
Abstract
Purpose
Both mobile (MB) and fixed (FB) bearing implants are routinely used for total knee arthroplasty (TKA). This meta-analysis compared MB versus FB for TKA in terms of implant positioning, joint function, patient reported outcome measures (PROMs), and complications. It was hypothesised that MB performs better than FB implants in primary TKA.
Methods
This meta-analysis was conducted according to the 2020 PRISMA statement. In February 2022, the following databases were accessed: Pubmed, Web of Science, Google Scholar, Embase. All the randomized clinical trials (RCTs) comparing mobile versus fixed bearing for primary TKA were considered.
Results
Data from 74 RCTs (11,116 procedures) were retrieved. The mean follow-up was 58.8 (7.5 to 315.6) months. The MB group demonstrated greater range of motion (ROM) (P = 0.02), Knee Society Score (KSS) score (P < 0.0001), and rate of deep infections (P = 0.02). No difference was found in implant positioning: tibial slope, delta angle, alpha femoral component angle, gamma femoral component angle, beta tibial component angle, tibiofemoral alignment angle, posterior condylar offset, radiolucent lines. No difference was found in duration of the surgical procedure. No difference was found in the following PROMs: Oxford Knee Score (OKS), Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), visual analogue scale (VAS), function and pain subscales of the KSS score. No difference was found in the rate of anterior knee pain, revision, aseptic loosening, fractures, and deep vein thrombosis.
Conclusion
There is no evidence in support that MB implants promote greater outcomes compared to FB implants in primary TKA.
Level of evidence
Level I.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Knee osteoarthritis (OA) is common [6, 94]. Knee OA impairs joint function and quality of life, limiting physical activities and patient independency [71, 73, 115]. Total knee arthroplasty (TKA) is advocated for end-stage knee OA [46, 74, 85]. Both mobile (MB) and fixed (FB) bearing implants are available for primary TKA [1, 49]. FB implants were introduced first, and still represent the most common type of TKA [21, 84]. The polyethylene inlay of FB implants is secured on the tibial plateau. On the other hand, MB implants allow rotation of the polyethylene inlay around its longitudinal axis, miming the physiological kinematics of the knee and promoting a wider range of motion [22, 34, 93]. Previous evidence suggested that MB may promote greater outcomes in functional scores and complications [40, 44, 45, 75, 95]. However, the difference was minimal, and whether mobile bearing provide better outcomes remains controversial [5, 16, 38, 46, 63, 82, 96, 100, 103, 111]. Several randomized clinical trials (RCTs), which have not been yet considered in any previous meta-analyses, have recently been recently published [8, 24, 28, 59, 93, 105, 107, 123]. An update of current evidence could clarify whether MB implants promote greater outcomes to FB in TKA in terms of outcome and complication rate. This meta-analysis compared MB versus FB for primary TKA in terms of implant positioning, patient reported outcome measures (PROMs), and complications. It was hypothesised that MB promotes better outcomes than FB implants in primary TKA.
Materials and methods
Eligibility criteria
All the clinical investigations comparing mobile versus fixed bearing for primary TKA were considered. Only randomized clinical trials (RCTs) with level I to II of evidence, according to Oxford Centre of Evidence-Based Medicine [47], were considered. Only articles in English, German, Italian, French, and Spanish were eligible. Only studies published in peer reviewed journals with accessible full-text article were considered. Only studies which clearly stated the number of included procedures with a minimum of 8 months follow-up were considered. Reviews, opinions, letters, and editorials were not considered. Animals, in vitro, biomechanics, computational, and cadaveric studies were not eligible. All studies investigating the efficacy of experimental rehabilitation protocols were also not included. Studies reporting revision surgeries were also excluded from the analysis.
Search strategy
This meta-analysis was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses: the 2020 PRISMA statement [89]. The PICODT algorithm was preliminary pointed out:
-
P (Population): end-stage knee osteoarthritis;
-
I (Intervention): TKA;
-
C (Comparison): Mb versus Fb;
-
O (Outcomes): implant alignment, surgical duration, range of motion, PROMs, complications;
-
D (Design); RCT;
-
T (Follow-up): minimum 8 months.
In February 2022, the following databases were accessed: Pubmed, Web of Science, Google Scholar, Embase. The search was limited to RCTs, with no time constrains. The following keywords were used in combination using the Boolean operator AND/OR: knee, osteoarthritis, total, arthroplasty, replacement, prosthesis, implant, mobile bearing, fixed bearing, patient reported outcome measures, PROMs, function, efficacy, complication, revision, reoperation, pain, outcome.
Selection and data collection
Two authors (F.C. and K.E.) independently performed the database search. All the resulting titles were screened and if suitable, the abstract was accessed. The full-text of the abstracts which matched the topic was accessed. A cross reference of the bibliography of the full-text articles were also screened for inclusion. All disagreements between the authors were debated and, if necessary, solved by a third author (NM).
Data items
Two authors (F.C. and K.E.) independently performed data extraction.
The following data at baseline were extracted:
-
Generalities of the study: name of the first author, year of publication and journal, length of the follow-up, number of patients, percentage of women (%), body mass index (BMI).
The following data at baseline and at last follow-up were extracted:
-
Range of motion (ROM);
-
PROMs: Oxford Knee Score (OKS), Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), visual analogue scale (VAS), Knee Society Score (KSS), and relate function (KSFS and pain (KSPS) subscales.
The following data at last follow-up were collected:
-
Implant alignment: tibial slope, delta angle, alpha femoral component angle, gamma femoral component angle, beta tibial component angle, tibiofemoral alignment angle, posterior condylar offset, radiolucent lines;
-
Surgical duration;
-
Complications: anterior knee pain (AKP), revision, aseptic loosening, fractures, deep vein thrombosis (DVT).
Study risk of bias assessment
The risk of bias was valuated using the software Review Manager 5.3 (The Nordic Cochrane Collaboration, Copenhagen). The risk of bias was evaluated, based on the guidelines in the Cochrane Handbook for Systematic Reviews of Interventions [27], by the two reviewers (F.C. and K.E.). The following endpoints were evaluated: selection, detection, performance, attrition, reporting, and other bias. To assess the overall risk of publication bias, the funnel plot of the most commonly reported outcome was performed. The funnel plot charted the standard error (SE) of the Log Odd Ratio (LogOR) versus its OR. The degree of asymmetry of the plot is directly proportional to the degree of bias. To assess the risk of bias of each included studies, the risk of bias graph was performed.
Statistical analysis and synthesis methods
The statistical analyses were performed by the main author (F.M.). For descriptive statistics, the IBM SPSS software (version 25) was used. The mean difference and standard deviation were adopted. The T test was performed to assess baseline comparability, with values of P > 0.1 considered satisfactory. For the meta-analyses, the software Review Manager 5.3 (The Nordic Cochrane Collaboration, Copenhagen) was used. For continuous data, the inverse variance method with mean difference (MD) effect measure was used. For binary data, the Mantel–Haenszel method with odd ratio (OR) effect measure was used. The confidence interval (CI) was set at 0.95 in all the comparison. Heterogeneity was assessed using \(\chi\)2 and Higgins-I2 tests. If \(\chi\)2 > 0.05, no statistically significant heterogeneity was found. If \(\chi\)2 < 0.05 and Higgins-I2 > 60% high heterogeneity was found. A fixed model effect was used as default. In case of high heterogeneity, a random model was used. Overall values of P < 0.05 were considered statistically significant.
Results
Study selection
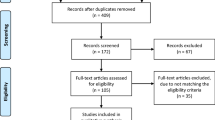
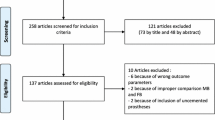
The literature search resulted in 414 articles. After removal of duplicates (N = 200), a further 140 articles were not eligible for the following reasons: study design (N = 78), language limitation (N = 17), short follow-up (N = 19), lacking quantitative data under the endpoints of interest (N = 26). Finally, 74 comparative studies were included. The results of the literature search are shown in Fig. 1.

Flow chart of the literature search
Risk of publication bias
The funnel plot of the most commonly reported outcome (revision) was performed to assess the risk of publication bias. The plot evidenced very good symmetry, with optimal distribution of the estimated effects of the included studies. The Egger’s test score was P = 0.6, attesting a low risk of publication bias (Fig. 2).

Funnel plot
Study risk of bias assessment
Given the randomized design of the included studies, the risk of selection bias was low. The risk of detection bias was low to moderate, as was the risk of attrition and reporting biases. The risk of other bias was also low to moderate. Concluding, the quality of the methodological assessment was good. The Cochrane risk of bias graph is shown in Fig. 3.

Methodological quality assessment
Study characteristics and results of individual studies
Data from 11,116 procedures were retrieved. 69% (7670 of 11,116 patients) were women. The mean follow-up was 58.8 (7.5 to 315.6) months. The mean age was 67.5 ± 5.9 years, the mean BMI was 28.6 ± 2.3 kg/m2. Comparability was found at baseline concerning the mean age, mean BMI, female, ROM, KSS, OKS, KSS pain, WOMAC, VAS, and KSS function. Generalities and patient baseline of the included studies are shown in greater detail in Table 1, the baseline comparability between the two groups at baseline in Table 2.
Results of syntheses
Eighteen studies (3827 procedures) were included in the comparison of ROM [4, 9, 10, 12, 14, 18, 23, 25, 41, 54, 59, 60, 62, 70, 75, 118]. The MB group demonstrated greater ROM (MD 1.58; 95% CI 0.22 to 2.93; P = 0.02; Fig. 4).

Forest plot of the comparison: ROM (IV: inverse variance; CI: confidence interval). The square represents the effect of each single study. The horizontal line represents the confidence interval of each study. The vertical line “0” represent the no effect threshold. The diamond represents the final effect of the overall analysis
Thirty-one studies (5094 procedures) were included in the comparison of the KSS score [4, 10, 12, 13, 17, 18, 25, 32, 33, 39, 41, 42, 48, 54, 57, 59, 60, 62, 66, 70, 75, 83, 87, 91, 95, 96, 104, 106, 107, 110, 118]. The MB evidenced greater KSS score (MD 1.23; 95% CI 0.85 to 1.61; P < 0.0001; Fig. 5).

Forest plot of the comparison: KSS score (IV: inverse variance; CI: confidence interval). The square represents the effect of each single study. The horizontal line represents the confidence interval of each study. The vertical line “0” represent the no effect threshold. The diamond represents the final effect of the overall analysis
Thirty-two studies (6489 procedures) were included in the comparison of rate of deep infection [4, 7, 13, 14, 17, 23, 25, 33, 35, 36, 39, 41, 42, 55,56,57, 60,61,62,63,64, 67, 70, 72, 76, 95, 104, 113, 122].The MB group evidenced a greater rate of deep infections (OR 1.64; 95% CI 1.07 to 2.52; P = 0.02; Fig. 6).

Forest plot of the comparison: rate of deep infection (M–H: Mantel–Haenszel; CI: confidence interval). The square represents the effect of each single study. The horizontal line represents the confidence interval of each study. The vertical line “0” represent the no effect threshold. The diamond represents the final effect of the overall analysis
No difference was found in implant positioning: tibial slope, delta angle, alpha femoral component angle, gamma femoral component angle, beta tibial component angle, tibiofemoral alignment angle, posterior condylar offset, radiolucent lines. No difference was found in duration of the surgical procedure. No differences were found in the following PROMs: OKS, WOMAC, VAS, function and pain subscales of the KSS score. No difference were found in the rate of the following complications: AKP, revision, aseptic loosening, fractures, DVT.
Discussion
The main finding of the present study was that the MB implants performed in a similar fashion to FB implants for TKA. The analyses evidenced greater KSS, ROM, and rate of the deep infection in MB implants. However, though statistically significant, their clinical relevance is likely limited. Concerning the KSS score, its overall difference between the two implants does not overcome their minimal clinically important difference (MCID), which has been estimated between 6/100 and 9/100 [40, 52, 68, 69, 112]. A formal MCID for the ROM has not yet been estimated. However, given its minimal difference, the clinical relevance of this finding is dubious. Marques et al. [75] conducted a RCT on 99 patients. After 1-year follow-up, a statistically significant increase in ROM and KSS was found in the MB group. After 4-year follow-up no difference was found between the MB and FB group. Kim et al. [59] conducted a RTC on 291 patients, with a follow-up period of 27 years. No differences were found in ROM and KSS between the two groups. Powell et al. [95] analysed 167 patients at 10 years of follow-up, with no statistically significant difference in KSS between MB and FB groups. However, a trend was seen with higher mean scores over the years for the MB group. Given the minimal difference between the two groups in ROM and KSS, the clinical relevance of these findings was dubious. A slight improvement of PROMs was not necessarily associated with a functional advantage [15]. The minimal functional improvement may be explained by greater axial rotation promoted by the MB implants [29, 53, 99]. Amaro et al. [8] evaluating kinematic differences in 64 patients, found that axial rotation was higher in the MB group after 1 year, but disappeared at 2-year follow-up. A histological study showed the development of fibrotic tissue in the synovial membrane and infrapatellar fat pad after a TKA [3]. This produces a hardening effect that may minimize the kinematic differences between the MB and FB groups [8]. MB actively corrects the rotational femoral offset while standing, improving stepping and squatting [46]. However, this difference is not clinically relevant [88]. Moreover, different types of MB implants have different kinematics during stepping and squatting [46], and the final clinical outcome of MB can be influenced by the brand. A long-term study comparing different types of MB and FB implants could be useful to further understand the real benefits of different type of prostheses.
The rate of deep infection was strongly influenced by the study by Breeman et al. [17], which weighted 17.6% on the final effect. Indeed, when conducting the analyses without those data [17], the rate of deep infection is similar between the two groups. Nevertheless, the authors evidenced no difference between the two implants in terms of infections in their study [17]. Indeed, a deep infection was present in 12 of 276 patients in the MB group, and in 6 of 263 patients in the FB group [17]. Some limitations that may have influence our results should be discussed. The authors conducted a multicentre study involving 116 surgeons [17, 99]. Surgeon experience and approaches, implants design and post-operative protocols were not considered.
No differences in radiographic alignment were shown in the present study. Only one study showed a radiographic difference in patellar translation [104]. A tendency to increase patellar translation in the MB group was also evidenced in the present study. In MB implants, the rotation of the tibial component and the variable position of the tibial relative to the femoral implant can affect patellar tracking [90]. However, other meta-analyses comparing patellar translation did not evidence any differences between MB and FB implants [86, 111].
The MB design has been introduced to better simulate knee kinematics, reducing contact stresses, aseptic loosening, and polyethylene wear [20]. The self-alignment promoted by the MB implants compensates the physiological tibial and the femoral component offset [30]. The latter has been hypothesized to improve the conformity between femoral component and mobile insert during stepping and squatting, thus reducing contact pressure and loosening of polyethylene wear [46]. However, this study was unable to identify differences between the two implants, in contest with previous evidence [59, 62, 105]. Though there is less wear at the femoral condyle interface in MB than in FB implant, the former produce additional wear at the surface of metallic tibial implant, which may explain the similarity in the rate of overall wear [105]. Only one study [37] showed a higher rate of aseptic loosening in the MB group. The risk was higher only in certain models. In the MB implants, the geometry of tibial component is such that the shortening of the keel and the under-face texture increase the risk for micromotion and aseptic loosening [26, 53, 65, 101, 104, 108].
This study certainly has limitations. The analyses were conducted irrespective of the surgical exposure and approach. In the present study, both minimally and standard invasive techniques were included. Surgical exposure may influence outcomes, and minimally invasive surgery performed by experienced surgeon may offer short- and mid-term clinical and functional benefits over the conventional exposure [78]. Moreover, the surgical approach may influence the clinical outcomes. A recent network meta-analysis demonstrated that the mini-subvastus approach outperformed all other approaches (mini-medial parapatellar, midvastus, quadriceps sparring) [77]. Patellar retaining or resurfacing has not been investigated, and may represent a further limitation [80]. Different inlay designs (posterior stabilized, cruciate/bicruciate retaining) were not considered as separate. A previous meta-analysis demonstrated no difference in the outcome between the posterior stabilized versus cruciate retaining [81], while no study which compared MB versus FB using bicruciate retaining implants were included in the present study. The manufacturer of the implants was often biased. MB implants are more sensitive to soft tissue release and optimal gap balancing over flexion and extension. Differently, in FB implants planned resection following the anatomical landmarks (anteroposterior and trans-epicondylar axis) can be performed [79]. Few authors appropriately described the surgical protocol, and further subgroups comparisons were not possible. This may generate bias and increase heterogeneity. The conclusion of the present meta-analysis should be considered with these limitations. Results of the present study indicated that bearing in TKA, whether mobile or fixed, does not influence the clinical outcome.
Conclusion
There is no evidence to support that MP implants promote better outcomes compared to FB implants in primary TKA. The analyses evidenced greater KSS, ROM, and greater rate of the deep infection in MB implants. However, though statistically significant, their clinical relevance is limited. Further clinical trials are required.
Availability of data and materials
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Abdel MP, Tibbo ME, Stuart MJ, Trousdale RT, Hanssen AD, Pagnano MW (2018) Infographic: fixed- versus mobile-bearing total knee arthroplasty at ten years. Bone Joint J 100-B:923–924
Abdel MP, Tibbo ME, Stuart MJ, Trousdale RT, Hanssen AD, Pagnano MW (2018) A randomized controlled trial of fixed- versus mobile-bearing total knee arthroplasty: a follow-up at a mean of ten years. Bone Joint J 100-B:925–929
Abdul N, Dixon D, Walker A, Horabin J, Smith N, Weir DJ et al (2015) Fibrosis is a common outcome following total knee arthroplasty. Sci Rep 5:16469
Aggarwal AK, Agrawal A (2013) Mobile vs fixed-bearing total knee arthroplasty performed by a single surgeon: a 4- to 6.5-year randomized, prospective, controlled, double-blinded study. J Arthroplasty 28:1712–1716
Aglietti P, Baldini A, Buzzi R, Lup D, De Luca L (2005) Comparison of mobile-bearing and fixed-bearing total knee arthroplasty: a prospective randomized study. J Arthroplasty 20:145–153
Ahrar H, Aghili K, Sobhan MR, Mahdinezhad-Yazdi M, Akbarian-Bafghi MJ, Neamatzadeh H (2019) Association of rs2234693 and rs9340799 polymorphisms of estrogen receptor-1 gene with radiographic defined knee osteoarthritis: a meta-analysis. J Orthop 16:234–240
Amaro JT, Arliani GG, Astur DC, Debieux P, Kaleka CC, Cohen M (2017) No difference between fixed- and mobile-bearing total knee arthroplasty in activities of daily living and pain: a randomized clinical trial. Knee Surg Sports Traumatol Arthrosc 25:1692–1696
Amaro JT, Novaretti JV, Astur DC, Cavalcante ELB, Rodrigues Junior AG, Debieux P et al (2020) Higher axial tibiofemoral rotation and functional outcomes with mobile-bearing compared with fixed-bearing total knee arthroplasty at 1- but not at 2-year follow-up-a randomized clinical trial. J Knee Surg 33:474–480
Artz NJ, Hassaballa MA, Robinson JR, Newman JH, Porteous AJ, Murray JR (2015) Patient reported kneeling ability in fixed and mobile bearing knee arthroplasty. J Arthroplasty 30:2159–2163
Bailey O, Ferguson K, Crawfurd E, James P, May PA, Brown S et al (2015) No clinical difference between fixed- and mobile-bearing cruciate-retaining total knee arthroplasty: a prospective randomized study. Knee Surg Sports Traumatol Arthrosc 23:1653–1659
Baktir A, Karaaslan F, Yurdakul E, Karaoglu S (2016) Mobile- versus fixed-bearing total knee arthroplasty: a prospective randomized controlled trial featuring 6–10-year follow-up. Acta Orthop Traumatol Turc 50:1–9
Ball ST, Sanchez HB, Mahoney OM, Schmalzried TP (2011) Fixed versus rotating platform total knee arthroplasty: a prospective, randomized, single-blind study. J Arthroplasty 26:531–536
Beard DJ, Pandit H, Price AJ, Butler-Manuel PA, Dodd CA, Murray DW et al (2007) Introduction of a new mobile-bearing total knee prosthesis: minimum three year follow-up of an RCT comparing it with a fixed-bearing device. Knee 14:448–451
Bhan S, Malhotra R, Kiran EK, Shukla S, Bijjawara M (2005) A comparison of fixed-bearing and mobile-bearing total knee arthroplasty at a minimum follow-up of 4.5 years. J Bone Joint Surg Am 87:2290–2296
Birnir B, Tierney ML, Lim M, Cox GB, Gage PW (1997) Nature of the 5’ residue in the M2 domain affects function of the human alpha 1 beta 1 GABAA receptor. Synapse 26:324–327
Bistolfi A, Massazza G, Lee GC, Deledda D, Berchialla P, Crova M (2013) Comparison of fixed and mobile-bearing total knee arthroplasty at a mean follow-up of 116 months. J Bone Joint Surg Am 95:e83
Breeman S, Campbell MK, Dakin H, Fiddian N, Fitzpatrick R, Grant A et al (2013) Five-year results of a randomised controlled trial comparing mobile and fixed bearings in total knee replacement. Bone Joint J 95-B:486–492
Breugem SJ, Sierevelt IN, Schafroth MU, Blankevoort L, Schaap GR, van Dijk CN (2008) Less anterior knee pain with a mobile-bearing prosthesis compared with a fixed-bearing prosthesis. Clin Orthop Relat Res 466:1959–1965
Breugem SJ, van Ooij B, Haverkamp D, Sierevelt IN, van Dijk CN (2014) No difference in anterior knee pain between a fixed and a mobile posterior stabilized total knee arthroplasty after 7.9 years. Knee Surg Sports Traumatol Arthrosc 22:509–516
Buechel FF, Pappas MJ (1986) The New Jersey low-contact-stress knee replacement system: biomechanical rationale and review of the first 123 cemented cases. Arch Orthop Trauma Surg 105:197–204
Capella M, Dolfin M, Saccia F (2016) Mobile bearing and fixed bearing total knee arthroplasty. Ann Transl Med 4:127
Castellarin G, Bori E, Innocenti B (2021) Experimental and clinical analysis of the use of asymmetric vs symmetric polyethylene inserts in a mobile bearing total knee arthroplasty. J Orthop 23:25–30
Chaudhry A, Goyal VK (2018) Fixed-bearing versus high-flexion RP total knee arthroplasty (TKA): midterm results of a randomized controlled trial. J Orthop Traumatol 19:2
Chen P, Huang L, Zhang D, Zhang X, Ma Y, Wang Q (2022) Mobile bearing versus fixed bearing for total knee arthroplasty: meta-analysis of randomized controlled trials at minimum 10-year follow-up. J Knee Surg 35:135–144
Choi WC, Lee S, Seong SC, Jung JH, Lee MC (2010) Comparison between standard and high-flexion posterior-stabilized rotating-platform mobile-bearing total knee arthroplasties: a randomized controlled study. J Bone Joint Surg Am 92:2634–2642
Crossett L (2006) Evolution of the low contact stress (LCS) complete knee system. Orthopedics 29:S17-22
Cumpston M, Li T, Page MJ, Chandler J, Welch VA, Higgins JP et al (2019) Updated guidance for trusted systematic reviews: a new edition of the Cochrane handbook for systematic reviews of interventions. Cochrane Database Syst Rev 10:142
Dalyan S, Ozan F, Altun I, Kahraman M, Gunay AE, Ozdemir K (2022) The influence of component rotational malalignment on early clinical outcomes in total knee arthroplasty. Cureus 14:e22444
Delport HP, Banks SA, De Schepper J, Bellemans J (2006) A kinematic comparison of fixed- and mobile-bearing knee replacements. J Bone Joint Surg Br 88:1016–1021
Dennis DA, Komistek RD (2006) Mobile-bearing total knee arthroplasty: design factors in minimizing wear. Clin Orthop Relat Res 452:70–77
Feczko PZ, Jutten LM, van Steyn MJ, Deckers P, Emans PJ, Arts JJ (2017) Comparison of fixed and mobile-bearing total knee arthroplasty in terms of patellofemoral pain and function: a prospective, randomised, controlled trial. BMC Musculoskelet Disord 18:279
Ferguson KB, Bailey O, Anthony I, James PJ, Stother IG, M JGB, (2014) A prospective randomised study comparing rotating platform and fixed bearing total knee arthroplasty in a cruciate substituting design—outcomes at two year follow-up. Knee 21:151–155
Fransen BL, Hoozemans MJ, Keijser LC, van Lent ME, Verheyen CC, Burger BJ (2015) Does insert type affect clinical and functional outcome in total knee arthroplasty? A Randomised controlled clinical trial with 5-year follow-up. J Arthroplasty 30:1931–1937
Fransen BL, van Duijvenbode DC, Hoozemans MJM, Burger BJ (2017) No differences between fixed- and mobile-bearing total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc 25:1757–1777
Garling EH, Valstar ER, Nelissen RG (2005) Comparison of micromotion in mobile bearing and posterior stabilized total knee prostheses: a randomized RSA study of 40 knees followed for 2 years. Acta Orthop 76:353–361
Gioe TJ, Glynn J, Sembrano J, Suthers K, Santos ER, Singh J (2009) Mobile and fixed-bearing (all-polyethylene tibial component) total knee arthroplasty designs. A prospective randomized trial. J Bone Joint Surg Am 91:2104–2112
Gothesen O, Espehaug B, Havelin L, Petursson G, Lygre S, Ellison P et al (2013) Survival rates and causes of revision in cemented primary total knee replacement: a report from the Norwegian Arthroplasty Register 1994–2009. Bone Joint J 95-B:636–642
Hansson U, Toksvig-Larsen S, Jorn LP, Ryd L (2005) Mobile vs. fixed meniscal bearing in total knee replacement: a randomised radiostereometric study. Knee 12:414–418
Hanusch B, Lou TN, Warriner G, Hui A, Gregg P (2010) Functional outcome of PFC Sigma fixed and rotating-platform total knee arthroplasty. A prospective randomised controlled trial. Int Orthop 34:349–354
Hao D, Wang J (2021) Fixed-bearing vs mobile-bearing prostheses for total knee arthroplasty after approximately 10 years of follow-up: a meta-analysis. J Orthop Surg Res 16:437
Harrington MA, Hopkinson WJ, Hsu P, Manion L (2009) Fixed- vs mobile-bearing total knee arthroplasty: does it make a difference?—a prospective randomized study. J Arthroplasty 24:24–27
Hasegawa M, Sudo A, Uchida A (2009) Staged bilateral mobile-bearing and fixed-bearing total knee arthroplasty in the same patients: a prospective comparison of a posterior-stabilized prosthesis. Knee Surg Sports Traumatol Arthrosc 17:237–243
Henricson A, Dalen T, Nilsson KG (2006) Mobile bearings do not improve fixation in cemented total knee arthroplasty. Clin Orthop Relat Res 448:114–121
Hernigou P, Huys M, Pariat J, Roubineau F, Flouzat Lachaniette CH, Dubory A (2018) Comparison of fixed-bearing and mobile-bearing total knee arthroplasty after high tibial osteotomy. Int Orthop 42:317–322
Hofstede SN, Nouta KA, Jacobs W, van Hooff ML, Wymenga AB, Pijls BG et al (2015) Mobile bearing vs fixed bearing prostheses for posterior cruciate retaining total knee arthroplasty for postoperative functional status in patients with osteoarthritis and rheumatoid arthritis. Cochrane Database Syst Rev. https://doi.org/10.1002/14651858.CD003130.pub3CD003130
Hoshi K, Watanabe G, Kurose Y, Tanaka R, Fujii J, Gamada K (2020) Mobile-bearing insert used with total knee arthroplasty does not rotate on the tibial tray during a squatting activity: a cross-sectional study. J Orthop Surg Res 15:114
Howick J CI, Glasziou P, Greenhalgh T, Carl Heneghan, Liberati A, Moschetti I, Phillips B, Thornton H, Goddard O, Hodgkinson M (2011) The 2011 Oxford CEBM levels of evidence. Oxford Centre for Evidence-Based Medicine. Available at: https://www.cebm.net/. Accessed May 2022
Jacobs WC, Christen B, Wymenga AB, Schuster A, van der Schaaf DB, ten Ham A et al (2012) Functional performance of mobile versus fixed bearing total knee prostheses: a randomised controlled trial. Knee Surg Sports Traumatol Arthrosc 20:1450–1455
Jamshed S, Shah R, Arooj A, Turner A, Plakogiannis C (2020) A novel radiographic technique to assess 180 degrees rotational spin of the Oxford unicompartmental knee mobile bearing. J Orthop 21:438–443
Jolles BM, Grzesiak A, Eudier A, Dejnabadi H, Voracek C, Pichonnaz C et al (2012) A randomised controlled clinical trial and gait analysis of fixed- and mobile-bearing total knee replacements with a five-year follow-up. J Bone Joint Surg Br 94:648–655
Kalisvaart MM, Pagnano MW, Trousdale RT, Stuart MJ, Hanssen AD (2012) Randomized clinical trial of rotating-platform and fixed-bearing total knee arthroplasty: no clinically detectable differences at five years. J Bone Joint Surg Am 94:481–489
Khow YZ, Liow MHL, Goh GS, Chen JY, Lo NN, Yeo SJ (2021) Defining the minimal clinically important difference for the knee society score following revision total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. https://doi.org/10.1007/s00167-021-06628-2
Killen CJ, Murphy MP, Hopkinson WJ, Harrington MA, Adams WH, Rees HW (2020) Minimum twelve-year follow-up of fixed- vs mobile-bearing total knee arthroplasty: double blinded randomized trial. J Clin Orthop Trauma 11:154–159
Kim D, Seong SC, Lee MC, Lee S (2012) Comparison of the tibiofemoral rotational alignment after mobile and fixed bearing total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc 20:337–345
Kim TK, Chang CB, Kang YG, Chung BJ, Cho HJ, Seong SC (2010) Early clinical outcomes of floating platform mobile-bearing TKA: longitudinal comparison with fixed-bearing TKA. Knee Surg Sports Traumatol Arthrosc 18:879–888
Kim YH, Kim DY, Kim JS (2007) Simultaneous mobile- and fixed-bearing total knee replacement in the same patients. A prospective comparison of mid-term outcomes using a similar design of prosthesis. J Bone Joint Surg Br 89:904–910
Kim YH, Kim JS (2009) Prevalence of osteolysis after simultaneous bilateral fixed- and mobile-bearing total knee arthroplasties in young patients. J Arthroplasty 24:932–940
Kim YH, Kim JS, Choe JW, Kim HJ (2012) Long-term comparison of fixed-bearing and mobile-bearing total knee replacements in patients younger than fifty-one years of age with osteoarthritis. J Bone Joint Surg Am 94:866–873
Kim YH, Park JW, Jang YS (2021) Long-term (Up to 27 years) prospective, randomized study of mobile-bearing and fixed-bearing total knee arthroplasties in patients < 60 years of age with osteoarthritis. J Arthroplasty 36:1330–1335
Kim YH, Park JW, Kim JS (2018) Comparison of high-flexion fixed-bearing and high-flexion mobile-bearing total knee arthroplasties—a prospective randomized study. J Arthroplasty 33:130–135
Kim YH, Park JW, Kim JS (2019) The long-term results of simultaneous high-flexion mobile-bearing and fixed-bearing total knee arthroplasties performed in the same patients. J Arthroplasty 34:501–507
Kim YH, Park JW, Kim JS, Kulkarni SS, Kim YH (2014) Long-term clinical outcomes and survivorship of press-fit condylar sigma fixed-bearing and mobile-bearing total knee prostheses in the same patients. J Bone Joint Surg Am 96:e168
Kim YH, Yoon SH, Kim JS (2009) Early outcome of TKA with a medial pivot fixed-bearing prosthesis is worse than with a PFC mobile-bearing prosthesis. Clin Orthop Relat Res 467:493–503
Kim YH, Yoon SH, Kim JS (2007) The long-term results of simultaneous fixed-bearing and mobile-bearing total knee replacements performed in the same patient. J Bone Joint Surg Br 89:1317–1323
Kutzner I, Hallan G, Hol PJ, Furnes O, Gothesen O, Figved W et al (2018) Early aseptic loosening of a mobile-bearing total knee replacement. Acta Orthop 89:77–83
Ladermann A, Lubbeke A, Stern R, Riand N, Fritschy D (2008) Fixed-bearing versus mobile-bearing total knee arthroplasty: a prospective randomised, clinical and radiological study with mid-term results at 7 years. Knee 15:206–210
Ladermann A, Saudan M, Riand N, Fritschy D (2008) Fixed-bearing versus mobile-bearing total knee arthroplasty: a prospective randomized clinical and radiological study. Rev Chir Orthop Reparatrice Appar Mot 94:247–251
Lee WC, Kwan YH, Chong HC, Yeo SJ (2017) The minimal clinically important difference for Knee Society Clinical Rating System after total knee arthroplasty for primary osteoarthritis. Knee Surg Sports Traumatol Arthrosc 25:3354–3359
Lizaur-Utrilla A, Gonzalez-Parreno S, Martinez-Mendez D, Miralles-Munoz FA, Lopez-Prats FA (2020) Minimal clinically important differences and substantial clinical benefits for Knee Society Scores. Knee Surg Sports Traumatol Arthrosc 28:1473–1478
Lizaur-Utrilla A, Sanz-Reig J, Trigueros-Rentero MA (2012) Greater satisfaction in older patients with a mobile-bearing compared with fixed-bearing total knee arthroplasty. J Arthroplasty 27:207–212
Maffulli GD, Bridgman S, Maffulli N (2012) Early functional outcome after subvastus or parapatellar approach in knee arthroplasty is comparable. Knee Surg Sports Traumatol Arthrosc 20:1883–1884 (author reply 1885–1886)
Mahoney OM, Kinsey TL, D’Errico TJ, Shen J (2012) The John Insall Award: no functional advantage of a mobile bearing posterior stabilized TKA. Clin Orthop Relat Res 470:33–44
Malahias MA, Manolopoulos PP, Mancino F, Jang SJ, Gu A, Giotis D et al (2021) Safety and outcome of simultaneous bilateral unicompartmental knee arthroplasty: a systematic review. J Orthop 24:58–64
Mannani M, Motififard M, Farajzadegan Z, Nemati A (2022) Length of stay in patients undergoing total knee arthroplasty. J Orthop 32:121–124
Marques CJ, Daniel S, Sufi-Siavach A, Lampe F (2015) No differences in clinical outcomes between fixed- and mobile-bearing computer-assisted total knee arthroplasties and no correlations between navigation data and clinical scores. Knee Surg Sports Traumatol Arthrosc 23:1660–1668
Matsuda S, Mizu-uchi H, Fukagawa S, Miura H, Okazaki K, Matsuda H et al (2010) Mobile-bearing prosthesis did not improve mid-term clinical results of total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc 18:1311–1316
Migliorini F, Aretini P, Driessen A, El Mansy Y, Quack V, Tingart M et al (2020) Better outcomes after mini-subvastus approach for primary total knee arthroplasty: a Bayesian network meta-analysis. Eur J Orthop Surg Traumatol 30:979–992
Migliorini F, Eschweiler J, Baroncini A, Tingart M, Maffulli N (2020) Better outcomes after minimally invasive surgeries compared to the standard invasive medial parapatellar approach for total knee arthroplasty: a meta-analysis. Knee Surg Sports Traumatol Arthrosc. https://doi.org/10.1007/s00167-020-06306-9
Migliorini F, Eschweiler J, Mansy YE, Quack V, Schenker H, Tingart M et al (2020) Gap balancing versus measured resection for primary total knee arthroplasty: a meta-analysis study. Arch Orthop Trauma Surg 140:1245–1253
Migliorini F, Eschweiler J, Niewiera M, El Mansy Y, Tingart M, Rath B (2019) Better outcomes with patellar resurfacing during primary total knee arthroplasty: a meta-analysis study. Arch Orthop Trauma Surg 139:1445–1454
Migliorini F, Eschweiler J, Tingart M, Rath B (2019) Posterior-stabilized versus cruciate-retained implants for total knee arthroplasty: a meta-analysis of clinical trials. Eur J Orthop Surg Traumatol 29:937–946
Migliorini F, Maffulli N, Cuozzo F, Elsner K, Hildebrand F, Eschweiler J et al (2022) Mobile bearing versus fixed bearing for unicompartmental arthroplasty in monocompartmental osteoarthritis of the knee: a meta-analysis. J Clin Med 11:2837
Minoda Y, Iwaki H, Ikebuchi M, Yoshida T, Mizokawa S, Itokazu M et al (2015) Mobile-bearing prosthesis and intraoperative gap balancing are not predictors of superior knee flexion: a prospective randomized study. Knee Surg Sports Traumatol Arthrosc 23:1986–1992
Morikawa LH, Combs DB, Andrews SN, Mathews K, Nakasone CK (2021) Component positioning of the first 300 mobile bearing unicompartmental knee arthroplasties. J Orthop 27:9–12
Mortman R, Gioia C, Stake S, Berger PZ, Gu A, Fassihi SC et al (2021) Linked kinematic knee balancing in unicompartmental knee arthroplasty. J Orthop 24:182–185
Moskal JT, Capps SG (2014) Rotating-platform TKA no different from fixed-bearing TKA regarding survivorship or performance: a meta-analysis. Clin Orthop Relat Res 472:2185–2193
Nutton RW, Wade FA, Coutts FJ, van der Linden ML (2012) Does a mobile-bearing, high-flexion design increase knee flexion after total knee replacement? J Bone Joint Surg Br 94:1051–1057
Okamoto N, Nakamura E, Nishioka H, Karasugi T, Okada T, Mizuta H (2014) In vivo kinematic comparison between mobile-bearing and fixed-bearing total knee arthroplasty during step-up activity. J Arthroplasty 29:2393–2396
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD et al (2021) The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 372:n71
Pagnano MW, Trousdale RT, Stuart MJ, Hanssen AD, Jacofsky DJ (2004) Rotating platform knees did not improve patellar tracking: a prospective, randomized study of 240 primary total knee arthroplasties. Clin Orthop Relat Res 428:221–227
Park CH, Kang SG, Bae DK, Song SJ (2019) Mid-term clinical and radiological results do not differ between fixed- and mobile-bearing total knee arthroplasty using titanium-nitride-coated posterior-stabilized prostheses: a prospective randomized controlled trial. Knee Surg Sports Traumatol Arthrosc 27:1165–1173
Pijls BG, Valstar ER, Kaptein BL, Nelissen RG (2012) Differences in long-term fixation between mobile-bearing and fixed-bearing knee prostheses at ten to 12 years’ follow-up: a single-blinded randomised controlled radiostereometric trial. J Bone Joint Surg Br 94:1366–1371
Poirier N, Graf P, Dubrana F (2015) Mobile-bearing versus fixed-bearing total knee implants. Results of a series of 100 randomised cases after 9 years follow-up. Orthop Traumatol Surg Res 101:S187-192
Poornima S, Subramanyam K, Khan IA, G S, Hasan Q, (2019) Role of SREBP2 gene polymorphism on knee osteoarthritis in the South Indian Hyderabad Population: a hospital based study with G595C variant. J Orthop 16:293–297
Powell AJ, Crua E, Chong BC, Gordon R, McAuslan A, Pitto RP et al (2018) A randomized prospective study comparing mobile-bearing against fixed-bearing PFC Sigma cruciate-retaining total knee arthroplasties with ten-year minimum follow-up. Bone Joint J 100-B:1336–1344
Price AJ, Rees JL, Beard D, Juszczak E, Carter S, White S et al (2003) A mobile-bearing total knee prosthesis compared with a fixed-bearing prosthesis. A multicentre single-blind randomised controlled trial. J Bone Joint Surg Br 85:62–67
Radetzki F, Wienke A, Mendel T, Gutteck N, Delank KS, Wohlrab D (2013) High flex total knee arthroplasty—a prospective, randomized study with results after 10 years. Acta Orthop Belg 79:536–540
Rahman WA, Garbuz DS, Masri BA (2010) Randomized controlled trial of radiographic and patient-assessed outcomes following fixed versus rotating platform total knee arthroplasty. J Arthroplasty 25:1201–1208
Ranawat CS, Komistek RD, Rodriguez JA, Dennis DA, Anderle M (2004) In vivo kinematics for fixed and mobile-bearing posterior stabilized knee prostheses. Clin Orthop Relat Res 418:184–190
Riaz O, Aqil A, Sisodia G, Chakrabarty G (2017) P.F.C Sigma((R)) cruciate retaining fixed-bearing versus mobile-bearing knee arthroplasty: a prospective comparative study with minimum 10-year follow-up. Eur J Orthop Surg Traumatol 27:1145–1149
Ries C, Heinichen M, Dietrich F, Jakubowitz E, Sobau C, Heisel C (2013) Short-keeled cemented tibial components show an increased risk for aseptic loosening. Clin Orthop Relat Res 471:1008–1013
Roh YW, Jang J, Choi WC, Lee JK, Chun SH, Lee S et al (2013) Preservation of the posterior cruciate ligament is not helpful in highly conforming mobile-bearing total knee arthroplasty: a randomized controlled study. Knee Surg Sports Traumatol Arthrosc 21:2850–2859
Ruckenstuhl P, Revelant F, Hauer G, Bernhardt GA, Leitner L, Gruber G et al (2022) No difference in clinical outcome, pain, and range of motion between fixed and mobile bearing Attune total knee arthroplasty: a prospective single-center trial. BMC Musculoskelet Disord 23:413
Sappey-Marinier E, de Abreu FGA, O’Loughlin P, Gaillard R, Neyret P, Lustig S et al (2020) No difference in patellar position between mobile-bearing and fixed-bearing total knee arthroplasty for medial osteoarthritis: a prospective randomized study. Knee Surg Sports Traumatol Arthrosc 28:1542–1550
Sappey-Marinier E, Swan J, Maucort-Boulch D, Batailler C, Malatray M, Neyret P et al (2020) No significant clinical and radiological differences between fixed versus mobile bearing total knee replacement using the same semi-constrained implant type: a randomized controlled trial with mean 10 years follow-up. Knee Surg Sports Traumatol Arthrosc. https://doi.org/10.1007/s00167-020-06346-1
Schotanus MGM, Pilot P, Kaptein BL, Draijer WF, Tilman PBJ, Vos R et al (2017) No difference in terms of radiostereometric analysis between fixed- and mobile-bearing total knee arthroplasty: a randomized, single-blind, controlled trial. Knee Surg Sports Traumatol Arthrosc 25:2978–2985
Schotanus MGM, Pilot P, Vos R, Kort NP (2017) No difference in joint awareness after mobile- and fixed-bearing total knee arthroplasty: 3-year follow-up of a randomized controlled trial. Eur J Orthop Surg Traumatol 27:1151–1155
Scott CE, Biant LC (2012) The role of the design of tibial components and stems in knee replacement. J Bone Joint Surg Br 94:1009–1015
Scuderi GR, Hedden DR, Maltry JA, Traina SM, Sheinkop MB, Hartzband MA (2012) Early clinical results of a high-flexion, posterior-stabilized, mobile-bearing total knee arthroplasty: a US investigational device exemption trial. J Arthroplasty 27:421–429
Shemshaki H, Dehghani M, Eshaghi MA, Esfahani MF (2012) Fixed versus mobile weight-bearing prosthesis in total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc 20:2519–2527
Smith H, Jan M, Mahomed NN, Davey JR, Gandhi R (2011) Meta-analysis and systematic review of clinical outcomes comparing mobile bearing and fixed bearing total knee arthroplasty. J Arthroplasty 26:1205–1213
Song SJ, Lee HW, Bae DK, Park CH (2020) High incidence of tibial component loosening after total knee arthroplasty using ceramic titanium-nitride-coated mobile bearing prosthesis in moderate to severe varus deformity: a matched-pair study between ceramic-coated mobile bearing and fixed bearing prostheses. J Arthroplasty 35:1003–1008
Tiwari V, Meshram P, Park CK, Bansal V, Kim TK (2019) New mobile-bearing TKA with unique ball and socket post-cam mechanism offers similar function and stability with better prosthesis fit and gap balancing compared to an established fixed-bearing prosthesis. Knee Surg Sports Traumatol Arthrosc 27:2145–2154
Tjornild M, Soballe K, Hansen PM, Holm C, Stilling M (2015) Mobile- vs. fixed-bearing total knee replacement. Acta Orthop 86:208–214
Tornese D, Robustelli A, Ricci G, Rancoita PMV, Maffulli N, Peretti GM (2021) Predictors of postoperative hospital length of stay after total knee arthroplasty. Singapore Med J. https://doi.org/10.11622/smedj.2021142
Urwin SG, Kader DF, Caplan N, St Clair Gibson A, Stewart S (2014) Gait analysis of fixed bearing and mobile bearing total knee prostheses during walking: do mobile bearings offer functional advantages? Knee 21:391–395
Van Hamersveld KT, Marang-Van De Mheen PJ, Van Der Heide HJL, Der Linden-Van V, Der Zwaag HMJ, Valstar ER, Nelissen R (2018) Migration and clinical outcome of mobile-bearing versus fixed-bearing single-radius total knee arthroplasty. Acta Orthop 89:190–196
Vasdev A, Kumar S, Chadha G, Mandal SP (2009) Fixed- versus mobile-bearing total knee arthroplasty in Indian patients. J Orthop Surg 17:179–182
Watanabe T, Tomita T, Fujii M, Hashimoto J, Sugamoto K, Yoshikawa H (2005) Comparison between mobile-bearing and fixed-bearing knees in bilateral total knee replacements. Int Orthop 29:179–181
Wohlrab D, Ditl J, Herrschelmann R, Schietsch U, Hein W, Hube R (2005) Does the NexGen LPS flex mobile knee prosthesis offer advantages compared to the NexGen LPS?—a comparison of clinical and radiological results. Z Orthop Ihre Grenzgeb 143:567–572
Woolson ST, Epstein NJ, Huddleston JI (2011) Long-term comparison of mobile-bearing vs fixed-bearing total knee arthroplasty. J Arthroplasty 26:1219–1223
Wylde V, Learmonth I, Potter A, Bettinson K, Lingard E (2008) Patient-reported outcomes after fixed- versus mobile-bearing total knee replacement: a multi-centre randomised controlled trial using the Kinemax total knee replacement. J Bone Joint Surg Br 90:1172–1179
Zeng YM, Yan MN, Li HW, Zhang J, Wang Y (2020) Does mobile-bearing have better flexion and axial rotation than fixed-bearing in total knee arthroplasty? A randomised controlled study based on gait. J Orthop Translat 20:86–93
Acknowledgements
None.
Funding
Open Access funding enabled and organized by Projekt DEAL. The authors received no financial or material support for the research, authorship, and/or publication of this article.
Author information
Authors and Affiliations
Contributions
FM: writing, revising, selection, data collection, data extraction, synthesis methods, study risk of bias assessment, final approval; KE: writing, revising, study selection, data collection, data extraction, study risk of bias assessment, final approval; MP: writing, revising, final approval; FC: writing, revising, final approval; FH: writing, revising, study risk of bias assessment, final approval; JE: writing, revising, final approval; NM: writing, revising, final approval.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have any competing interests for this article.
Ethical approval
This study complies with ethical standards.
Consent to publish
Not applicable.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Migliorini, F., Maffulli, N., Cuozzo, F. et al. No difference between mobile and fixed bearing in primary total knee arthroplasty: a meta-analysis. Knee Surg Sports Traumatol Arthrosc 30, 3138–3154 (2022). https://doi.org/10.1007/s00167-022-07065-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-022-07065-5