
Abstract
Aims/hypothesis
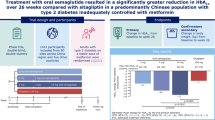
The aim of this study was to evaluate the efficacy and safety of oral semaglutide monotherapy vs placebo in a predominantly Chinese population with type 2 diabetes insufficiently controlled with diet and exercise alone.
Methods
The Peptide Innovation for Early Diabetes Treatment (PIONEER) 11 trial was a double-blind, randomised, Phase IIIa trial conducted across 52 sites in the China region (mainland China and Taiwan), Hungary, Serbia and Ukraine. Eligible participants were ≥18 years (≥20 years in Taiwan), had a diagnosis of type 2 diabetes with HbA1c 53–86 mmol/mol (7.0–10.0%) and were not receiving any glucose-lowering drugs. After a 4-week run-in period in which participants were treated with diet and exercise alone, those who fulfilled the randomisation criteria were randomised (1:1:1:1) using a web-based randomisation system to receive once-daily oral semaglutide 3 mg, 7 mg or 14 mg or placebo for 26 weeks (using a 4-week dose-escalation regimen for the higher doses). Randomisation was stratified according to whether participants were from the China region or elsewhere. The primary and confirmatory secondary endpoints were change from baseline to week 26 in HbA1c and body weight (kg), respectively. Safety was assessed in all participants exposed to at least one dose of the trial product.
Results
Between October 2019 and October 2021, a total of 774 participants were screened and 521 participants were randomised to oral semaglutide 3 mg (n=130), 7 mg (n=130), 14 mg (n=130) or placebo (n=131); most participants (92.5%, n=482) completed the trial, with 39 participants prematurely discontinuing treatment. The number of participants contributing to the trial analyses was based on the total number of participants who were randomised at the beginning of the trial. The majority of participants were male (63.7%), and the mean age of participants was 52 years. At baseline, mean HbA1c and body weight were 63 mmol/mol (8.0%) and 79.6 kg, respectively. Oral semaglutide resulted in significantly greater reductions in HbA1c than placebo at week 26 (p<0.001 for all doses). The estimated treatment differences (ETDs [95% CIs]) for oral semaglutide 3 mg, 7 mg and 14 mg vs placebo were –11 (–13, –9) mmol/mol, –16 (–18, –13) mmol/mol and –17 (–19, –15) mmol/mol, respectively. The corresponding ETDs in percentage points (95% CI) vs placebo were –1.0 (–1.2, –0.8), –1.4 (–1.6, –1.2) and –1.5 (–1.8, –1.3), respectively. Significantly greater reductions in body weight were also observed for oral semaglutide 7 mg and 14 mg than for placebo at week 26 (ETD [95% CI] –1.2 kg [–2.0 kg, –0.4 kg; p<0.01] and –2.0 kg [–2.8 kg, –1.2 kg; p<0.001], respectively), but not for oral semaglutide 3 mg (ETD [95% CI] –0.0 kg [–0.9 kg, 0.8 kg; not significant]). Similar reductions in HbA1c and body weight were observed in the Chinese subpopulation, which represented 74.9% of participants in the overall population. Adverse events (AEs) occurred in between 65.4% and 72.3% of participants receiving oral semaglutide (for all doses) and 57.3% of participants with placebo. Most AEs were mild to moderate in severity, with few serious AEs reported; the most commonly reported AEs were gastrointestinal-related and were more frequent with semaglutide (all doses) than with placebo. The proportion of AEs was slightly higher in the Chinese subpopulation.
Conclusions/interpretation
Oral semaglutide resulted in significantly greater reductions in HbA1c across all doses and in significant body weight reductions for the 7 mg and 14 mg doses when compared with placebo in predominantly Chinese participants with type 2 diabetes insufficiently controlled by diet and exercise alone. Oral semaglutide was generally well tolerated, with a safety profile consistent with that seen in the global PIONEER trials.
Trial registration
ClinicalTrials.gov NCT04109547.
Funding
Novo Nordisk A/S.
Graphical Abstract

Similar content being viewed by others

Avoid common mistakes on your manuscript.

Introduction
The most recent literature search to inform the IDF Diabetes Atlas reported that, in 2021, there were approximately 530 million people living with diabetes globally and estimated that this number will increase to around 780 million in 2045 [1]. In China the trend is no different: there were approximately 140 million cases of diabetes in 2021, which is predicted to increase to 174 million by 2045 [1]. Both globally and in China, type 2 diabetes accounts for the majority of cases [1], highlighting a clear need for more treatment options.
Achievement and maintenance of glycaemic targets and weight loss are important treatment goals for people with type 2 diabetes and can help reduce the long-term risk of some complications associated with chronic disease [2, 3]. Recently, distinct differences in the clinical phenotype and pathophysiology of type 2 diabetes in East Asian populations and Western populations have been recognised [4,5,6]. These differences can impact therapeutic approaches and responses to treatment; therefore, adjustments to treatment strategies across different populations should be considered [4,5,6].
Treatment with glucagon-like peptide-1 receptor agonists (GLP-1RAs) enables people with type 2 diabetes to achieve reductions in HbA1c and body weight [7,8,9]. Some GLP-1RAs, including s.c. semaglutide, reduce the risk of major adverse cardiovascular events and have beneficial effects on cardiometabolic risk factors, including BP and lipid profiles [10,11,12]. Furthermore, HbA1c and body weight reductions with s.c. semaglutide are largely consistent across different ethnic groups [13,14,15,16]. GLP-1RAs are recommended for treating type 2 diabetes in international (ADA/EASD) and Chinese guidelines [17, 18]. The Chinese Diabetes Society (CDS) recommends the use of GLP-1RAs or sodium–glucose cotransporter 2 inhibitors (unless contraindicated) as an adjunct to metformin regardless of the glycaemic target in people with type 2 diabetes and established atherosclerotic CVD, or in those with high CVD risk [18]. Additionally, the CDS recommends considering GLP-1RAs, among other glucose-lowering drugs, alongside lifestyle interventions for people with type 2 diabetes and a BMI ≥27 kg/m2 [18]. In China, the use of s.c. GLP-1RAs is typically less common than the use of other glucose-lowering drugs, possibly because of the need to administer them by injection, highlighting the need for effective and easily administered therapies [19].
Oral semaglutide, a co-formulation of the human glucagon-like peptide-1 (GLP-1) analogue semaglutide and the absorption enhancer sodium N-[8(2-hydroxybenzoyl)amino]caprylate (SNAC), is the first GLP-1RA developed for oral administration in type 2 diabetes [20, 21]. Although semaglutide is also available as an s.c. injection [22, 23], the availability of an oral GLP-1RA presents a useful alternative to injectables, removing the administrative burden and encouraging greater uptake of GLP-1RAs [20, 24]. The efficacy and safety of once-daily oral semaglutide have been extensively evaluated in participants with type 2 diabetes in the global Peptide Innovation for Early Diabetes Treatment (PIONEER) Phase IIIa clinical trial programme (PIONEER 1–8) [7, 8, 25,26,27,28,29,30]. Oral semaglutide was effective at improving glycaemic control compared with placebo and active comparators, with a safety profile consistent with the GLP-1RA class; gastrointestinal symptoms were the most common adverse events (AEs) [7, 8, 25,26,27,28,29,30]. Although the global Phase IIIa clinical programme included Asian racial and ethnic groups, there is limited evidence of the efficacy and safety of oral semaglutide in predominantly Chinese populations [7, 8, 25,26,27,28,29,30]. Two trials (PIONEER 9 and 10) have demonstrated the efficacy and safety of oral semaglutide in a predominantly Japanese population [31, 32]. The current study has some similarities with the PIONEER 1 trial, with similar treatment arms, inclusion criteria, trial length and endpoints; however, PIONEER 1 was a global trial and as such had a far smaller Asian population [7]. PIONEER 1 may provide a useful comparison in terms of outcomes, highlighting differences in response between Asian and non-Asian individuals receiving oral semaglutide and providing a point of comparison with placebo [7].
This multiregional PIONEER 11 Phase IIIa trial aimed to assess the efficacy and safety of oral semaglutide monotherapy compared with placebo in a predominantly Chinese population with type 2 diabetes, insufficiently controlled with diet and exercise. An additional Phase III trial, PIONEER 12 (NCT04017832), was also conducted to assess the efficacy and safety of oral semaglutide vs the dipeptidyl peptidase-4 inhibitor (DPP-4i), sitagliptin, in a predominantly Chinese population with type 2 diabetes, insufficiently controlled with metformin [33].
Methods
Trial design
PIONEER 11 (ClinicalTrials.gov NCT04109547) was a 26 week, randomised, double-blind, placebo-controlled, parallel-group Phase IIIa trial with a 4-week run-in period conducted at 52 sites in the China region (including mainland China and Taiwan), Hungary, Serbia and Ukraine. The trial protocol was approved by the appropriate health authorities according to local guidelines and by an institutional review board/independent ethics committee, and the trial was conducted in accordance with the Declaration of Helsinki 2013 and International Council for Harmonisation Good Clinical Practice guidelines. A list of investigators is provided in electronic supplementary material (ESM) Appendix 1. Participants were required to provide written informed consent prior to commencing any trial-related activity.
Participants
Participants with diagnosed type 2 diabetes were eligible for participation if they were aged ≥18 years at the time of informed consent (≥20 years in Taiwan) and had an HbA1c between 53 and 86 mmol/mol (7.0–10.0%). Key exclusion criteria included treatment with a glucose-lowering medication or medication for obesity within 60 days before screening, except for short-term (14 days) insulin use; renal impairment (eGFR <60 ml/min per 1.73 m2); history/presence of pancreatitis (acute or chronic); history/presence of malignant neoplasms within 5 years before screening; family (first-degree relative) or personal history of multiple endocrine neoplasia type 2 or medullary thyroid carcinoma; and uncontrolled or potentially unstable diabetic retinopathy or maculopathy. Full inclusion, exclusion and randomisation criteria are provided in ESM Table 1. Demographic data including date of birth, sex, and race and ethnicity were recorded according to local regulations and were self-reported.
Trial procedures, randomisation and masking
The key randomisation criterion was HbA1c between 53 and 80 mmol/mol (7.0–9.5%) inclusive, measured at visit 3 (1 week before randomisation). After a 4 week run-in period, all eligible participants were randomised 1:1:1:1 using a web-based randomisation system to once-daily oral semaglutide (3 mg, 7 mg or 14 mg) or placebo for 26 weeks, with a follow-up visit taking place at 31 weeks (ESM Fig. 1). Participants initiated treatment with 3 mg once daily and those randomised to 7 mg or 14 mg followed a fixed 4-week dose-escalation regimen until reaching the randomised maintenance dose (7 mg was reached after 4 weeks and 14 mg after 8 weeks). Full treatment administration details are provided in ESM Appendix 2. Randomisation was stratified according to whether participants were from the China region (including mainland China and Taiwan) or elsewhere. The population of participants from the China region is referred to henceforth as the Chinese subpopulation.
Oral semaglutide or placebo were administered as a once-daily tablet in the morning with up to half a glass of water (approximately 120 ml) in a fasting state, at least 30 min before participants’ first meal. Participants with persistent and unacceptable hyperglycaemia (fasting plasma glucose [FPG] >13.3 mmol/l from week 8 to week 13, or >11.1 mmol/l from week 14 until the end of the trial) were offered rescue medication, which was applied from week 8 (visit 7) onwards. Rescue medication, excluding GLP-1RAs, DPP-4is or amylin analogues, were prescribed at the investigators’ discretion according to ADA/EASD guidelines [18]. Participants who prematurely discontinued semaglutide were switched to another glucose-lowering drug at the investigators’ discretion.
Adherence to the trial protocol was maintained where possible during the COVID-19 pandemic (see ESM Appendix 3 for further details).
Endpoints and assessments
The primary endpoint was change in HbA1c from baseline to week 26, and the confirmatory secondary endpoint was change in body weight (kg) from baseline to week 26. Supportive secondary endpoints included achievement of the American Association of Clinical Endocrinology (AACE) target of HbA1c ≤48 mmol/mol (≤6.5%), the ADA target of HbA1c <53 mmol/mol (<7.0%) or body weight loss ≥5% or ≥10% at week 26, and change from baseline to week 26 in FPG, 7-point self-monitored plasma glucose (SMPG) profile, body weight (%), BMI, waist circumference, BP and fasting lipid profile. Two composite endpoints were assessed: HbA1c <53 mmol/mol (<7.0%) without treatment-emergent severe hypoglycaemia or blood glucose-confirmed (plasma glucose <3.1 mmol/l) symptomatic hypoglycaemia and no body weight gain; and HbA1c reduction ≥10.9 mmol/mol (≥1%) and body weight loss ≥3%. The change from baseline to week 26 in participant-reported outcomes was assessed using the 36-item Short Form Health Survey (Acute Version) (SF-36v2).
Safety was evaluated up to approximately 31 weeks by assessment of AEs, number of hypoglycaemic episodes and the change from baseline in vital signs and laboratory assessments. Hypoglycaemic episodes were defined according to the three-tier ADA 2018 definition [34].
An independent external event adjudication committee was established to perform an assessment of certain AEs (deaths, acute coronary syndrome, cerebrovascular events, heart failure requiring hospitalisation, acute pancreatitis, malignant neoplasm, thyroid disease [malignant neoplasm or C-cell hyperplasia], acute kidney injury and lactic acidosis) according to predefined diagnostic criteria. To assess the incidence of diabetic retinopathy, a fundus eye examination was performed prior to randomisation and at the end of treatment (either week 26 or at the time of product discontinuation).
Statistical analysis
A sample size calculation was performed to ensure that the trial had ≥90% statistical power to confirm the superiority of oral semaglutide vs placebo at each dose level for change in HbA1c from baseline to week 26 (primary estimand). In total, it was planned to include130 participants in each treatment group (520 participants in total). The planned number of participants from the China region was 75% of the total sample size (n=390). Analyses of efficacy endpoints were based on the full analysis set, which included all randomised participants, and analyses of safety endpoints were based on the safety analysis set, which included all participants exposed to one or more dose of trial product.
Two questions relating to the efficacy objectives were addressed through the definition of two estimands. The trial product estimand (primary) evaluated the treatment effect for all randomised participants under the assumption that all participants continued taking the trial product for the entire planned duration of the trial and did not use rescue medication. The treatment policy estimand (secondary) evaluated the treatment effect for all randomised participants regardless of trial product discontinuation or use of rescue medication. A series of observation periods was also defined (ESM Appendix 4).
The primary analysis for the trial product estimand was a mixed model for repeated measures using a restricted maximum likelihood, with treatment and region as categorical fixed effects and baseline HbA1c or body weight as a covariate. For the trial product estimand, a closed testing procedure was used to control the overall type 1 error at a nominal two-sided 5% level. Overall significance of 0.05 (two-sided) was initially allocated to the HbA1c superiority test on the highest dose level. The statistical testing strategy ensured that superiority was established in terms of HbA1c before testing for the benefits on body weight at the same dose. Superiority for HbA1c had to be established for higher doses before continuing to test hypotheses at lower doses (ESM Fig. 2). The local significance level was to be reallocated if a hypothesis was confirmed. For the primary analysis for the treatment policy estimand, a pattern mixture model using multiple imputation to handle missing data was used. Change in HbA1c from baseline to week 26 was analysed using ANCOVA, with treatment and region as categorical fixed effects and baseline HbA1c or body weight as a covariate.
All analyses described for the primary and secondary endpoints were also performed on the Chinese subpopulation, except for the removal of region as a categorical fixed effect in the model (prespecified). Given the uniformity of diabetes across gender and sex, no special consideration was given to a sex and gender analysis.
Results
Participants and baseline characteristics
Between October 2019 and October 2021, 774 participants were screened and 521 participants were randomised to receive oral semaglutide 3 mg (n=130), 7 mg (n=130), 14 mg (n=130) or placebo (n=131) (Fig. 1). All 521 participants were included in the full analysis set, and 520 participants were included in the safety analysis set. Most participants (92.5%) completed treatment (oral semaglutide 3 mg, n=121; 7 mg, n=122; 14 mg, n=118; placebo, n=121), with 39 (7.5%) participants among all treatment groups discontinuing early. Of those receiving oral semaglutide, 88.5–91.5% completed treatment without receiving rescue medication, compared with 80.9% receiving placebo; rescue medication was started after a significantly longer time period with oral semaglutide (7 mg and 14 mg) compared with placebo (ESM Table 2). Across the entire study population, 4.6% of participants received rescue medication, with more participants in the placebo group receiving rescue medication than those in the oral semaglutide groups (ESM Table 3). Furthermore, 6.5% of all participants received additional concomitant glucose-lowering medication throughout the study (ESM Table 4).

Participant flow diagram
Baseline demographics and characteristics were generally similar between treatment groups (Table 1). The majority of participants were male (63.7% [n=332]) and from the China region (74.9% [n=390]). The mean age of participants was 52 years, mean duration of type 2 diabetes was 2.2 years, mean HbA1c was 63 mmol/mol (8.0%), mean FPG was 8.71 mmol/l and mean body weight was 79.6 kg. Most participants had a BMI ≥25 kg/m2; the mean BMI across all treatment groups was 28.2 kg/m2.
Primary endpoint
For the trial product estimand, oral semaglutide (3 mg, 7 mg and 14 mg) was superior to placebo in reducing HbA1c from baseline to week 26 (Fig. 2). The estimated mean changes in HbA1c from baseline to week 26 were –12 mmol/mol (–1.1 percentage points), –16 mmol/mol (–1.5 percentage points), –17 mmol/mol (–1.6 percentage points) and –0 mmol/mol (–0.0 percentage points) for oral semaglutide 3 mg, 7 mg and 14 mg and placebo, respectively. The estimated treatment differences (ETDs [95% CIs]) for oral semaglutide 3 mg, 7 mg and 14 mg vs placebo were –11 (–13, –9) mmol/mol, –16 (–18, –13) mmol/mol and –17 (–19, –15) mmol/mol, respectively (p<0.001 for all doses; Fig. 2a,b). The corresponding ETDs in percentage points (95% CI) vs placebo were –1.0 (–1.2, –0.8), –1.4 (–1.6, –1.2) and –1.5 (–1.8, –1.3), respectively. Similar significant reductions in HbA1c were observed for oral semaglutide vs placebo for the treatment policy estimand (p<0.001 for all doses; Fig. 2c,d). Additionally, similar significant HbA1c reductions were observed in the Chinese subpopulation for both estimands (Fig. 3).

Change in HbA1c from baseline to week 26 (primary endpoint) in the overall trial population. Observed and estimated mean (±SEM) and estimated mean change from baseline for HbA1c by the trial product estimand (a, b) and the treatment policy estimand (c, d). Data are for the on-treatment period without rescue medication (a, b) or for the in-trial period (c, d) for the total trial population. Baseline mean (SD) HbA1c values were 63 (7) mmol/mol (7.9% [0.6%]), 62 (7) mmol/mol (7.9% [0.7%]) and 64 (10) mmol/mol (8.0% [0.9%]) for oral semaglutide 3 mg, 7 mg and 14 mg, respectively, and 64 (8) mmol/mol (8.0% [0.7%]) for placebo. ETDs (95% CI) for oral semaglutide 3 mg, 7 mg and 14 mg vs placebo for the trial product estimand were –11 (–13, –9), –16 (–18, –13) and –17 (–19, –15) mmol/mol, respectively. ETDs (95% CI) for oral semaglutide 3 mg, 7 mg and 14 mg vs placebo for the treatment policy estimand were –8 (–11, –6), –13 (–15, –10) and –14 (–16, –11) mmol/mol, respectively. aEstimated means and corresponding error bars are from the primary analysis. ***p<0.001

Change in HbA1c from baseline to week 26 (primary endpoint) in the Chinese subpopulation. Observed and estimated mean values (±SEM) and estimated mean change from baseline for HbA1c by the trial product estimand (a, b) and the treatment policy estimand (c, d). Data are for the on-treatment without rescue medication period (a, b) or for the in-trial period (c, d) for the Chinese subpopulation. Baseline mean (SD) HbA1c values were 63 (7) mmol/mol (7.9% [0.7%]), 63 (8) mmol/mol (7.9% [0.7%]) and 64 (8) mmol/mol (8.0% [0.7%]) for oral semaglutide 3 mg, 7 mg and 14 mg, respectively, and 64 (8) mmol/mol (8.0% [0.7%]) for placebo. ETDs (95% CI) for oral semaglutide 3 mg, 7 mg and 14 mg vs placebo for the trial product estimand were –13 (–15, –10), –18 (–20, –16) and –18 (–20, –16) mmol/mol, respectively. ETDs (95% CI) for oral semaglutide 3 mg, 7 mg and 14 mg vs placebo for the treatment policy estimand were –9 (–12, –7), –15 (–17, –12) and –14 (–17, –12) mmol/mol, respectively. aEstimated means and corresponding error bars are from the primary analysis. ***p<0.001
Confirmatory secondary endpoint
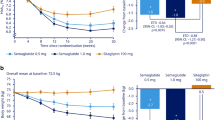
For the trial product estimand, oral semaglutide (7 mg and 14 mg) was superior to placebo in reducing body weight from baseline to week 26 (Fig. 4). The estimated mean changes in body weight from baseline to week 26 were –1.1 kg, –2.2 kg, –3.0 kg and –1.0 kg for oral semaglutide 3 mg, 7 mg and 14 mg and placebo, respectively. The ETDs for oral semaglutide 3 mg, 7 mg and 14 mg vs placebo were –0.0 kg (95% CI –0.9, 0.8; not significant), –1.2 kg (95% CI –2.0, –0.4; p<0.01) and –2.0 kg (95% CI –2.8, –1.2; p<0.001), respectively (Fig. 4a,b). Similar reductions in body weight were observed for the treatment policy estimand (Fig. 4c,d) and in the Chinese subpopulation for both estimands (Fig. 5).

Change in body weight from baseline to week 26 (confirmatory secondary endpoint) in the overall trial population. Observed and estimated mean values (±SEM) and estimated mean change from baseline for body weight by the trial product estimand (a, b) and the treatment policy estimand (c, d). Data are for the on-treatment without rescue medication period (a, b) or for the in-trial period (c, d) for the total trial population. Baseline mean (SD) body weight was 76.6 (15.8) kg, 80.8 (17.4) kg and 79.7 (19.7) kg for oral semaglutide 3 mg, 7 mg and 14 mg, respectively, and 81.1 (16.5) kg for placebo. ETDs (95% CI) for oral semaglutide 3 mg, 7 mg and 14 mg vs placebo for the trial product estimand were –0.0 (–0.9, 0.8), –1.2 (–2.0, –0.4) and –2.0 (–2.8, –1.2) kg, respectively. ETDs (95% CI) for oral semaglutide 3 mg, 7 mg and 14 mg for placebo for the treatment policy estimand were –0.1 (–0.9, 0.7), –1.1 (–2.0, –0.3) and –1.9 (–2.8, –1.1) kg, respectively. aEstimated means and corresponding error bars are from the primary analysis. **p<0.01; ***p<0.001

Change in body weight from baseline to week 26 (confirmatory secondary endpoint) in the Chinese subpopulation. Observed and estimated mean values (±SEM) and estimated mean change from baseline for body weight by the trial product estimand (a, b) and the treatment policy estimand (c, d). Data are for the on-treatment without rescue medication period (a, b) or for the in-trial period (c, d) for the Chinese subpopulation. Baseline mean (SD) body weight was 71.2 (11.9) kg, 75.2 (12.2) kg and 72.6 (11.6) kg for oral semaglutide 3 mg, 7 mg and 14 mg, respectively, and 77.5 (15.5) kg for placebo. ETDs (95% CI) for oral semaglutide 3 mg, 7 mg and 14 mg vs placebo for the trial product estimand were –0.1 (–1.0, 0.8), –1.2 (–2.1, –0.4) and –1.9 (–2.8, –1.0) kg, respectively. ETDs (95% CI) for oral semaglutide 3 mg, 7 mg and 14 mg vs placebo for the treatment policy estimand were –0.2 (–1.1, 0.7), –1.2 (–2.1, –0.3) and –1.8 (–2.8, –0.8) kg, respectively. aEstimated means and corresponding error bars are from the primary analysis. **p<0.01; ***p<0.001
Supportive secondary endpoints (trial product estimand)
For the trial product estimand, a greater observed proportion of participants achieved the AACE target of HbA1c ≤48 mmol/mol (≤6.5%) and the ADA target of HbA1c <53 mmol/mol (<7.0%) with oral semaglutide than with placebo at week 26 (Table 2). The estimated odds for achieving each HbA1c target were significantly in favour of oral semaglutide vs placebo (p<0.001 for all doses). The mean changes from baseline in FPG and 7-point SMPG were significantly greater with oral semaglutide vs placebo (p<0.001 for all doses; Table 2).
Significantly greater reductions in body weight (%) were observed with oral semaglutide 7 mg and 14 mg (p<0.01 for both doses), but not with 3 mg (p=0.80), compared with placebo (Table 2). Greater observed proportions of participants achieved body weight loss of ≥5% or ≥10% with oral semaglutide than with placebo (Table 2); the odds of achieving body weight loss of ≥5% were significantly greater with oral semaglutide 7 mg and 14 mg vs placebo, as were the odds of achieving body weight loss of ≥10% with oral semaglutide 14 mg vs placebo (Table 2). Similarly, BMI was significantly reduced with oral semaglutide 7 mg and 14 mg (p<0.001 for both doses) vs placebo, but not with 3 mg (ESM Table 5). Waist circumference was significantly reduced from baseline with oral semaglutide 14 mg (p<0.05) vs placebo, but not with oral semaglutide 3 mg or 7 mg (ESM Table 5).
Greater observed proportions of participants achieved both composite endpoints ≥10.9 mmol/mol (≥1 percentage point) HbA1c reduction and ≥3% weight loss, and HbA1c <53 mmol/mol (<7.0%) without severe or blood glucose-confirmed symptomatic hypoglycaemia and with no weight gain with oral semaglutide (all doses) than with placebo (Table 2). The estimated odds for achieving each composite endpoint were significantly in favour of oral semaglutide vs placebo (p<0.01 for all doses).
Treatment with oral semaglutide 14 mg resulted in significant reductions from baseline to week 26 in total cholesterol, LDL-cholesterol and triglycerides vs placebo (p<0.05 for all endpoints), although no noticeable differences were observed with oral semaglutide 3 mg or 7 mg (Table 2).
Overall, participant-reported outcomes, assessed using the SF-36v2 (general health and mental health), were not significantly different between oral semaglutide and placebo (ESM Table 5).
Results for the supportive secondary endpoints were broadly similar for the treatment policy estimand (Table 3 and ESM Table 5).
Adverse events and tolerability
Overall, the proportion of participants experiencing AEs was higher for all doses of oral semaglutide than for placebo (Table 3). Gastrointestinal disorders were the most frequently reported AEs; a higher proportion of participants experienced these with oral semaglutide (3 mg: 16.2%, 7 mg: 32.3% and 14 mg: 31.8%) than with placebo (9.2%). Diarrhoea and nausea were the most common gastrointestinal AEs, although most cases were mild and of short duration. Diabetic retinopathy was reported in 4.6% (n=6) and 1.5% (n=2) of participants on oral semaglutide 3 mg and placebo, respectively, while no cases were reported with oral semaglutide 7 mg and 14 mg.
Most AEs were mild to moderate in severity, and the proportion of serious adverse events (SAEs) was low across treatment groups, but was highest with oral semaglutide 7 mg (Table 3). Three SAEs were considered to be possibly related to the trial product by the investigator, including one mild event of cholelithiasis with oral semaglutide 14 mg. There were two event adjudication committee-confirmed events (ESM Table 6). Hypoglycaemic events were rare, with only two participants experiencing a level 2 hypoglycaemic event (one each with oral semaglutide 3 mg and 7 mg) and no participants experiencing a level 3 (severe) hypoglycaemic event. No deaths occurred (Table 3).
Mean eGFR, calcitonin and creatine kinase levels and the bilirubin ratio were similar between treatment groups (ESM Table 7). There were significant increases in amylase and lipase with all doses of oral semaglutide vs placebo (except for amylase with oral semaglutide 3 mg), although increases were mostly observed in the first 14 weeks of treatment (ESM Table 6). BP decreased during treatment with oral semaglutide 7 mg and 14 mg and placebo, but the changes with semaglutide did not significantly differ from that seen with placebo (ESM Table 7). Pulse rate slightly increased from baseline by 2–5 beats/min with oral semaglutide; significant increases were observed with oral semaglutide 7 mg and 14 mg compared with placebo (ESM Table 7).
Compared with the overall population, the proportions of participants experiencing AEs were higher in the Chinese subpopulation (73.2–80.6% with oral semaglutide vs 65.3% with placebo; ESM Table 8). Similar to the overall population, more AEs occurred with oral semaglutide 7 mg than with the 3 mg and 14 mg doses; gastrointestinal AEs were among the most frequent AEs and were more commonly experienced with oral semaglutide than with placebo. The time to the first gastrointestinal event for 25% of participants was numerically shorter for the overall population than for the Chinese subpopulation (ESM Fig. 3). The proportion of participants in the Chinese subpopulation experiencing SAEs remained low and was higher with oral semaglutide (4.2–6.1%) than with placebo (2.0%) (ESM Table 8).
Discussion
This double-blind, randomised trial demonstrated that once-daily oral semaglutide monotherapy was superior to placebo in reducing HbA1c using the trial product estimand in a predominantly Chinese population with type 2 diabetes that was insufficiently controlled with diet and exercise. Significant reductions in HbA1c at week 26 were observed for oral semaglutide vs placebo and the magnitude of the reductions was similar between the overall population and the Chinese subpopulation, which represented 74.9% of the overall population. Similar results were observed for the treatment policy estimand. Reductions in HbA1c with oral semaglutide were comparable to those reported in the global PIONEER 1 trial, which also assessed the efficacy of oral semaglutide monotherapy vs placebo [7], providing a unique comparison between Chinese individuals and their global counterparts. Furthermore, participants treated with all doses of oral semaglutide were more likely to achieve the ADA and AACE HbA1c targets of <53 mmol/mol (<7.0%) and ≤48 mmol/mol (≤6.5%), respectively, than those treated with placebo.
Early intensive glycaemic control is associated with improvements in type 2 diabetes management, including a reduced risk of microvascular complications and all-cause mortality [35, 36]. In China, there is a need for new treatment approaches with more convenient administration routes for people with type 2 diabetes, as a recent Chinese population survey study including over 170,000 people indicated that 49.9% of those with diabetes did not reach glycaemic targets, despite treatment [37].
Superior reductions in body weight from baseline to week 26 were observed for oral semaglutide 7 mg and 14 mg vs placebo (trial product estimand). While no statistical comparisons were made, the magnitude of the reductions was numerically smaller in the Chinese subpopulation than in the overall trial population. Comparatively, body weight reductions with oral semaglutide have been found to be numerically smaller from baseline to week 26 in predominantly Asian populations than in global populations, as demonstrated by the reductions observed in this trial and the PIONEER 9 trial (conducted in a predominantly Japanese population) vs the global PIONEER 1 trial [7, 31]. It should also be noted that the ETDs observed in this trial were numerically inferior to those seen in PIONEER 1 in participants receiving oral semaglutide 3 mg and 14 mg [7]. Although cross-trial comparisons should be viewed with caution, as differences in study design may affect results, these inconclusive results may warrant further investigation. A similar result was observed for s.c. semaglutide (0.5 mg and 1.0 mg) between a China region population (SUSTAIN China) and a global population (SUSTAIN 1) [15, 38]. Of note, although the body weight reductions were smaller, the Asian populations in the trials above had a lower mean baseline body weight and BMI than the equivalent global populations of predominantly Western ethnicity, which may account for the smaller reductions seen [7, 15, 31, 32, 38].
The increasing prevalence of obesity in China presents many health risks, including an increased risk of developing type 2 diabetes. In two studies among individuals living in China with type 2 diabetes, the prevalence of overweight or obesity was 34.6% or 4.4%, respectively (WHO criteria), and the prevalence of dyslipidaemia was 87.7% [39, 40]. During the current trial, notable proportions of participants achieved a clinically meaningful body weight loss of ≥5% with oral semaglutide 7 mg and 14 mg (24% and 37%, respectively). Weight loss is an important consideration when treating type 2 diabetes, as weight loss alongside improved glycaemic control can be beneficial in terms of lipid levels and BP improvements [2, 41, 42].
A higher proportion of AEs was reported for oral semaglutide (mostly the 7 mg dose) than placebo. Diarrhoea, decreased appetite, nausea and upper respiratory tract infections were the most commonly reported AEs, although nausea rates were low and less frequent than in most of the previous global trials [7, 8, 26,27,28,29]. Few SAEs were reported across all treatment groups, although more SAEs were reported in the semaglutide groups than in the placebo group. No level 3 hypoglycaemic episodes occurred, and similar proportions of participants across all treatment groups discontinued treatment due to AEs. These observations are consistent with the results of the global PIONEER trials and the observed safety profile of the GLP-1RA drug class [43]. Of note, the incidence of AEs was higher in the Chinese subpopulation than in the overall population, which is likely to have been driven by the higher number of gastrointestinal AEs.
The strengths of this trial include the randomised, double-blind, controlled trial design, the high number of participants enrolled, particularly in the Chinese subpopulation, and the high number of participants completing the trial, despite the global COVID-19 pandemic. The impact of the pandemic was considered to be limited and thus the data are considered to be robust and acceptable for interpretation. Potential limitations include the trial duration (26 weeks including up to 8 weeks of dose escalation), as this may have limited the time for observing treatment effects (particularly regarding long-term change in glycaemic variables and weight loss), and the inclusion of participants who were generally considered to be healthy; most participants had a healthy eGFR (>90 ml/min per 1.73 m2) and a BMI <30 kg/m2 and were <65 years of age, which may not be representative of the wider Chinese population with type 2 diabetes [37, 44]. A further limitation is that this analysis did not investigate the efficacy of oral semaglutide in terms of sex or gender distribution and, as such, conclusions regarding this cannot be made.
In conclusion, oral semaglutide was superior to placebo in reducing HbA1c (3 mg, 7 mg and 14 mg) and body weight (7 mg and 14 mg) after 26 weeks of treatment in a predominantly Chinese population with type 2 diabetes treated with diet and exercise only (trial product estimand). All doses of oral semaglutide were generally well tolerated and the safety profile was consistent with that of the GLP-1RA class. Given the high proportion of individuals in China with insufficiently controlled type 2 diabetes, and the increasing prevalence of diabetes, it is important to consider new therapeutic options for early intensive treatment of type 2 diabetes.
Abbreviations
- AACE:
-
American Association of Clinical Endocrinology
- AE:
-
Adverse event
- CDS:
-
Chinese Diabetes Society
- DPP-4i:
-
Dipeptidyl peptidase-4 inhibitor
- ETD:
-
Estimated treatment difference
- FPG:
-
Fasting plasma glucose
- GLP-1:
-
Glucagon-like peptide-1
- GLP-1RA:
-
Glucagon-like peptide-1 receptor agonist
- PIONEER:
-
Peptide Innovation for Early Diabetes Treatment
- SAE:
-
Serious adverse event
- SF-36v2:
-
36-item Short Form Health Survey (Acute Version)
- SMPG:
-
Self-monitored plasma glucose
References
Sun H, Saeedi P, Karuranga S et al (2022) IDF diabetes atlas: global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res Clin Pract 183:109119. https://doi.org/10.1016/j.diabres.2021.109119
ElSayed NA, Aleppo G, Aroda VR et al (2023) 8. Obesity and weight management for the prevention and treatment of type 2 diabetes: standards of care in diabetes–2023. Diabetes Care 46(Suppl. 1):S128–S139. https://doi.org/10.2337/dc23-S008
ElSayed NA, Aleppo G, Aroda VR et al (2023) 6. Glycemic targets: standards of care in diabetes–2023. Diabetes Care 46(Suppl. 1):S97–S110. https://doi.org/10.2337/dc23-S006
Hu C, Jia W (2018) Diabetes in China: epidemiology and genetic risk factors and their clinical utility in personalized medication. Diabetes 67(1):3–11. https://doi.org/10.2337/dbi17-0013
Ke C, Narayan KMV, Chan JCN, Jha P, Shah BR (2022) Pathophysiology, phenotypes and management of type 2 diabetes mellitus in Indian and Chinese populations. Nat Rev Endocrinol 18(7):413–432. https://doi.org/10.1038/s41574-022-00669-4
Yabe D, Seino Y, Fukushima M, Seino S (2015) β cell dysfunction versus insulin resistance in the pathogenesis of type 2 diabetes in East Asians. Curr Diab Rep 15(6):602. https://doi.org/10.1007/s11892-015-0602-9
Aroda VR, Rosenstock J, Terauchi Y et al (2019) PIONEER 1: randomized clinical trial of the efficacy and safety of oral semaglutide monotherapy in comparison with placebo in patients with type 2 diabetes. Diabetes Care 42(9):1724–1732. https://doi.org/10.2337/dc19-0749
Rodbard HW, Rosenstock J, Canani LH et al (2019) Oral semaglutide versus empagliflozin in patients with type 2 diabetes uncontrolled on metformin: the PIONEER 2 trial. Diabetes Care 42(12):2272–2281. https://doi.org/10.2337/dc19-0883
Lyseng-Williamson KA (2019) Glucagon-like peptide-1 receptor analogues in type 2 diabetes: their use and differential features. Clin Drug Investig 39(8):805–819. https://doi.org/10.1007/s40261-019-00826-0
Sattar N, Lee MMY, Kristensen SL et al (2021) Cardiovascular, mortality, and kidney outcomes with GLP-1 receptor agonists in patients with type 2 diabetes: a systematic review and meta-analysis of randomised trials. Lancet Diabetes Endocrinol 9(10):653–662. https://doi.org/10.1016/S2213-8587(21)00203-5
Leiter LA, Bain SC, Hramiak I et al (2019) Cardiovascular risk reduction with once-weekly semaglutide in subjects with type 2 diabetes: a post hoc analysis of gender, age, and baseline CV risk profile in the SUSTAIN 6 trial. Cardiovasc Diabetol 18(1):73. https://doi.org/10.1186/s12933-019-0871-8
Marso SP, Bain SC, Consoli A et al (2016) Semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med 375(19):1834–1844. https://doi.org/10.1056/NEJMoa1607141
Seino Y, Terauchi Y, Osonoi T et al (2018) Safety and efficacy of semaglutide once weekly vs sitagliptin once daily, both as monotherapy in Japanese people with type 2 diabetes. Diabetes Obes Metab 20(2):378–388. https://doi.org/10.1111/dom.13082
Kaku K, Yamada Y, Watada H et al (2018) Safety and efficacy of once-weekly semaglutide vs additional oral antidiabetic drugs in Japanese people with inadequately controlled type 2 diabetes: a randomized trial. Diabetes Obes Metab 20(5):1202–1212. https://doi.org/10.1111/dom.13218
Ji L, Dong X, Li Y et al (2021) Efficacy and safety of once-weekly semaglutide versus once-daily sitagliptin as add-on to metformin in patients with type 2 diabetes in SUSTAIN China: a 30-week, double-blind, phase 3a, randomized trial. Diabetes Obes Metab 23(2):404–414. https://doi.org/10.1111/dom.14232
DeSouza C, Cariou B, Garg S, Lausvig N, Navarria A, Fonseca V (2020) Efficacy and safety of semaglutide for type 2 diabetes by race and ethnicity: a post hoc analysis of the SUSTAIN trials. J Clin Endocrinol Metab 105(2):543–556. https://doi.org/10.1210/clinem/dgz072
Davies MJ, Aroda VR, Collins BS et al (2022) Management of hyperglycemia in type 2 diabetes, 2022. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetologia 65:1925–1966. https://doi.org/10.1007/s00125-022-05787-2
Chinese Diabetes Society (2021) Guideline for the prevention and treatment of type 2 diabetes mellitus in China (2020 edition). Chin J Diabetes Mellitus 13(4):315–409. https://doi.org/10.3760/cma.j.cn115791-20210221-00095
Li C, Guo S, Huo J, Gao Y, Yan Y, Zhao Z (2022) Real-world national trends and socio-economic factors preference of sodium-glucose cotransporter-2 inhibitors and glucagon-like peptide-1 receptor agonists in China. Front Endocrinol (Lausanne) 13:987081. https://doi.org/10.3389/fendo.2022.987081
US Food and Drug Administration (2021) Rybelsus®: highlights of prescribing information. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2021/213051s006lbl.pdf. Accessed 8 Aug 2022
European Medicines Agency (2013) Rybelsus. Available from: https://www.ema.europa.eu/en/medicines/human/EPAR/Rybelsus. Accessed 19 Jun 2023
European Medicines Agency (2013) Ozempic. Available from: https://www.ema.europa.eu/en/medicines/human/EPAR/ozempic. Accessed 19 Jun 2023
US Food and Drug Administration (2021) Ozempic®: highlights of prescribing information. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2021/209637s008lbl.pdf. Accessed 27 Apr 2021
Gallwitz B, Giorgino F (2021) Clinical perspectives on the use of subcutaneous and oral formulations of semaglutide. Front Endocrinol 12:645507. https://doi.org/10.3389/fendo.2021.645507
Rosenstock J, Allison D, Birkenfeld AL et al (2019) Effect of additional oral semaglutide vs sitagliptin on glycated hemoglobin in adults with type 2 diabetes uncontrolled with metformin alone or with sulfonylurea: the PIONEER 3 randomized clinical trial. JAMA 321(15):1466–1480. https://doi.org/10.1001/jama.2019.2942
Pratley R, Amod A, Hoff ST et al (2019) Oral semaglutide versus subcutaneous liraglutide and placebo in type 2 diabetes (PIONEER 4): a randomised, double-blind, phase 3a trial. Lancet 394(10192):39–50. https://doi.org/10.1016/S0140-6736(19)31271-1
Mosenzon O, Blicher TM, Rosenlund S et al (2019) Efficacy and safety of oral semaglutide in patients with type 2 diabetes and moderate renal impairment (PIONEER 5): a placebo-controlled, randomised, phase 3a trial. Lancet Diabetes Endocrinol 7(7):515–527. https://doi.org/10.1016/S2213-8587(19)30192-5
Pieber TR, Bode B, Mertens A et al (2019) Efficacy and safety of oral semaglutide with flexible dose adjustment versus sitagliptin in type 2 diabetes (PIONEER 7): a multicentre, open-label, randomised, phase 3a trial. Lancet Diabetes Endocrinol 7(7):528–539. https://doi.org/10.1016/S2213-8587(19)30194-9
Zinman B, Aroda VR, Buse JB et al (2019) Efficacy, safety, and tolerability of oral semaglutide versus placebo added to insulin with or without metformin in patients with type 2 diabetes: the PIONEER 8 trial. Diabetes Care 42(12):2262–2271. https://doi.org/10.2337/dc19-0898
Husain M, Birkenfeld AL, Donsmark M et al (2019) Oral semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med 381(9):841–851. https://doi.org/10.1056/NEJMoa1901118
Yamada Y, Katagiri H, Hamamoto Y et al (2020) Dose-response, efficacy, and safety of oral semaglutide monotherapy in Japanese patients with type 2 diabetes (PIONEER 9): a 52-week, phase 2/3a, randomised, controlled trial. Lancet Diabetes Endocrinol 8(5):377–391. https://doi.org/10.1016/S2213-8587(20)30075-9
Yabe D, Nakamura J, Kaneto H et al (2020) Safety and efficacy of oral semaglutide versus dulaglutide in Japanese patients with type 2 diabetes (PIONEER 10): an open-label, randomised, active-controlled, phase 3a trial. Lancet Diabetes Endocrinol 8(5):392–406. https://doi.org/10.1016/S2213-8587(20)30074-7
Ji L, Agesen RM, Bain SC et al (2024) Efficacy and safety of oral semaglutide vs sitagliptin in a predominantly Chinese population with type 2 diabetes uncontrolled with metformin: PIONEER 12, a double-blind, Phase IIIa, randomised trial. Diabetologia. https://doi.org/10.1007/s00125-024-06133-4
ADA (2018) 6. Glycemic targets: standards of medical care in diabetes-2018. Diabetes Care 41(Suppl 1):S55–S64. https://doi.org/10.2337/dc18-S006
Lind M, Imberg H, Coleman RL, Nerman O, Holman RR (2021) Historical HbA1c values may explain the type 2 diabetes legacy effect: UKPDS 88. Diabetes Care 44(10):2231–2237. https://doi.org/10.2337/dc20-2439
Patel A, MacMahon S, Chalmers J et al (2008) Intensive blood glucose control and vascular outcomes in patients with type 2 diabetes. N Engl J Med 358(24):2560–2572. https://doi.org/10.1056/NEJMoa0802987
Wang L, Li X, Wang Z et al (2021) Prevalence and treatment of diabetes in China, 2013–2018. JAMA 326(24):2498–2506. https://doi.org/10.1001/jama.2021.22208
Sorli C, Harashima SI, Tsoukas GM et al (2017) Efficacy and safety of once-weekly semaglutide monotherapy versus placebo in patients with type 2 diabetes (SUSTAIN 1): a double-blind, randomised, placebo-controlled, parallel-group, multinational, multicentre phase 3a trial. Lancet Diabetes Endocrinol 5(4):251–260. https://doi.org/10.1016/S2213-8587(17)30013-X
Lv F, Cai X, Lin C et al (2021) Sex differences in the prevalence of obesity in 800,000 Chinese adults with type 2 diabetes. Endocr Connect 10(2):139–145. https://doi.org/10.1530/EC-20-0547
Li J, Nie Z, Ge Z, Shi L, Gao B, Yang Y (2022) Prevalence of dyslipidemia, treatment rate and its control among patients with type 2 diabetes mellitus in Northwest China: a cross-sectional study. Lipids Health Dis 21(1):77. https://doi.org/10.1186/s12944-022-01691-1
Rodbard HW, Bellary S, Hramiak I et al (2019) Greater combined reductions in HbA1c ≥1.0% and weight ≥5.0% with semaglutide versus comparators in type 2 diabetes. Endocr Pract 25(6):589–597. https://doi.org/10.4158/ep-2018-0444
Dungan KM, Bardtrum L, Christiansen E et al (2023) Greater combined reductions of HbA1c ≥ 1.0% and body weight loss ≥ 5.0% or ≥ 10.0% with orally administered semaglutide versus comparators. Diabetes Ther Res Treat Educ Diabetes Relat Disord 14(8):1415–1425. https://doi.org/10.1007/s13300-023-01413-5
Thethi TK, Pratley R, Meier JJ (2020) Efficacy, safety and cardiovascular outcomes of once-daily oral semaglutide in patients with type 2 diabetes: the PIONEER programme. Diabetes Obes Metab 22(8):1263–1277. https://doi.org/10.1111/dom.14054
Li Y, Teng D, Shi X et al (2020) Prevalence of diabetes recorded in mainland China using 2018 diagnostic criteria from the American Diabetes Association: national cross sectional study. BMJ 369:m997. https://doi.org/10.1136/bmj.m997
Author information
Authors and Affiliations
Consortia
Corresponding author
Ethics declarations
Acknowledgements
Medical writing and editorial support were provided by A. Richold (Apollo, OPEN Health Communications, London, UK) and were funded by Novo Nordisk, in accordance with Good Publication Practice 3 (GPP3) guidelines (www.ismpp.org/gpp3). The authors thank the participants, the investigators, all trial site staff and all Novo Nordisk A/S employees involved in the trial. The authors also thank W. Liu of Novo Nordisk A/S for her role in reviewing this manuscript.
Data availability
Data will be shared with researchers submitting a research proposal approved by the independent review board. Information on requesting access to datasets can be found at www.novonordisk-trials.com. Data will be made available after research completion and approval of the product and product use in the European Union and the USA. Individual participant data will be shared in datasets in a de-identified and anonymised format, with no limitations on how the data can be used.
Funding
This trial was funded by Novo Nordisk A/S, Søborg, Denmark. The study sponsor was involved in the study design, data collection, analysis and interpretation and the writing of this report.
Authors’ relationships and activities
SCB received honoraria and teaching and research sponsorship/grants from AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, Eli Lilly, GlaxoSmithKline, MSD, Novo Nordisk, Pfizer, Sanofi and Takeda. RC and BL are employees and shareholders of Novo Nordisk (China) Pharmaceuticals Co., Ltd. SG and TBJ are employees and shareholders of Novo Nordisk A/S. All other authors declare that there are no relationships or activities that might bias, or be perceived to bias, their work.
Contribution statement
All authors made substantial contributions to the conception and design of the trial, acquisition of data and/or the analysis and interpretation of data. All authors had access to the study data, critically reviewed the manuscript and approved the final version to be published. WW, RC, SG, TBJ and BL are guarantors of this work and, as such, have full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
A complete list of investigators in the Peptide Innovation for Early Diabetes Treatment 11 (PIONEER 11) trial is provided in the electronic supplementary material.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Wang, W., Bain, S.C., Bian, F. et al. Efficacy and safety of oral semaglutide monotherapy vs placebo in a predominantly Chinese population with type 2 diabetes (PIONEER 11): a double-blind, Phase IIIa, randomised trial. Diabetologia 67, 1783–1799 (2024). https://doi.org/10.1007/s00125-024-06142-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00125-024-06142-3