
Abstract
Aims/hypothesis
There are limited data comparing dipeptidyl peptidase-4 (DPP-4) inhibitors directly. We compared the safety and efficacy of vildagliptin and sitagliptin in patients with type 2 diabetes and severe renal impairment (RI).
Methods
This study was a parallel-arm, randomised, multicentre, double-blind, 24 week study conducted in 87 centres across Brazil and the USA. Patients with type 2 diabetes, either drug naive or treated with any glucose-lowering agents, who had inadequate glycaemic control (HbA1c 6.5–10.0% [48–86 mmol/mol]) and an estimated GFR <30 ml min−1 [1.73 m]−2 were randomised (via interactive voice response technology) to vildagliptin 50 mg once daily or sitagliptin 25 mg once daily. These doses are recommended in this patient population and considered maximally effective. Participants, investigators and the sponsor were blinded to group assignment. Efficacy endpoints included change in HbA1c and fasting plasma glucose (FPG) at all visits and the primary safety endpoint was assessment of treatment-emergent adverse events.
Results
In total, 148 patients were randomised, 83 to vildagliptin and 65 to sitagliptin. All patients were analysed. After 24 weeks, the adjusted mean change in HbA1c was −0.54% (5.9 mmol/mol) from a baseline of 7.52% (59 mmol/mol) with vildagliptin and −0.56% (6.1 mmol/mol) from a baseline of 7.80% (62 mmol/mol) with sitagliptin (p = 0.874). FPG decreased by 0.47 ± 0.37 mmol/l with vildagliptin and increased by 0.16 ± 0.43 mmol/l with sitagliptin (p = 0.185). Both treatments were well tolerated with overall similar safety profiles.
Conclusions/interpretation
At their recommended doses for severe RI, vildagliptin (50 mg once daily) compared with sitagliptin (25 mg once daily) demonstrated similar efficacy and both drugs were well tolerated. This study provides further support for the use of DPP-4 inhibitors in patients with severe RI.
Trial registration: ClinicalTrials.gov NCT00616811 (completed)
Funding: This study was planned and conducted by Novartis
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Renal impairment (RI) is very common in patients with type 2 diabetes [1], as diabetes is the leading cause of kidney failure and end-stage renal disease (ESRD) [2]. In particular, the management of patients with type 2 diabetes and severe RI poses a vast challenge, as therapeutic options are limited because of contraindications and/or increased risk of hypoglycaemia in this patient population [3, 4]. Hypoglycaemia is more common in patients with RI because of decreased renal gluconeogenesis [5], and in particular, overexposure to insulin secretagogues or exogenous insulin is often associated with an increased risk of hypoglycaemia [6].
Dipeptidyl peptidase-4 (DPP-4) inhibitors such as vildagliptin and sitagliptin are generally well tolerated, and are approved for use in patients with severe RI. Owing to their glucose-dependent mechanism of action, they are generally associated with a low risk of hypoglycaemia and are an attractive treatment option for these difficult-to-treat patients [7]. All DPP-4 inhibitors improve glycaemic control by extending the meal-induced increases in glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP) for several hours by slowing the rate of inactivation of these peptides. There are differences in the mechanisms of action of DPP-4 inhibitors, in particular their catalytic binding kinetics [8], which may translate into clinical differences. For example, vildagliptin blocks DPP-4 through substrate-like binding to the active site of the enzyme for an extended time [8]. By contrast, sitagliptin exerts its effect through competitive enzyme inhibition [8, 9]. Only vildagliptin has been shown to block the inactivation of GLP-1 and GIP between meals and overnight [8, 9]. However, there are limited data comparing the various agents directly.
We report here the efficacy and safety/tolerability of vildagliptin compared with sitagliptin in patients with type 2 diabetes and severe RI, with a focus on glycaemic control relative to hypoglycaemic risk.
Methods
Study design
This study was a multicentre, randomised, parallel-arm, double-blind, 24 week, clinical trial of vildagliptin (50 mg once daily) and sitagliptin (25 mg once daily) in patients with type 2 diabetes and severe RI (ClinicalTrials.gov registration no. NCT00616811). The primary objective of the study was to evaluate the safety and tolerability of both treatments in this patient population. The study was conducted between January 2008 and October 2010. Participants were recruited as outpatients in 87 centres across Brazil (6) and the USA (81).
Key inclusion criteria for this study included age 18–85 years, BMI 18–42 kg/m2, HbA1c 6.5–10.0% (48–86 mmol/mol), type 2 diabetes either untreated (no glucose-lowering medication in the past 8 weeks) or treated with a stable dose of sulfonylurea, thiazolidinedione, meglitinide or insulin, as monotherapy or in combination (for at least 4 weeks), and severe RI (estimated GFR [eGFR] by the Modification of Diet in Renal Disease [MDRD] formula <30 ml min−1 [1.73 m]−2). Patients were excluded if they had a history of renal transplant, significant cardiovascular history within 6 months, liver disease, abnormal liver function tests (alanine transaminase [ALT] >2× upper limit of normal [ULN], aspartate transaminase >2× ULN or total bilirubin >2× ULN and/or direct bilirubin >ULN) or any treatment that is contraindicated (i.e. metformin) in the severe RI population. The initial protocol excluded patients undergoing any dialysis, but it was subsequently amended to remove this restriction to facilitate recruitment.
Patients continued their initial background treatment throughout the study. After a 2 week, single-blind, placebo run-in period, eligible patients were randomised using interactive voice response technology (IVRS) to receive either vildagliptin (50 mg once daily) or sitagliptin (25 mg once daily) for 24 weeks in addition to continuing their background treatment, if applicable. IVRS assigned a randomisation number to the patient, which was used to link the patient to a treatment arm and to specify unique medication numbers for the first package of study drug to be dispensed to the patient.
This clinical trial targeted enrolling a population of approximately 33% elderly women as a patient population considered more vulnerable. Therefore, patient randomisation was stratified by a combined age and sex factor (≥65 year old women versus others) and background glucose-lowering medication. Randomisation procedures were performed by the investigator or his/her delegate. The study drugs were supplied by Novartis as tablets, and patients were instructed to take one pill a day orally before breakfast. Patients, investigator staff, persons performing the assessments and data analysts remained blinded to the identity of the treatment from the time of randomisation until database lock. Both medications were used at the doses recommended in the label for patients with severe RI. Rescue medication (insulin addition or intensification) could be administered on or after week 4 if fasting plasma glucose (FPG) was >15 mmol/l, after week 8 if FPG >13.3 mmol/l and after week 16 if FPG >12.2 mmol/l.
Outcomes
HbA1c and FPG were measured at all visits. An analysis of responder rate was also performed to assess the percentage of patients achieving HbA1c ≤6.5% (48 mmol/mol) and <7.0% (53 mmol/mol). HbA1c and routine biochemistry laboratory assessments were performed by a central laboratory (Covance, Indianapolis, IN, USA).
For assessment of safety and tolerability all treatment-emergent adverse events (AEs) were recorded and evaluated by the investigator for severity and possible relationship to study medication. Hypoglycaemia was defined as symptoms suggestive of low blood glucose confirmed by a self-monitored blood glucose measurement <3.1 mmol/l plasma glucose equivalent.
Statistical analyses
A total of 150 patients (in a 1.5:1 allocation ratio to vildagliptin 50 mg once daily and sitagliptin 25 mg once daily) were planned to be randomised. Assuming an approximate 35% dropout rate (i.e. patients who did not complete the 24 weeks of treatment), 90 patients randomised to the vildagliptin group would provide approximately 58 patients who completed 24 weeks of treatment. A sample size of 58 patients who completed the 24 week study in the vildagliptin treatment group would have 83% power to observe at least one AE with an underlying rate of 3%. For efficacy variables (HbA1c and FPG), the adjusted mean changes from baseline to endpoint (with last observation carried forward) were compared between treatments using an ANCOVA model, with the baseline value as the covariate, and background therapy, pooled centre and treatment as the classification variables. In addition, the time course of HbA1c values and change from baseline by treatment were tabulated and plotted. Efficacy data were censored at the start of rescue medication. The values presented are means ± SE unless otherwise specified. The safety data were summarised descriptively by treatment. Safety analyses were performed on all collected data regardless of rescue medication.
Ethics and good clinical practice
The study was conducted in accordance with the Helsinki Declaration of 1975, as revised in 2000 and 2008, and the International Conference on Harmonization/Good Clinical Practice guidelines. The study protocol was approved by an independent ethics committee/institutional review board at each site and all patients provided written informed consent.
Results
Patient disposition and patient demographic/clinical characteristics
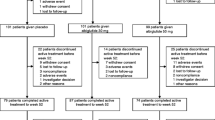
A total of 148 patients with type 2 diabetes and severe RI were randomised, 83 patients to vildagliptin (50 mg once daily) and 65 patients to sitagliptin (25 mg once daily), in addition to their stable background glucose-lowering medication. Of the 148 randomised patients, 117 patients completed the study, 64 (77.1%) in the vildagliptin group and 53 (81.5%) in the sitagliptin group, with the most common reasons for discontinuation being withdrawal of consent (vildagliptin 12.0%, sitagliptin 4.6%) and AEs (vildagliptin 4.8%, sitagliptin 6.2%) (Fig. 1). The recruited population with severe RI also included a limited number of patients with ESRD on haemodialysis (six patients in each treatment group).

Flow diagram of patient disposition. aMore than one reason for discontinuing
Table 1 summarises the demographic and clinical characteristics of the patients in the randomised population as well as baseline glucose-lowering medication. There were no clinically meaningful differences between groups in the baseline characteristics. Forty-six (31.1%) patients were elderly women (≥65 years). Mean eGFR (MDRD) was 19.7 ml−1 min [1.73 m]−2 in the vildagliptin group and 20.4 ml min−1 [1.73 m]−2 in the sitagliptin group. Patients (48% men/52% women) had a mean age of 66.8 years (with nearly two-thirds ≥65 years), mean BMI of 33.2 kg/m2 (with more than two-thirds ≥30 kg/m2) and longstanding type 2 diabetes (mean disease duration 19.2 years). Nearly two-thirds of the patients were white, more than 20% were black and about 12% were Hispanic/Latino. Before entering the study, almost all patients (97.3%) were treated with one or more glucose-lowering agents. About 80% of patients received insulin as either monotherapy or combination therapy, at mean doses of 53 U/day in the vildagliptin group and 60 U/day in the sitagliptin group. Mean HbA1c was 7.5% (58 mmol/mol) in the vildagliptin group vs 7.8% (62 mmol/mol) in the sitagliptin group and mean FPG was 8.1 and 7.7 mmol/l, respectively.
Patients had concomitant medical conditions expected in patients with type 2 diabetes and severe RI. Hypertension was reported in more than 95%, dyslipidaemia in about 90% and cardiac disorders in nearly 60% of the randomised patients. Nearly all the patients received antihypertensive (95%) and lipid-lowering (88%) medications and more than 60% were taking platelet aggregation inhibitors.
Glycaemic control and hypoglycaemia
The adjusted mean changes in HbA1c and FPG during the 24 week treatment period as well as the percentage of patients achieving a target HbA1c ≤6.5% (48 mmol/mol) are represented in Fig. 2. The adjusted mean change in HbA1c was −0.54% ± 0.12% (5.9 ± 1.3 mmol/mol) from a baseline of 7.52% (59 mmol/mol) in the vildagliptin group and −0.56% ± 0.13% (6.1 ± 1.4 mmol/mol) from a baseline of 7.80% (62 mmol/mol) in the sitagliptin group (p = 0.874 for between-group difference; Fig. 2a). A reduction in FPG of 0.47 ± 0.37 mmol/l was seen with vildagliptin, while a slight increase of 0.16 ± 0.43 mmol/l was found with sitagliptin. This difference did not reach statistical significance given the relatively small cohorts (p = 0.185 for between-group difference; Fig. 2b). The percentage of patients achieving a target HbA1c ≤7.0% (53 mmol/mol) was similar in both treatment groups (39% vs 40%); however, the proportion of patients achieving a target HbA1c ≤6.5% (48 mmol/mol) in the vildagliptin group was twice that in the sitagliptin group (29.0% vs 14.3%; p = 0.050; Fig. 2c). Even though there was a trend towards lower FPG levels in the vildagliptin group, the incidence of hypoglycaemia was similar between the two treatment groups (16% vs 15%). Furthermore, as depicted in Table 2, several AEs probably related to hypoglycaemia were reported less frequently in the vildagliptin group than the sitagliptin group (33% vs 51%). This difference was primarily driven by AEs of hyperhidrosis, tremor and asthaenia, as well as asymptomatic low blood glucose levels.

(a) Adjusted mean (SE) change in HbA1c from baseline with vildagliptin 50 mg once daily (n = 78) or sitagliptin 25 mg once daily (n = 62), p = 0.874. (b) Adjusted mean (SE) change in FPG from baseline with vildagliptin 50 mg once daily (n = 79) or sitagliptin 25 mg once daily (n = 62), p = 0.185. (c) Percentage of patients achieving HbA1c ≤6.5% and ≤7.0% with vildagliptin 50 mg once daily (n = 69) or sitagliptin 25 mg once daily n = 56), p = 0.050. Black bars, vildagliptin 50 mg once daily; white bars, sitagliptin 25 mg once daily. To convert values for HbA1c in DCCT % into mmol/mol, subtract 2.15 and multiply by 10.929
Overall safety and tolerability
There were no important differences in the overall AE profiles between vildagliptin and sitagliptin. The incidence of AEs (82% vs 86%), serious AEs (24% vs 23%) and discontinuations due to AEs (7% vs 9%) were comparable for vildagliptin and sitagliptin. Deaths were reported in two patients in each group (cardiac arrest and septic shock in the vildagliptin group, and acute pulmonary oedema and asphyxia in the sitagliptin group). Infections and infestations (vildagliptin 35% vs sitagliptin 39%), skin and subcutaneous tissue disorders (25% vs 28%), musculoskeletal and connective tissue disorders (22% vs 23%), cardiac disorders (13% vs 15%), hepatobiliary disorders (0.0% vs 2%) and pancreatitis (0% in both groups) were reported with similar frequencies in both groups. The most commonly reported AE was peripheral oedema, which occurred at a similar frequency in the vildagliptin (23%) and sitagliptin (25%) groups. No deterioration of renal function was observed with either vildagliptin or sitagliptin. Two patients on sitagliptin had ALT elevations (one patient with ALT >3× ULN in the context of a gastritis, one asymptomatic with ALT >5× ULN); both events resolved on treatment. There were no such liver enzyme elevations on vildagliptin. While a limited number of patients with ESRD on haemodialysis were included in the study (n = 6 in each group), the safety data did not indicate that these patients receiving vildagliptin or sitagliptin were at an increased risk compared with the overall population with RI.
Discussion
The study presented here is the first to directly compare efficacy and safety/tolerability of two DPP-4 inhibitors, namely vildagliptin and sitagliptin, in patients with type 2 diabetes and severe RI. The overall HbA1c lowering effect was similar for both drugs and both drugs were well tolerated.
Both drugs in this study were used at their expected maximal effective and recommended doses (in accordance with product labelling) for patients with severe RI. Vildagliptin is mostly hydrolysed to inactive metabolites, with approximately 20% being excreted unchanged [10]. In patients with severe RI, a 50 mg once daily dose of vildagliptin provides full efficacy, as slower elimination effectively doubles the period of time it prevents GLP-1 and GIP inactivation [10, 11]. The HbA1c reductions seen with vildagliptin 50 mg once daily in patients with severe RI were similar to the reductions observed with vildagliptin 50 mg twice daily in patients with preserved renal function [12], and also consistent with HbA1c reductions initially shown in a large, placebo-controlled trial in 515 patients with type 2 diabetes and moderate or severe RI [11]. As sitagliptin is essentially excreted unchanged by the kidney (80% is excreted as the unchanged compound with only a small fraction being metabolised) and peak plasma concentration (C max) increases approximately fourfold in patients with severe RI, the expected maximal effective dose and the dose recommended on the label in patients with severe RI for sitagliptin is 25 mg once daily [13–16].
The comparative efficacy of 50 mg vildagliptin and 25 mg sitagliptin cannot be determined from this study with certainty as it was not powered to assess relatively small differences in efficacy. In the current study, 80% of patients were on insulin treatment, which likely blunts any differences associated with extending the effects of GLP-1 with vildagliptin during the overnight period. Still, the numerical reduction in FPG with vildagliptin and the slight increase in FPG with sitagliptin are consistent with an effect of vildagliptin during the overnight period. A limitation of the study is that no postprandial blood glucose profiles were obtained. However, studies comparing vildagliptin and sitagliptin in patients with preserved renal function did not find relevant differences in postprandial glucose excursions [17, 18]. Therefore, it is unlikely that this would be the case in our study in patients with RI. The percentage of patients achieving an HbA1c target of ≤6.5% (48 mmol/mol) was higher in the vildagliptin group than the sitagliptin group. This difference is unlikely to reflect a true difference in efficacy between the drugs, and may be a consequence of the slightly lower baseline HbA1c level in the vildagliptin group. Interestingly, this higher responder rate with vildagliptin was not associated with an increased risk of hypoglycaemia with vildagliptin. Overall, the nearly identical drops in HbA1c in our study indicate that the clinical efficacy of both DPP-4 inhibitors is similar in spite of the differences discussed above.
Both drugs were well tolerated. The incidence of hypoglycaemia was similar between the two treatment groups (16% vs 15%). These incidences are low given the vulnerable patient population and that the majority of patients were on insulin treatment. In a study with a similar design, the rates of hypoglycaemia in vildagliptin-treated and placebo-treated patients were of similar magnitude as in our study [11]. The longer extension of the meal-induced increase in GLP-1 and GIP with vildagliptin was not associated with a safety concern in the present study. Of interest, in a prior study in which vildagliptin was dosed at either 50 mg once daily or 50 mg twice daily (i.e. double the recommended dose on the global label) in patients with ESRD, both dosing regimens were well tolerated [19]. Thus, this and other clinical trials demonstrated a good safety and tolerability profile of the entire DPP-4 inhibitor class in populations with severe RI, irrespective of the degree of renal excretion or catalytic binding kinetics [7, 11, 16, 20–24].
In summary, this study demonstrates that vildagliptin 50 mg once daily and sitagliptin 25 mg once daily have similar efficacy and safety profiles in patients with severe RI, supporting the use of DPP-4 inhibitors in patients with severe RI.
Abbreviations
- AE:
-
Adverse event
- ALT:
-
Alanine transaminase
- DPP-4:
-
Dipeptidyl peptidase-4
- eGFR:
-
Estimated GFR
- ESRD:
-
End-stage renal disease
- FPG:
-
Fasting plasma glucose
- GIP:
-
Glucose-dependent insulinotropic polypeptide
- GLP-1:
-
Glucagon-like peptide-1
- IVRS:
-
Interactive voice response technology
- MDRD:
-
Modification of diet in renal disease
- RI:
-
Renal impairment
- ULN:
-
Upper limit of normal
References
de Boer IH, Rue TC, Hall YN, Heagerty PJ, Weiss NS, Himmelfarb J (2011) Temporal trends in the prevalence of diabetic kidney disease in the United States. JAMA 305:2532–2539
Villar E, Zaoui P (2010) Diabetes and chronic kidney disease: lessons from renal epidemiology. Nephrol Ther 6:585–590
Lubowsky ND, Siegel R, Pittas AG (2007) Management of glycemia in patients with diabetes mellitus and CKD. Am J Kidney Dis 50:865–879
Ritz E (2011) Limitations and future treatment options in type 2 diabetes with renal impairment. Diabetes Care 34(Suppl 2):S330–S334
Gerich JE, Meyer C, Woerle HJ, Stumvoll M (2001) Renal gluconeogenesis: its importance in human glucose homeostasis. Diabetes Care 24:382–391
Arem R (1989) Hypoglycemia associated with renal failure. Endocrinol Metab Clin N Am 18:103–121
Scheen AJ (2015) Pharmacokinetics and clinical use of incretin-based therapies in patients with chronic kidney disease and type 2 diabetes. Clin Pharmacokinet 54:1–21
Ahrén B, Schweizer A, Dejager S, Villhauer EB, Dunning BE, Foley JE (2011) Mechanisms of action of the dipeptidyl peptidase-4 inhibitor vildagliptin in humans. Diabetes Obes Metab 13:775–783
Davis JA, Singh S, Sethi S et al (2010) Nature of action of sitagliptin, the dipeptidyl peptidase-IV inhibitor in diabetic animals. Indian J Pharm 42:229–233
Dejager S, Schweizer A (2012) Incretin therapies in the management of patients with type 2 diabetes mellitus and renal impairment. Hosp Pract 40:7–21
Lukashevich V, Schweizer A, Shao Q, Groop PH, Kothny W (2011) Safety and efficacy of vildagliptin versus placebo in patients with type 2 diabetes and moderate or severe renal impairment: a prospective 24-week randomised placebo-controlled trial. Diabetes Obes Metab 13:947–954
Keating GM (2014) Vildagliptin: a review of its use in type 2 diabetes mellitus. Drugs 74:587–610
Herman GA, Stevens C, Van Dyck K et al (2005) Pharmacokinetics and pharmacodynamics of sitagliptin, an inhibitor of dipeptidyl peptidase-IV, in healthy subjects: results from two randomized, double-blind, placebo-controlled studies with single oral doses. Clin Pharmacol Ther 78:675–688
Vincent SH, Reed JR, Bergman AJ et al (2007) Metabolism and excretion of the dipeptidyl peptidase 4 inhibitor [14C]sitagliptin in humans. Drug Metab Dispos 35:533–538
Bergman AJ, Cote J, Yi B et al (2007) Effect of renal insufficiency on the pharmacokinetics of sitagliptin, a dipeptidyl peptidase-4 inhibitor. Diabetes Care 30:1862–1864
Chan JC, Scott R, Arjona Ferreira JC et al (2008) Safety and efficacy of sitagliptin in patients with type 2 diabetes and chronic renal insufficiency. Diabetes Obes Metab 10:545–555
Marfella R, Barbieri M, Grella R, Rizzo MR, Nicoletti GF, Paolisso G (2010) Effects of vildagliptin twice daily vs sitagliptin once daily on 24-hour acute glucose fluctuations. J Diabetes Complications 24:79–83
Rizzo MR, Barbieri M, Marfella R, Paolisso G (2012) Reduction of oxidative stress and inflammation by blunting daily acute glucose fluctuations in patients with type 2 diabetes: role of dipeptidyl peptidase-IV inhibition. Diabetes Care 35:2076–2082
Ito M, Abe M, Okada K et al (2011) The dipeptidyl peptidase-4 [DPP-4] inhibitor vildagliptin improves glycemic control in type 2 diabetic patients undergoing hemodialysis. Endocr J 58:979–987
Kothny W, Shao Q, Groop PH, Lukashevich V (2012) One-year safety, tolerability and efficacy of vildagliptin in patients with type 2 diabetes and moderate or severe renal impairment. Diabetes Obes Metab 14:1032–1039
Ligueros-Saylan M, Foley JE, Schweizer A, Couturier A, Kothny W (2010) An assessment of adverse effects of vildagliptin versus comparators on the liver, the pancreas, the immune system, the skin and in patients with impaired renal function from a large pooled database of phase II and III clinical trials. Diabetes Obes Metab 12:495–509
Nowicki M, Rychlik I, Haller H et al (2011) Saxagliptin improves glycaemic control and is well tolerated in patients with type 2 diabetes mellitus and renal impairment. Diabetes Obes Metab 13:523–532
Nowicki M, Rychlik I, Haller H et al (2011) Long-term treatment with the dipeptidyl peptidase-4 inhibitor saxagliptin in patients with type 2 diabetes mellitus and renal impairment: a randomised controlled 52-week efficacy and safety study. Int J Clin Pract 65:1230–1239
McGill JB, Sloan L, Newman J et al (2013) Long-term efficacy and safety of linagliptin in patients with type 2 diabetes and severe renal impairment: a 1-year, randomised, double-blind, placebo-controlled study. Diabetes Care 36:237–244
Acknowledgements
The authors gratefully acknowledge all the investigators, staff and patients at the participating sites and A. Dandu (Novartis Healthcare Pvt. Ltd.) for technical help. A list of investigators is provided in the electronic supplementary material (ESM, list of participating investigators). This study was previously presented in poster form at the European Association for the Study of Diabetes 50th Annual Meeting, September 15–19, 2014, Vienna, Austria.
Funding
This study was funded by Novartis Pharma AG, Basel, Switzerland. The sponsor was involved in study design, and collection, analysis and interpretation of data.
Duality of interest
WK, VL, JEF and AS are employed by Novartis and own shares. MSR is involved in clinical trials for Novartis, Sanofi, Merck, Boehringer Ingelheim, AbbVie and Eli Lilly. No other potential conflicts of interest relevant to this article were reported.
Contribution statement
WK, VL, JEF and AS wrote the manuscript and researched data. MSR reviewed and edited the manuscript and researched data, and also participated in the study as an investigator. All authors read and approved the final manuscript for submission. WK is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
ESM List of participating investigators
(PDF 12 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Kothny, W., Lukashevich, V., Foley, J.E. et al. Comparison of vildagliptin and sitagliptin in patients with type 2 diabetes and severe renal impairment: a randomised clinical trial. Diabetologia 58, 2020–2026 (2015). https://doi.org/10.1007/s00125-015-3655-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00125-015-3655-z