
Abstract
Purpose
The aim of this study was to assess whether coaching doctors to enhance ethical decision-making in teams improves (1) goal-oriented care operationalized via written do-not-intubate and do-not attempt cardiopulmonary resuscitation (DNI-DNACPR) orders in adult patients potentially receiving excessive treatment (PET) during their first hospital stay and (2) the quality of the ethical climate.
Methods
We carried out a stepped-wedge cluster randomized controlled trial in the medical intensive care unit (ICU) and 9 referring internal medicine departments of Ghent University Hospital between February 2022 and February 2023. Doctors and nurses in charge of hospitalized patients filled out the ethical decision-making climate questionnaire (ethical decision-making climate questionnaire, EDMCQ) before and after the study, and anonymously identified PET via an electronic alert during the entire study period. All departments were randomly assigned to a 4-month coaching. At least one month of coaching was compared to less than one month coaching and usual care. The first primary endpoint was the incidence of written DNI-DNACPR decisions. The second primary endpoint was the EDMCQ before and after the study period. Because clinicians identified less PET than required to detect a difference in written DNI-DNACPR decisions, a post-hoc analysis on the overall population was performed. To reduce type I errors, we further restricted the analysis to one of our predefined secondary endpoints (mortality up to 1 year).
Results
Of the 442 and 423 clinicians working before and after the study period, respectively 270 (61%) and 261 (61.7%) filled out the EDMCQ. Fifty of the 93 (53.7%) doctors participated in the coaching for a mean (standard deviation [SD]) of 4.36 (2.55) sessions. Of the 7254 patients, 125 (1.7%) were identified as PET, with 16 missing outcome data. Twenty-six of the PET and 624 of the overall population already had a written DNI-DNACPR decision at study entry, resulting in 83 and 6614 patients who were included in the main and post hoc analysis, respectively. The estimated incidence of written DNI-DNACPR decisions in the intervention vs. control arm was, respectively, 29.7% vs. 19.6% (odds ratio 4.24, 95% confidence interval 4.21–4.27; P < 0.001) in PET and 3.4% vs. 1.9% (1.65, 1.12–2.43; P = 0.011) in the overall study population. The estimated mortality at one year was respectively 85% vs. 83.7% (hazard ratio 2.76, 1.26–6.04; P = 0.011) and 14.5% vs. 15.1% (0.89, 0.72–1.09; P = 0.251). The mean difference in EDMCQ before and after the study period was 0.02 points (− 0.18 to 0.23; P = 0.815).
Conclusion
This study suggests that coaching doctors regarding ethical decision-making in teams safely improves goal-oriented care operationalized via written DNI-DNACPR decisions in hospitalized patients, however without concomitantly improving the quality of the ethical climate.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Coaching doctors regarding ethical decision making in teams may improve goal-oriented care operationalized via written do-not-intubate and do-not attempt cardiopulmonary resuscitation orders. |
Introduction
Fast medical progress and technological innovation pose a significant challenge to doctors, who are asked to find the delicate balance between life-prolonging treatment and palliative care [1,2,3]. Although the medical community continues to put tremendous efforts in trying to enhance prognostication via objective and thus universal factors or scoring systems [4], literature highlights a large variability in written do-not-intubate and do-not attempt cardiopulmonary resuscitation (DNI-DNACPR) decisions, use of health care resources at end-of-life, referral to the intensive care unit (ICU), palliative care and place of death across continents, countries, hospitals, wards, doctors and patients [5,6,7,8,9,10,11,12,13,14]. This indicates that organizational [10, 15, 16] but also subjective factors at the continent and country (“culture”), team (“climate”) and personal (“style”) level exert a greater influence than objective factors in medical ethical decision-making [10, 15,16,17,18,19,20]. However, subjective factors are rarely acknowledged by clinicians, more specifically by doctors at the bedside [20,21,22,23,24].
Becoming aware of one’s personal underlying emotions (self-reflection) that are inherent to complex medical ethical decisions such as anxiety, powerlessness and guilt, and learning to better cope with these emotions (self-regulation) are thus together with motivation, empathy and social skills (emotional intelligence) [25, 26] essential to guarantee patient-centered care [20,21,22,23,24]. Furthermore, timely sharing of emotions, conflicting ideas, values, knowledge and experience between professionals with different backgrounds within a safe ethical climate may help in reducing prognostic uncertainty in doctors and in stimulating ethical awareness in the team [8, 20, 27,28,29,30,31,32]. For instance, whereas doctors focus more on the proportionality between treatment intensity and estimated prognosis than nurses, nurses acknowledge dignified care [32] and the need for open communication towards patients and relatives sooner than doctors during hospital stay [29]. This collective awareness based on complementary visions enriches the ethical decision-making process for the benefit of the patient and may increase doctors’ self-confidence in effectively communicating and making decisions with regard to immediate or future potentially excessive treatments together with the patient and his or her relatives [8, 20, 27]. Besides mitigating the risk of prolonged suffering and complicated grief among patients and relatives respectively [2, 3, 33, 34], timely and appropriate ethical decision-making within teams may also reduce burnout and intent to leave among clinicians [3, 20, 35,36,37] and the cost for society [3, 38, 39]. However, creating a safe ethical climate which enables nurses and other members of the team to speak up about patient safety concerns [40], more specifically with regard to potentially excessive treatments, requires specific leadership skills [20, 25,26,27, 41,42,43] that are not or insufficiently taught in the medical curriculum [43, 44].
The aim of this study was to assess whether coaching doctors during 4 months in self-reflective and empowering leadership, and in managing team dynamics with regard to ethical decision-making increases the incidence of goal-oriented care operationalized by written DNI-DNACPR decisions in adult patients potentially receiving excessive treatment (PET) during their first hospital stay and the perception of the quality of the ethical climate by clinicians.
Methods
We refer to a previous publication for the detailed study and coaching protocol [20].
Participants
All medical and surgical departments within Ghent University Hospital frequently referring adult (> 18 year old) patients to the ICU were invited to participate in the current study during meetings organized in 2018–2019. Surgical departments did not express the need to improve ethical decision-making in our hospital. All eight internal medicine departments (Cardiology, Gastro-enterology and Hepatology, General Internal Medicine, Geriatrics, Hematology, Medical Oncology, Nephrology, Pulmonology) frequently referring adult patients to the ICU and the Neurology department acknowledged room to improve their ethical decision-making [20] and were thus included in this study together with the medical ICU.
All junior and senior doctors taking care of hospitalized patients in the ten participating departments were eligible for the intervention. Junior doctors were defined as doctors in training. All nurses and doctors were invited to fill out the ethical decision-making climate questionnaire (EDMCQ) [27] before and after the 12 months study period (February 2022 until February 2023) and to identify PET during the study period. In line with a previous study performed in 68 ICUs, PET were defined as patients who were perceived by two or more doctors or nurses as receiving excessive treatment [8]. These patients had a 7% probability of surviving at home with a good quality of life at 1 year [8]. Excessive treatment was defined as treatment that is perceived to be no longer consistent with the expected survival or quality of life (“too much treatment”) or that is perceived as being provided against the patient’s or relatives’ wishes [3, 8]. This definition entails thus potentially futile, non-beneficial, inappropriate or even harmful treatments [3, 45], which has been estimated to be provided to 33–38% of patients near the end-of-life [9], as well as treatments that are potentially being provided without voluntary and informed consent [3]. Only adult patients hospitalized for the first time in the hospital were included in this study. Study data were collected and managed using REDCap electronic data capture tools hosted at the Ghent University Hospital [46].
We refer to Tables 1 and 2 for the baseline characteristics that were collected at the clinician and patient level, respectively.
Study design and randomization
The study followed a stepped wedge cluster randomized trial design, run across the ten different participating departments. All ten departments were randomly assigned to start a 4-month coaching period based on a random number generator in the software R by the statistician. The study was not blinded, however clinicians were asked to not actively inform patients or relatives about the timing of the intervention.
Intervention
The intervention in junior and senior doctors consisted of four components: (1) a single interactive session lasting 2–3 h focusing on the concepts of medical ethical decision-making, the psychological challenge of dealing with ethically sensitive medical topics, and empowering leadership; (2) observation of interdisciplinary team meetings by a first coach who also gave feedback to the doctor in charge to enhance self-reflection on empowering leadership and managing group dynamics during the 4-months intervention period; (3) individual coaching by a second coach, centered on fostering self-reflection and empowering leadership, along with addressing group dynamics concerning ethical decision-making about PET during the four months intervention period. In absence of such cases, the focus shifted to encompass all critical aspects of ethical decision-making pertinent to doctors. Each doctor was invited to participate to at least eight coaching sessions of 1 h during the intervention period, to be extended upon request. Coaching was provided by senior clinical psychologists specialized in systemic psychodynamic coaching. Both coaches received supervision provided by an internationally recognized coaching expert and faculty within this coaching model; (4) throughout the intervention coaches and doctors in charge were informed of the presence of a PET within their ward by an electronic alert. This alert was accessible via the electronic patient data record. Nurses and doctors were instructed to use this CODE alert for each patient under their care in whom they deemed that treatment was excessive. The CODE alert and the study are briefly explained in the video available at https://youtu.be/68TDLdW1vFQ. This video was also used in the multifaceted communication campaign that was held throughout the entire study period to enhance participation and inclusion of PET (supplementary File 1). Progress in self-reflection was surveyed by the second coach.
Primary endpoints and hypotheses
The first primary endpoint in this study was written DNI-DNACPR decision. The second primary endpoint was the EDMCQ. The EDMCQ is a 32-item validated questionnaire [8, 20, 27] that consists of seven domains: factor F1 “self-reflective and empowering leadership of doctors”, F2 “open and interdisciplinary reflection”, F3 “not avoiding end-of-life decisions”, F4 “mutual respect within the interdisciplinary team”, F5 “active involvement of nurses in end-of-life care and decision-making”, F6 “active decision-making by doctors” and F7 “ethical awareness”. For this study, we focused on the 30 EDMCQ items that are also applicable outside the ICU setting. We decided to use two endpoints because ethical sensitive decisions and the climate in which these decisions are taken are intrinsically connected with each other. We hypothesized that the intervention would affect F1, which in turn would affect all other EDMCQ factors and via these, the incidence of written DNI-DNACPR decisions [20].
These primary objectives were formalized in the following hypotheses: (1) the intervention changes the incidence in written DNI-DNACPR decisions in PET from 35% to 50% over the 12-month study period; (2) the intervention increases the mean EDMCQ factor sum-score in clinicians (doctors and nurses) by at least 2.8 points (equals the sum of the differences in the 7 factors between units with “good” and with an “average ethical climate with involvement of nurses at end-of-life” in the DISPROPRICUS study) over the 12-month study period [8, 20].
Power analysis
A Monte Carlo simulation based on a pilot study conducted in 2019 evaluated that 605 PET would be required to detect an increase in written DNI-DNACPR decisions from 35% before to 50% post intervention with 86% power at the 5% significance level [20]. For the change in EDMCQ score after versus before the intervention, a Monte Carlo power evaluation showed that 5 clinicians per department were required to detect an increase with 2.8 points with 93% power at the 5% significance level.
Statistical analysis
The written DNI-DNACPR decision analysis was conducted by logistic mixed effect models with random intercept to account for between-department variability, assuming a constant risk before and after intervention, and a linearly changing risk (0 to 1) during the intervention [20], considering at least 1 month of coaching for an effect. This adjustment captures a potentially time-dependent treatment effect, not explicitly accounted for in the initial protocol, while maintaining balance between the intervention and the control arm. The analysis included patients without a written DNI-DNACPR decision at the time of the first registration, in order to investigate the coaching effect on written DNI-DNACPR incidence during the study period. The change in EDMCQ score was analyzed based on linear mixed effects models including an intervention indicator and a random intercept to account for between-department variability. Survival analysis at 1-year was conducted using stratified cox proportional hazards model by department, while allowing potential variations across departments. Naive models are department-specific adjusted models only including intervention effect as predictor. To evaluate the robustness of our findings, these naive models were additionally adjusted for differences in baseline patients characteristics. Two-sided P-values were calculated.
Because of the small number of PET and subsequent power issues, we decided to perform a post hoc analysis on the overall population of first admissions and to restrict this analysis to the primary endpoints and one of our predefined secondary safety endpoints (mortality up to 1 year) to reduce the risk of type I errors. After the study period, clinicians were surveyed about the reasons for the low identification of PET.
Ethics
This study was conducted according to the Declaration of Helsinki and has been reviewed and approved by the Ethics Committee of the Ghent University Hospital (BC-09828, date of approval May 27th 2021). This committee includes patient representatives.
An electronic and written informed consent was required for clinicians to participate to this study and to the individual coaching sessions, respectively. Informed consent was waived for post-hoc anonymous data on written DNI-DNACPR decisions and mortality provided by the independent Data Science Institute. We asked informed consent to PET to collect survey data on satisfaction and well-being, however, these data were not used because of underpowering.
In line with the models for shared decision making [1, 47], attending doctors in Belgium must obtain voluntary and informed consent for treatment limitation decisions such as DNI-DNACPR from the patient or one of his/her representatives in case of incapacity (“Patients Rights Act” 2002, Article 96).
Results
Of the 93 and 94 doctors, and 349 and 329 nurses working before February 2022 and after February 2023 in the ten departments, respectively 63 (67.7%), 63 (67%), 207 (59.3%) and 198 (60.1%) filled out the EDMCQ, resulting in an overall response rate of 61% and 61.7% (Fig. 1). Thirty-eight doctors and 127 nurses filled out the EDMCQ at both moments, before and after the study period. The characteristics of the departments and clinicians are listed in the supplementary File 2 and Table 1, respectively.

Flowchart. PET patients potentially receiving excessive treatment, DNI-DNACPR do-not-intubate and do-not-attempt-cardiopulmonary resuscitation
Of the 7254 patients hospitalized for the first time during the study period, 125 (1.7%) were identified as PET. In 16 PET outcome data were missing. Twenty-six of the 109 (23.9%) PET and 624 of the 7238 (8.6%) overall study population already had a written DNI-DNACPR decision at study entry, resulting in 83 and 6614 patients who were included in the main and post-hoc analysis, respectively. Randomization at the department level resulted in 37 vs. 46 patients respectively in the intervention vs. control arm for the main analysis and 4012 vs. 2602 for the post hoc analysis. The baseline characteristics of the PET and the overall study population in both arms are listed in Table 2.
The reasons according to the clinicians for having identified less PET than in our pilot study are listed in supplementary File 2. The top five reasons were: fading attention for the study over time (respectively, 53.7% in doctors and 74.7% in nurses), poor visibility of the CODE alert to identify patients in the electronic patient file (34.3% and 50.7%), fear of blaming doctors (28.4% and 44.2%), disbelief that the identification will change something at the patient level (14.9% and 42.9%), and because interdisciplinary meetings about end-of-life issues increased during the study (35.8% and 35%). Respectively, 71.6% of the doctors and 94.5% of the nurses wished to keep on using the CODE alert in the future, although 9% and 23% were concerned about their anonymity.
Reach and adherence to the coaching and observed progress by the coach
Overall, 78 observations (7–8 per department) of interdisciplinary team meetings occurred during the 4-month intervention period, where feedback was provided to the doctors about their empowering leadership style and the group dynamic. Of the 51 senior and 42 junior doctors, respectively 34 (66.7%) and 22 (52.3%) participated in the single interactive session of 2–3 h focusing on the concepts of medical ethical decision-making and 32 (62.7%) and 18 (42.8%) participated in the individual coaching for a mean (standard deviation, SD) of 4.36 (2.55) sessions. Of the 248 individual coaching sessions, 40 (16.1%) concerned PET who were identified by the team during the intervention period, 102 (41.1%) concerned hospitalized patients who were mentioned by the doctor as potentially receiving excessive treatment and who were not identified by the team during the intervention period, and 116 (46.7%) concerned patients who potentially received excessive treatment according to the doctor prior to the intervention or coaching how to cope with ethical dilemmas in general. The observed progress in the five self-reflection items regarding ethical decision-making in teams according to the coach before and after the intervention is depicted in the supplementary File 2.
Main and post hoc analysis of the first primary endpoint and safety endpoint
The estimated incidence of written DNI-DNACPR decisions in PET was 29.7% in the intervention vs. 19.6% in the control arm (Table 3). The odds ratios (95% confidence interval) of the intervention in the naive and adjusted analysis were, respectively, 4.24 (4.21–4.27) and 3.71 (0.54–25.5). The estimated one-year mortality was 85% and 83.7%, respectively. The hazard ratios of the intervention regarding 1-year mortality were, respectively, 2.76 (1.26–6.04) and 3.26 (1.35–7.84).
The estimated incidence of written DNI-DNACPR decisions in the overall study population was 3.4% in the intervention vs. 1.9% in the control arm. There was a statistically significant increase in nearly all written treatment-limitation-decisions other than DNI-DNACPR after the intervention (supplementary File 2), including the decision of not referring the patient to the medical ICU (2.17% vs 1.19%, P = 0.004). The odds ratios (95% confidence interval) for written DNI-DNACPR orders in the naive and adjusted analysis were, respectively, 1.65 (1.12–2.43) and 2 (1.34–3). The estimated 1-year mortality was 14.5% and 15.1%, respectively. The hazard ratios of the intervention regarding 1-year mortality were, respectively, 0.89 (0.72–1.09) and 1.03 (0.84–1.27).
The results of the adjusted models, in which we observed a linear coaching exposure effect relationship of the intervention, and the Kaplan–Meier survival curves are depicted in detail in supplementary File 2.
Main analysis and sub-analysis of the second primary endpoint
The mean (standard deviation) EDMCQ before and after the study period was 0.45 (0.16) vs. 0.47 (0.16) points (Table 2). The absolute effect estimate of the intervention in the naive and adjusted analysis was 0.02 (0.11) and 0.02 points (0.11), respectively (P = 0.81 and P = 0.83).
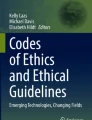
The sub-analysis of the differences across the 7 EDMCQ factors before and after the study period are depicted in Fig. 2. We observed only a highly statistically significant increase in the factor “ethical awareness” (P < 0.001) and a statistically significant decrease in the factor “mutual respect within the interdisciplinary team” (P = 0.032).

EDMCQ pre-post for all clinicians. EDMCQ ethical-decision-making climate questionnaire. Two-sided t-tests on combined paired and unpaired data were performed. The stars are only intended to flag levels of significance: *P < 0.05; **P < 0.01; ***P < 0.001.
Safety and adverse events
We received no complaints from patients or clinicians via the service, heads or head nurses from the departments.
Discussion
According to four recent meta-analyses [48,49,50,51], this is the first large multi-department cluster randomized trial assessing the impact of coaching doctors in self-reflective and empowering leadership, as well as in managing groups dynamics on concrete patient and clinician outcomes, more specifically regarding ethical decision-making in teams. In this study, we observed that (1) although ethical decision-making is a burning issue in many hospitals, clinicians identified a much smaller number of PET during the current interventional study than during our observational pilot study in 2019, (2) the intervention highly likely increased the incidence of written DNI-DNACPR decisions in the overall study population without increasing the 1-year mortality and (3) the intervention was not associated with a significant improvement in the quality of the ethical climate as perceived by clinicians.
Despite advance care planning and goal-oriented care being officially considered as a strategic priority in our hospital, and an intensive communication campaign in the weeks preceding and during the study period, clinicians identified ten times less PET than observed in our pilot study [20], resulting in a fivefold lower inclusion rate required to detect an intervention effect according to our power analysis. In contrast to our pilot study, we focused only on patients admitted for the first time in the hospital during the current study, which represents 63.6% of the entire patient population that is in average admitted in the participating wards yearly (supplementary file 2). With a 10% estimated incidence of PET, we still expected to include enough PET to detect a difference with 86% power at the 5% significance level [20]. However, we also used the CODE alert to identify PET instead of a dedicated researcher who actively surveyed clinicians. Identifying PET in the current study had also consequences for doctors and potentially for patients. Although fading attention for the study over time and visibility of the electronic CODE alert to identify PET was claimed as the main reasons by 75% and 50.7% of the nurses, respectively, in comparison to 53.7% and 34.3% of the doctors, 95% and 71.6% expressed the desire to keep on using this alert in the future. This underscores a deeper concern, particularly in nurses. More than 40% expressed fear of blaming doctors or skepticism regarding the impact of identifying PET. Nonetheless, 35% acknowledged improvement in interdisciplinary meetings about end-of-life issues since study initiation. These findings together with the incidence of written DNI-DNACPR decisions in the overall study population that remained low after the intervention (3.4%) in comparison to the 1-year mortality (14.5%) highlights the need to additionally coach the entire team in future studies to ensure safety and enhance speaking-up for the benefit of patients, more specifically among nurses.
Due to deviation from the predefined hypothesis, we cannot entirely claim a causal effect between our intervention and the first primary endpoint. However, the statistically significant increase in written DNI-DNACPR decisions from 1.9% in the control to 3.4% in the intervention arm within the overall study population, both in our naive (P = 0.011) and adjusted post hoc analysis (P < 0.001), along with the linear coaching exposure effect pattern, strongly suggest that our intervention bolstered doctors’ self-confidence in implementing goal-oriented care operationalized via written DNI-DNACPR decisions. This is further supported by a concomitant statistically significant increase in nearly all treatment-limitation-decisions other than DNI-DNACPR after the intervention, including the decision of not referring the patient to the medical ICU (supplementary File 2). Moreover, we found no significant increase in 1-year mortality, suggesting with a high probability that our intervention did not make doctors overconfident in taking written DNI-DNACPR decisions. Therefore, such decisions should not be considered as a death sentence but rather as a way to clarify to patients, relatives and the team what can fairly be expected from additional interventions in case of deterioration. This observation aligns with meta-analyses that did not find a relationship between palliative care or surrogate decision-making interventions and patient survival [52, 53]. After adjustment for confounders we found a statistically significant increase in 1-year mortality in PET, however, without concomitant increase in written DNI-DNACPR decisions. Whether this finding should be considered as a true indirect effect of the intervention or as a spurious result due to underpowering should be assessed in future studies.
Our intervention was not associated with an overall increase in EDMCQ. We observed only an increase in the factor “ethical awareness” and a decrease in the factor “mutual respect within the interdisciplinary team” (Fig. 2). Although the intervention increased self-reflection as reported by the coach (supplementary File 2) and subsequent self-confidence in operationalizing goal-oriented care via written DNI-DNACPR decisions, this finding suggests that the intervention helped doctors in enhancing ethical awareness in the team, however, without really empowering and involving the team during ethical decision-making. Failed expectations about the intervention together with the improvement in ethical awareness may have increased moral distress, more specifically among nurses, with a decrease in mutual respect in the interdisciplinary team as a consequence in some departments. This is another argument for coaching entire teams in future interventions.
Limitations of this study
Our study has several limitations. First, external validation of the results may pose a challenge. However, the positive intervention effect across most of the departments in combination with the high variability in ethical decision-making climate (supplementary File 2) suggest that our findings may be extrapolated to other centers. Second, external validation might be further compromised by the fact that the success of the intervention is largely coach-dependent. To guarantee the safety of the doctors and maximize the pre-test probability of the intervention’s effectiveness, we decided to collaborate with experienced senior clinical psychologists who were trained in systemic psychodynamic coaching and who received supervision by an internationally recognized coaching expert and faculty. Coaches were also asked to follow as much as possible the coaching protocol [20]. Nevertheless, the success of such interventions has been shown to be more dependent on the quality of the human relationship between the coach and the coachee than on the intervention itself [51]. Doctors’ satisfaction with the coach and coaching sessions in our study was good to excellent [unpublished]. Third, by the nature of the stepped-wedge design, with the timing of the intervention per department difficult to conceal, blinding the patients and relatives to the intervention could not be guaranteed. Fourth, because of pre-post design, we cannot claim causality regarding our second primary endpoint. Fifth, written DNI-DNACPR orders are only a proxy of decisions that many patients would make in the context of life-limiting illness [1, 54]. Therefore, albeit written DNI-DNACPR orders can easily and objectively be measured, they do not truly measure or represent the ground truth of either goal-oriented care or shared decision making. Finally, due to deviation from the initial targeted population, we were unfortunately not able to assess the impact of our intervention on satisfaction and wellbeing of patients and their relatives. Although we think it is reasonable to assume that our intervention also stimulated the development of a relationship with patient and relatives during shared decision-making in a similar way as in a team [20, 47], this should be certainly assessed in future interventions.
Conclusion
Our study suggests that coaching doctors regarding ethical decision-making in teams improves goal-oriented care operationalized via written DNI-DNACPR decisions in adult patients during their first hospital stay without increasing their mortality at 1 year. However, the small number of PET identified by the teams and the absence of improvement in ethical climate highlight the need to additionally coach entire teams in future interventions.
Change history
19 September 2024
A Correction to this paper has been published: https://doi.org/10.1007/s00134-024-07648-5
References
Berger Z (2015) Navigating the unknown: shared decision-making in the face of uncertainty. J Gen Intern Med 30:675–678. https://doi.org/10.1007/s11606-014-3074-8
Curtis JR, Vincent JL (2010) Ethics and end-of-life care for adults in the intensive care unit. Lancet 376:1347–1353. https://doi.org/10.1016/S0140-6736(10)60143-2
Kompanje EJ, Piers RD, Benoit DD (2013) Causes and consequences of disproportionate care in intensive care medicine. Curr Opin Crit Care 19(6):630–635. https://doi.org/10.1097/MCC.0000000000000026
Maley JH, Wanis KN, Young JG, Celi LA (2020) Mortality prediction models, causal effects, and end-of-life decision making in the intensive care unit. BMJ Health Care Inform 27(3):e100220. https://doi.org/10.1136/bmjhci-2020-100220
Mark NM, Rayner SG, Lee NJ, Curtis JR (2015) Global variability in withholding and withdrawal of life-sustaining treatment in the intensive care unit: a systematic review. Intensive Care Med 41(9):1572–1585. https://doi.org/10.1007/s00134-015-3810-5
Sprung CL, Ricou B, Hartog CS et al (2019) Changes in end-of-life practices in European Intensive Care Units from 1999 to 2016. JAMA 322(17):1692–1704. https://doi.org/10.1001/jama.2019.14608.Erratum.In:JAMA2019;322(17):1718
Kruser JM, Aaby DA, Stevenson DG et al (2019) Assessment of variability in end-of-life care delivery in Intensive Care Units in the United States. JAMA Netw Open 2(12):e1917344. https://doi.org/10.1001/jamanetworkopen.2019.17344
Benoit DD, Jensen HI, Malmgren J et al (2018) Outcome in patients perceived as receiving excessive care across different ethical climates: a prospective study in 68 intensive care units in Europe and the USA. Intensive Care Med 44(7):1039–1049. https://doi.org/10.1007/s00134-018-5231-8
Cardona-Morrell M, Jch K, Turner RM, Anstey M, Michell IA, Hillman K (2016) Non-beneficial treatments in hospital at end of life: a systematic review on the extent of the problem. Int J Qual Health Care 28:456–469. https://doi.org/10.1093/intqhc/mzw060
Dzeng E, Batten JN, Dohan D, Blythe J, Ritchie CS, Curtis JR (2023) Hospital culture and intensity of end-of-life care at 3 Academic Medical Centers. JAMA Intern Med 183(8):839–848. https://doi.org/10.1001/jamainternmed.2023.2450
Crosby MA, Cheng L, DeJesus AY, Travis EL, Rodriguez MA (2016) Provider and patient gender influence on timing of do-not-resuscitate orders in hospitalized patients with cancer. J Palliat Med 19(7):728–733. https://doi.org/10.1089/jpm.2015.0388
Pivodic L, Pardon K, Morin L et al (2016) Place of death in the population dying from diseases indicative of palliative care need: a cross-national population-level study in 14 countries. J Epidemiol Community Health 70(1):17–24. https://doi.org/10.1136/jech-2014-205365
Bekelman JE, Halpern SD, Blankart CR et al (2016) Comparison of site of death, health care utilization, and hospital expenditures for patients dying with cancer in 7 developed countries. JAMA 315(3):272–283. https://doi.org/10.1001/jama.2015.18603
Teno JM, Gozalo P, Trivedi AN et al (2018) Site of death, place of care, and health care transitions among US Medicare beneficiaries, 2000–2015. JAMA 320(3):264–271. https://doi.org/10.1001/jama.2018.8981
Weller J, Boyd M, Cumin D (2014) Teams, tribes and patient safety: overcoming barriers to effective teamwork in healthcare. Postgrad Med J 90:149–154. https://doi.org/10.1136/postgradmedj-2012-131168
Joseph-Williams N, Lloyd A, Edwards A et al (2017) Implementing shared decision making in the NHS: lessons from the MAGIC programme. BMJ 357:j1744. https://doi.org/10.1136/bmj.j1744
Willmott L, White B, Gallois C et al (2016) Reasons doctors provide futile treatment at end of life: a qualitative study. J Med Ethics 42:496–503. https://doi.org/10.1136/medethics-2016-103370
Palda VA, Bowman KW, McLean RF, Chapman MG (2005) “Futile care”: do we provide it? Why? A semistructured Canada-wide survey of intensive care unit doctors and nurses. J Crit Care 20:207–213. https://doi.org/10.1016/j.jcrc.2005.05.006
Chamberlin P, Lambden J, Kozlov E et al (2019) Clinicians’ perceptions of futile or potentially inappropriate care and associations with avoidant behaviors and burnout. J Palliat Med 22(9):1039–1045. https://doi.org/10.1089/jpm.2018.0385
Benoit DD, Vanheule S, Manesse F et al (2023) Coaching doctors to improve ethical decision-making in adult hospitalised patients potentially receiving excessive treatment: study protocol for a stepped wedge cluster randomised controlled trial. PLoS ONE 18(3):e0281447. https://doi.org/10.1371/journal.pone.0281447
Menzies-Lyth I (1988) Containing anxiety in institutions: selected essays. Free Association Books, London
Lievrouw A, Vanheule S, Deveugele M et al (2016) Coping with moral distress in oncology practice: nurse and physician strategies. Oncol Nurs Forum 43(4):505–512. https://doi.org/10.1188/16.ONF.505-512
Meier DE, Back AL, Morrison RS (2011) The inner life of physicians and care of the seriously ill. JAMA 286(23):3007–3014. https://doi.org/10.1001/jama.286.23.3007
Childers J, Arnold B (2019) The inner lives of doctors: physician emotion in the care of the seriously ill. Am J Bioethics 19(12):29–34. https://doi.org/10.1080/15265161.2019.1674409
Goleman D (1998) What makes a leader? Harv Bus Rev 76(6):93–102
Stoller JK (2021) Emotional intelligence: leadership essentials for chest medicine professionals. Chest 59(5):1942–1948. https://doi.org/10.1016/j.chest.2020.09.093
Van den Bulcke B, Piers R, Jensen HI et al (2018) Ethical decision-making climate in the ICU: theoretical framework and validation of a self-assessment tool. BMJ Qual Saf 27(10):781–789. https://doi.org/10.1136/bmjqs-2017-007390
Piers RD, Azoulay E, Ricou B et al (2011) Perceptions of appropriateness of care among European and Israeli intensive care unit nurses and physicians. JAMA 306(24):2694–2703. https://doi.org/10.1001/jama.2011.1888
Piers RD, Azoulay E, Ricou B et al (2014) Inappropriate care in European ICUs: confronting views from nurses and junior and senior physicians. Chest 146(2):267–275. https://doi.org/10.1378/chest.14-0256
Jensen HI, Hebsgaard S, Hansen TCB et al (2019) Perceptions of ethical decision-making climate among clinicians working in European and US ICUs: differences between nurses and physicians. Crit Care Med 47(12):1716–1723. https://doi.org/10.1097/CCM.0000000000004017
Michalsen A, Long AC, DeKeyser GF et al (2019) Interprofessional shared decision-making in the ICU: a systematic review and recommendations from an expert panel. Crit Care Med 47(9):1258–1266. https://doi.org/10.1097/CCM.0000000000003870
Huwel L, Van Eessen J, Gunst J et al (2023) What is appropriate care? A qualitative study into the perceptions of healthcare professionals in Flemish university hospital intensive care units. Heliyon 9(2):e13471. https://doi.org/10.1016/j.heliyon.2023.e13471
Wright AA, Zhang B, Ray A et al (2008) Associations between end-of-life discussions, patient mental health, medical care near death, and caregiver bereavement adjustment. JAMA 300(14):1665–1673. https://doi.org/10.1001/jama.300.14.1665
Kentish-Barnes N, Chaize M, Seegers V et al (2015) Complicated grief after death of a relative in the intensive care unit. Eur Respir J 45(5):1341–1352. https://doi.org/10.1183/09031936.00160014
Dzeng E, Curtis JR (2018) Understanding ethical climate, moral distress, and burnout: a novel tool and a conceptual framework. BMJ Qual Saf 27(10):766–770. https://doi.org/10.1136/bmjqs-2018-007905
Embriaco N, Papazian L, Kentish-Barnes N, Pochard F, Azoulay E (2007) Burnout syndrome among critical care healthcare workers. Curr Opin Crit Care 13(5):482–488. https://doi.org/10.1097/MCC.0b013e3282efd28a
Van den Bulcke B, Metaxa V, Reyners AK et al (2020) Ethical climate and intention to leave among critical care clinicians: an observational study in 68 intensive care units across Europe and the United States. Intensive Care Med 46(1):46–56. https://doi.org/10.1007/s00134-019-05829-1
Cheung MC, Earle CC, Rangrej J et al (2015) Impact of aggressive management and palliative care on cancer costs in the final month of life. Cancer 121(18):3307–3315. https://doi.org/10.1002/cncr.29485
Chaudhuri D, Tanuseputro P, Herritt B, D’Egidio G, Chalifoux M, Kyeremanteng K (2017) Critical care at the end of life: a population-level cohort study of cost and outcomes. Crit Care 21(1):124. https://doi.org/10.1186/s13054-017-1711-4
Alingh CW, van Wijngaarden JDH, van de Voorde K, Paauwe J, Huijsman R (2019) Speaking up about patient safety concerns: the influence of safety management approaches and climate on nurses’ willingness to speak up. BMJ Qual Saf 28(1):39–48. https://doi.org/10.1136/bmjqs-2017-007163
Stoller JK (2021) Leadership essentials for CHEST medicine professionals: models, attributes, and styles. Chest 159(3):1147–1154. https://doi.org/10.1016/j.chest.2020.09.095
Stoller JK (2021) Building teams in health care. Chest 159(6):2392–2398. https://doi.org/10.1016/j.chest.2020.09.092
Stoller JK (2018) Developing physician leaders: a perspective on rationale, current experience, and needs. Chest 154(1):16–20. https://doi.org/10.1016/j.chest.2017.12.014
Silverman HJ, Dagenais J, Gordon-Lipkin E et al (2013) Perceived comfort level of medical students and residents in handling clinical ethics issues. J Med Ethics 39(1):55–58. https://doi.org/10.1136/medethics-2011-100300
Torjesen I (2016) Doctors give patients potentially harmful procedures at end of life, global review finds. BMJ 353:i3613. https://doi.org/10.1136/bmj.i3613
Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG (2009) Research electronic data capture (REDCap)—a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform 42(2):377–381. https://doi.org/10.1016/j.jbi.2008.08.010
Elwyn G, Durand MA, Song J et al (2017) A three-talk model for shared decision making: multistage consultation process. BMJ 359:j4891. https://doi.org/10.1136/bmj.j4891
Frich JC, Brewster AL, Cherlin EJ, Bradley EH (2015) Leadership development programs for physicians: a systematic review. J Gen Intern Med 30(5):656–674. https://doi.org/10.1007/s11606-014-3141-1
Geerts JM, Goodall AH, Aglus S (2020) Evidence-based leadership development for physicians: a systematic review. Soc Sci Med 20(246):112709. https://doi.org/10.1016/j.socscimed.2019.112709
Lyons O, George R, Galante JR et al (2021) Evidence-based medical leadership development: a systematic review. BMJ Leader 5:206–213. https://doi.org/10.1136/leader-2020-000360
De Haan E, Nilsson VO (2023) What can we know about the effectiveness of coaching? A meta-analysis based only on randomized controlled trials. Acad Manag Learn Educ 22:641–661. https://doi.org/10.5465/amle.2022.0107
Kavalieratos D, Corbelli J, Zhang D et al (2016) Association between palliative care and patient and caregiver outcomes: a systematic review and meta-analysis. JAMA 316(20):2104–2114. https://doi.org/10.1001/jama.2016.16840
Bibas L, Peretz-Larochelle M, Adhikari NK et al (2019) Association of surrogate decision-making interventions for critically ill adults with patient, family, and resource use outcomes: a systematic review and meta-analysis. JAMA Netw Open 2(7):e197229. https://doi.org/10.1001/jamanetworkopen.2019.7229
Sallnow L, Smith S, Ahledzai SH et al (2022) Report of the Lancet Commission on the value of death: brining death back into life. Lancet 399(10327):837–884. https://doi.org/10.1016/S0140-6736(21)02314-X
Acknowledgements
We thank all of the participants who volunteered for this study as well as the heads (not included in the co-author list: Sylvie Rottey, Medical Oncology; Paul Boon, Neurology; Steven Callens, Internal Medicine and Infectious Diseases; Guy Brusselle Pneumology), doctors ( Sofie Gevaert and Els Vandecasteele, Cardiology), chief nurses of the participating departments (Kristof Alluyn, Medical Oncology; Bart Sobrie, Internal Medicine; Isabelle Danel, Neurology; Els Carrijn, Geriatrics; Jo Vandenbossche, Medical Intensive Care Unit; Tania Helleputte, Gastro-intestinal and Liver Diseases; Fatima Snoussi, Pneumology; Katrien Schelfhout, Hematology, Gastroenterology and Pneumology; Annelies Masset, Cardiology and Internal Medicine; Jens Boelens, Cardiology Intensive Care; Christelle Lizy, Nephrology and Endocrinology; Delphine Lacante, Hematology and Stem Cell Transplantation) and care managers (Lieve De Geyter from the Man, Woman and Child Cluster; An Van Holsbeek from the Blood, Respiratory and Gastro-intestinal Cluster, Geert De Smet from the Metabolic and Cardiovascular Cluster and Hilde Goedertier from the Critical Care Cluster) for their commitment to this challenging study. We are also grateful to the nurses of the ICU trial cell (Anouska De Smeytere, Daisy Vermeiren, Jolien Van Hecke and Lesley Decoster) for their professional support and for empowering the co-investigators and chief nurses in including participants. We also want to thank Bram Gadeyne of the Intensive Care Medicine Department for the IT support, Els Goetghebeur (Faculty of Applied Mathematics, Computer Sciences and Statistics, Ghent University) for the statistical supervision and Marie-Laure Solie, Tessa Verheecke and Lies Ketels of the Ghent University Hospital Communication Department for helping us to set up a professional communication campaign. Last but not least, we would like to thank the following members of the Executive Board of the Ghent University Hospital for making this study possible; Eric Mortier, CEO; Frank Vermassen, Chief doctor; Rik Verhaeghe, Chief Nursing Officer; Kristof Eeckloo, responsible for the Strategic Policy, Quality Management, Information Management & Clinical Networks and Chantal Haeck, responsible for the Company Supporting Service.
Funding
This study is supported by grants from the Ghent University Hospital "Fonds voor Innovatie en Wetenschappelijk Onderzoek" and the Belgian "Fonds voor Wetenschappelijk Onderzoek" FWO (senior clinical investigators grant 1800518N obtained by Benoit in 2017). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
DDB and RP had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Corresponding author
Ethics declarations
Conflicts of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest with regard to the content of this manuscript
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original online version of this article was revised: The Methods section was accidently shortened by a typesetting mistake. The original article has been corrected.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Benoit, D.D., De Pauw, A., Jacobs, C. et al. Coaching doctors to improve ethical decision-making in adult hospitalized patients potentially receiving excessive treatment. The CODE stepped-wedge cluster randomized controlled trial. Intensive Care Med (2024). https://doi.org/10.1007/s00134-024-07588-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00134-024-07588-0