
Abstract
Background
This study aimed to investigate the clinical and molecular genetic characteristics of ten children with ornithine carbamoyltransferase deficiency (OTCD) in southeastern China, as well as the correlation between the genotype and phenotype of OTCD.
Methods
A retrospective analysis was performed on the clinical manifestations, laboratory testing, and genetic test findings of ten children with OTCD admitted between August 2015 and October 2021 at Quanzhou Maternity and Children’s Hospital of Fujian Province in China.
Results
Five boys presented with early-onset symptoms, including poor appetite, drowsiness, groaning, seizures, and liver failure. In contrast, five patients (one boy and four girls) had late-onset gastrointestinal symptoms as the primary clinical manifestation, all presenting with hepatic impairment, and four with hepatic failure.Nine distinct variants of the OTC gene were identified, including two novel mutations: c.1033del(p.Y345Tfs*50) and c.167T > A(p.M56K). Of seven patients who died, five had early-onset disease despite active treatment. Three patients survived, and two of them underwent liver transplantation.
Conclusions
The clinical manifestations of OTCD lack specificity. However, elevated blood ammonia levels serve as a crucial diagnostic clue for OTCD. Genetic testing aids in more accurate diagnosis and prognosis assessment by clinicians. In addition, we identified two novel pathogenic variants and expand the mutational spectrum of the gene OTC, which may contribute to a better understanding of the clinical and genetic characteristics of OTCD patients.
Similar content being viewed by others


Background
Ornithine transcarbamylase deficiency (OTCD; MIM 311250) is an X-linked inborn error of the urea cycle caused by mutations in the gene OTC located on chromosome Xp11.4. Consequently, hemizygous males develop this condition. They have a spectrum of severity ranging from complete OTCD, which presents at the neonatal stage with acute hyperammonemia, to partial OTCD, manifesting with mild symptoms and late-onset [1]. The clinical presentation of carrier females also differs greatly, owing to the degree of X-inactivation in hepatocytes [2]. Therefore, OTCD can be easily misdiagnosed.
In the urea cycle, ornithine transcarbamylase (OTC) is required for the production of citrulline and inorganic phosphates from carbamyl phosphate and ornithine. OTC variants result in decreased or absent OTC enzyme activity, blocking citrulline synthesis and interrupting the urea cycle. This leads to hyperammonemia and accumulation of orotic acid [3]. The clinical manifestations of hyperammonemia are nonspecific, often resulting in a delay in the diagnosis of OTCD [4]. According to the onset period, OTCD can typically be divided into two groups: early-onset (≤ 30 days) and late-onset (> 30 days). Since the first symptoms of OTCD are extremely variable and molecular genetic testing is necessary for diagnosis, it is essential to accumulate information on genetic analyses and clinical phenotypes to determine genotype-phenotype correlations. This study reports the clinical and biochemical features and molecular characteristics of ten Chinese patients with OTCD. We also reviewed the relevant literature and analyzed the relationship between the phenotypes and genotypes.
Materials and methods
Study subjects
Ten patients diagnosed with OTCD were recruited between August 2015 and October 2021 at Quanzhou Maternity and Children’s Hospital of Fujian Province in China.Diagnosis of OTCD was based on clinical features, specific biochemical criteria, and molecular analyses. A retrospective review of clinical manifestations and laboratory tests, including blood ammonia levels, liver function tests, tandem mass spectrometry (MS/MS), urine organic acids, in addition to color ultrasound, was conducted. This study was approved by the Ethics Committee of the Quanzhou Maternity and Children’s Hospital, China. The patients’ parents provided written informed consent for participation in the study.
Genetic analysis
After obtaining informed consent, 2 mL of peripheral blood was collected from patients and their parents. Whole-exome sequencing (WES) was performed on samples from the ten patients. Raw reads were processed by fastp, followed by paired-end sequencing of reads aligned to the human GRCh37/hg19 genome using the Burrows-Wheeler Aligner (BWA) software package. GATK software (https://software.Broadinstitute.org/gatk/) was used for SNPs and indel calling. Mutations were described according to the HGVS recommendations (http://wwwhgvs.org/mutnomen/recsprot.htm1). PolyPhen-2, PROVEAN, Mutation Taster, and Sorting Intolerant From Tolerant (SIFT) were used to analyze the potential pathogenicity of the missense mutations. Amino acid conservation was predicted using phyloP and phastCons, and homologous amino acid sequences were compared using DNAMAN software. The pathogenicity of all variants was evaluated according to the American College of Medical Genetics and Genomics (ACMG) clinical practice guidelines [5]. These variants were considered novel if they were not found in the Human Gene Mutation, ClinVarMiner, or Exome Aggregation databases. The results were verified using Sanger sequencing.
Results
Clinical features of OTCD patients
Table 1 presents the demographic and clinical findings of ten patients with OTCD from nine unrelated families. All patients appeared normal at birth. Five patients (one boy and four girls) had a late-onset form of the disease, with a median age of 3.2 years (ranging 1.5 years to 6.3 years) and normal growth and development until the time of the first clinical manifestations. The most prevalent symptoms observed in these five patients were gastrointestinal distress, including vomiting and feeding refusal, followed by liver dysfunction and psychiatric symptoms. Treatment was initiated with a low-protein diet, intravenous fluid and energy replenishment, arginine supplementation to reduce blood ammonia, continuous renal replacement therapy (CRRT). Two died of hyperammonemia. Three exhibited clinical remission, and two of them underwent liver transplantation with normal growth and development after surgery. The other girl experienced multiple hospitalizations due to hepatic dysfunction and hyperammonemia, and she also experienced mild intellectual disability. Five male patients presented with early-onset symptoms within 1–7 days after birth, including poor appetite, drowsiness, groaning, and seizures. Initially misdiagnosed as neonatal infection or neonatal encephalopathy, the patients’ condition progressed to seizures and coma within 1–2 days, resulting in death within 10 days after birth.
Biochemical results and liver ultrasound at OTCD diagnosis
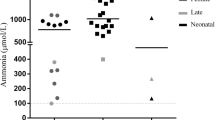
Table 1 summarizes the results of the biochemical analyses for each patient. Notably, elevated blood ammonia levels were observed in all patients tested. Peak ammonia levels were significantly higher in the early-onset group than those in the late-onset group, indicating a potential association with disease severity. In the late-onset group, all patients exhibited elevated transaminase levels. Four of them (P1, P2, P4, and P7) experienced liver failure, while only one patient in the early-onset group did. Urinary orotic acid levels increased in all patients tested except for one, for whom specimens were retained after CRRT therapy. Only six patients demonstrated decreased serum levels of citrulline. Five patients underwent color Doppler ultrasound examination of the liver, and three showed hyperechoic livers.
Mutation analysis of the OTC gene
We detected nine distinct mutations in the OTC gene in ten patients, consisting of six missense mutations, two frameshift mutations, and one gross deletion (Table 2). Two of these mutations were previously unreported (NM_000531.6): c.1033del and c.167T > A. According to the ACMG guidelines, the variant c.1033del (p.Y345Tfs*50) was evaluated as pathogenic (PVS1 + PS2_Moderate + PM2) and c.167T > A (p.M56K) as likely pathogenic (PM1 + PM2 + PM5 + PP3). Multiple sequence alignment using Clustal X was performed. The methionine residue at position 56 and tyrosine residue at position 345 (highlighted by a red box) are highly conserved among different species (Fig. 1). The remaining seven variants (c.140del, c.1028 C > G, c.116G > T, c.674 C > T, exon5 del, c.77G > A, and c.725 C > T) have been documented in Human Gene Mutation Database(HGMD), ClinVar, and the literature. Both variants identified in P1 and P2 were de novo and were not detected in the peripheral blood of their mother. The mutations in the remaining eight patients were inherited from their healthy mothers.

A conservative analysis of the two new loci
Discussion
The clinical symptoms of OTCD are non-specific and often misdiagnosed as gastrointestinal disease or liver disease, food or drug poisoning, or central nervous system infection. This can delay diagnosis and treatment, leading to a high mortality rate [6,7,8]. Hyper-ammonemia is a critical diagnostic indicator. In this study, five male patients presented with early-onset symptoms. Clinical manifestations of affected subjects include eating difficulties, drowsiness, groaning, and seizures. The main symptoms in our late-onset patients were poor appetite, vomiting, lethargy and abnormal liver function.
Blood ammonia levels should be promptly tested in patients with unexplained gastrointestinal symptoms, abnormal liver function, or encephalopathy. Early-onset patients exhibited significantly increased ammonia levels, while late-onset ones exhibited greater variability. Among our late-onset patients, two with significantly increased blood ammonia levels died despite active treatment, while two children who underwent liver transplantation survived. One patient (P7) with moderately increased blood ammonia levels improved after receiving low protein diet and arginine treatment, but later presented with recurrent hyperammonemia and mild intellectual disability. These cases underscore the high mortality rate associated with OTCD and highlight the crucial role of blood ammonia levels in determining the disease severity and prognosis.
The correlation between OTCD and liver complications is increasingly recognized, with over 50% of symptomatic OTCD patients experiencing such condition [9,10,11,12]. In some instances, acute liver diseases(ALF) may be the first sign of OTCD [10, 12]. Furthermore, patients with acute hyperammonemia may experience recurrent episodes of ALF [11, 13]. ALF is the most common complication in male newborns with severe OTCD [10, 11]. In this study, all four girls with late-onset OTCD had ALF, whereas only one of five boys with early-onset OTCD experienced ALF. More recently, a comprehensive review has summarized that acute liver failure is a more frequent observation in OTCD, but the specific underlying mechanisms are still not well elucidated [9]. Moreover, a late-onset patient with a peak blood ammonia level of 222 mol/L developed severe ALF, indicating that the blood ammonia level is not always the direct cause of liver failure. Studies have proposed that the inhibition of liver protein synthesis rather than nonspecific cell death due to hyperammonemia is a potential mechanism in hyperammonemia-induced ALF [11]. One study showed that patients had a high rate of liver hyperechogenicity, and more precisely in the 53% of female patients and 42% of male ones [9]. In our study, five patients underwent color Doppler ultrasound examination of the liver, of which three showed a hyperechoic liver and one did not. The specific significance of liver hyperechogenicity is unclear.Further research is needed to investigate the underlying mechanisms of liver disease in OTCD to provide better treatment strategies for this complication.
The interaction between genomic and epigenetic factors leads to different phenotypes of disease [14],OTC mutations show high heterogeneity [1, 6]. In this study, nine OTC gene variants were detected in ten patients: seven were previously reported, while two variants, c.1033del and c.167T > A are novel. The heterozygous deletion of c.1033del resulted in a frameshift mutation, leading to the formation of a truncated protein (p.Y345Tfs*50) and a loss-of-function variant, identified by ACMG as pathogenic (PVS1 + PS2_Moderate + PM2). The c.167T > A missense variant is located in a highly conserved region of OTC enzymes at the junction of three crucial helices (helices 1, 5, and 11) that bridge the two domains of the protein [15]. Therefore, this variant may affect interdomain alignment, thus affecting enzyme activity, as well as a mutation in the pathogenic amino acid residue p.M56T at this locus, which has been reported to be related to late-onset OTCD [15,16,17]. According to the pathogenicity classification of ACMG, this is likely to be a pathogenic mutation (PM1 + PM2 + PM5 + PP3).
Disease severity depends on OTC activity, which is influenced by the type and site of mutations [16, 18] and environmental factors, including daily protein intake [7, 8]. The complete loss of OTC function caused by large deletions, frameshifts, or nonsense mutations often leads to a severe neonatal onset [16, 17]. This study found P8 with the deletion of exon 5 of the OTC gene exhibiting early-onset, while two patients (P1 and P2) with frameshift mutations who showed severe late-onset. The c.140del variant of P2 has also been reported in a Chinese female patient who died after drug treatment [6].
Some missense mutations can cause a complete loss of OTC function, leading to severe neonatal-onset diseases in hemizygous males and most symptomatic heterozygous females. Missense mutations which retain some OTC activity can cause late-onset in hemizygous males [16, 17]. In this study, we detected the missense mutation c.1028 C > G in P3, which has a relatively mild late-onset clinical presentation. This mutation was previously found in a male late-onset patient without neurological damage [19], suggesting that it may partially preserve OTC activity and present as late-onset in male subjects. P225L is a relatively common mutation in the Chinese OTCD population [6]. It has been identified in several male patients with early-onset, all of whom experienced severe hyperammonemia and died during the neonatal period [20,21,22,23,24]. This indicates that the P225L variant is associated with severe male early-onset. Although the correlation between genotype and phenotype is not yet clear, genetic testing can support the clinician in providing a more precise diagnostic evaluation and solid evidence for counselling to the affected families [25], and it should facilitate the functional study on the proteins in urea cycle.
In this study, among the seven patients with parental validation, five had mutations in healthy mothers, including two female patients with severe hyperammonemia whose mothers were also healthy. Members of the same family with the same mutation can have great differences in phenotype. Moreover, the clinical manifestations of OTCD in affected women within the same family may differ [20, 26] due to random X chromosome inactivation or mosaicism, epigenetics, diet, lifestyle, nutrition, and other factors [2, 27]. This highlights the diversity of clinical manifestations of late-onset OTCD and the multi-factor influence of the OTC gene, which further complicates the prenatal diagnosis of female heterozygotes.
Conclusions
Overall, we analyzed the clinical and genetic characteristics of ten patients with OTCD and identified two novel OTC pathogenic variants. The clinical symptoms of the disease are nonspecific. However, hyperammonemia is an important diagnostic clue and is related to prognosis. Genetic testing not only helps to make a definitive diagnosis, but also supports the clinician in providing a more precise prognostic evaluation. More samples are needed to deeply explore the correlation between genotype and phenotype. The prognosis of OTCD is closely related to liver complications. Further studies are needed to better understand the potential mechanisms.
Data availability
The datasets used and analyzed in the current study are available from the corresponding author upon reasonable request.
Abbreviations
- OTCD:
-
Ornithine carbamoyltransferase deficiency
- OTC:
-
Ornithine transcarbamylase
- MS/MS:
-
Tandem mass spectrometry
- WES:
-
Whole-exome sequencing
- ACMG:
-
American Academy of Medical Genetics and Genomics
- UCD:
-
Urea cycle disorder
- ALF:
-
Acute liver diseases
- CRRT:
-
Continuous renal replacement therapy
References
Choi JH, Lee BH, Kim JH, Kim GH, Kim YM, Cho J, et al. Clinical outcomes and the Mutation Spectrum of the Otc Gene in patients with Ornithine Transcarbamylase Deficiency. J Hum Genet. 2015;60(9):501–7.
Musalkova D, Sticova E, Reboun M, Sokolova J, Krijt J, Honzikova J, et al. Variable X-Chromosome inactivation and enlargement of Pericentral glutamine synthetase zones in the liver of heterozygous females with Otc Deficiency. Virchows Arch. 2018;472(6):1029–39.
Wraith JE. Ornithine Carbamoyltransferase Deficiency. Arch Dis Child. 2001;84(1):84–8.
Häberle J, Burlina A, Chakrapani A, Dixon M, Karall D, Lindner M, et al. Suggested guidelines for the diagnosis and management of Urea Cycle disorders: first revision. J Inherit Metab Dis. 2019;42(6):1192–230.
Richards S, Aziz N, Bale S, Bick D, Das S, Gastier-Foster J, et al. Standards and guidelines for the interpretation of sequence variants: a Joint Consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet Med. 2015;17(5):405–24.
Lu D, Han F, Qiu W, Zhang H, Ye J, Liang L, et al. Clinical and molecular characteristics of 69 Chinese patients with Ornithine Transcarbamylase Deficiency. Orphanet J Rare Dis. 2020;15(1):340.
Brassier A, Gobin S, Arnoux JB, Valayannopoulos V, Habarou F, Kossorotoff M, et al. Long-term outcomes in Ornithine Transcarbamylase Deficiency: a Series of 90 patients. Orphanet J Rare Dis. 2015;10:58.
Barkovich E, Gropman AL. Late Onset Ornithine Transcarbamylase Deficiency triggered by an Acute increase in protein intake: a review of 10 cases reported in the literature. Case Rep Genet. 2020;2020:7024735.
Ranucci G, Rigoldi M, Cotugno G, Bernabei SM, Liguori A, Gasperini S, et al. Chronic liver involvement in Urea Cycle disorders. J Inherit Metab Dis. 2019;42(6):1118–27.
Gallagher RC, Lam C, Wong D, Cederbaum S, Sokol RJ. Significant hepatic involvement in patients with Ornithine Transcarbamylase Deficiency. J Pediatr. 2014;164(4):720–e56.
Laemmle A, Gallagher RC, Keogh A, Stricker T, Gautschi M, Nuoffer JM, et al. Frequency and pathophysiology of Acute Liver failure in Ornithine Transcarbamylase Deficiency (Otcd). PLoS ONE. 2016;11(4):e0153358.
Rajabi F, Rodan LH, Jonas MM, Soul JS, Ullrich NJ, Wessel A, et al. Liver failure as the presentation of Ornithine Transcarbamylase Deficiency in a 13-Month-Old Female. JIMD Rep. 2018;40:17–22.
Samuel N, Politansky AK, Hoffman R, Itzkovich S, Mandel H. Coagulopathy Unmasking Hepatic Failure in a child with Ornithine Transcarbamylase Deficiency. Isr Med Assoc J. 2013;15(12):777–9.
Serra G, Felice S, Antona V, et al. Cardio-facio-cutaneous syndrome and gastrointestinal defects: report on a newborn with 19p13.3 deletion including the MAP 2 K2 gene. Ital J Pediatr. 2022;48(1):65.
Shih VE, Safran AP, Ropper AH, Tuchman M. Ornithine Carbamoyltransferase Deficiency: unusual clinical findings and Novel Mutation. J Inherit Metab Dis. 1999;22(5):672–3.
Yamaguchi S, Brailey LL, Morizono H, Bale AE, Tuchman M. Mutations and polymorphisms in the human ornithine transcarbamylase (otc) gene. Hum Mutat. 2006;27(7):626–32.
Tuchman M, Morizono H, Rajagopal BS, Plante RJ, Allewell NM. Identification of ‘Private’ mutations in patients with Ornithine Transcarbamylase Deficiency. J Inherit Metab Dis. 1997;20(4):525–7.
Caldovic L, Abdikarim I, Narain S, Tuchman M, Morizono H. Genotype-phenotype correlations in Ornithine Transcarbamylase Deficiency: a mutation update. J Genet Genomics. 2015;42(5):181–94.
Martín-Hernández E, Aldámiz-Echevarría L, Castejón-Ponce E, Pedrón-Giner C, Couce ML, Serrano-Nieto J, et al. Urea Cycle disorders in Spain: an Observational, cross-sectional and multicentric study of 104 cases. Orphanet J Rare Dis. 2014;9:187.
Hentzen D, Pelet A, Feldman D, Rabier D, Berthelot J, Munnich A. Fatal hyperammonemia resulting from a C-to-T mutation at a Mspi Site of the Ornithine Transcarbamylase Gene. Hum Genet. 1991;88(2):153–6.
Liu N, Feng Y, Jiang M, Kong X. [Genetic testing and prenatal diagnosis in seven pedigrees affected with Ornithine Transcarbamylase Deficiency]. Zhonghua Yi Xue Yi Chuan Xue Za Zhi. 2020;37(2):106–9.
Shao Y, Jiang M, Lin Y, Mei H, Zhang W, Cai Y, et al. Clinical and mutation analysis of 24 Chinese patients with Ornithine Transcarbamylase Deficiency. Clin Genet. 2017;92(3):318–22.
Matsuda I, Tanase S. The Ornithine transcarbamylase (otc) gene: mutations in 50 Japanese families with Otc Deficiency. Am J Med Genet. 1997;71(4):378–83.
García-Pérez MA, Climent C, Briones P, Vilaseca MA, Rodés M, Rubio V. Missense mutations in Codon 225 of Ornithine Transcarbamylase (Otc) result in decreased amounts of otc protein: a hypothesis on the molecular mechanism of the Otc Deficiency. J Inherit Metab Dis. 1997;20(6):769–77.
Serra G, Antona V, Giuffrè M, et al. Interstitial deletions of chromosome 1p: novel 1p31.3p22.2 microdeletion in a newborn with craniosynostosis, coloboma and cleft palate, and review of the genomic and phenotypic profiles. Ital J Pediatr. 2022;48(1):38.
Pizzi MA, Alejos D, Hasan TF, Atwal PS, Krishnaiengar SR, Freeman WD. Adult Presentation of Ornithine Transcarbamylase Deficiency: 2 Illustrative Cases of Phenotypic Variability and Literature Review. Neurohospitalist (2019) 9(1):30 – 6.
Lee T, Misaki M, Shimomura H, Tanaka Y, Yoshida S, Murayama K, et al. Late-Onset Ornithine Transcarbamylase Deficiency caused by a somatic Mosaic mutation. Hum Genome Var. 2018;5:22.
Acknowledgements
The authors wish to thank the patients and their families for their participation in this study.We are grateful to Dr. Zhongshi Zheng for his invaluable advice.
Funding
This work was funded by Science and Technology Plan Project of Quanzhou Science and Technology Bureau (Grant No. 2022C002).
Author information
Authors and Affiliations
Contributions
GY and ZL conceived the study and wrote the first draft of the manuscript. WZ and DC helped critically revise the manuscript for important intellectual content and were the mentors who designed and guided the research study. XZ and ZC oversaw patient care and collected the clinical data. All authors contributed to manuscript revision, read, and approved the final submitted version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Medical Ethics Committee of Quanzhou Women’s and Children’s Hospital.All procedures in this study involving human participants were carried out in line with the principles of Helsinki Declaration.And informed consent from the patient’s parents prior to conducting the exome sequencing had been obtained, including the patient’s clinical details in the manuscript for the purpose of publication.
Consent for publication
The written informed consent was waived because of the retrospective and anonymous nature of the data.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Yuan, G., Liu, Z., Chen, Z. et al. Clinical characteristics and molecular genetic analysis of ten cases of ornithine carbamoyltransferase deficiency in southeastern China. Ital J Pediatr 50, 171 (2024). https://doi.org/10.1186/s13052-024-01740-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13052-024-01740-8