28]. Education level: Based on different levels of educational attainment, education is categorized into two types: primary school or below, and middle school or above.
Statistical analysis
Statistical analyses were implemented in R software (version 4.2.3) and SPSS (version 23.0). P-values under 0.05 were regarded as statistically significant. Continuous variables were presented as mean ± standard deviation (SD), while categorical variables were shown as frequency and percentage (n (%)). Chi-square tests and one-way analysis of variance (ANOVA) were utilized for comparisons of categorical and continuous variables, respectively. Participants were categorized into two groups based on the number of CMM: ≥2 and none. Quartile classifications of VA, VD, and Hcy levels were generated, and logistic regression models were employed to evaluate the associations between VA, VD, Hcy, and CMM using odds ratios (ORs) and 95% confidence intervals (CIs). Model 1 was unadjusted; Model 2 was adjusted for gender and age based on Model 1; Model 3 was further adjusted for smoking, drinking, and BMI based on Model 2; Model 4 additionally adjusted for energy based on Model 3. Restricted cubic spline (RCS) models were utilized to examine potential non-linear relationships of VA, VD, and Hcy with CMM. To assess the robustness of the VA, VD, Hcy and CMM associations, subgroup analyses were performed.
Result
Characteristics of the subjects
A total of 5,000 participants were enrolled in this study for analysis. Among them, 2,057 (41.14%) were males and 2,943 (58.86%) were females. The mean age of the participants was 58.00 ± 10.00 years. Compared to the No-CMM group, participants in the CMM group were older (with a mean age of 62.33 ± 8.43 years), and had smoking and alcohol drinking rates of 12.80% and 19.10%, respectively. The CMM group exhibited elevated mean levels of FPG, SBP, DBP, TG, TC, LDL-C, Hcy, and vitamin A (8.60 ± 4.06, 148.48 ± 18.40, 89.60 ± 12.64, 2.19 ± 1.54, 5.04 ± 1.22, 3.00 ± 0.98, 20.28 ± 12.38, 446.23 ± 178.97, respectively) compared to the No-CMM group. With the exception of Hcy and vitamin A, these differences were statistically significant (P < 0.05). Furthermore, the mean levels of vitamin D and HDL-C (13.27 ± 8.62 and 1.28 ± 0.34, respectively) were lower in the CMM group compared to the No-CMM group, and these differences were also statistically significant (P < 0.05). Other indicators are presented in Table 1. Table 2 presents the serum levels of Hcy, vitamin A and vitamin D across different groups. In comparison to the No-CMM group, no statistically significant differences in Hcy levels were observed between the CMM group (P > 0.05). The vitamin A levels showed a significant difference between the hypertension and non-hypertension groups (P < 0.05), however no overt discrepancies were evidenced among the other groups. With the exception of the stroke and coronary heart disease groups, vitamin D levels demonstrated statistically significant differences in the CMM group relative to the No-CMM group (P < 0.05), with diminished vitamin D levels exhibited universally across the CMM group.
Multimorbidity pattern analysis
Among the 5,000 participants enrolled in this study, 973 (19.46%) met the diagnostic criteria for cardiometabolic syndrome, which includes metabolic disorders such as hypertension, diabetes mellitus, stroke and coronary artery disease. Of those with cardiometabolic syndrome, the majority (n = 642, 65.96%) had concurrent diabetes mellitus and hypertension, followed by those (n = 130, 13.36%) with both hypertension and coronary artery disease. Additionally, among the total study cohort, 19.46% had two or more component conditions of cardiometabolic syndrome, while 2.66% had three or more components (Fig. 1). Furthermore, the prevalence of cardiometabolic syndrome was slightly higher in females compared to males (20.05% vs. 18.62%). The prevalence also demonstrated an age-dependent increase, with the fastest growth occurring in the 45–59 years age group (Figure S2).

Distribution patterns of CMM in the study population. CHD: coronary heart disease
Associations between vitamin D, vitamin A and hcy and CMM
Table 3 illustrates the correlations between vitamin A, vitamin D, Hcy and various indicators. Vitamin D displayed weak negative correlations with the indicators (P < 0.05) except for TG and LDL-C. Weak positive correlations of vitamin A with the indicators were observed (P < 0.05), excluding SBP. No correlations were evident between Hcy and the indicators (P > 0.05). Logistic regression analysis was conducted to examine the association between serum levels of vitamin D, vitamin A, and Hcy concentrations and the risk of CMM (Fig. 2). In the unadjusted models, compared with the highest quartile, the lower three quartiles of vitamin D were significantly and positively associated with increased CMM risk (third quartile: OR = 1.427, 95% CI 1.151–1.768; second quartile: OR = 1.781, 95% CI 1.440–2.204; first quartile: OR = 1.799, 95% CI 1.446–2.238, P < 0.001). After adjusting for confounding factors, decreased serum vitamin D levels remained negatively correlated with increased CMM risk (third quartile: OR = 1.251, 95% CI 1.003–1.561; second quartile: OR = 1.527, 95% CI 1.223–1.907; first quartile: OR = 1.553, 95% CI 1.233–1.956, P < 0.001), while vitamin A and Hcy were not statistically significantly associated with CMM risk (P > 0.05). Moreover, to validate the reliability of the linear association between vitamin D and CMM, we implemented RCS analysis and observed an inverse dose-response relationship between vitamin D concentrations and CMM (Fig. 3), indicating that escalating levels of vitamin D were associated with a declining risk of developing CMM (P-overall < 0.0001; P-non-linear = 0.003).

Associations (ORs and 95% CIs) between tertiles of vitamin D, vitamin A and Hcy and CMM among population. Model 1 was unadjusted; Model 2 was adjusted for age and sex; Model 3: Model 2 + smoking, alcohol consumption, BMI; Model 4: Model 3 + Energy

The relationship between vitamin D concentration and CMM risk. Horizontal black dashed lines represent the positions where OR = 1. OR: Odds ratio; CI: Confidence interval; RCS: Restricted cubic spline
Stratified analyses
To evaluate the robustness of the association between vitamin D and CMM, subsequent subgroup analyses stratified by sex, age, TC, TG, HDL-C, LDL-C, FPG, and BMI were conducted. Figure 4 presents the odds ratios for developing CMM in stratified analyses. In the stratified analyses, the first three quartile groups with lower vitamin D levels, compared to the fourth quartile group, showed positive associations with CMM to a certain extent among the subgroups of females, TG, TC < 6.2 mmol/L, HDL-C ≥ 1 mmol/L, LDL-C < 4.1 mmol/L, and BMI ≥ 24 kg/m2. These associations attained statistical significance (P < 0.05).

Association between Vitamin D and CMM in subset analysis. Hcy: Homocysteine; BMI: Body mass index; FPG: Fasting plasma glucose; TC: Total cholesterol; TG: Triglycerides; HDL-C: High-density lipoprotein cholesterol; LDL-C: Low-density lipoprotein cholesterol
Discussion
The current study analyzed cohort data from a natural population in northwest China to examine the associations between vitamin D, vitamin A, Hcy, and CMM in the northwest Chinese population. The findings revealed that the prevalence of CMM was higher in females and increased with advancing age. Furthermore, an inverse association and dose-response relationship were observed between CMM occurrence and vitamin D levels, whereas no significant relationships were found between CMM and either vitamin A or Hcy.
The present study found hypertension to be the most prevalent disease within the CMM disease pattern, clustering more frequently with other comorbidities, aligning with findings from other studies [29]. However, some studies have also identified diabetes as the most common condition in CMM, potentially attributable to genetic predispositions in the population [30]. CMM prevalence increased with age, and was higher among females. Studies across various regions of China have also shown rising CMM prevalence over time, with increasing prevalence of cardiometabolic diseases at older ages [31]. These trends signify the emergence of cardiometabolic diseases as a novel public health concern in China. Such changes may be related to shifts in dietary patterns and lifestyle transitions [32, 33]. Furthermore, research from other countries has also documented high cardiometabolic disease prevalence, including the U.K. (16.84%) [34], the U.S. (14.4%) [35], and South Africa (10.5%) [29]. The cross-national variation in prevalence may stem from differences in disease definitions and dietary habits across populations.
Vitamin D deficiency has been closely associated with obesity, diabetes and cardiovascular diseases [36]. Accumulating evidence demonstrates that vitamin D levels are closely related to cardiac metabolic diseases, and vitamin D deficiency may be an important etiological factor underlying the epidemic of these diseases [37]. Our study also revealed an inverse correlation between blood vitamin D concentrations and risk of CMM, with lower vitamin D levels associated with higher disease risk. The prevalence of hypertension is high among patients with cardiac metabolic diseases. Vitamin D has been implicated in maintaining blood pressure homeostasis through regulating the renin-angiotensin-aldosterone system [38]. Furthermore, vitamin D deficiency can impact carbohydrate metabolism, particularly glucose metabolism [14]. Therefore, vitamin D deficiency may be a key contributor to hypertension and diabetes development, subsequently leading to CMM. Substantial evidence indicates gut microbiota are involved in the pathogenesis of various chronic inflammatory conditions including diabetes and cardiovascular diseases. Vitamin D can maintain gut barrier integrity by modulating associated proteins, thereby preventing bacterial products and metabolites from entering circulation [39]. Consequently, vitamin D deficiency may disrupt the intestinal barrier and cause dysbiosis, eventually inducing diseases such as CMM.
Previous studies have demonstrated that vitamin A and its derivatives play a crucial role in modulating cardiovascular metabolism, including energy utilization, glucose homeostasis, hepatic steatosis, and atherosclerosis. They are also implicated in the pathogenesis of various adverse cardiovascular metabolic diseases like cardiovascular disease and diabetes [40]. However, the current study did not find any definite association between vitamin A and CMM. Furthermore, several large-scale prospective studies also did not reveal any significant correlation between vitamin A and CVD as well as diabetes. Some studies even reported conclusions contradictory to other reports [41]. The discrepancies among different studies could be attributed to subgroup analyses of the study population. Additionally, liver and kidney function, which play a pivotal role in vitamin A-related cardiovascular metabolism risks, may also influence the relationship between vitamin A and cardiovascular metabolic endpoints [42]. Finally, the heterogeneity between vitamin A and cardiovascular metabolism may arise from variations in outcome definitions, ethnicity, vitamin A dosage range, and study duration across different studies. Homocysteine is an important biomarker for various metabolic diseases and organ damage, but its role in cardiovascular metabolic risk remains unclear. The present study did not find any association between homocysteine and cardiovascular metabolic abnormalities. However, some studies suggest that homocysteine may mildly influence the development of cardiovascular metabolic abnormalities through oxidative stress and endothelial dysfunction [43]. Furthermore, differences in living pressure, dietary habits, and susceptibility genes for specific diseases among various populations could also lead to discrepancies between study findings. The exact mechanisms by which homocysteine affects cardiovascular metabolic abnormalities warrant further investigation through additional studies with diverse designs.
In addition, this study found that the influence of vitamin D on CMM was more pronounced in certain subgroups. For instance, CMM occurs more frequently in males, potentially due to males engaging in more behaviors associated with CMM risk, including smoking, alcohol consumption, and physical inactivity, compared to females [33]. The association between vitamin D and CMM was stronger in populations with normal blood lipid levels than in those with dyslipidemia. This may be because dyslipidemia can affect vitamin D absorption and utilization, thus obscuring the relationship between vitamin D and CMM. Moreover, higher BMI is also closely associated with increased CMM risk. The high-paced lifestyle and lack of physical activity are key factors contributing to elevated BMI, which in turn may raise metabolic disease risk through various pathways (e.g. inflammatory response) [26].Therefore, besides examining the influence of vitamin D on CMM, consideration of other contributing factors is warranted. For CMM prevention and control, priority should be given to improving unhealthy behaviors like smoking cessation, moderating alcohol intake, increasing physical activity, and controlling life stress. Blood lipid levels need monitoring and BMI should be maintained within the normal range. Only by comprehensively mitigating the various CMM risk factors can effective prevention and control of CMM be achieved.
This study possesses both strengths and limitations. Regarding strengths, our investigation utilized large-scale, population-based survey data with a substantial sample size and broad age distribution, imparting high generalizability to the results. We verified the vitamin D-CMM relationship from multiple vantage points, bolstering the robustness of our findings. Stratification by demographic traits facilitated the identification of high-risk CMM subpopulations. However, certain limitations exist. The cross-sectional design precludes causal inferences between vitamin D and CMM. Self-reported metabolic disease data may have underestimated true morbidity. Additionally, residual confounding likely persists. In summary, our study furnished further evidence supporting the vitamin D-CMM association but was unable to establish causality. The extensive, representative sample constitutes a major strength, although self-reported data may have introduced misclassification bias. Future efforts could implement objective assessment tools to minimize potential biases.
Conclusions
In conclusion, the present study demonstrates a significant age-related increase in the incidence of CMM, especially among males who exhibit higher CMM morbidity. The data verify a linear association between vitamin D status and CMM risk, whereby lower serum vitamin D levels correlate with greater CMM risk. Our findings provide preliminary evidence that vitamin D may independently modulate CMM risk. Furthermore, cardiovascular metabolic diseases pose a pressing public health concern. Consequently, prioritizing medical resources for cardiovascular metabolic disease screening, prevention and management is warranted, alongside heightened vigilance for CMM occurrence, particularly in populations with vitamin D insufficiency.
Data availability
No datasets were generated or analysed during the current study.
Abbreviations
- BMI:
-
Body mass index
- CHD:
-
Coronary heart disease
- CI:
-
Confidence interval
- CMM:
-
Cardiometabolic Multimorbidity
- CNC-NX:
-
Northwestern Chinese Natural Population Cohort-Ningxia Project
- CVD:
-
Cardiovascular disease
- FPG:
-
Fasting blood glucose
- Hcy:
-
Homocysteine
- HDL-C:
-
High density lipoprotein cholesterol
- HHcy:
-
Hyperhomocysteinemia
- LDL-C:
-
Low density lipoprotein cholesterol
- OR:
-
Odd ratio
- TC:
-
Total cholesterol
- TG:
-
Triglyceride
- SBP:
-
Systolic blood pressure
- DBP:
-
Diastolic blood pressure
- WC:
-
Waist circumference
- RCS:
-
Restricted cubic spline
References
Fabbri E, Zoli M, Gonzalez-Freire M, Salive ME, Studenski SA, Ferrucci L. Aging and multimorbidity: New tasks, priorities, and Frontiers for Integrated Gerontological and Clinical Research. J Am Med Dir Assoc. 2015;16(8):640–7. https://doi.org/10.1016/j.jamda.2015.03.013.
Zhao Y, Atun R, Oldenburg B, McPake B, Tang S, Mercer SW, et al. Physical multimorbidity, health service use, and catastrophic health expenditure by socioeconomic groups in China: an analysis of population-based panel data. Lancet Glob Health. 2020;8(6):e840. https://doi.org/10.1016/s2214-109x(20)30127-3.
Busija L, Lim K, Szoeke C, Sanders KM, McCabe MP. Do replicable profiles of multimorbidity exist? Systematic review and synthesis. Eur J Epidemiol. 2019;34(11):1025–53. https://doi.org/10.1007/s10654-019-00568-5.
Booth GL, Kapral MK, Fung K, Tu JV. Relation between age and cardiovascular disease in men and women with diabetes compared with non-diabetic people: a population-based retrospective cohort study. Lancet. 2006;368(9529):29–36. https://doi.org/10.1016/s0140-6736(06)68967-8.
Rao Kondapally Seshasai S, Kaptoge S, Thompson A, Di Angelantonio E, Gao P, Sarwar N, et al. Diabetes mellitus, fasting glucose, and risk of cause-specific death. N Engl J Med. 2011;364(9):829–41. https://doi.org/10.1056/NEJMoa1008862.
Shah AD, Langenberg C, Rapsomaniki E, Denaxas S, Pujades-Rodriguez M, Gale CP, et al. Type 2 diabetes and incidence of cardiovascular diseases: a cohort study in 1·9 million people. Lancet Diabetes Endocrinol. 2015;3(2):105–13. https://doi.org/10.1016/s2213-8587(14)70219-0.
Huang ZT, Luo Y, Han L, Wang K, Yao SS, Su HX, et al. Patterns of cardiometabolic multimorbidity and the risk of depressive symptoms in a longitudinal cohort of middle-aged and older Chinese. J Affect Disord. 2022;301:1–7. https://doi.org/10.1016/j.jad.2022.01.030.
Di Angelantonio E, Kaptoge S, Wormser D, Willeit P, Butterworth AS, Bansal N, et al. Association of Cardiometabolic Multimorbidity with Mortality. JAMA. 2015;314(1):52–60. https://doi.org/10.1001/jama.2015.7008.
Sattar N, Lee MMY, Kristensen SL, Branch KRH, Del Prato S, Khurmi NS, et al. Cardiovascular, mortality, and kidney outcomes with GLP-1 receptor agonists in patients with type 2 diabetes: a systematic review and meta-analysis of randomised trials. Lancet Diabetes Endocrinol. 2021;9(10):653–62. https://doi.org/10.1016/s2213-8587(21)00203-5.
Ren J, Grundy SM, Liu J, Wang W, Wang M, Sun J, et al. Long-term coronary heart disease risk associated with very-low-density lipoprotein cholesterol in Chinese: the results of a 15-Year Chinese multi-provincial cohort study (CMCS). Atherosclerosis. 2010;211(1):327–32. https://doi.org/10.1016/j.atherosclerosis.2010.02.020.
Barkas F, Bathrellou E, Nomikos T, Panagiotakos D, Liberopoulos E, Kontogianni MD. Plant sterols and Plant Stanols in cholesterol management and Cardiovascular Prevention. Nutrients. 2023;15(13). https://doi.org/10.3390/nu15132845.
Holick MF. Vitamin D: importance in the prevention of cancers, type 1 diabetes, heart disease, and osteoporosis. Am J Clin Nutr. 2004;79(3):362–71. https://doi.org/10.1093/ajcn/79.3.362.
Pittas AG, Lau J, Hu FB, Dawson-Hughes B. The role of vitamin D and calcium in type 2 diabetes. A systematic review and meta-analysis. J Clin Endocrinol Metab. 2007;92(6):2017–29. https://doi.org/10.1210/jc.2007-0298.
Dibaba DT. Effect of vitamin D supplementation on serum lipid profiles: a systematic review and meta-analysis. Nutr Rev. 2019;77(12):890–902. https://doi.org/10.1093/nutrit/nuz037.
Mokhtari E, Hajhashemy Z, Saneei P. Serum Vitamin D Levels in relation to hypertension and pre-hypertension in adults: a systematic review and dose-response Meta-analysis of epidemiologic studies. Front Nutr. 2022. https://doi.org/10.3389/fnut.2022.829307.
Mirhosseini N, Rainsbury J, Kimball SM, Vitamin D, Supplementation. Serum 25(OH)D concentrations and Cardiovascular Disease Risk factors: a systematic review and Meta-analysis. Front Cardiovasc Med. 2018;5:87. https://doi.org/10.3389/fcvm.2018.00087.
Hodge C, Taylor C, Vitamin A, Deficiency. StatPearls. Treasure Island (FL) ineligible companies. Disclosure: Christopher Taylor declares no relevant financial relationships with ineligible companies.: StatPearls Publishing Copyright © 2024. StatPearls Publishing LLC.; 2024.
Rogers MA, Chen J, Nallamshetty S, Pham T, Goto S, Muehlschlegel JD, et al. Retinoids Repress Human Cardiovascular Cell Calcification with evidence for distinct selective Retinoid Modulator effects. Arterioscler Thromb Vasc Biol. 2020;40(3):656–69. https://doi.org/10.1161/atvbaha.119.313366.
Mu ZJ, Fu JL, Sun LN, Chan P, Xiu SL. Associations between homocysteine, inflammatory cytokines and Sarcopenia in Chinese older adults with type 2 diabetes. BMC Geriatr. 2021;21(1):692. https://doi.org/10.1186/s12877-021-02622-y.
Li C, Qin J, Liu W, Lv B, Yi N, Xue J, et al. Profiling of Homocysteine metabolic pathway related metabolites in plasma of Diabetic Mellitus based on LC-QTOF-MS. Molecules. 2023;28(2). https://doi.org/10.3390/molecules28020656.
Qi Z, Yang W, Xue B, Chen T, Lu X, Zhang R, et al. ROS-mediated lysosomal membrane permeabilization and autophagy inhibition regulate bleomycin-induced cellular senescence. Autophagy. 2024;1–17. https://doi.org/10.1080/15548627.2024.2353548.
Liu W, Li Q, Wang Q, Ma S, Yang X, Zhang J, et al. Association between body fat composition and hyperhomocysteinemia in the analysis of the baseline data of the Northwest China Natural Population Cohort: Ningxia Project (CNC-NX). J Clin Hypertens (Greenwich). 2023;25(6):573–81. https://doi.org/10.1111/jch.14666.
Vidal-Petiot E. Thresholds for hypertension definition, treatment initiation, and treatment targets: recent guidelines at a glance. Circulation. 2022;146(11):805. https://doi.org/10.1161/circulationaha.121.055177.
Harreiter J, Roden M. [Diabetes mellitus: definition, classification, diagnosis, screening and prevention (update 2023)]. Wien Klin Wochenschr. 2023;135(Suppl 1):7–17. https://doi.org/10.1007/s00508-022-02122-y.
Joseph JJ, Rajwani A, Roper D, Zhao S, Kline D, Odei J, et al. Associations of Cardiometabolic Multimorbidity with all-cause and Coronary Heart Disease Mortality among black adults in the Jackson Heart Study. JAMA Netw Open. 2022;5(10):e2238361. https://doi.org/10.1001/jamanetworkopen.2022.38361.
Kivimäki M, Kuosma E, Ferrie JE, Luukkonen R, Nyberg ST, Alfredsson L, et al. Overweight, obesity, and risk of cardiometabolic multimorbidity: pooled analysis of individual-level data for 120 813 adults from 16 cohort studies from the USA and Europe. Lancet Public Health. 2017;2(6):e277. https://doi.org/10.1016/s2468-2667(17)30074-9.
Yu X, Zheng Y, Liu Y, Han P, Chen X, Zhang N, et al. Association of osteoporosis with Sarcopenia and its components among community-dwelling older Chinese adults with different obesity levels: a cross-sectional study. Med (Baltim). 2024;103(24):e38396. https://doi.org/10.1097/md.0000000000038396.
Zhang J, Cheng Y, Chen C, Wang Q, Yang C, Qiu J, et al. Interaction of estradiol and vitamin D with low skeletal muscle mass among middle-aged and elderly women. BMC Womens Health. 2023;23(1):491. https://doi.org/10.1186/s12905-023-02646-z.
Sewpaul R, Mbewu AD, Fagbamigbe AF, Kandala NB, Reddy SP. Prevalence of multimorbidity of cardiometabolic conditions and associated risk factors in a population-based sample of South africans: a cross-sectional study. Public Health Pract (Oxf). 2021. https://doi.org/10.1016/j.puhip.2021.100193.
Peer N, Balakrishna Y, de Villiers A, Naidoo P. Differential associations of cardio-metabolic diseases by population group, gender and adiposity in South Africa. PLoS ONE. 2018;13(9):e0202899. https://doi.org/10.1371/journal.pone.0202899.
Zhao Y, Zhang H, Liu X, Desloge A, Wang Q, Zhao S, et al. The prevalence of cardiometabolic multimorbidity and its associations with health outcomes among women in China. Front Cardiovasc Med. 2023. https://doi.org/10.3389/fcvm.2023.922932.
Kim J, Baek Y, Jeong K, Lee S. Association of Dietary factors with grip Strength, Body Fat, and prevalence of sarcopenic obesity in rural Korean Elderly with Cardiometabolic Multimorbidity. Front Nutr. 2022. https://doi.org/10.3389/fnut.2022.910481.
Xie H, Li J, Zhu X, Li J, Yin J, Ma T, et al. Association between healthy lifestyle and the occurrence of cardiometabolic multimorbidity in hypertensive patients: a prospective cohort study of UK Biobank. Cardiovasc Diabetol. 2022;21(1):199. https://doi.org/10.1186/s12933-022-01632-3.
Cheng X, Ma T, Ouyang F, Zhang G, Bai Y. Trends in the prevalence of Cardiometabolic Multimorbidity in the United States, 1999–2018. Int J Environ Res Public Health. 2022;19(8). https://doi.org/10.3390/ijerph19084726.
Sakakibara BM, Obembe AO, Eng JJ. The prevalence of cardiometabolic multimorbidity and its association with physical activity, diet, and stress in Canada: evidence from a population-based cross-sectional study. BMC Public Health. 2019;19(1):1361. https://doi.org/10.1186/s12889-019-7682-4.
Marquina C, Mousa A, Scragg R, de Courten B. Vitamin D and cardiometabolic disorders: a review of current evidence, genetic determinants and pathomechanisms. Obes Rev. 2019;20(2):262–77. https://doi.org/10.1111/obr.12793.
Patel L, Vecchia C, Alicandro G. Serum vitamin D and cardiometabolic risk factors in the UK population. J Hum Nutr Diet. 2023;36(3):1019–30. https://doi.org/10.1111/jhn.13075.
Pilz S, Tomaschitz A, Ritz E, Pieber TR. Vitamin D status and arterial hypertension: a systematic review. Nat Rev Cardiol. 2009;6(10):621–30. https://doi.org/10.1038/nrcardio.2009.135.
Sukik A, Alalwani J, Ganji V, Vitamin D. Gut microbiota, and Cardiometabolic Diseases-A possible three-way Axis. Int J Mol Sci. 2023;24(2). https://doi.org/10.3390/ijms24020940.
Yadav AS, Isoherranen N, Rubinow KB. Vitamin a homeostasis and cardiometabolic disease in humans: lost in translation? J Mol Endocrinol. 2022;69(3):R95. https://doi.org/10.1530/jme-22-0078.
Rist PM, Jiménez MC, Tworoger SS, Hu FB, Manson JE, Sun Q, et al. Plasma retinol-binding protein 4 levels and the risk of ischemic stroke among women. J Stroke Cerebrovasc Dis. 2018;27(1):68–75. https://doi.org/10.1016/j.jstrokecerebrovasdis.2017.08.003.
Schiborn C, Weber D, Grune T, Biemann R, Jäger S, Neu N, et al. Retinol and Retinol binding protein 4 levels and Cardiometabolic Disease Risk. Circ Res. 2022;131(7):637–49. https://doi.org/10.1161/circresaha.122.321295.
Gupta M, Meehan-Atrash J, Strongin RM. Identifying a role for the interaction of homocysteine and copper in promoting cardiovascular-related damage. Amino Acids. 2021;53(5):739–44. https://doi.org/10.1007/s00726-021-02979-9.
Acknowledgements
We are grateful to all participants in this study and the data collection staff; without them, the work of the research could never have been completed.
Funding
The current study was supported by the National Natural Science Foundation of China (grant number: 82060592, U22A20360), the Key Research and Development Program of Ningxia Hui Autonomous Region (grant number: 2021BEG02026). The funders had no role in the study design, data collection, data analysis, data interpretation, or writing of the report.
Author information
Authors and Affiliations
Contributions
YZ and YHZ designed the study and drafted the outline. JLand XWL wrote the original draft and reviewed and edited the manuscript. XLY and YLC participated in the Hcy, vitamin A, and vitamin D experiment. JL, XWL and LL organized and analyzed the data. YHZ and YZ critically reviewed and revised the manuscript. All authors read and approved the final version to be published.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Institutional Ethics Committee (IEC) of Ningxia Medical University (Ethics ID 2018-012, 2020 − 689). Written informed consent was obtained from all participants. All investigations were conducted in accordance with the principles of the Helsinki Declaration.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Li, J., Liu, X., Yang, X. et al. Impact of vitamins A, D, and homocysteine on cardiometabolic multimorbidity in Northwest China. Nutr Metab (Lond) 21, 70 (2024). https://doi.org/10.1186/s12986-024-00845-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12986-024-00845-5