
Abstract
Inequities in mental health service use (MHSU) and treatment are influenced by social stratification processes linked to socially contextualised interactions between individuals, organisations and institutions. These complex relations underpin observed inequities and their experience by people at the intersections of social statuses. Discrimination is one important mechanism influencing such differences. We compared inequities in MHSU/treatment through single and intersectional status analyses, accounting for need. We assessed whether past-year discrimination differentially influences MHSU/treatment across single and intersecting statuses. Data came from a population survey (collected 2014–2015) nationally representative of English households (N = 7546). We used a theory and datadriven approach (latent class analysis) which identified five intersectional groups in the population comprising common combinations of social statuses. Single status analyses identified characteristics associated with MHSU/treatment (being a sexual minority (adjusted odds ratio (AOR) 1.65 95% CI:1.09-2.50), female (AOR 1.71, 95% CI:1.45–2.02), economically inactive (AOR 2.02, 95% CI:1.05–3.90), in the most deprived quintile (AOR 1.33, 95% CI:1.02–1.74), and Black (AOR 0.36 95% CI:0.20–0.66)). Intersectional analyses detected patterns not apparent from single status analyses. Compared to the most privileged group (“White British, highly educated, employed, high social class”), “Retired White British” had greater odds of MHSU/treatment (AOR 1.88, 95% CI:1.53-2.32) while “Employed migrants” had lower odds (AOR 0.39, 95% CI:0.27–0.55). Past-year discrimination was associated with certain disadvantaged social statuses and greater MHSU/treatment but—except for sexual minorities—adjusting for discrimination had little influence using either analytic approach. Observing patterns only by single social statuses masks potentially unanticipated and contextually varying inequities. The latent class approach offers policy-relevant insights into patterns and mechanisms of inequity but may mask other key intersectional patterns by statuses less common or under represented in surveys (e.g. UK-born ethnic minority groups). We propose multiple, context-relevant, theory-driven approaches to intersectional understanding of mental health inequalities.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Stress process theory describes how social stratification systems lead to inequalities in mental health through accumulative lifetime exposure to adversities and disparities in access to social, cultural and material resources [47]. Such hierarchical categorisations (e.g., on the basis of race/ethnicity, gender or social class) are emergent from, maintained by, and transformed through interactions between individuals, organisations and institutions within and across social contexts [36]. However, they relate to stress and mental health in complex ways [37], reflected in the differences in experience across and at the intersections of various statuses and contexts (e.g., social class). This is in addition to the inter- and intra-personal processes linked to social identity, meaning construction, and reflexive deliberation [36, 57]. To understand the mechanisms through which observed patterns of inequality are produced and to inform interventions, sociological studies of mental health inequ(al)ities should incorporate and explore this complexity.
One such inequity pertains to the distribution of support for commonly occurring mental disorders, such as anxiety and depression. Despite being a major cause of disability, internationally, there is a large treatment gap and disparities across population groups [29, 39]. Studies have identified several social status characteristics associated with inequitable mental health service use [18, 38, 39] and indicate structural and subjective barriers arising in patient, provider and healthcare system interactions [52, 58].
Seeking help or maintaining service engagement is a socially negotiated process influenced by biases and discrimination based on social statuses, such as race/ethnicity, religion, age, gender, socio-economic status (SES), sexual orientation, and migration status [30, 33]. However, such systems of stratification are likely to shape access to and uptake of mental health support in complex and contextually specific ways. For example, among women but not men, Pakistani and Bangladeshi ethnic groups in England are less likely than White groups to have used mental health services [27]; and, lower rates of primary care depression screening have been reported among Black than White non-Latinx patients in the United States—with an elevated discrepancy among females [25]. Nonetheless, there is little understanding about whether and why people occupying multiple advantaged or disadvantaged statuses differentially access mental health treatment or services.
Intersectionality theory [14] emphasises the simultaneity of multiple social statuses (gender, race/ethnicity, social class, etc.) by recognising people’s experiences of being at a junction of more than one social status or position, each, respectively, shaped by social power. It is therefore inadequate to examine statuses in isolation [11]. People’s multiple statuses may include a mix of privileged and disadvantaged social categories [36] which influence each other, adding further complexity to people’s experiences embedded in different systems of stratification [14, 64]. This is supported by studies finding that patterns of inequalities in mental health differ when examining social statuses singly or intersectionally [22, 24]. Moreover, there may be contextual differences in patterns of inequality in mental health treatment [17]. English-based research from South East London has found that, compared to privileged groups, groups characterised by multiply disadvantaged or a mix of advantaged and disadvantaged positions were more likely to be in receipt of treatment for mental health reasons after accounting for need [21]. The extent to which this is reflected in the wider national setting is unknown.
Moving beyond describing inequalities
Quantitative studies assessing intersectionality focus on two main approaches: descriptively examining outcomes by generating categories representing multiple statuses, or regressing an outcome on multiple social status markers and their interactions [5, 6]. While descriptive approaches are important for identifying intersectional differences in outcomes, analyses incorporating markers of modifiable causal mechanisms are also important to monitor and tackle such inequities [6]. This ‘analytical intersectionality’ should also permit examination of differences in mechanisms underpinning inequities across intersectional status groups, such that neither outcomes nor underlying processes are assumed additive. Here, underlying processes are considered ‘causal’, to the extent that the influences of multiple social advantages or disadvantages on outcomes occur through, or are mediated by, other social processes.
Social stressors, such as stigma and discrimination, are important mechanisms underpinning status-based inequities in mental health treatment and support [6, 7, 13]. Such stressors are grounded in wider social inequalities experienced as both acute life events and chronic hassles. Discrimination—alone and particularly in conjunction with other stressors—is widely demonstrated to elicit psychological and physiological stress responses that impair health [32, 50, 56, 63, 65]. As a stressor, discrimination has adverse effects linked to social devaluation and reduced mastery, eroding psychosocial resources protective against further discriminatory experiences and stress [36, 48, 49]. Discrimination may therefore predict not only greater need for support but also elevated service use [21]. In contrast, experiencing and anticipating discrimination may also inhibit help-seeking by increasing mistrust and fear, affecting service use discontinuation and deterring future service engagement, thus also impacting upon outcomes [26, 56]. Moreover, the experience and impact of discrimination on mental health and service use are also likely to differ within, at the intersections of, and across social statuses [32, 60, 64].
This study builds on previous UK-based work in an urban diverse setting in Southeast London which examined associations between discrimination and health service use for mental health reasons. Adjusting for intersecting social statuses and need, they found that anticipated discrimination predicted higher levels of use supporting its role as a stressor [21]. This study utilises a similar approach using national population-based data representative of households in England to examine mental health service use (MHSU) and treatment at the intersections of multiple advantaged and disadvantaged social statuses. It examines whether discrimination has a differential influence on MHSU/treatment across different intersecting social statuses after accounting for markers of need. Specifically, we address the following hypotheses:
- H1:
-
People with single and multiple disadvantaged social statuses will report greater discrimination and greater MHSU/treatment than more advantaged groups after accounting for need.
- H2:
-
Patterns of discrimination and MHSU/treatment will differ when considering single, compared to multiple social statuses.
- H3:
-
Accounting for discrimination will partially attenuate associations between social status and MHSU/treatment.
- H4:
-
Discrimination will have a greater influence on MHSU/treatment for people occupying multiply disadvantaged social statuses than more advantaged groups, or groups comprising a mix of advantaged and disadvantaged social statuses.
Methods
Data sources
Adult psychiatric morbidity survey
The 2014 Adult Psychiatric Morbidity Survey (APMS) provides data collected between 2014 and 2015 on the prevalence of psychiatric disorders in the English adult population [39]. The sample (N = 7546) was designed to be representative of the population aged 16 years and above living in private households in England. APMS incorporated assessment of common mental disorders, substance misuse and less prevalent psychiatric disorders, such as psychosis. It also collected data on demographic and socio-economic characteristics, discrimination, stressful life events, social support and health service use. Detailed survey profile information is available [40].
Measures
Mental health service use and treatment
APMS permits identification of people receiving any treatment for mental ill health, including any current use of medication (excluding medication solely for dementia, dependence or epilepsy) and any current counselling or therapy. MHSU is indicated by any inpatient or outpatient use of hospital services for mental ill health in the past quarter, or any past-year contact with a GP about being anxious or depressed or a mental, nervous or emotional problem.
Need
We examined variables identified in a recent systematic review [54] as key need factors predicting MHSU for common mental disorders. Severity of symptoms was assessed using the Revised Clinical Interview Schedule (CIS-R) [31]. This structured interview asks about 14 symptom domains: fatigue, sleep problems, irritability, worry, depression, depressive ideas, anxiety, obsessions, subjective memory and concentration, somatic symptoms, compulsions, phobias, physical health worries and panic. We grouped scores as 0–5 (little or no symptoms), 6–11 (sub-threshold), 12–17 (symptoms warranting primary care recognition), or 18 + (symptoms very likely to warrant intervention) [31, 39]. We also included a binary marker of self-reported general health (fair/poor vs good/very good/excellent) and of any physical illness conditions in the past 12 months. Finally, we included a measure of social functioning using the eight-item Social Functioning Questionnaire (SFQ, [61] which assesses ratings of performance and stress related to domains, such as work, household tasks, financial matters, relationships and spare time. We developed a binary variable, where the median (a score of 14) was used to identify ‘better’ (< 14) and ‘worse’ (14 +) social functioning.
Intersectional social status indicators
APMS collects data on ethnicity aligned with the UK census, where participants are asked to choose from eighteen categories across five broad sections to best describe race/ethnic group. Each section contains an ‘Any Other’ category to permit individuals for whom existing options do not apply to self-complete. We distinguished five broad groups due to small sample sizes in the ethnic minority categories, as in previous work with this dataset [39]: White British, White Other, Black/African/Caribbean/Black British, Asian/Asian British, Mixed/Multiple/Other.
Migration status was derived from country of birth, distinguishing migrants (non-UK-born) and non-migrants (UK-born). Gender was available only as a binary variable (male or female). Sexual orientation was included, although was only asked of participants aged under 65 years. We distinguished people identifying as heterosexual or straight from those identifying as gay or lesbian, bisexual, or other (‘sexual minority’), and those unclassified (participants aged 65 + who are not asked to disclose their sexual orientation).
Socio-economic indicators included educational qualification attainment (none, GCSE/vocational-level, A-level, degree level); employment status (employed, unemployed, and three economically inactive groups: student, retired, and other—including sick/disabled and looking after family home); and social class, measured through the National Statistics Socio-economic Classification (NS-SEC) which ordinally categorises socio-economic groups based on employment relations and occupational conditions (Office for National Statistics (ONS) 2019). We used the four-category NS-SEC version, distinguishing managerial/professional, intermediate, routine/manual, or not worked recently.
Assessing intersectionality
Following from previous work [10, 21, 22], we used latent class analysis (LCA), a data-driven method to define intersectional groups with similar profiles according to salient characteristics of social stratification: socio-economic status (education, employment status, social class), ethnicity, migration status, gender, and sexual orientation. In LCA, individuals are categorised based on conditional probabilities such that members of each class have similar patterns of responses to the variables included. Previous intersectionality studies have used the traditional ‘classify-analyse method’ to examine associations between latent class membership and distal outcomes (participants are assigned to a latent class, these data are then exported and analysed separately). However, this approach is now contraindicated [44] due to risk of classification error tending to produce attenuated estimates (biased towards zero) and standard errors for the effect of latent class membership on distal outcomes of interest [4, 9].
In our examination of distal outcomes, we therefore used a three-step approach which can account for classification error [8]. This is achieved by identifying the best fitting LCA model and saving the posterior probabilities and modal class assignment for that model. Classification errors for individuals are then computed, and the inverse logits of those individual-level error rates are used as weights. The reweighted data are then used as observed data to estimate associations with distal outcomes of interest [2, 3].
Confounders
Potential confounders of the association between social status measures and MHSU, between social status measures and discrimination, and between discrimination and MHSU included age (recorded in APMS in 10 year age bands (16–24, 25–34, 35–44, 45–54, 55–64, 65–74, 75 +), marital status (single, married/civil partnered/cohabiting, separated/divorced/widowed), a binary variable to indicate urban/rural residence, and area-level deprivation quintile (Index of Multiple Deprivation, IMD) [23].
Discrimination
APMS asked participants if they had been treated unfairly in the past year because of age, sex, ethnicity, religion, sexual orientation, physical health, or mental health. To explore whether discrimination attributable to multiple social statuses was related to mental health service use, we developed a binary indicator of past-year unfair treatment for any reason (no/yes) rather than restricting analyses to a single attribution [6].
Statistical analyses
Using MPlus [42], optimal latent class models were developed for men and women. We selected the optimal number of classes using a series of goodness of fit (GoF) statistics: Akaike's information criteria (AIC) [1], sample-size-adjusted Bayesian information criteria (SSABIC) [55], and the Lo–Mendell–Rubin-Adjusted likelihood ratio test (LMRA–LRT) [34]. Lower values for these indicate a better fit. Entropy measures accuracy of classification for an individual participant with higher values indicative of better classification [53]. To distinguish between classes with similar GoF statistics, the LMRA–LRT p values were assessed, with significance indicative of good fit. Finally, parsimony and interpretability were considered in deciding the optimal number of classes [43].
Next, logistic regression analyses were used to explore associations between (i) single social status characteristics and any past-year discrimination (considered to be a mental health stressor, [21], and (ii) intersectional latent class groups and any past-year discrimination. We present unadjusted and adjusted odds ratios (OR/AOR) with 95% confidence intervals (CI). Adjustments were made for all socio-demographic/economic characteristics: age, marital status, urban/rural residence, area-level deprivation.
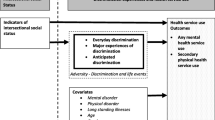
Finally, a series of multivariable logistic regression models were estimated to examine associations between (i) single social statuses and MHSU/treatment and (ii) intersectional status (latent classes) and MHSU/treatment (incorporating the three-step approach discussed above). OR/AORs and 95% CIs for the following models are presented, in which additional variables were sequentially added in the order described: (1) unadjusted; and adjusted for: (2) socio-demographic/economic confounders (including as appropriate: age, gender, marital status, urban/rural residence, area-level deprivation, ethnicity, social class, employment status, migration status, sexual orientation, educational attainment); (3) past-year discrimination; (4) CIS-R symptom severity and (5) self-reported general health, physical illness and social functioning (see Fig. 1).

Directed acyclic graph to illustration the relationships modelled in our analysis
Acknowledging the limitations of mediation analysis using cross-sectional data, evidence for mediation by discrimination was putatively indicated if discrimination was associated with single or intersectional social statuses and with MHSU/treatment, and adjustments for discrimination attenuated associations between status and MHSU/treatment (Kenny n.d.). Analyses accounted for study design including strata, clustering and survey weights.
Results
Intersectional social statuses—Latent Class Analysis (LCA)
Initially, five-class solutions were selected as optimal for both men and women (see Supplementary file). We found almost identical classes and similar patterns of findings for both samples. However, stratifying by gender led to low numbers for some classes. This was particularly noticeable for the male sample which is both smaller than the female sample and has lower engagement with mental health services. We therefore decided to conduct analyses using the full sample and including gender as an indicator for the latent class model. We found the same class composition overall as in the separate models for men and women.
The classes in our final model (Table 1) were characterised as predominantly: (1) Employed White British, educated to degree level and belonging to the managerial/professional NS-SEC category (designated most privileged) (23.7% of the sample). (2) Employed White British, educated below degree level and belonging to the routine/manual NS-SEC category, this class contains the most men (26.4%); (3) Primarily non-working migrants, of varied ethnicity and education (4.6%), this class contains the most women; (4) Employed migrants, of varied ethnicity, social class and education level (6.9%), this class contains more highly educated and economically active participants than LCA3; and (5) Retired White British (38.3%). There was not much variation between classes in conditional probabilities of being either female or a sexual minority.
Discrimination and social status
Our first and second hypotheses relating to elevated discrimination and MHSU/treatment among disadvantaged social groups and to differential patterns for single versus multiple social status analyses, were partially supported by our findings.
Single status modelling
Following adjustments for relevant socio-demographic/economic variables, there were significantly greater odds of past-year discrimination among those aged 16–24 years than older age groups, sexual minority compared to heterosexual participants, ethnic minority (particularly of Black ethnicity) compared to White British participants, migrants versus non-migrants, economically inactive compared to employed people, and those with degree-level educational attainment, compared to those with no qualifications (Table 2).
Intersectional analysis modelling
Intersectional analyses indicated that, after adjusting for additional socio-demographic confounders not included in the LCA models (age, marital status, urban/rural residence and area-level deprivation), the ‘Employed migrant’ (AOR 2.14, CI 1.57–2.92) and ‘Retired White British’ (AOR 1.37, CI 1.04–1.81) groups had greater odds of reporting past-year discrimination compared to the most privileged group (Table 3).
Mental health service use/treatment and social status
As illustrated in Table 4, all markers of need and past-year discrimination were positively associated with MHSU/treatment.
Single status modelling
Following adjustments for socio-demographic/economic variables, additional adjustments for need fully or partially attenuated positive associations between MHSU/treatment and minority sexual orientation, migrant status, being unemployed and greater deprivation. There remained elevated MHSU/treatment among females compared to males (AOR 1.71, CI 1.45–2.02), those who were economically inactive (AOR 2.02, CI 1.05–3.90), sexual minority (AOR 1.65, CI 1.09–2.50), and those living in the most deprived quintile (AOR 1.33, CI 1.02–1.74) compared to the most advantaged group. Those identifying as any Black ethnic group had lower odds of MHSU/treatment compared to White British participants, and adjustments for need strengthened rather than attenuated this negative association (AOR 0.36, CI 0.20–0.66).
Intersectional analysis modelling
Using the typology generated by latent class analyses (Table 5) in models adjusted for remaining socio-demographic/economic variables, compared to the most privileged White British group, the ‘Non-working migrants’ and ‘Retired White British’ had greater odds of MHSU/treatment, while the ‘Employed migrants’ had lower odds. Adjustments for need accounted for the association for ‘Non-working migrants’ (fully accounted for by common mental disorder symptoms), and partially accounted for the association for the ‘Retired White British’ group, though this remained significant (AOR 1.88, CI 1.53–2.32). Adjustments for need had little impact on the negative association with MHSU/treatment observed for ‘Employed migrants’ (AOR 0.39, CI 0.27–0.55).
Discrimination and mental health service use/treatment
Our third and fourth hypotheses, that accounting for past-year discrimination would attenuate associations with MHSU/treatment, and that the influence of discrimination on MHSU/treatment would be greater for people with multiple disadvantaged social statuses, were in general not supported by our findings.
Single status modelling
Adjustments for discrimination had little or no influence on effect sizes for most single status groups (Table 4). However, for sexual minorities relative to heterosexuals, the association became non-significant after adjustment (AOR 1.50, CI 0.99–2.28), indicating discrimination partly accounted for some of the elevated MHSU/treatment in this group. In contrast, a positive association with MHSU/treatment emerged for those aged 35–44 years compared to the youngest age group (AOR 1.58, CI 1.03–2.41).
Intersectional analysis modelling
In intersectional analyses, adjustments for discrimination had no influence on respectively positive and negative associations with MHSU/treatment for the ‘Retired White British’ and ‘Employed migrants’ groups despite finding significantly greater odds of discrimination in these same two groups (Tables 3, 5).
Discussion
Using population-level data, we examined experiences of past-year discrimination, mental health service use (MHSU) and treatment. Controlling for need, we compared patterns across single and intersectional social statuses (using latent class analysis) and examined the influence of discrimination on MHSU/treatment. Analyses revealed different patterns of discrimination and MHSU/treatment when examining single or intersectional social groups. Single status analyses identified characteristics (e.g., being a sexual minority, Black or female) associated with MHSU/treatment (and discrimination) that were not distinctive markers of intersecting class membership in the data-driven models, and therefore were not highlighted by our intersectional approach. Intersectional analyses also detected patterns not observed by single statuses, finding the “Retired White British” group had greater odds and “Employed migrants” lower odds of MHSU/treatment following adjustments for need. Though discrimination was associated with certain social statuses and with greater MHSU/treatment, there was little evidence that it acted as a mediator in either analytic approach.
Examining single versus multiple social statuses
Our findings support the importance of multiple approaches to understanding complexities of social stratification and support prior research identifying differences in mental health and healthcare at the junctures of different social identities [21, 59]. While the variables included in LCA analyses were theoretically considered in relation to salient social stratification categorisations, the data-driven approach allows examination of classes which commonly occur in the population of interest (and are thus sensitive to context). This may mask important inequalities among less frequent classes within the populations and/or who are underrepresented in surveys (e.g., UK-born ethnic minorities). Complimentary analyses could examine a priori defined dyads or triads of social status depending on the research focus.
There are other ways of tailoring analyses to the research question or conceptualisation of intersectionality. For instance, in using LCA, our study took an ‘intercategorical’ approach, looking at dimensions across categories of social status [35]. Therefore, individuals classified, for example, as ‘non-working migrants’ were placed at the intersection of employment and migration status, but in a way that reduces these heterogeneous experiences into a single dimension for measurement. While this may be helpful for public health professionals to have a more nuanced picture of inequities in the population, those interested in understanding the experiences of people occupying particular intersections of social status (perhaps selected on the basis of intercategorical findings) may prefer to conduct ‘intracategorical’ analyses, which lend themselves more to qualitative approaches [35]. Nonetheless, it is important to move beyond describing patterns and emphasise understanding how the experience of intersecting identities might affect mental health and service use. This paper has been able to achieve this by not just using LCA to identify homogeneous patterns of intersectionality that occur within the data, but also examine how people with similar intersectional profiles engage with health services. Future work can build on this by taking a more targeting approach, possibly with the use of coded intersections and/or multilevel modelling to establish whether specific combinations of characteristics drive inequalities more than others.
Social status and MHSU/treatment
After accounting for need, MHSU/treatment was elevated among females, sexual minorities, economically inactive and participants living in the most deprived areas in single status analyses, but lower among Black participants. This reflects previously reported findings [39] and the wider literature (e.g., [54]. Our study extends this to indicate how MHSU/treatment among intersectional social groups common in the population compare to the most privileged (multiply advantaged) group.
MHSU/treatment was elevated for the ‘Retired White British’ latent class but was significantly lower for the ‘Employed migrants’ group. Being retired was not associated with MHSU/treatment in single status analyses, thus our intersectional findings for this class were not expected. This latent class was the largest, reflecting that White British make up the majority of the population in England and retirement is proportionately more common in this group given its older age profile compared to other racial/ethnic groups (ONS 2011).
Residual confounding by need
Elevated MHSU/treatment may be partly due to residual confounding by mental health: our measure of common mental disorders reflects current mental health (in the past two weeks) while MHSU/treatment referred to the past year. Therefore, given the relapsing–remitting nature of symptoms of anxiety and depression, it may not adequately capture people’s mental health during that time. However, this caveat would have also held for other intersectional groups with initially elevated MHSU/treatment (the ‘Non-working migrants’ group), for whom adjustments for mental health completely attenuated the association.
Similarly, although the lower odds of MHSU/treatment in the ‘Employed migrants’ group remained despite adjustments for differences in age and need, there may be some residual confounding by need reflective of a ‘healthy migrant effect’ that would not necessarily have been observed for the ‘Non-working migrants’ group, which had greater levels of economic activity.
Opportunity costs
Greater MHSU/treatment among the ‘Retired White British’ group may also reflect lower opportunity costs (e.g., lack of work commitments, greater leisure time) associated with seeking help, as has been reported previously for healthcare utilisation among retirees more generally [66]. Opportunity costs may also have influenced lower MHSU/treatment among the ‘Employed migrants’ group (comprising predominantly White Other and to a lesser extent Asian ethnic groups). This group had a greater conditional probability of having degree-level education than the retired or lower social class White British group, yet, it was heterogeneous in terms of occupational social class. This reflects UK statistics that migrants are more likely to experience downward social mobility, working in jobs for which they are overqualified, which is associated with poorer mental health [15]. This is particularly the case for those from recent European Union (EU) accession countries (included in the White Other category) who are more likely to be in low-skilled occupations than migrants from India, East, and Southeast Asia (Migration [41] and more likely to have non-standard work (e.g., temporary/short/part-time/daily work) [19]. Such occupational circumstances may be less flexible and accrue greater opportunity costs to seeking healthcare [62].
This explanation is undermined by the discrepancy found between the ‘Employed White British, low social class’ and the ‘Employed migrants’ group. The lower social class White British group had a greater probability of routine/manual skilled work (potentially less flexible, with higher opportunity costs of help-seeking) and lower education than the employed migrants group; yet, they did not have significantly different odds of MHSU/treatment. However, in support of the opportunity cost explanation, the ‘Employed migrants’ group comprised a mix of occupational social classes with a greater conditional probability of being managerial/professional than the lower social class employed White British group. Further, this ‘Employed migrants’ group may more commonly comprise self-employed people [12], accruing greater opportunity costs in terms of seeking mental health care than those working in more standard employment, thus partially explaining lower MHSU/treatment.
Unmeasured confounders: social integration and networks
Finally, length of residence may be an important unmeasured confounder for the migrant groups. Compared to the ‘Non-working migrants’ group, the ‘Employed migrants’ group is likely to include a greater proportion of more recently arrived migrants [20]. Previous UK evidence indicates that more recent (but not longer-resident) migrants had lower odds of being registered with a GP, particularly White migrants and those who migrated for work [20]. Lower MHSU/treatment in the employed migrant group may thus reflect lack of integration into the healthcare system and lack of access to treatment—particularly since this is predominantly gatekept by primary care. They may also be less familiar with services available which could limit opportunities for self-referral, or have concerns about seeking out help which act as a barrier to care. For example, Polling et al. [51] found that (among an ethnically diverse UK sample), often those who require support or health services do not seek help because they anticipated being treated unfairly, cultural insensitivity of care or concerns that they will be brought to the attention of other authorities.
Influence of discrimination on mental health service use
As with MHSU/treatment, observed patterns of discrimination differ when considering social status singly or intersectionally. Past-year discrimination was positively associated with specific disadvantaged single social statuses and was significantly elevated in the two intersectional classes associated MHSU/treatment (‘Retired White British’ and ‘Employed migrants’), but not—as might be expected—in the multiply disadvantaged ‘Non-working migrants’ group. Previous research has identified higher odds of discrimination among White Other compared to White British groups, particularly for more recent migrants [26], though the findings for the ‘Retired White British’ group were less expected. While we did not examine attributions, it is possible that discrimination on the basis of age was more common in this latter group.
However, while discrimination predicted greater MHSU/treatment, adjustments for discrimination had little or no influence on associations MHSU/treatment in either single (except sexual orientation) or intersectional status analyses. This contrasts with previous findings [21, 24] though these studies were able to examine different forms of discrimination which may explain the discrepancy. For example, anticipated, but not everyday or major experiences of discrimination was associated with increased MHSU/treatment in analyses adjusting for intersectional social status and need [21]. Also, while a recent review indicates that racism predicts poorer satisfaction, reduced trust, and possibly delayed access to services, it may not predict health service use [7]. Further work may therefore usefully examine whether discrimination has differential effects on different aspects of service use (e.g., delayed treatment, adherence, treatment pathways) for multiply disadvantaged groups. Finally, only a small proportion of APMS participants disclosed their experiences of discrimination. Though underreporting may not be unexpected in such surveys, there may be differences in likelihood to disclose different discrimination types (e.g., ageism, sexism, racism).
Additional qualitative or policy development work to improve MHSU could be achieved is by identifying people that have key intersecting characteristics defined by the model. For example, recruiting heterosexual, White British people who are educated to degree level and are employed in senior roles would reflect latent class 1, while recruiting economically inactive/retired migrants from a variety of ethnic minority groups would reflect latent class 3.
Strengths and limitations
Key strengths of this study are its use of national-level data representative of households in England building on an approach previously used in a regional UK sample. Also, our approach to identifying inequalities in MHSU/treatment moves beyond single status analyses to incorporate an intersectional approach using LCA which identifies common intersectional classes in the population and picks up patterns not visible in single status analyses alone—though LCA can sometimes focus on certain categories and ignore others, which is a limitation of quantitative explorations of intersectionality [16]. Our approach is one approach to examining intersectionality, specifically identifying latent classes present in the population in terms of probability of belonging to potentially marginalised social statuses and contrasting exposure to discrimination (a form of oppression) outcomes across groups classified as multiply advantaged, disadvantaged or a mix of advantaged and disadvantaged, and thus with differing positions in terms of social power, and differing ‘vulnerability’ to health inequalities (e.g., [36]. We agree that this differs from examining the experiences of individuals/groups at the intersections of two or more social statuses but consider our approach to add (although partially and incrementally) to our understanding of how experiences are distributed in the population beyond examining single social statuses at a time. A further strength is that we move beyond describing inequities to examine discrimination as a potential underpinning mechanism driving such inequalities.
The main limitation of this study is our use of a binary measure of discrimination. This was necessary due to low n and the limited nature of the discrimination measures in APMS, though this does underestimates the complexity of experienced discrimination in patterning health outcomes. Similarly, it was also necessary to dichotomise sexual orientation due to low n, potentially obscuring findings from specific orientation. APMS is also a survey of private households, thus excluding individuals living in institutions or who are homeless (though there are small groups of APMS participants who have experienced homelessness) who may be more likely to experience poor mental health and less likely to receive help. Furthermore, as data were cross-sectional, mediation by discrimination could not have been causally inferred due to the concurrent temporal reporting. Also, although this is a national sample, participant numbers in some racial/ethnic minority groups were small. This may have impacted on sample size/inferences, exemplifying the need for surveys to implement ethnic minority booster samples. Finally, although a pervasive adversity, the measures of discrimination used here did not directly enquire about fear of discrimination from mental health services, and thus may not have adequately captured underpinning mechanisms relevant to MHSU/treatment.
Conclusion
Patterns of both MHSU/treatment and discrimination differ when considering single and multiple statuses, highlighting how both approaches each identify inequities that may not otherwise have been apparent. There is little evidence that our measure of discrimination affects associations between social status and MHSU/treatment. However, to improve understanding and inform action on social status-based inequalities, further research should incorporate multiple and mixed-methods approaches to identify and characterise the complexities of social stratification processes, examine different dimensions of inequalities in mental health problems and care, different health service delivery contexts, as well as different and more specific aspects of discrimination.
References
Akaike H (1987) Factor Analysis and AIC. Selected papers of hirotugu akaike. Springer, New York, pp 371–386
Asparouhov T, Muthén B (2014) Auxiliary variables in mixture modeling: three-step approaches using M Plus. Struct Equ Modeling 21(3):329–341
Asparouhov T, Muthén B (2014) Auxiliary variables in mixture modeling: using the BCH method in mplus to estimate a distal outcome model and an arbitrary secondary model. Mplus Web Notes 21(2):1–22
Bakk Z, Tekle FB, Vermunt JK (2013) Estimating the association between latent class membership and external variables using bias-adjusted three-step approaches. Sociol Methodol 43(1):272–311
Bauer GR (2014) Incorporating intersectionality theory into population health research methodology: challenges and the potential to advance health equity. Soc Sci Med 110:10–17
Bauer GR, Scheim AI (2019) Methods for analytic intercategorical intersectionality in quantitative research: discrimination as a mediator of health inequalities. Soc Sci Med 226:236–245
Ben J, Cormack D, Harris R, Paradies Y (2017) Racism and health service utilisation: a systematic review and meta-analysis. PLoS ONE 12(12):e0189900
Bolck A, Croon M, Hagenaars J (2004) Estimating latent structure models with categorical variables: one-step versus three-step estimators. Polit Anal 12(1):3–27
Bray BC, Lanza ST, Tan X (2015) Eliminating bias in classify-analyze approaches for latent class analysis. Struct Equ Modeling 22(1):1–11
Budge SL, Thai JL, Tebbe EA, Howard KAS (2016) The intersection of race, sexual orientation, socioeconomic status, trans identity, and mental health outcomes. Couns Psychol 44:1025–1049
Cho S, Crenshaw KW, McCall L (2013) Toward a field of intersectionality studies: theory, applications, and praxis. Signs J Women Culture Soc 38(4):785–810
Clark K, Drinkwater S, Robinson C (2016) Self-employment amongst migrant groups: new evidence from in England and Wales. Small Bus Econ
Clement S, Schauman O, Graham T, Maggioni F, Evans-Lacko S, Bezborodovs N, Morgan C, Rüsch N, Brown JSL, Thornicroft G (2015) What is the impact of mental health-related stigma on help-seeking? A systematic review of quantitative and qualitative studies. Psychol Med 45(1):11–27
Crenshaw K (1989) Demarginalizing the intersection of race and sex: a black feminist critique of antidiscrimination doctrine, feminist theory and antiracist politics. Univ Chic Leg Forum 1989(1):139–167
Das-Munshi J, Leavey G, Stansfeld SA, Prince MJ (2012) Migration, social mobility and common mental disorders: critical review of the literature and meta-analysis. Ethn Health 17(1–2):17–53. https://doi.org/10.1080/13557858.2011.632816
Dietze G, Yekani EH, Michaelis B (2018) Modes of being vs. categories: queering the tools of intersectionality. Beyond gender. Routledge, London, pp 117–136
Evans CR (2019) Reintegrating contexts into quantitative intersectional analyses of health inequalities. Health Place 60:102214
Evans-Lacko S, Aguilar-Gaxiola S, Al-Hamzawi A, Alonso J, Benjet C, Bruffaerts R, Chiu WT, Florescu S, De Girolamo G, Gureje O (2018) Socio-economic variations in the mental health treatment gap for people with anxiety, mood, and substance use disorders: results from the WHO World Mental Health (WMH) Surveys. Psychol Med 48(9):1560–1571
Fernández-Reino, M., & Rienzo, C. (2019). Migrants in the UK labour market: an overview. The Migration Observatory Briefing, 1–8. http://storage0.dms.mpinteractiv.ro/media/1/186/3927/10538667/2/briefing-migrants-the-uk-labour-market-0.pdf
Gazard B, Frissa S, Nellums L, Hotopf M, Hatch SL (2015) Challenges in researching migration status, health and health service use: an intersectional analysis of a South London community. Ethn Health 20(6):564–593
Gazard B, Chui Z, Harber-Aschan L, MacCrimmon S, Bakolis I, Rimes K, Hotopf M, Hatch SL (2018) Barrier or Stressor? The role of discrimination experiences in health service use. BMC Public Health 18(1):1354
Goodwin L, Gazard B, Aschan L, MacCrimmon S, Hotopf M, Hatch SL (2018) Taking an intersectional approach to define latent classes of socioeconomic status, ethnicity and migration status for psychiatric epidemiological research. Epidemiol Psychiatric Sci 27(6):589–600
Gov.UK 2015. ‘English Indices of Deprivation 2015’. https://www.gov.uk/government/statistics/english-indices-of-deprivation-2015. Accessed 20 Aug 2020
Grollman EA (2014) Multiple disadvantaged statuses and health: the role of multiple forms of discrimination. J Health Soc Behav 55(1):3–19
Hahm HC, Cook BL, Ault-Brutus A, Alegría M (2015) Intersection of race-ethnicity and gender in depression care: screening, access, and minimally adequate treatment. Psychiatr Serv 66(3):258–264
Hatch SL, Gazard B, Williams DR, Frissa S, Goodwin L, Hotopf M (2016) Discrimination and common mental disorder among migrant and ethnic groups: findings from a south east london community sample. Soc Psychiatry Psychiatr Epidemiol 51(5):689–701
Kapadia D, Nazroo J, Tranmer M (2018) Ethnic differences in women’s use of mental health services: do social networks play a role? Findings from a national survey. Ethn Health 23(3):293–306
Kenny D (n.d.) ‘Mediation (David A. Kenny)’. http://davidakenny.net/cm/mediate.htm. Accessed 26 Nov 2020
Kohn R, Saxena S, Levav I, Saraceno B (2004) The treatment gap in mental health care. Bull World Health Organ 82:858–866
Lasalvia A, Zoppei S, Van Bortel T, Bonetto C, Cristofalo D, Wahlbeck K, Bacle SV, Van Audenhove C, Van Weeghel J, Reneses B (2013) Global pattern of experienced and anticipated discrimination reported by people with major depressive disorder: a cross-sectional survey. Lancet 381(9860):55–62
Lewis G, Pelosi AJ, Araya R, Dunn G (1992) Measuring psychiatric disorder in the community: a standardized assessment for use by lay interviewers. Psychol Med 22(2):465–486
Lewis TT, Van Dyke ME (2018) Discrimination and the Health of African Americans: The Potential Importance Of Intersectionalities. Curr Dir Psychol Sci 27(3):176–182
Link BG, Phelan JC (2001) Conceptualizing stigma. Ann Rev Sociol 27(1):363–385
Lo Y, Mendell NR, Rubin DB (2001) Testing the number of components in a normal mixture. Biometrika 88(3):767–778
McCall L (2008) The Complexity of Intersectionality. Intersectionality and beyond. Routledge, London, pp 65–92
McLeod JD (2015) Why and how inequality matters. J Health Soc Behav 56(2):149–165
McLeod JD, Lively KJ (2007) Social Psychology and stress research. Mental health, social mirror. Springer, New York, pp 275–303
McManus S, Bebbington PE, Jenkins R, Morgan Z, Brown L, Collinson D, Brugha T (2019) Data resource profile: adult psychiatric morbidity survey (APMS). Int J Epidemiol. https://doi.org/10.1093/ije/dyz224
McManus S, Bebbington P, Jenkins R, Brugha T (2016) ‘Mental Health and Wellbeing in England: Adult Psychiatric Morbidity Survey 2014. A Survey Carried out for NHS Digital by NatCen Social Research and the Department of Health Sciences, University of Leicester’. https://files.digital.nhs.uk/pdf/q/3/mental_health_and_wellbeing_in_england_full_report.pdf. Retrieved 21 Jan 2020
McManus S, Gunnell D, Cooper C, Bebbington PE, Howard LM, Brugha T, Jenkins R, Hassiotis A, Weich S, Appleby L (2019) Prevalence of non-suicidal self-harm and service contact in England, 2000–14: repeated cross-sectional surveys of the general population. Lancet Psychiatry 6(7):573–581
Migration Observatory (2019) ‘Migrants in the UK Labour Market: an overview’. Migration Observatory. https://migrationobservatory.ox.ac.uk/resources/briefings/migrants-in-the-uk-labour-market-an-overview/. Accessed 27 Jan 2020
Muthén LK, Muthén BO (2012) Mplus. Comprehensive Modelling Program for Applied Researchers: User’s Guide. Los Angeles, CA
Nylund KL, Asparouhov T, Muthén BO (2007) Deciding on the number of classes in latent class analysis and growth mixture modeling: a Monte Carlo Simulation Study. Struct Equ Modeling 14(4):535–569
Nylund-Gibson K, Grimm RP, Masyn KE (2019) Prediction from latent classes: a demonstration of different approaches to include distal outcomes in mixture models. Struct Equ Model Multidiscip J 26:1–19
Office for National Statistics (ONS) (2011) 2011 Census analysis: Ethnicity and the Labour Market, England and Wales. https://www.ons.gov.uk/peoplepopulationandcommunity/culturalidentity/ethnicity/articles/ethnicityandthelabourmarket2011censusenglandandwales/2014-11-13. Accessed 20 Aug 2020
Office for National Statistics (ONS) (2019) ‘The National Statistics Socio-Economic Classification (NS-SEC)—Office for National Statistics’. https://www.ons.gov.uk/methodology/classificationsandstandards/otherclassifications/thenationalstatisticssocioeconomicclassificationnssecrebasedonsoc2010. Accessed 27 Jan 2020
Pearlin LI (1989) The sociological study of stress. J Health Soc Behav 30:241–256
Pearlin LI (1999) The stress process revisited. Handbook of the sociology of mental health. Springer, New York, pp 395–415
Pearlin LI, Menaghan EG, Lieberman MA, Mullan JT (1981) The stress process. J Health Soc Behav 22:337–356
Perry BL, Harp KLH, Oser CB (2013) Racial and gender discrimination in the stress process: implications for African American Women’s Health and Well-Being. Sociol Perspect 56(1):25–48
Polling C, Woodhead C, Harwood H, Hotopf M, Hatch SL (2020) “There is so much more for us to lose if we were to kill ourselves”: understanding paradoxically low rates of self-harm in a socioeconomically disadvantaged community in London. Qual Health Res 31:122–136 (Doi: 1049732320957628)
Prins M, Meadows G, Bobevski I, Graham A, Verhaak P, van der Meer K, Penninx B, Bensing J (2011) Perceived need for mental health care and barriers to care in the Netherlands and Australia. Soc Psychiatry Psychiatr Epidemiol 46(10):1033–1044
Ramaswamy V, DeSarbo WS, Reibstein DJ, Robinson WT (1993) An empirical pooling approach for estimating marketing mix elasticities with PIMS data. Mark Sci 12(1):103–124
Roberts T, Esponda GM, Krupchanka D, Shidhaye R, Patel V, Rathod S (2018) Factors associated with health service utilisation for common mental disorders: a systematic review. BMC Psychiatry 18(1):262
Sclove SL (1987) Application of model-selection criteria to some problems in multivariate analysis. Psychometrika 52(3):333–343
Sue DW, Capodilupo CM, Torino GC, Bucceri JM, Holder A, Nadal KL, Esquilin M (2007) Racial microaggressions in everyday life: implications for clinical practice. Am Psychol 62(4):271
Thoits PA (2013) Self, identity, stress, and mental health. Handbook of the sociology of mental health. Springer, New York, pp 357–377
Thornicroft G (2008) Stigma and discrimination limit access to mental health care. Epidemiol Psychiat Sci 17(1):14–19
Trygg NF, Gustafsson PE, Månsdotter A (2019) Languishing in the crossroad? A scoping review of intersectional inequalities in mental health. Int J Equity Health 18(1):115
Turan JM, Elafros MA, Logie CH, Banik S, Turan B, Crockett KB, Pescosolido B, Murray SM (2019) Challenges and opportunities in examining and addressing intersectional stigma and health. BMC Med 17(1):7
Tyrer P, Nur U, Crawford M, Karlsen S, MacLean C, Rao B, Johnson T (2005) The Social Functioning Questionnaire: a rapid and robust measure of perceived functioning. Int J Soc Psychiatry 51(3):265–275
Virtanen P, Kivimäki M, Vahtera J, Koskenvuo M (2006) Employment status and differences in the one-year coverage of physician visits: different needs or unequal access to services? BMC Health Serv Res 6(1):123
Wallace S, Nazroo J, Bécares L (2016) Cumulative effect of racial discrimination on the mental health of ethnic minorities in the United Kingdom. Am J Public Health 106(7):1294–1300
Williams DR, Kontos EZ, Viswanath K, Haas JS, Lathan CS, MacConaill LE, Chen J, Ayanian JZ (2012) Integrating multiple social statuses in health disparities research: the case of lung cancer. Health Serv Res 47(32):1255–1277
Williams DR, Yan Yu, Jackson JS, Anderson NB (1997) Racial differences in physical and mental health: socio-economic status, stress and discrimination. J Health Psychol 2(3):335–351
Zhang Y, Salm M, van Soest A (2018) The effect of retirement on healthcare utilization: Evidence from China. J Health Econ 62:165–177
Funding
This work was supported by the Wellcome Trust [203380/Z/16/Z] and the National Institute for Health Research (NIHR) Biomedical Research Centre at South London and Maudsley NHS Foundation Trust and King’s College London. CW and SH are supported by the Economic and Social Research Council (ESRC) Centre for Society and Mental Health at King’s College London (ESRC Reference: ES/S012567/1). JD is part supported by the ESRC Centre for Society and Mental Health at King’s College London (ESRC Reference: ES/S012567/1), grants from the ESRC (ES/S002715/1), by the Health Foundation working together with the Academy of Medical Sciences, for a Clinician Scientist Fellowship, and by the National Institute for Health Research (NIHR) Biomedical Research Centre at South London and Maudsley NHS Foundation Trust and King's College London and the National Institute for Health Research (NIHR) Applied Research Collaboration South London (NIHR ARC South London) at King’s College Hospital NHS Foundation Trust. GA is supported by an ESRC PhD studentship, via the London Interdisciplinary Social Science Doctoral Training Partnership, (ESRC reference: ES/P000703/1). SM is supported by the UKRI (MR-VO49879/1). The views expressed are those of the authors and not necessarily those of the funders. The funders did not have a role in the study design; collection, analysis, or interpretation of data; the writing of the manuscript; or in the decision to submit the manuscript for publication.
Author information
Authors and Affiliations
Contributions
SH oversaw the production of this article. RR conducted the statistical analysis supervised by CW. CW and RR wrote the article. SM provided guidance on use of the data. GA and JD provided insight into the topic area. All authors provided critical feedback on the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The author declares that they have no conflict of interest.
Ethical statement
This study received ethical approval from King’s College London Research Ethics Committee for Psychiatry, Nursing and Midwifery (REC reference: HR-17/18-4629—IRAS project ID: 230692). It also received approval from South London and Maudsley NHS Foundation Trust and was approved by the CRIS Oversight Committee.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Rhead, R.D., Woodhead, C., Ahmad, G. et al. A comparison of single and intersectional social identities associated with discrimination and mental health service use: data from the 2014 Adult Psychiatric Morbidity Survey in England. Soc Psychiatry Psychiatr Epidemiol 57, 2049–2063 (2022). https://doi.org/10.1007/s00127-022-02259-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00127-022-02259-1