
Abstract
Aims/hypothesis
Approximately 10% of total healthcare budgets worldwide are spent on treating diabetes and its complications, and budgets are increasing globally because of ageing populations and more expensive second-line medications. The aims of the study were to estimate the within-trial and lifetime cost-effectiveness of the weight management programme, which achieved 46% remissions of type 2 diabetes at year 1 and 36% at year 2 in the Diabetes Remission Clinical Trial (DiRECT).
Methods
Within-trial analysis assessed costs of the Counterweight-Plus intervention in DiRECT (including training, programme materials, practitioner appointments and low-energy diet), along with glucose-lowering and antihypertensive medications, and all routine healthcare contacts. Lifetime cost per quality-adjusted life-year (QALY) was estimated according to projected durations of remissions, assuming continued relapse rates as seen in year 2 of DiRECT and consequent life expectancy, quality of life and healthcare costs.
Results
Mean total 2 year healthcare costs for the intervention and control groups were £3036 and £2420, respectively: an incremental cost of £616 (95% CI –£45, £1269). Intervention costs (£1411; 95% CI £1308, £1511) were partially offset by lower other healthcare costs (£796; 95% CI £150, £1465), including reduced oral glucose-lowering medications by £231 (95% CI £148, £314). Net remission at 2 years was 32.3% (95% CI 23.5%, 40.3%), and cost per remission achieved was £1907 (lower 95% CI: intervention dominates; upper 95% CI: £4212). Over a lifetime horizon, the intervention was modelled to achieve a mean 0.06 (95% CI 0.04, 0.09) QALY gain for the DiRECT population and mean total lifetime cost savings per participant of £1337 (95% CI £674, £2081), with the intervention becoming cost-saving within 6 years.
Conclusions/interpretation
Incorporating the lifetime healthcare cost savings due to periods of remission from diabetes and its complications, the DiRECT intervention is predicted to be both more effective (QALY gain) and cost-saving in adults with type 2 diabetes compared with standard care. This conclusion appears robust to various less favourable model scenarios, providing strong evidence that resources could be shifted cost-effectively to support achieving remissions with the DiRECT intervention.
Trial registration
ISRCTN03267836

Graphical abstract
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.

Introduction
Type 2 diabetes, until recently considered a permanent and inevitably progressive chronic disease, impacts rates of mortality and morbidity as well as quality of life (QoL). Affecting between 5% and 35% of post-industrial adult populations [1], it presents a major and increasing economic burden, currently accounting for 10% of total healthcare expenditure in the UK [2] and 12.5% in the USA [3]. Management has usually focused on pharmacotherapy, with increasing emphasis in guidelines on earlier prescription of more modern and expensive glucose-lowering, lipid-lowering and antihypertensive drugs, to control blood glucose and reduce the associated complications and elevated cardiovascular risks. Despite these treatments, younger people, in particular, commonly face irreversible declines in health from type 2 diabetes, characterised by chronic pain and multiple disabilities, and life expectancy is reduced substantially [4]. However, remission of type 2 diabetes is now known to be possible [5,6,7]. In the Diabetes Remission Clinical Trial (DiRECT), an integrated diet programme delivered entirely within primary care produced remissions of type 2 diabetes (non-diabetic HbA1c on no glucose-lowering medication) in 46% of participants at 1 year and 36% at 2 years [8, 9].
The DiRECT study, reported in detail elsewhere [8, 10], recruited 298 adults with a diagnosis of diabetes within the past 6 years, BMI 27–45 kg/m2 and HbA1c >48 mmol/mol (6.5%), or >42 mmol/mol (6.0%) if receiving glucose-lowering medication. Half the participants were in practices randomised to receive the Counterweight-Plus weight management programme, and all received usual care under current clinical guidelines. The Counterweight-Plus programme is initiated as ‘total diet replacement’ with a low-energy formula diet (soups and shakes) providing 3452–3569 kJ (825–853 kcal) per day for 12–20 weeks (Counterweight, UK). This is followed by structured food reintroduction for 2–8 weeks and a subsequent longer-term programme of weight loss maintenance. For relapse management, 2–4 week ‘rescue packages’ of the formula diet are provided if >2 kg weight is regained or if diabetes returns. All oral glucose-lowering and antihypertensive medications are suspended on safety grounds at the start of the programme but are reintroduced according to blood glucose and blood pressure measurements taken at each primary care appointment, following clinical guidelines.
Remission of type 2 diabetes has the potential to lead to substantial long-term health gains and cost savings. Decision analytic models are commonly used to extrapolate long-term costs and outcomes from clinical trials, supplementing trial data with other sources of evidence on longer-term disease progression such as diabetes relapse, health-related QoL, mortality and costs [11]. Here we report a lifetime cost-effectiveness analysis of the Counterweight-Plus intervention, based on resource use measured in DiRECT over 2 years, and projected longer-term cost and quality-adjusted life-years (QALYs), assuming a limited duration of diabetes remission.
Methods
A within-trial cost analysis was conducted using the 2 year data from DiRECT, including both the intervention costs and routine healthcare resource use measured during the time course of the study, for all participants (including those who did not complete the trial or who were unsuccessful in achieving remission). Lifetime cost-effectiveness was then estimated by predicting time to relapse (i.e. re-emergence of diabetes, assumed to be permanent thereafter) among those who were in remission at 2 years, applying the mean management costs for type 2 diabetes incurred within the UK National Health Service (NHS), under clinical guidelines which tend to favour older, less expensive medications. An NHS perspective for costing was adopted for both within-trial and lifetime analyses. Costs are presented in 2018 UK prices (£).
Ethics approval
Ethics approval was granted in January 2014 by the West of Scotland Research Ethics Committee 3, with approvals by the NHS health board areas in Scotland and by clinical commissioning groups in Tyneside, UK.
Two year within-trial economic analysis
DiRECT intervention costs over the 2 year trial period included costs for initial training of practitioners (dietitians or nurse practitioners, who each received a total of 16 h face-to-face training from Counterweight-Plus instructors), sachets of low-energy formula diet, practitioner monitoring appointments and the tailored Counterweight-Plus workbooks issued to each participant (Table 1). Costs of the sessions included practitioners’ attendance time and standard Counterweight-Plus materials. The number of sachets issued to each participant and the number and duration of practitioner appointments were collected prospectively throughout the study. Full costs for participant Counterweight-Plus workbooks were applied irrespective of participants’ persistence with the programme, the details of which are described elsewhere [8, 10, 12].
Details of all primary and secondary care visits for each of the participants were obtained directly from the participating general practitioner (GP) practice records. The costs of these were calculated using the recorded duration of contact for each appointment. Medication use was costed based on dose, frequency and start and end dates of individual participants’ medication records in each participating GP practice. Hospitalisation costs were estimated by matching reason for admission and recorded length of stay in DiRECT to the appropriate NHS reference cost (excluding excess bed-days, where length of stay recorded in DiRECT exceeded the national average). Unit costs were obtained from published national sources (Personal Social Service Research Unit [13], NHS reference costs [14], or Information Services Division Scotland [15], and British National Formulary [16]) and have been reported previously [17].
Statistical analysis was conducted based on the intention-to-treat principle. Missing data were minimal, as all resource use data were obtained directly from participating GP practices. Five intervention (3%) and three control (2%) participants relocated with loss to follow-up during the study. Their medication use was assumed to continue as at their last available records, and other healthcare resource use was assumed to be zero after relocation. Twenty intervention (13.4%) and six control (4%) participants had no data available for the 2 year remission outcome. In line with the primary outcome analysis, these participants were assumed not to have achieved remission.
Mean costs were calculated for each group, with clustering-adjusted SEs for each cost item. Incremental cost per remission at 2 years was reported as the difference in the groups’ total 2 year costs, divided by the difference in diabetes remission rates. All analyses were undertaken in Stata/MP, version 14.2 (StataCorp LP, USA), with 95% CIs based on 1000 non-parametric bootstrap iterations.
Long-term projection
Long-term outcomes were projected for each treatment arm in DiRECT. A three-state model (remission, diabetes, death) was constructed. Individuals enter the model with existing diabetes. After 1 year a proportion achieve remission but are subject to relapse in future years. The proportion remaining in remission over time was estimated based on the rate of relapse observed in year 2; however, all participants were assumed to relapse after a given number of years (a maximum period of 10 years of remission in the base case). Life expectancy was calculated for each potential year of remission by applying rates of mortality for people free of diabetes up to the year of relapse and with diabetes thereafter. Along with life expectancy, quality-adjusted life expectancy and healthcare costs were estimated conditional on each potential year of relapse.
Life expectancy was calculated based on rates of mortality in people free of diabetes (N = 2.75 million) and with diabetes (N = 272,597), based on a recent UK study [18] which reported mortality rates by sex and 5 year age bands during the period 2012–2014 in Scotland. Reported life expectancy for men aged 55–59 years was 23.0 and 26.0 years with diabetes and free of diabetes, respectively, and 24.4 and 28.7 for women.
QALYs were calculated by applying standard UK age-dependent health state utility population norms [19]. These were assigned directly to people in remission from diabetes. For people not in remission, including those who had relapsed, these age-dependent health state utilities were reduced using a constant multiplier of 0.925 to reflect a decrement due to diabetes. This was estimated based on the mean population score (0.828) and the regression coefficient for diabetes (−0.0621) in the US Medical Expenditure Panel Survey catalogue of UK EuroQol EQ-5D scores [20]. This estimate was employed rather than being based on data from DiRECT, for reasons discussed below.
The lifetime healthcare costs associated with diabetes were compiled first from the measured costs for the first 2 years of DiRECT, to which were added further costs for ongoing weight management for participants remaining in remission and long-term healthcare costs associated with diabetes. Long-term diabetes-related healthcare costs were assumed to increase linearly with duration of diabetes (i.e. time since relapse), over 15 years, from £1250 in the year of diagnosis to £3117 after 15 years, based on a UK cost of diabetes study [2, 21]. No further increase in long-term healthcare costs beyond 15 years was applied. Long-term healthcare costs due to diabetes were applied to the proportion of people projected to be in the diabetes state each year after year 2.
We compared the incremental cost and QALYs for the intervention and control arms over the 2 year follow-up of DiRECT and over a lifetime horizon. Sensitivity analysis was undertaken for the long-term analysis, including exploring the impact of alternative relapse rates and maximum assumed durations of diabetes remission. Probabilistic sensitivity analysis was performed using 1000 bootstrap iterations of the DiRECT data (remission and 2 year costs), and Monte Carlo simulations for other variables (e.g. long-term mortality rates). Model input data are summarised in Table 2; all costs and outcomes beyond year 1 were discounted at the standard UK annual rate of 3.5%.
Results
Within-trial results
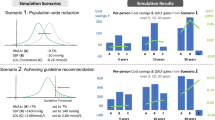
During the first year of the DiRECT intervention, a mean of approximately 500 sachets of low-energy formula diet were issued to each participant, over 80% of the total 2 years’ consumption being consumed during the initial total diet replacement phase (Fig. 1). Each participant received a mean of 23 practitioner visits, the majority of these also during year 1. The cost of formula diet and practice visits together was £1364 (95% CI £1260, £1464) per participant entered over 2 years, and total intervention costs, including amortised clinic set-up costs, amounted to £1411 (95% CI £1308, £1511).

Mean use of low-energy-diet sachets (a) and health practitioner appointments (b) per participant, according to intervention phase. Error bars show 95% CI
The focus and resource need of the Counterweight-Plus programme shifts from weight loss using total diet replacement in the initial 12–20 weeks to long-term weight maintenance, with data currently available for 2 years (Table 1, Fig. 1). Use of formula diet sachets in year 2 was limited to regular maintenance, for those who elected to use them, and for relapse management purposes (when participants regained over 2 kg body weight). Their total use amounted to less than 20% of the year 1 consumption, when they were used for total diet replacement, and decreased over the food reintroduction phase. Similarly, planned practitioner appointments in year 2, for maintenance and relapse management, were approximately 50% fewer than in year 1.
Participants in the intervention group had substantially fewer days on oral glucose-lowering and antihypertensive drugs. Over the 2 years, participants in the intervention group had a mean of 290 days on oral glucose-lowering medications, compared with 910 for those in the control group (difference 620 days; 95% CI 501, 738), and a mean of 381 days on antihypertensive medications, compared with 782 for those in the control group (difference 410 days; 95% CI 258, 537) (Table 3). The intervention group had fewer GP visits related to diabetes (difference 0.6 visits; 95% CI 0.2, 1.0). Other items of resource use were mostly lower in the intervention arm, including fewer hospital days. Lower use of glucose-lowering and antihypertensive medications, combined with fewer healthcare contacts, provided total savings in the intervention arm over 2 years of £796 (95% CI £150, £1465). This cost saving in routine (non-trial) resource use offset 56% of the 2 year intervention costs, leaving a 2 year incremental cost for the intervention of £616 (95% CI –£45, £1269) per participant entered. Given remission rates of 35.6% and 3.4% in the intervention and control arms, respectively, at 2 years, the resulting incremental cost per remission at 2 years was £1907 (lower 95% CI: intervention dominates, i.e. is cost-saving and more effective; upper 95% CI: £4212). Medication cost savings were principally due to lower use of glucose-lowering medicines (approximately 90% of total medication savings) and were divided equally between years 1 and 2. The difference in the total other non-intervention resource use (i.e. healthcare contacts and hospitalisations) in year 1 was negligible [17] and over the 2 years did not reach statistical significance; however, these cost savings were significant in year 2 (£521; 95% CI £12, £1085).
Long-term cost-effectiveness
Across both arms of the trial, 79 participants achieved remission during the 2 year period, including five who did so during year 2. Of 74 participants in remission at year 1, 21 had relapsed by the end of year 2. At this observed annual relapse rate in DiRECT (28%), mean time to relapse would be approximately 3.5 years, with 13% of participants expected to remain in remission beyond 5 years. The resulting mean gain in life expectancy for a person in remission at 1 year is 0.30, and, for all participants entered in DiRECT, 0.13. Discounted QALYs were modelled to be increased by 0.06. Total costs relating to diabetes (other than ongoing intervention costs) were modelled, based on current treatment costs, ranging from approximately £15,000 for people remaining in remission until year 10 to £30,000 for those not in remission after 1 year. After accounting in the model for intervention costs and time to relapse, the intervention generated a £1337 cost saving (95% CI £674, £2081) per participant entered into the programme (Table 4). The intervention therefore dominated standard care and had the probability of being both cost-saving and cost-effective at a threshold of £20,000 per QALY of 1.00.
Follow-up of participants in DiRECT is continuing. As this analysis relies on 2 year data we estimated time to total cost equivalence (or break-even) and explored sensitivity to shorter times to relapse. The model predicted the intervention would become cost-saving overall after a period of 5–6 years under base case assumptions for relapse (Fig. 2). Assuming all people who achieved remission relapsed after a maximum of 3 years, the intervention remained cost-saving due to deferred diabetes (Table 5). Increasing the rate of relapse without modifying the maximum period of remission had a lesser impact on cost savings. The intervention also remained cost-saving when a reduced rate of remission after 1 year was assumed, and with a shorter time horizon for analysis. In these cases, although QALY gains were also reduced, the intervention remained dominant.

Cumulative predicted cost (per participant entered) for DiRECT/Counterweight-Plus intervention and standard care, up to 10 years. Dashed lines indicate financial break-even point
Relapses were more frequent among women than among men in year 2. When the analysis was performed using sex-specific relapse rates, the overall QALY gain and cost were little different, although health gains and cost savings were more concentrated in men.
Assuming no detrimental impact of diabetes on QoL resulted in an increased QALY gain, the result of life expectancy being valued more highly. The model assumed that type 2 diabetes, with a diagnosis at about 55 years of age, and without intervention, would reduce life expectancy by 3.2 years in men and by 5.2 years in women. Reducing mortality rates for people with diabetes by 10% reduces the QALY gains from intervention to approximately 0.05. The intervention remained cost-saving both when excluding other healthcare cost savings in the early period and when substantially lower long-term costs due to diabetes were assumed.
Discussion
It is most unusual to be able to provide a new medical treatment for a major chronic disease which is both health-improving and cost-saving. The DiRECT study has shown that durable remissions of type 2 diabetes to a non-diabetic state can be achieved through an integrated weight management programme, mostly for those achieving weight loss >10 kg, for almost half of all participants. Weight loss >15 kg in the intervention arm led to remissions for 86% at 1 year and 82% at 2 years [9]. The present analysis indicates that the intervention is likely to generate QALY gains and be not only cost-effective but also cost-saving after 5–6 years. Given the rate at which second-line glucose-lowering medication costs have been rising in recent years, cost-saving estimates may be conservative.
Although individuals with remissions are assumed to relapse to diabetes over time, cost savings were modelled to accrue beyond the point of relapse, with a delay in the requirement for more intense resource use due to diabetic complications. We have previously noted that roll-out of the intervention in routine practice may provide for efficiencies that could reduce costs; however, even under trial conditions, set-up costs are a minor component of total intervention costs, and no adjustment was made for such efficiencies in the present analysis.
There were fewer medical appointments for intercurrent medical problems in the DiRECT intervention group and fewer serious adverse events in year 2 [9]. This is in line with improved diabetes control and remissions for many. Better QoL would therefore be expected, and this was borne out by a general pattern of modestly improved EuroQol EQ-5D scores in the intervention group at both 12 and 24 months. [9] However, the mean duration of diabetes at baseline, of 3 years, is too short for the full impact of diabetes and its complications to have already impaired QoL. Therefore, QoL measurements over a 2 year period so early in the disease course cannot be expected to capture the long-term impact of more sustained diabetes remissions. Given that diabetes ultimately carries a major long-term burden for health-related QoL, we calculated QALY losses using a health state utility decrement due to diabetes based on the US Medical Expenditure Panel Survey [20]. Long-term health gains in our analysis are, however, attributable principally to improved life expectancy due to periods of remission, as our model assumed, perhaps conservatively, that over time all individuals in remission would return to the diabetes state by 10 years.
In the analysis of the Scottish Care Information Diabetes Database (SCI-Diabetes), life expectancy was found to be significantly lower in people with type 2 diabetes, irrespective of age group or socioeconomic status (with the exception of men >80 years in the most deprived quintile) [18]. These published Scottish survival rate data, on which estimates of life expectancy losses were based, are somewhat more conservative than the estimates from a large European study [22], which indicated that the years of life lost for people without known vascular disease would be about 5.2 years for men and 6.1 years for women.
An important assumption in our analysis was that remission returned participants to a life expectancy similar to that of the diabetes-free population. However, the benefit in terms of reduced mortality risk was modelled to be temporary, as all individuals in remission were assumed to relapse to diabetes within 10 years, and many were assumed to do so within 5 years. As yet, there are no published data from any country on the future health or life expectancy of people who achieve dietary--weight-loss-induced remissions of type 2 diabetes. Many of the participants in remission from diabetes in DiRECT had HbA1c in the range of ‘prediabetes’ (42–48 mmol/mol [6.0–6.5%]). About 30–40% of the adult population have HbA1c in this range, which is associated with progression to type 2 diabetes for perhaps a fifth, and poorer health outcomes than with lower HbA1c [23,24,25]. The health outcomes for people in this range, which may be considered ‘post-diabetes’, after improving diet and lifestyle, are still unknown: they may be worse or better than those of the general population.
No subgroup effects have been proposed clinically, and we did not seek to do so. Relapse to diabetes in year 2, however, was significantly more likely among women than among men (p= 0.016). The SCI-Diabetes analysis found that women with diabetes lost more years of life compared with men [18]. A very large European study found a similar difference between sexes [22]. When we performed separate analyses for men and women, however, we modelled greater life expectancy gains in men than in women because of the lower rates of relapse in men, though life-year and QALY gains remained statistically significant for both; the intervention was cost-saving in both men and women, and the noted difference in relapse could be due to chance. These results should not imply withholding treatment for women, as they still did very well, but there may be benefit from modifying the intervention in the future to better support maintenance of weight loss and diabetes remission in women.
The present analysis is based on UK data both in terms of the DiRECT trial itself, and other data for costs of diabetes care under the NHS, and observed long-term mortality. Intervention costs in other countries may differ; though, as noted above, more efficient delivery, both in the UK and elsewhere, might be expected once the programme is established in routine practice. The major element of intervention cost is the formula diet, whose acquisition cost might fall in the future through economies of scale. Costs of routine diabetes care under clinical guidelines may be expected to increase with wider and earlier use of newer medications and an increasing duration of disease after younger onset.
A 2019 position statement issued by the joint Association of British Clinical Diabetologists and the Primary Care Diabetes Society [5] reviewed the current evidence for remission of type 2 diabetes, ranging from bariatric surgery, in 1987 [26], to the most recent evidence of dietary and behavioural interventions including DiRECT [9, 27, 28]. It concluded there was ample evidence to support the recommendation of achieving remission through weight loss, but that long-term follow-up was needed given the risk of weight regain. Relapse into diabetes, driven by weight regain, incurs costs from relapse management and from resumption of progressive costs for diabetes and its complications. Though relapse had a bearing on outcomes in our study, even relatively rapid relapse did not alter the conclusion that the low-energy diet intervention was capable of producing long-term health gains without adding long-term costs. The Counterweight-Plus intervention may therefore be expected to be transferable to other diabetes care settings in a similarly cost-effective manner.
Data availability
Once the data collection and planned analyses of DiRECT are complete (expected 2024), anonymised participant level data will be shared on reasonable request. The study protocol and statistical analysis plan may be obtained from the corresponding author.
Abbreviations
- DiRECT:
-
Diabetes Remission Clinical Trial
- GP:
-
General practitioner
- NHS:
-
National Health Service
- QALY:
-
Quality-adjusted life-year
- QoL:
-
Quality of life
- SCI-Diabetes:
-
Scottish Care Information Diabetes Database
References
NCD Risk Factor Collaboration (NCD-RisC) (2016) Worldwide trends in diabetes since 1980: a pooled analysis of 751 population-based studies with 4.4 million participants. Lancet 387(10027):1513–1530. https://doi.org/10.1016/S0140-6736(16)00618-8
Hex N, Bartlett C, Wright D, Taylor M, Varley D (2012) Estimating the current and future costs of type 1 and type 2 diabetes in the UK, including direct health costs and indirect societal and productivity costs. Diabet Med 29(7):855–862. https://doi.org/10.1111/j.1464-5491.2012.03698.x
American Diabetes Association (2018) Economic costs of diabetes in the U.S. in 2017. Diabetes Care 41(5):917–928. https://doi.org/10.2337/dci18-0007
Lascar N, Brown J, Pattison H, Barnett AH, Bailey CJ, Bellary S (2018) Type 2 diabetes in adolescents and young adults. Lancet Diabetes Endocrinol 6(1):69–80. https://doi.org/10.1016/S2213-8587(17)30186-9
Nagi D, Hambling C, Taylor R (2019) Remission of type 2 diabetes: a position statement from the Association of British Clinical Diabetologists (ABCD) and the Primary Care Diabetes Society (PCDS). Br J Diabetes 19:73–76. https://doi.org/10.15277/bjd.2019.221
Sjostrom L, Lindroos AK, Peltonen M et al (2004) Lifestyle, diabetes, and cardiovascular risk factors 10 years after bariatric surgery. N Engl J Med 351(26):2683–2693. https://doi.org/10.1056/NEJMoa035622
Lim EL, Hollingsworth KG, Aribisala BS, Chen MJ, Mathers JC, Taylor R (2011) Reversal of type 2 diabetes: normalisation of beta cell function in association with decreased pancreas and liver triacylglycerol. Diabetologia 54(10):2506–2514. https://doi.org/10.1007/s00125-011-2204-7
Lean ME, Leslie WS, Barnes AC et al (2018) Primary care-led weight management for remission of type 2 diabetes (DiRECT): an open-label, cluster-randomised trial. Lancet 391(10120):541–551. https://doi.org/10.1016/S0140-6736(17)33102-1
Lean MEJ, Leslie WS, Barnes AC et al (2019) Durability of a primary care-led weight-management intervention for remission of type 2 diabetes: 2-year results of the DiRECT open-label, cluster-randomised trial. Lancet Diabetes Endocrinol 7(5):344–355. https://doi.org/10.1016/S2213-8587(19)30068-3
Leslie WS, Ford I, Sattar N et al (2016) The Diabetes Remission Clinical Trial (DiRECT): protocol for a cluster randomised trial. BMC Fam Pract 17:20. https://doi.org/10.1186/s12875-016-0406-2
Briggs AH, Claxton K, Sculpher MJ (2006) Decision modelling for health economic evaluation. Oxford University Press, Oxford
Xin Y, Davies A, McCombie L et al (2019) Within-trial cost and 1-year cost-effectiveness of the DiRECT/Counterweight-Plus weight-management programme to achieve remission of type 2 diabetes. Lancet Diabetes Endocrinol 7(3):169–172. https://doi.org/10.1016/S2213-8587(18)30346-2
Curtis L, Burns A (2018) Unit costs of health and social care 2018. University of Kent, Canterbury
NHS Improvement (2018) Reference costs 2017/18: highlights, analysis and introduction to the data. Available from: https://improvement.nhs.uk/documents/1972/1_-_Reference_costs_201718.pdf. Accessed 1 Aug 2019
Public Health Scotland (2018) Specialty costs. Available from: www.isdscotland.org/Health-Topics/Finance/Costbook/Speciality-Costs/. Accessed 1 Aug 2019
National Institute for Health and Care Excellence (2020) BNF. Available from: https://bnf.nice.org.uk/. Accessed 1 Aug 2019
Xin Y, Davies A, McCombie L et al (2019) Type 2 diabetes remission: economic evaluation of the DiRECT/Counterweight-Plus weight management programme within a primary care randomized controlled trial. Diabet Med 36(8):1003–1012. https://doi.org/10.1111/dme.13981
Walker J, Colhoun H, Livingstone S et al (2018) Type 2 diabetes, socioeconomic status and life expectancy in Scotland (2012–2014): a population-based observational study. Diabetologia 61(1):108–116. https://doi.org/10.1007/s00125-017-4478-x
Ara R, Brazier JE (2010) Populating an economic model with health state utility values: moving toward better practice. Value Health 13(5):509–518. https://doi.org/10.1111/j.1524-4733.2010.00700.x
Sullivan PW, Slejko JF, Sculpher MJ, Ghushchyan V (2011) Catalogue of EQ-5D scores for the United Kingdom. Med Decis Mak 31(6):800–804. https://doi.org/10.1177/0272989X11401031
Roberts S, Craig D, Adler A, McPherson K, Greenhalgh T (2018) Economic evaluation of type 2 diabetes prevention programmes: Markov model of low- and high-intensity lifestyle programmes and metformin in participants with different categories of intermediate hyperglycaemia. BMC Med 16(1):16. https://doi.org/10.1186/s12916-017-0984-4
Rao Kondapally Seshasai S, Kaptoge S, Thompson A et al (2011) Diabetes mellitus, fasting glucose, and risk of cause-specific death. N Engl J Med 364(9):829–841. https://doi.org/10.1056/NEJMoa1008862
US Centers for Disease Control and Prevention (2020) National diabetes statistics report. Available from: https://www.cdc.gov/diabetes/data/statistics/statistics-report.html. Accessed 07 June 2020
Hostalek U (2019) Global epidemiology of prediabetes - present and future perspectives. Clin Diabetes Endocrinol 5:5. https://doi.org/10.1186/s40842-019-0080-0
Mainous AG, Tanner RJ, Baker R, Zayas CE, Harle CA (2014) Prevalence of prediabetes in England from 2003 to 2011: population-based, cross-sectional study. BMJ Open 4(6):e005002. https://doi.org/10.1136/bmjopen-2014-005002
Pories WJ, Caro JF, Flickinger EG, Meelheim HD, Swanson MS (1987) The control of diabetes mellitus (NIDDM) in the morbidly obese with the Greenville gastric bypass. Ann Surg 206(3):316–323. https://doi.org/10.1097/00000658-198709000-00009
Steven S, Hollingsworth KG, Al-Mrabeh A et al (2016) Very low-calorie diet and 6 months of weight stability in type 2 diabetes: pathophysiological changes in responders and nonresponders. Diabetes Care 39(5):808–815. https://doi.org/10.2337/dc15-1942
Look AHEAD Research Group (2014) Eight-year weight losses with an intensive lifestyle intervention: the Look AHEAD study. Obesity (Silver Spring) 22(1):5–13. https://doi.org/10.1002/oby.20662
Acknowledgements
We thank the NHS Primary Care Research Network and North East Commissioning Support for their support and valuable input to the study recruitment. We thank M. McNee, E. Butler, J. Cooney, S.-J. Duffus and P. Stewart, from the University of Glasgow (Glasgow, UK), for providing technical assistance; H. Pilkington, from the Newcastle upon Tyne Hospitals NHS Foundation Trust (Newcastle upon Tyne, UK), for providing research nurse support; and S. Weeden and S. Boyle, from the Robertson Centre for Biostatistics (University of Glasgow, Glasgow, UK), for project and data management. We are grateful to the general practices, healthcare professionals and volunteers who participated in this study.
Authors’ relationships and activities
All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare that no support was received from any organisation for the submitted work. MEJL reports grants from Diabetes UK and non-financial support from Cambridge Weight Plan during the conduct of the study, and he has given unpaid advice about management of medically complicated participants to Counterweight Ltd. AB reports personal fees from Novo Nordisk, Bristol Myers Squibb and GSK, outside the submitted work. RT reports grants from Diabetes UK, personal fees from Novo Nordisk and Wilmington Healthcare, and non-financial support from the Scientific Advisory Committee on Nutrition, outside the submitted work. WSL reports support for conference attendance from Cambridge Weight Plan, outside the submitted work. CMM reports grants from Diabetes UK during the conduct of the study. LM was previously employed by Counterweight Ltd. and reports research funding from Cambridge Weight Plan and consultancy fees from Counterweight Ltd. The authors declare that there are no relationships or activities that might bias, or be perceived to bias, their work.
Funding
DiRECT is funded by Diabetes UK as a Strategic Research Initiative (award number 13/0004691), with support in kind (Counterweight-Plus formula diet sachets) provided by Cambridge Weight Plan to Counterweight Ltd. This economic analysis was funded by a separate project grant from Diabetes UK (award number 17/0005695). The funders had no role in the design, conduct, analysis or reporting of the study.
Author information
Authors and Affiliations
Contributions
YX and AD led the conduct of the statistical analysis of cost-effectiveness and reporting of the work. LM contributed to the data acquisition and was significantly involved in data interpretation and manuscript writing. AB supervised the design, conduct and interpretation of the cost-effectiveness analysis. CMM managed the study data and contributed to data acquisition and interpretation. EG contributed significantly to the cost-effectiveness analysis design and assisted with the costing of intervention delivery. WSL is the DiRECT trial coordinator, responsible for recruitment and study data acquisition. RT is joint principal investigator of the DiRECT trial, which provided the data, and contributed to planning of the present study. MEJL is joint principal investigator of the DiRECT trial and contributed significantly to the study design and interpretation, presentation and drafting of the present manuscript. All authors critically reviewed and revised the manuscript and have read and approved the final version. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted. MEJL is the guarantor of this work.
Corresponding author
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Yiqiao Xin and Andrew Davies are joint first authors.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Xin, Y., Davies, A., Briggs, A. et al. Type 2 diabetes remission: 2 year within-trial and lifetime-horizon cost-effectiveness of the Diabetes Remission Clinical Trial (DiRECT)/Counterweight-Plus weight management programme. Diabetologia 63, 2112–2122 (2020). https://doi.org/10.1007/s00125-020-05224-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00125-020-05224-2