
Abstract
Background
Follow-up studies on coronavirus disease 2019(COVID-19) were mainly focused on short-term sequelae in patients with comorbid diseases. The aim of this study was to investigate the pulmonary and extrapulmonary sequelae of moderate to severe COVID-19 in the midterm follow-up of healthy young adults.
Methods
In this prospective cohort study, we used the hospital information system (HIS) to identify patients who had recovered from moderate to severe COVID-19 without comorbidity. All eligible patients were invited to participate in the study. Participants were asked to fill out a set of questionnaires to evaluate fatigue, anxiety, and post-traumatic stress disorder (PTSD). They also underwent chest computed tomography (CT) scan, pulmonary function test (PFT), and tissue doppler imaging (TDI) echocardiography. A blood sample and a 12-lead electrocardiogram (ECG) were obtained.
Results
A total of 50 recovered patients and 12 healthy controls were enrolled in the study. Fifteen out of 50 patients received intensive care. Patients had significantly higher fatigue and anxiety scores than controls. PTSD criteria were met in 29 out of 50 patients. Ground glass opacities, nodules, and subpleural lines were the most frequent abnormalities in chest CT scans of patients. Patients had significantly lower left ventricular end-diastolic diameter (LVEDD) and left ventricular end-systolic diameter (LVESD) than controls (P value 0.019 and < 0.001, respectively).
Conclusions
According to our findings, COVID-19 survivors might experience anxiety, fatigue, PTSD, pulmonary impairment, leading to reduced cardiac function up to 6 months after discharge.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Introduction
During the ongoing pandemic, approximately 269 million people have been infected by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), of whom 243 million have recovered as of 13th December 2021 [1]. Hundreds of thousands of people are getting infected with COVID-19 every day, and a significant proportion of them recover from the disease.
A good deal of literature has focused on the treatment and course of the illness and vaccination against it. As the number of the recovered COVID-19 patients increases, there is a concern about the post-acute and long-term sequelae, also known as long COVID [2]. According to previous literature, the severity of COVID-19 is associated with that of sequelae [3].
The radiological findings on the lung computed tomography (CT) scan, laboratory and pulmonary function test findings, mental health disturbances, and cardiac workup in the short-term follow-up have been studied [2, 4,5,6,7,8]. Most studies included old patients with comorbidities [9].
An increasing number of studies have investigated mid-to-long-term sequelae of COVID-19 in the young population. According to a recent systematic review, long-term follow-up in healthy young adults, especially cardiac and pulmonary sequelae of COVID-19, has yet to be studied [9]. Therefore, this study aimed to investigate the pulmonary and extrapulmonary sequelae of moderate to severe COVID-19 in the midterm follow-up of healthy young adults.
Materials and methods
Study design
We conducted a prospective cohort study on moderate to severe COVID-19 survivors to investigate the pulmonary and extrapulmonary midterm sequelae.
The study population
The study population in the exposed group consisted of COVID-19 survivors aged 18–50 without underlying medical conditions who were hospitalized in Hospitals affiliated to Alborz University of Medical Sciences in Karaj, Iran, between April 3, 2020, and August 22, 2020. We identified them using a hospital information system (HIS).
The unexposed participants were recruited from healthy hospital staff younger than 50 years without a history of COVID-19.
The study inclusion criteria for recruiting COVID-19 Survivors were as follows:
-
Having a positive real-time reverse transcriptase polymerase-chain-reaction (RT-PCR) test result for SARS-CoV-2
-
Aged 18 to 50 years
-
Having a minimum of 1 month from the discharge date
-
Without underlying medical conditions (including diabetes mellitus, hypertension, hypo/hyper-thyroidism, cardiovascular disease, autoimmune disease, pulmonary disease, hepatic dysfunction, kidney dysfunction)
Exclusion criteria
-
Unwillingness to participate in the study
Ethical approval statement
The ethics committee of Alborz University of Medical Sciences approved the study protocol . The written informed consent was obtained from all the participants.
Data collection
The patients’ medical records were reviewed to collect the demographics and clinical characteristics, and contact information of the participants . All patients were contacted by phone to invite them to participate in the study. Participants were asked to fill out a series of questionnaires, including the brief fatigue inventory (BFI), post-traumatic stress disorder checklist (PCL), Hamilton, 36-item short-form survey (SF-36), and the demographic data questionnaire. On the follow-up visit, patients underwent a chest CT scan, PFT, TDI echocardiography, and also a blood sample, and a standard 12-lead electrocardiography were obtained. The participants’ weight and height were also measured and recorded.
Questionnaires
The first questionnaire consisted of demographic data, filled out by the participants, and heart rate and blood pressure were measured by a team member. The brief fatigue inventory (BFI) was used to measure fatigue intensity and its interference with daily activity. BFI is composed of nine to eleven-point (0 to 10) scale. A mean BFI score was calculated. A mean BFI score greater than or equal to seven is considered severe fatigue [10].
The post-traumatic stress disorder checklist for civilians (PCL-C) is a 17-item questionnaire measuring 17 Diagnostic and statistical manual of mental disorders (DSM-IV) symptoms ranging from 1 to 5. A total score greater than 33 is considered diagnostic for post-traumatic stress disorder (PTSD) [11]. Hamilton anxiety scale (HAMA) is a questionnaire consisting of 14- to 5-point scale [12].
The 36-item short-form survey (SF-36) was used to measure eight health concepts as follows: physical functioning (10 items), role limitations due to physical health (4 items), role limitations due to mental health (3 items), energy (4 items), emotional well-being (5 items), social functioning (2 items), pain (2 items), and general health (5 items) [13].
Pulmonary function test and chest computed tomography (CT) scan
A technician performed pulmonary function tests. The pulmonary function included forced expiratory volume in the first second (FEV1), forced vital capacity (FVC), FEV1/FFVC, forced mid-expiratory flow (FEF25-75%), and peak expiratory flow (PEF). Parameters were reported as a percentage (%) of the reference value for each patient, calculated by Global Lung Function 2012 equations [14].
CT scan images were acquired with the patient in the supine position at the end of inhalation using a 64-row CT scanner. Two senior cardiothoracic radiologists reviewed all CT images in random order who were not aware of any clinical or laboratory findings or patient outcomes. The readers independently assessed the CT features using axial and multiplanar reconstructed images. After the independent evaluation, the radiologists resolved any disagreement with discussion and consensus.
Tissue doppler echocardiography
Echocardiographic examinations were performed in the left lateral decubitus position. An ultrasound instrument (affinity 70, Phillips medical system) was used with an S5 transducer. All the measurements were performed by a single experienced echocardiography fellow in order to avoid inter-observer variability.
Lab data
Blood samples were taken for the measurement of lipid, glucose, iron, and coagulation profiles, liver enzymes, kidney and thyroid function tests, serum vitamin D3, electrolytes, uric acid, albumin, magnesium, and creatine kinase myocardial band (CPK-MB), and SARS-CoV-2 IgM and IgG level, quantitative troponin I, and C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), and complete blood count (CBC) with differentials.
Statistical analysis
Variables were summarized using median (interquartile range (IQR) ) or percentage (number), as appropriate. Mann-Whitney test, chi-square test, and Fisher’s exact analysis were used to compare the study groups. A significance level of 0.05 was used in all analyses. Statistical analyses were performed using SPSS Version 21.0.
Results
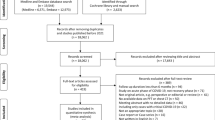
A total of 50 COVID-19 survivors with moderate to severe disease (response rate 10%) and 12 healthy controls provided their written informed consent to participate in our study. There were no significant differences between the two groups with respect to age and gender, but compared to controls, COVID-19 patients had a higher body mass index (BMI) (28.1 (26.1–30.2) vs. 24.8 (23.7–28.0)) and were less educated (college level 32% vs. 75%).
In the COVID-19 group, the median length of hospital stay was seven days (interquartile range ((IQR) 5 to 10); 15 patients received intensive care during the hospitalization, of whom three underwent invasive mechanical ventilation. The median time from discharge to follow-up was 6 months (IQR 3 to 7 months) (Table 1).
Laboratory findings at the follow–up time are presented in Table 2. A lower concentration of AST (median (IQR) 26.0 (20.8–32.0) vs. 35.0 (30.5–39.0) U/L), albumin (4.5 (3.9–4.7) vs. 4.9 (4.7–5.1) g/L), direct bilirubin (0.19 (0.1–0.2) vs. 0.2 (0.2–0.4) mmol/L), HDL (44.5 (39.7–54.0) vs. 62 (51–67) mg/Dl), LDL (112 (97–137) vs. 140 (114–157) mg/dL), and TSH (1.65 (0.78–2.43) vs. 2.05 (1.8–3.2) mIU/L) was found in COVID-19 survivors compared to controls, but a higher level of FBS (94.5 (86.8–100.0) vs. 81.0 (75.3–99.0) mmol/L), HbA1C (5.05 (4.7–5.43) vs. 4.6 (4.2–5.0) %), and mg (2.4 (2.1–2.5) vs. 2.1 (1.95–2.20) mg/Dl) was observed in COVID-19 survivors compared to controls. (all P value < 0.05).
Compared to other patients, COVID-19 patients admitted to the ICU had a higher level of Ferritin (136.0 (93.0–219.0) vs. 59.0 (14.0–104.0) ng/ml), total bilirubin (0.7 (0.4–1.2) vs. 0.5 (0.4–0.7) mmol/L), LDH (348 (299–391) vs. 282 (256–341) U/L), and D3 (23.0 (20.0–33.0) vs. 18.0 (12.0–23.0) ng/ml), (all P value < 0.05) but had a lower concentration of Albumin (4.0 (3.8–4.6) vs. 4.5 (4.0–4.8) g/L; P value = 0.052).
In addition, COVID-19 patients admitted to the ICU had a higher serum IgG level than other patients (7.8 (2.2–10.5) vs. 1.7 (1.2–3.3) g/L; P value = 0.017).
Health-related quality of life (HRQoL) and mental health
COVID-19 survivors had a lower score in all SF-36 dimensions compared to controls; however, these differences were not statistically significant in two domains: emotional well-being and social functioning (Table 3) (both P value > 0.05).
Symptom score for anxiety in COVID-19 patients was higher than that in controls (HAM-A median score (IQR) 13.0 (7.5, 20.5) vs. 4.0 (2.3, 7.8), P value < 0.001). However, symptoms of moderate to severe anxiety [a HAM-A score of 25 to 30] were observed in 20 % of COVID-19 patients and none of the controls.
Twenty-nine out of 50 COVID-19 patients met positive criteria for PTSD symptoms according to the PCL-C score [PCL ≥ 33].
Patients significantly had higher fatigue scores than controls (BFI median score (IQR) 4.78 (2.72, 6.56) vs. 2.67 (1.89, 3.11), P value = 0.004); 7 participants in COVID-19 group (14%) and no participant in control group had severe fatigue (BFI score 7 to 10).
No statistically significant differences were found between ICU and non-ICU patients in terms of HRQoL, fatigue, and anxiety levels, but non-ICU patients more frequently reported symptoms of PTSD than ICU patients (71% (25) vs. 27% (4), P value = 0.004).
Pulmonary function and chest computed tomography (CT) scan findings
A total of 47 COVID-19 survivors received the lung function test. Abnormalities in FVC, FEV1, and FEV1/FVC % predicted were observed in 6/47 (12.8%), 14/47 (29.8%), and 5/47 (11%), respectively. Proportion of patients with FEF 25-75 and peak expiratory flow % predicted < 80 were 55% (26) and 68% (32), respectively (Table 4).
During the hospitalization, 45 out of 50 COVID-19 patients had abnormalities on chest CT scans.
On follow-up CT imaging of these patients, 57.8% (26) of patients had consolidation was found in one of them. Subpleural line, Nodules, and radiological signs of fibrosis were present in 11.1% (5), 22.2% (10), and 33.3% (15) of patients, respectively. No patient had reticulation. Left and right S1 (N = 6), S2 (N = 6), and S3 (N = 7) were the most frequently involved segments (Table 4).
No significant differences were detected between ICU and non-ICU admitted patients with respect to the evaluated spirometry and CT scan parameters.
Cardiac evaluation
High-sensitivity troponin T concentration was within the normal range in all participants.
On standard ECG, 86% (43) of COVID-19 patients had normal sinus rhythm. In other patients, ECG rhythm findings include sinus bradycardia (n = 3), left anterior fascicular block (n = 2), and right bundle branch block (n = 2). The most common ECG changes, in order by frequency, were ST elevation (n = 18), Tall R wave (n = 17), inverted T wave (n = 16), and biphasic T wave (n = 15) (Table 5).
On echocardiography, COVID-19 group compared to controls had significantly lower LV end diastolic echo dimensions (LVEDD) (median (IQR) 4.33 (4.00, 4.55) vs. 4.53 (4.40, 4.80); P value = 0.019) and left ventricular end systolic diameter (LVESD) (2.1 (2.1, 2.3) vs. 2.4 (2.4, 2.8)), and Septal-Em (7.9 (6.2, 9.4) vs. 9.4 (8.0, 11.2), P value = 0.049) values (Table 5).
Left ventricle ejection fraction (LVEF) less than 50% was observed in three COVID-19 patients, and the ICU-admitted patient group, but none of the controls. In addition, Global longitudinal strain (GLS) less than 16% was more frequently detected in COVID-19 patients (20% (9)) than controls (9% (1), bur their difference were not statistically significant.
A higher proportion of ICU-admitted patients had abnormal LV diastolic dysfunction than non-ICU patients.
Discussion
In this study, we presented follow-up data of patients with moderate to severe COVID-19, 6 months after discharge from the hospital. One-fifth of patients had moderate to severe anxiety, more than half met PTSD criteria, and seven reported extreme fatigue. More than half of the patients had GGO without consolidation on chest CT imaging. GGO, nodule, and subpleural lines were the most frequent abnormalities in chest CT. In this study, the rate of restrictive lung impairment was approximately 12% after 6 months of discharge. More than half of the survivors had impaired peak expiratory flow rate or FEF 35–75. Patients had significantly lower LVEDD, LVESD, and septal-Em than the control group. Serum SARS-CoV-2 IgG concentration was higher in ICU admitted patients. Non-ICU patients reported PTSD symptoms more frequently compared to ICU-admitted patients. Pulmonary function tests and chest CT scans findings were similar between ICU and non-ICU admitted patients. Three ICU admitted patients had a LVEF less than 50%.
Our findings are in line with previous studies reporting that a large number of COVID-19 survivors would suffer from fatigue, anxiety, PTSD, and reduced quality of life weeks after the infection was subsided. These psychiatric disorders were reported up to 3 years after SARS-CoV and Middle East respiratory syndrome (MERS) infections [9]. ICU patients are often sedated. Sedation relieves stress. On the other hand, the literature suggests that the healthcare providers’ compassion can reduce post-discharge PTSD in critically ill patients [15]. The ICU staff are more compassionate. These might explain the lower incidence of PTSD among the non-ICU admitted survivors.
A 3-month follow-up study conducted by Salem et al. demonstrated that half of the COVID-19 survivors had restrictive lung impairment on PFT [16]. An 8-month follow-up study reported FEV1/FVC abnormality in 20% of participants, of whom 5% (two patients) had a history of chronic obstructive pulmonary disease (COPD) with a significant history of cigarette smoking [17]. Our findings are in line with a recent meta-analysis reporting a 15% overall prevalence of restrictive patterns [18]. Impaired peak expiratory flow rate and FEF 25–75% indicated small airway obstruction. A high prevalence of small airway obstruction is reported, similar to pervious literature [17]. Autopsies of COVID-19 patients have shown destructed alveolar structure and pulmonary interstitial fibrosis [18].
The most frequent ECG findings are bradycardia, conduction block, and ST-T wave changes. Persistent cardiovascular injury is suspected as the ECG abnormalities are observed in a significant proportion of recovered patients upon a 1-year follow-up [19]. On echocardiography, LV systolic dysfunction was only observed in the ICU-admitted survivors. LV diastolic dysfunction was more frequent in the ICU-admitted patients. This study is in line with a 4-month follow-up study reporting a lower ejection fraction than 50% in 10% of ICU-admitted patients [20].
This study shows a significant number of COVID-19 survivors had sequelae after 6 months of discharge, the most frequently psychological and pulmonary sequelae. Based on the experience with SARS and MERS, more extended follow-up studies are necessary. Future studies should consider the COVID-19 treatment received for each patient while assessing the disease’s long-term impact.
Strengths
The study population consisted of patients without comorbidity, so our findings are primarily suggestive of COVID-19 sequelae rather than exacerbation of the comorbid disease. We studied multiple organ systems in this comprehensive study.
Limitations
The first main limitation of this study was the small sample size. Low response rate is another limitation. Many patients had a bad experience during hospitalization and declined to come back for follow-up; underestimating the PTSD rate in COVID-19 survivors should be considered. We recruited control group from hospital staff who had no history of flu-like symptoms, cough, dyspnea, or confirmed COVID-19 diagnosis. Due to the occupational environment, the mental health of the control group is not the same as the general population, especially during the pandemic. Therefore, the long-term impact of COVID-19 on mental health may be even more prominent.
Conclusion
Many of the COVID-19 survivors may experience anxiety, fatigue, and PTSD. Pulmonary function might be impaired in some survivors. These post-recovery complications are noted up to 6 months after discharge. Further follow-up studies should be conducted to investigate the long-term complications.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- COVID-19:
-
Coronavirus disease 2019
- HIS:
-
Hospital information system
- PTSD:
-
Post-traumatic stress disorder
- CT:
-
Computed tomography
- PFT:
-
Pulmonary function test
- TDI:
-
Tissue doppler imaging
- ECG:
-
Electrocardiogram
- LVEDD:
-
Left ventricular end-diastolic diameter
- LVESD:
-
Left ventricular end-systolic diameter
- SARS-CoV-2:
-
Severe acute respiratory syndrome coronavirus 2
- RT-PCR:
-
Real-time reverse transcriptase polymerase-chain-reaction
- BFI:
-
Brief fatigue inventory
- PCL:
-
Post-traumatic stress disorder checklist
- SF-36:
-
36-Item short-form survey
- PCL-C:
-
Post-traumatic stress disorder checklist for civilians
- DSM-IV:
-
Diagnostic and statistical manual of mental disorders
- HAMA:
-
Hamilton anxiety scale
- FEV1:
-
Forced expiratory volume in the first second
- FVC:
-
Forced vital capacity
- FEF25-75%:
-
Forced mid-expiratory flow
- PEF:
-
Peak expiratory flow
- CPK-MB:
-
Creatine kinase myocardial band
- CRP:
-
C-reactive protein
- ESR:
-
Erythrocyte sedimentation rate
- CBC:
-
Complete blood count
- IQR:
-
Interquartile range
- BMI:
-
Body mass index
- AST:
-
Aspartate transaminase
- HDL:
-
High-density lipoprotein
- LDL:
-
Low-density lipoprotein
- TSH:
-
Thyroid stimulating hormone
- FBS:
-
Fasting blood sugar
- HbA1C:
-
Hemoglobin A1C
- ICU:
-
Intensive care unit
- LDH:
-
Lactate dehydrogenase
- HRQoL:
-
Health related quality of life
- GGO:
-
Ground-glass opacities
- LVEF:
-
Left ventricle ejection fraction
- GLS:
-
Global longitudinal strain
- MERS:
-
Middle East respiratory syndrome
- COPD:
-
Chronic obstructive pulmonary disease
References
Health OW (2021) World Health Organization. Accessed 13 Dec 2021
Yomogida K, Zhu S, Rubino F, Figueroa W, Balanji N, Holman E (2021) Post-acute sequelae of SARS-CoV-2 infection among adults aged ≥ 18 years—Long Beach, California, April 1–December 10, 2020. Morb Mortal Wkly Rep 70:1274
Daher A, Balfanz P, Cornelissen C, Müller A, Bergs I, Marx N, Müller-Wieland D, Hartmann B, Dreher M, Müller T (2020) Follow up of patients with severe coronavirus disease 2019 (COVID-19): pulmonary and extrapulmonary disease sequelae. Respir Med 174:106197
Zhao Y-m, Shang Y-m, Song W-b, Li Q-q, Xie H, Xu Q-f, Jia J-l, Li L-m, Mao H-l, Zhou X-m (2020) Follow-up study of the pulmonary function and related physiological characteristics of COVID-19 survivors three months after recovery. EClinicalMedicine 25:100463
Arnold DT, Hamilton FW, Milne A, Morley AJ, Viner J, Attwood M, Noel A, Gunning S, Hatrick J, Hamilton S (2021) Patient outcomes after hospitalisation with COVID-19 and implications for follow-up: results from a prospective UK cohort. Thorax 76:399–401
Tu Y, Zhang Y, Li Y, Zhao Q, Bi Y, Lu X, Kong Y, Wang L, Lu Z, Hu L (2021) Post-traumatic stress symptoms in COVID-19 survivors: a self-report and brain imaging follow-up study. Mol Psychiatry 26:7475–7480
van den Heuvel F, Vos J, van Bakel B, Duijnhouwer A, van Dijk A, Dimitriu-Leen A, Koopmans P, de Mast Q, van de Veerdonk F, Bosch F (2021) Comparison between myocardial function assessed by echocardiography during hospitalization for COVID-19 and at 4 months follow-up. Int J Cardiovasc Imaging 37:3459–3467
Radvan M, Kamenik M, Koc L, Bartecku E, Sykorova L, Kala P, COSUBR, (2021) Echocardiography and ECG monitoring not very beneficial in COVID-19 follow-up even in long haulers. Eur Heart J 42(ehab724):2729
Willi S, Lüthold R, Hunt A, Hänggi NV, Sejdiu D, Scaff C, Bender N, Staub K, Schlagenhauf P (2021) COVID-19 sequelae in adults aged less than 50 years: a systematic review. Travel Med Infect Dis 40:101995
Chen Y-W, Camp PG, Coxson HO, Road JD, Guenette JA, Hunt MA, Reid WD (2018) A comparison of pain, fatigue, dyspnea and their impact on quality of life in pulmonary rehabilitation participants with chronic obstructive pulmonary disease. COPD 15:65–72
Hartley TA, Sarkisian K, Violanti JM, Andrew ME, Burchfiel CM (2013) PTSD symptoms among police officers: associations with frequency, recency, and types of traumatic events. Int J Emerg Ment Health 15:241
Maier W, Buller R, Philipp M, Heuser I (1988) The Hamilton Anxiety Scale: reliability, validity and sensitivity to change in anxiety and depressive disorders. J Affect Disord 14:61–68
Framework IC (1992) The MOS 36-item short-form health survey (SF-36). Med Care 30:473–483
Quanjer PH, Stanojevic S, Cole TJ, Baur X, Hall GL, Culver BH, Enright PL, Hankinson JL, Ip MS, Zheng J (2012) Multi-ethnic reference values for spirometry for the 3–95-yr age range: the global lung function 2012 equations. Eur Respir Soc 1324–43
Moss J, Roberts MB, Shea L, Jones CW, Kilgannon H, Edmondson DE, Trzeciak S, Roberts BW (2019) Healthcare provider compassion is associated with lower PTSD symptoms among patients with life-threatening medical emergencies: a prospective cohort study. Intensive Care Med 45:815–822
Salem AM, Al Khathlan N, Alharbi AF, Alghamdi T, AlDuilej S, Alghamdi M, Alfudhaili M, Alsunni A, Yar T, Latif R (2021) The long-term impact of COVID-19 pneumonia on the pulmonary function of survivors. Int J Gen Med 14:3271
Zhang S, Bai W, Yue J, Qin L, Zhang C, Xu S, Liu X, Ni W, Xie M (2021) Eight months follow-up study on pulmonary function, lung radiographic, and related physiological characteristics in COVID-19 survivors. Sci Rep 11:1–13
Torres-Castro R, Vasconcello-Castillo L, Alsina-Restoy X, Solís-Navarro L, Burgos F, Puppo H, Vilaro J (2021) Respiratory function in patients post-infection by COVID-19: a systematic review and meta-analysis. Pulmonology 27:328–337
Liu T, Wu D, Yan W, Wang X, Zhang X, Ma K, Chen H, Zeng Z, Qin Y, Wang H (2022) Twelve-month systemic consequences of coronavirus disease 2019 (COVID-19) in patients discharged from hospital: a prospective cohort study in Wuhan, China. Clin Infect Dis 74:1953–1965
Group WCftCS (2021) Four-month clinical status of a cohort of patients after hospitalization for COVID-19. JAMA 325:1525–1534
Acknowledgements
The authors would like to appreciate the Clinical Research Development Units of Kamali and Rajaee Hospitals in Alborz University of Medical Science.
Funding
None.
Author information
Authors and Affiliations
Contributions
NSH and HR came up with the idea, and HR, MHMB, and FB designed the study. NSH, MHMB, FZ, ED, MS, ZK, MN, AZ, HDH, HK, ZKH, MD, AS, MRK, and AB collected the data. HR and NSH analyzed the data. All authors have drafted the paper. Also, all authors critically revised the manuscript for important intellectual content and gave final approval for the version to be published.
Corresponding authors
Ethics declarations
Ethical approval and consent to participate
The ethics committee of Alborz University of Medical Sciences approved the study protocol . The written informed consent was obtained from all the participants.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Shafiabadi Hassani, N., MozafaryBazargany, M., Zohrian, F. et al. Midterm follow-up of healthy young adults with moderate to severe COVID-19: pulmonary and extrapulmonary disease sequelae. Egypt J Bronchol 17, 35 (2023). https://doi.org/10.1186/s43168-023-00207-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43168-023-00207-4