
Abstract
Summary
We investigated the association between bisphosphonate and denosumab use and risk of hip fracture in Norway. These drugs protect against fractures in clinical trials, but their population-level effect is unknown. Our results showed lowered risk of hip fracture for treated women. Treatment of high-risk individuals could prevent future hip fractures.
Purpose
To investigate whether bisphosphonates and denosumab reduced the risk of first-time hip fracture in Norwegian women when adjusting for a medication-based comorbidity index.
Methods
Norwegian women aged 50–89 in 2005–2016 were included. The Norwegian prescription database (NorPD) supplied data on exposures to bisphosphonates, denosumab, and other drugs for the calculation of the Rx-Risk Comorbidity Index. Information on all hip fractures treated in hospitals in Norway was available. Flexible parametric survival analysis was used with age as time scale and with time-varying exposure to bisphosphonates and denosumab. Individuals were followed until hip fracture or censoring (death, emigration, age 90 years), or 31 December 2016, whichever occurred first. Rx-Risk score was included as a time-varying covariate. Other covariates were marital status, education, and time-varying use of bisphosphonates or denosumab with other indications than osteoporosis.
Results
Of 1,044,661 women 77,755 (7.2%) were ever-exposed to bisphosphonate and 4483 (0.4%) to denosumab. The fully adjusted hazard ratios (HR) were 0.95 (95% confidence interval (CI): 0.91–0.99) for bisphosphonate use and 0.60 (95% CI: 0.47–0.76) for denosumab use. Bisphosphonate treatment gave a significantly reduced risk of hip fracture compared with the population after 3 years and denosumab after 6 months. Fracture risk was lowest in denosumab users who had previously used bisphosphonate: HR 0.42 (95% CI: 0.29–0.61) compared with the unexposed population.
Conclusions
In population-wide real-world data, women exposed to bisphosphonates and denosumab had a lower hip fracture risk than the unexposed population after adjusting for comorbidity. Treatment duration and treatment history impacted fracture risk.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Norway has one of the highest incidence rates of hip fracture in the world [1,2,3]. Over the last two decades, there has been a decrease in incidence, but because of the increasing number of elderly in the population, the total annual number of hip fractures has been stable and is forecasted to increase [4].
Guidelines in Europe recommend bisphosphonates as first choice of treatment of osteoporosis and for fracture prevention [5], with alendronate being the most commonly used drug in Norway [6, 7]. While oral bisphosphonates have been in use since the late 1990s, denosumab for osteoporosis (Prolia™) was introduced in 2010 and is mostly prescribed as second-line treatment or as first-line for people with contraindications to bisphosphonate use [7, 8]. The efficacy of alendronate and other anti-osteoporosis drugs (AOD) in preventing fractures has been extensively investigated in clinical studies [9,10,11,12]. A recent review of meta-analyses and network meta-analyses of clinical trials showed that oral and parenteral bisphosphonates and denosumab were similarly efficient in reducing hip fracture risk in postmenopausal women, with relative risks between 0.45 and 0.64 for alendronate and between 0.50 and 0.60 for denosumab [13].
Although results from randomized controlled trials (RCTs) are considered the gold standard and form the basis for treatment guidelines, their external validity is limited. An international cross-sectional study showed that more than half of incident users of alendronate in 2005–2007 would not have qualified for inclusion in the Fracture Intervention Trial, a large, early RCT of alendronate [14]. The exclusion criteria in that study included age at or above 80 years. Adherence to and persistence with anti-osteoporosis drug treatment can also be low [15]. Despite convincing effects in RCTs, treatment uptake is low in many countries [16]. In a cohort study of Norwegians, only 24% of women with high risk of osteoporotic fracture used an anti-osteoporotic drug during the first 2 years following their risk assessment [17].
The efficacy of anti-osteoporosis drugs has to a limited extent been studied in a real-world setting. A recent observational study of Swedish women who started osteoporosis treatment and served as their own controls after the first 3 months of treatment showed an incidence rate ratio of 0.74 for hip fracture in the following 12 months [18], a reduction which is in line with results from RCTs [9]. A large longitudinal study on US women with a similar within-user design also found reduced incidence rates of hip fractures after initiation of treatment with either denosumab or bisphosphonate [19]. A study of French women using bisphosphonates found no significant protection on hip fracture risk [20]. None of these studies examined the risk of hip fracture according to duration of drug use.
Considering the apparent undertreatment of osteoporosis and limited knowledge of the effectiveness on the population level, we aimed to investigate whether use of bisphosphonates or denosumab protects against first-time hip fracture using real-world data on the female population aged 50–89 years in Norway from 2005 through 2016.
Methods
Study population and data sources
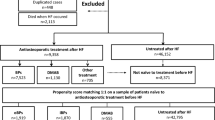
In this registry-based cohort study, the source population was the full Norwegian adult population identified in the Norwegian Population and Housing Census 2001 who were alive and residing in Norway by 1 January 2005. The study population were women aged between 50 and 89 years in the study period, defined as from January 2005 through December 2016. Individuals were included from the start of study in January 2005 or, for those currently aged < 50, January of the year of their 50th birthday. Year of birth thus ranged from 1916 through 1966.
Residential status and dates of death and emigration from the National Population Register were provided by Statistics Norway. The Norwegian Population and Housing Census 2001 provided year of birth, educational level, marital status, and urbanisation level of municipality of residence in 2001. These data were linked with information on filled prescriptions recorded in the Norwegian Prescription Database (NorPD) for the years 2005–2016 [21]. The NorPD contains data on all prescription drugs dispensed by pharmacies in Norway since 2004. For every filling, the drug name, dosage form, marketing name, and amount are registered. Amount of drug dispensed is registered in defined daily doses (DDDs), as per the World Health Organization Collaborating Centre for Drug Statistics Methodology [22]. Prescription filling data were used both to identify exposure to the drugs under study and to calculate the medication-based Rx-Risk Comorbidity Index [23]. Data on incident hip fractures in 1994–2016 were available in the Norwegian Epidemiologic Osteoporosis Studies (NOREPOS) hip fracture database and linked to the data on an individual level [24]. This database includes quality-assured information on all hip fractures treated in hospitals in Norway (http://www.norepos.no/documentation). Women who had suffered a hip fracture prior to the study period (i.e., between 1994 and 2004) were excluded, as were women who were exposed to bisphosphonates or denosumab the year before inclusion (1 year washout to exclude prevalent users).
Exposures
The drug exposures studied were bisphosphonates and denosumab for osteoporosis, prescribed in the study period. Drugs were distinguished by marketing name and grouped by the active ingredient and indication according to the Norwegian Pharmaceutical Product Compendium [25]. Bisphosphonates with osteoporosis as indication included alendronate (anatomical therapeutic chemical [ATC] code M05BA04), ibandronic acid (ATC code M05BA06), risedronic acid (ATC code M05BA07), and zoledronic acid (Aclasta™) (ATC code M05BA04), and denosumab with osteoporosis as indication included denosumab (Prolia™) (ATC code M05BX04). Within each of the two medication groups, we allowed exposure status (exposed/unexposed) to vary over time. The start of exposure was set at the date of filling the first prescription. Bisphosphonates were assigned an end of exposure according to the amount filled (in DDDs) with an additional 6 months to accommodate these drugs’ persisting effect [26]. Denosumab (Prolia™) is given as an injection with a dose covering 6 months, corresponding to 182.625 DDD, with no persisting effect [5]. Therefore, each prescription of denosumab was assigned an end of exposure according to the amount filled in DDDs, without any addition of time. For some drugs (injectable forms of ibandronic acid and zoledronic acid in the formulation marketed as Aclasta™), the registered DDDs were adjusted, as their values were not based on the dosage used in osteoporosis treatment [22]. The adjusted DDD corresponded to the dosage used when treating osteoporosis as listed in the Norwegian Pharmaceutical Product Compendium [25].
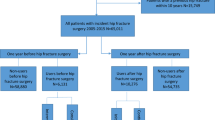
Risk of hip fracture by duration of current treatment was further investigated in five stages: 1–5 months, 6–11 months, 12–23 months, 24–35 months, and 36 months or more. Duration was calculated in a cumulative fashion, without regard to pauses in exposure. Each individual’s duration of treatment was time-varying and updated if they persisted on or re-initiated the treatment.
In addition, risk of hip fracture by treatment history was examined in four categories to indicate current bisphosphonate or denosumab treatment with or without previous treatment with the other drug type. Treatment history was also time-varying, updated according to the individual’s treatment trajectory.
Outcome
The outcome of interest was an individual’s first hip fracture occurring after start of follow-up. The date of hip fracture was set to that of the individual’s first occurrence in the NOREPOS hip fracture database.
Covariates
Filling of prescriptions of bisphosphonates and denosumab with an indication other than osteoporosis was included as two separate binary time-varying covariates constructed in the same way as the main exposure variables. These included the bisphosphonates etidronic acid (ATC code M05BA01), clodronic acid (ATC code M05BA02), pamidronic acid (ATC code M05BA03), and zoledronic acid (all formulations other than Aclasta™) and denosumab with the marketing name Xgeva™ (ATC code M05BX04).
Demographic covariates included decade of birth, sex, marital status, educational level, and urbanisation level of municipality of residence. Marital status was dichotomized into married/registered partner vs. not married. Attained educational level was grouped into nine levels according to the Norwegian Standard Classification of Education [27], and further combined into three levels: low (0 to 10 years of schooling), medium (11 to 14 years of schooling, including post-secondary schooling but not higher level education), and high (undergraduate, graduate, and postgraduate education). All municipalities were grouped in three categories based on the proportion living in densely populated areas (defined as < 50 m between houses): low (rural, less than one-third), medium (semirural, between one-third, and two-thirds), and high (urban, more than two-thirds), and each resident was assigned the urbanization level of their residential municipality [28].
In addition, a time-varying Rx-Risk Comorbidity Index score, updated every odd calendar year, was calculated for each individual based on their filled prescriptions in the NorPD [23]. The ATC-mapped Rx-Risk score was based on the number of different comorbidity categories (of a total of 45) from which the individual had filled a prescription in a specific calendar year, where each category has been assigned an empirical severity weight from − 1 through 6 according to the age- and sex-adjusted one-year mortality associated with the category (Supplementary Table 1). Finally, each person’s score was calculated as the net sum of weights for all categories from which the person had filled at least one prescription in the calendar year. Last observation was carried forward if the Rx-Risk Comorbidity Index score was missing in a next 2-year period. Rx-Risk scores ranging from − 8 to 54 were grouped into 13 categories (< 0, 0, 1, …9, ≥ 10, missing). Having no filled prescriptions could indicate institutionalisation since prescriptions given in hospitals and nursing homes are not recorded in the NorPD.
Statistical analysis
We fitted flexible parametric survival models using the stpm2 command in Stata/SE 17.0 for Windows to estimate hazard ratios (HRs) of hip fracture, with associated 95% confidence intervals (CIs), for individuals currently exposed to bisphosphonates and denosumab, respectively, compared to currently unexposed individuals. The analysis unit was person-time, and the time scale was attained age (in months since January in the year of the individual’s 50th birthday). Individuals were followed from 1 January 2005 (or from 1 January in the calendar year of their 50th birthday if younger than 50 years in 2005) until their first hip fracture, emigration, death, 31 December of the year of their 89th birthday or end of study on 31 December 2016, whichever occurred first. We performed three analyses with different characterisations of exposure. First, risk of hip fracture was investigated in person-time under exposure to bisphosphonates or denosumab vs. unexposed person-time, disregarding treatment duration and history. Second, we examined risk according to treatment duration for the drug in question across categories ranging from < 6 months to ≥ 36 months. Third, we examined risk according to treatment history, separating between denosumab use with and without previous bisphosphonate use, and correspondingly, separating between bisphosphonate use with or without previous denosumab use. Unexposed person-time (non-use of anti-osteoporosis drugs) in the total study population of women was the reference level in all analyses. The base model, performed for the first main analysis only, included mutual adjustment for any of the study drugs with or without osteoporosis as indication. In the fully adjusted model, we also included the Rx-Risk Comorbidity Index score as a time-varying categorical variable, and educational level, marital status, and decade of birth year as fixed covariates. Level of urbanisation did not influence the estimates for bisphosphonates and denosumab and was not included in the analyses. All analyses were performed separately for men and women.
First, models without time-dependent effects of exposure to bisphosphonates and denosumab were fitted to yield overall HR estimates, assuming proportional hazards [29]. Further, we fitted a model allowing for time-dependent effects of bisphosphonates and denosumab, respectively, by including the tvc option in the stpm2 command. In this last analysis, treatment duration or history was not taken into account.
A sensitivity analysis of the first main analysis was also performed where individuals were not considered as exposed to oral bisphosphonates (alendronate, risedronic acid, oral formulations of ibandronic acid, etidronic acid, and clodronic acid) until the second filling of a prescription of bisphosphonate tablets. No changes were made to the exposure definitions of the parenteral treatments.
Results
More than 1 million women were included in the study. On average, the women were followed for more than 8 years (Table 1). When restricting to drugs with osteoporosis as indication, 7.2% of women were exposed to bisphosphonates and 0.4% were exposed to denosumab during the 12-year study period (Table 1).
There was a marginally longer total time of exposure to anti-osteoporosis drugs for women who had an ever-exposure to denosumab, compared to women who only had ever-exposure to bisphosphonates. Among women ever-exposed to denosumab, 67.9% also had ever-exposed to bisphosphonates (data not shown). Of the women ever-exposed to both drugs, 97.4% had their first bisphosphonate exposure before their first denosumab exposure. These women had an average of 3.1 years (standard deviation 2.7) with bisphosphonate exposure before denosumab initiation.
For the ever-exposed women, both median Rx-Risk score and average age, naturally, was higher at the start of exposure than at the start of observation (Table 1).
Risk of hip fracture according to use of anti-osteoporosis drugs
With full adjustment, the overall HR of hip fracture between women exposed and unexposed to bisphosphonates was 0.95 (95% CI: 0.91–0.99) when disregarding treatment duration and history (Table 2). The corresponding HR of hip fracture between women exposed and unexposed to denosumab in the fully adjusted model was 0.60 (95% CI: 0.47–0.76). The time-dependent HR of hip fracture in women treated with bisphosphonates varied across attained age (Fig. 1). For women above approximately 81 years of age, treatment with bisphosphonates was associated with reduced HR of hip fracture. The HR estimate for denosumab exposure was below 1 for women of all ages, but statistically significant only for women above approximately 79 years of age (Fig. 2).

Time-dependent hazard ratios with 95% confidence intervals for hip fracture according to use of bisphosphonates (yes/no) in women in Norway, ages 52–89. Adjusted for marital status, 10-year birth cohort, education level, Rx-Risk index score, use of denosumab and use of bisphosphonate on other indications than osteoporosis. Age as time scale. The horizontal line indicates the null effect (HR = 1). Figure created in Stata/SE 17.0

Time-dependent hazard ratios with 95% confidence intervals for hip fracture according to use of denosumab (yes/no) in women in Norway, ages 60–89. Adjusted for marital status, 10-year birth cohort, education level, Rx-Risk index score, use of bisphosphonate and use of denosumab on other indications than osteoporosis. Age as time scale. The horizontal line indicates the null effect (HR = 1). Figure created in Stata/SE 17.0
The sensitivity analysis requiring two consecutive fillings of a prescription for oral bisphosphonates to assign exposure yielded only a slightly more protective effect of bisphosphonates in women, with an HR of 0.92 (95% CI: 0.88–0.96).
For both bisphosphonate and denosumab exposure, the risk of hip fracture was significantly elevated the first 5 months of treatment (Table 3). For bisphosphonate, the risk of hip fracture was lower for each increasing stage of treatment duration, but this was statistically significant only in those who had reached 3 or more years of treatment. These women had an HR of 0.79 (95% CI: 0.74–0.84). Women treated with denosumab had a significantly reduced risk of hip fracture if they persisted with treatment beyond 6 months. Treatment duration of more than 1 year but less than 2 years, yielded the most protective estimate: HR 0.31 (95% CI: 0.18–0.55) (Table 3).
Women who were initiated on a bisphosphonate had a slightly lower risk of hip fracture than unexposed women (Table 4). In contrast, women who used bisphosphonates after previous denosumab treatment, comprising the smallest subsample of current users, had a non-significant HR estimate of 1.63. When dividing current denosumab use according to previous bisphosphonate use, the HR estimate for women who were initiated on denosumab as their first drug type was non-significant, while women who were exposed to denosumab after receiving bisphosphonate treatment had a reduced risk of hip fracture, with HR 0.42 (95% CI: 0.29–0.61) compared with the unexposed population.
Fully adjusted survival curves showing hip fracture-free time (age) according to drug exposure are shown in Supplementary Figs. 1–4.
Discussion
Individuals with osteoporosis have up to sevenfold increased risk of hip fracture compared to individuals without osteoporosis [30, 31]. We aimed to investigate the effect of osteoporosis treatment on hip fracture risk in real-world data covering the population of women in Norway aged 50–89 years with no prior hip fracture. We found that women exposed to bisphosphonates had a hip fracture risk slightly below the level of unexposed women after adjusting for comorbidity, thus reducing the presumed excess risk of hip fracture associated with osteoporosis medication. Compared to unexposed, exposure to denosumab was associated with an even lower risk of hip fracture in women. For both treatments, the risk of fracture was increased in the first 5 months of treatment, in line with their likely clinical indication for treatment (elevated fracture risk). We observed a time-dependent association for both bisphosphonates and denosumab treatment across attained age, with a significantly reduced risk for hip fracture in the oldest women. Longer durations of treatment gave more protective estimates, for both drugs. Women who were initiated on denosumab after previous bisphosphonate treatment had the lowest risk estimate, with a 58% reduced risk of hip fracture compared with the background female population.
Time of exposure to denosumab was shorter than that to bisphosphonates, but the total duration of exposure to bisphosphonates and denosumab combined was similar between the two ever-exposed groups. Almost 70% of women ever-exposed to denosumab were also ever-exposed to bisphosphonates, and of these more than 97% used the bisphosphonate first. This is in accordance with bisphosphonates being the first-line treatment. It is more widely reimbursed, as denosumab (Prolia™) is directly reimbursed only to women who cannot take bisphosphonates (due to side-effects, contraindications, or unsatisfactory effect) and who are older than 75 years [25]. This last aspect likely explains the age difference at start of treatment between women exposed to bisphosphonates and denosumab. Having already had on average more than 3 years of treatment with bisphosphonate, the women starting denosumab as their second treatment will very likely have had a smaller imminent risk of fracture than the women initiating their first treatment. As seen in Table 3, this duration of bisphosphonate treatment gave a lower HR for hip fracture than in the first analysis, where treatment duration was not considered. This group of women, who transitioned from bisphosphonate to denosumab, were again found to have a lower risk of fracture, in Table 4, where their HR was as low as 0.42 compared with women who were unexposed to any treatment.
In a recent Danish population-based study comparing patients initiated on alendronate and denosumab, there was no difference in risk of hip fracture during 3 years of follow-up [32]. In the US study of real-world effectiveness of osteoporosis treatment, denosumab did have a more protective point estimate (incidence rate ratio) than both oral and parenteral bisphosphonate [19]. In a network meta-analysis of clinical trials from 2019, denosumab was effective in reducing hip fracture risk only when compared to placebo [11]. As these findings were based on RCTs, they may not be fully applicable to the real world. Our finding of a lower risk of hip fracture whilst exposed to denosumab may in part be explained by the accumulated treatment with bisphosphonate many of these women had. Having had a minimum of 3 years of bisphosphonate treatment gave an HR of 0.79 in our data, whilst using denosumab after bisphosphonate gave an HR of 0.41. One factor that may contribute to a more protective effect of denosumab is that of adherence and persistence. Oral alendronate is the most commonly used bisphosphonate, often prescribed in a once-a-week regimen [6]. This likely makes it more vulnerable to missed doses, in contrast to denosumab, which is administered by injection twice a year. There may also be some healthy user-bias in the group of women who transition to denosumab, who may be characterized by a higher degree of health literacy and have over-all better health. We have taken such variation into account by adjusting for educational level and a broad medication-based comorbidity index (Rx-Risk), although residual confounding may remain.
In the analysis with time-dependent effects, we found significantly reduced HR for women treated with bisphosphonates in older age (80–89). This is the age-group with the highest incidence of hip fracture [3, 33]. The younger age-groups are those most often included in RCTs, whilst women above 80 were for example not included in the Fracture Intervention Trial of alendronate [14]. Although our population was restricted to those who had not had a hip fracture previously, the proportion of prescriptions of anti-osteoporosis drugs representing secondary prevention after having experienced a forearm or other fracture is unknown. At younger ages, the prescriptions may to a larger degree be linked to secondary osteoporosis due to, e.g., premature menopause, prior anti-oestrogen treatment, gastro-intestinal disease or genetic susceptibility for low bone mass, rather than old age and overall poorer health and frailty, factors that can be partly captured in higher Rx Risk scores. The share of secondary osteoporosis in post-menopausal women is poorly documented, but it has been reported at 20 and 30% [34, 35]. That is, in our analysis, we may be capturing more of the confounding by indication for the older treated population, than for the younger treated population. In a population-based regional health study covering a subset of the Norwegian population, fracture risk among women and men exposed to bisphosphonates was studied using a similar time-varying exposure as in our study [36]. After adjustment for age and a fracture-risk score (FRAX®) based on clinical predictors [37], exposure to bisphosphonates was associated with a reduced risk of hip fracture in women, with an HR of 0.68 (95% CI: 0.46–1.02). This is a lower estimate than ours, albeit not statistically significant and with a wider 95% CI. The latter study only included individuals up until the age of 85 and most probably had a better opportunity to capture confounding by indication also among the younger participants because of more clinical variables.
A Swedish study showed reductions in fracture risk associated with treatment with any of several anti-osteoporosis drugs [18]. Their design reduced the risk of confounding by indication by allowing each treated individual to serve as their own control, using the first treatment period as an indicator of baseline risk and comparing this with a later treatment period. This setup allows to control for an individual’s underlying fracture risk. For women aged 80 years and older, the incidence rate ratio (IRR) of hip fracture between treated and untreated periods was 0.81 (95% CI: 0.68–0.95), whilst it was 0.69 (95% CI: 0.57–0.84) for women aged 60–79 years. These results lie between our risk estimates for women treated with bisphosphonates and denosumab, respectively. Contrary to our results, they found a more pronounced protection in the younger age group. A recent German study had a similar design with self-control and showed an IRR of hip fracture of 0.83 (95% CI: 0.38–1.84) for women treated with denosumab and 0.63 (95% CI: 0.41–0.97) for women treated with oral bisphosphonates [38]. In the Swedish study, the respective effects of different types of anti-osteoporosis drugs could not be distinguished, and the design of both studies is also fundamentally different from ours since they did not include a comparison with the untreated population.
At treatment initiation, risk of hip fracture is high [19]. Any fractures occurring shortly after initiating treatment may biologically not have been preventable by the treatment. This is especially the case for oral bisphosphonates, which may not be clinically effective until 12 months of use and treatment effect is shown to be increasing with duration and adherence [39, 40]. In our sensitivity analysis, we categorised individuals initiated on oral bisphosphonates as unexposed until the filling of their second prescription. This sensitivity analysis did not appreciably alter the findings of the first main analysis. In the analysis where we looked at the effect of duration of treatment, we can plainly see the high risk of fracture at initiation, with HRs close to and above 2 for women treated less than 6 months for both bisphosphonates and denosumab. At treatment initiation, the women had a larger risk of fracture than their non-exposed peers. With persistent treatment, their risk fell below that of their non-treated peers. The tendency of reduced HRs for the longer durations of treatment is clear, even if some stages of duration did not yield statistically significant estimates.
In our analysis of treatment history, one group stands out with a (non-significant) increased risk of fracture compared with non-treated women, the women transitioning to bisphosphonate after denosumab treatment. There is documentation that discontinuation of denosumab increased fracture risk due to rapid bone loss [41]. There is some evidence that bisphosphonate treatment after denosumab discontinuation may partly prevent this bone loss and alleviate the increased risk [42, 43]. In our data, women who transitioned to a bisphosphonate had a risk of hip fracture above that of the non-treated women, but their risk estimate was not quite as high as those of the women recently initiated on bisphosphonate or denosumab.
Strengths and limitations
A major strength of this study is its population-wide scope with the ability to link individual-level data from nationwide administrative databases and health registries based on each resident’s unique personal identification number. To our knowledge, this is one of very few nationwide studies of effectiveness of osteoporosis treatment in a real-world setting. Longitudinal prescription data allowed for inclusion of time-varying exposures in the analyses. In pharmacoepidemiologic studies, a fundamental challenge is confounding by indication that stems from an inherent difference in underlying risk between the treated and untreated population. The study is limited by our lack of data on fractures of other kinds; this could have helped reduce the confounding by indication as osteoporosis increases risk of many types of fractures [44]. We have however tried to take some of this underlying risk difference into account by adjusting for comorbidity expressed by the Rx-Risk Comorbidity Index. This lowered the HR of hip fracture for both exposed groups. Even before adjusting for comorbidity, women exposed to denosumab had a lower risk of hip fracture than unexposed women. The flexible parametric survival analysis allowed for illustration of HRs at different ages, revealing that there was a stronger protective association of bisphosphonates among older women.
The prescription data used in this study does not strictly indicate use, as some individuals who fill their prescription will end up not taking the drug as prescribed. This may lead to misclassification, attenuating the potentially protective effect of the drugs. There are also some Norwegians who receive treatment for osteoporosis in hospitals, care homes and outpatient clinics with infusions of zoledronic acid. This treatment is not registered in the NorPD, and so these individuals will be incorrectly classified as unexposed. To assess the extent of this misclassification, we have accessed wholesale-level data on Aclasta® between 2006 and 2016 (personal communication with Kari Furu at the Norwegian Institute of Public Health, June 2022). After subtracting the DDDs accounted for in the NorPD from the total wholesale DDDs, the remaining Aclasta™ doses not accounted for would cover the treatment of 27 patients in 2006. This number increased gradually to 2323 patients in 2015 and further to 5100 patients in 2016. However, some of this will represent treatment after hip fractures, which is not covered by our study. Overall, this misclassified person-time would be a small fraction of all the person-time in our analysis.
Conclusion
In conclusion, this study indicates a protective effect against hip fracture of bisphosphonates and denosumab in the Norwegian population of adult women. The findings indicate that if a larger proportion of those who have a high risk of hip fracture were to receive preventive medication, more hip fractures could presumably be avoided.
Data Availability
The Corresponding Author may be contacted for information about the data and materials. The data that support the findings of this study are available upon application to the respective data owners (Norwegian Institute of Public Health, Norwegian Directorate of Health, and Statistics Norway) but restrictions apply to the availability of these data, which were used under approval for the purpose of the current research project, and so are not publicly available
References
Kanis JA, Oden A, McCloskey EV, Johansson H, Wahl DA, Cooper C (2012) A systematic review of hip fracture incidence and probability of fracture worldwide. Osteoporos Int 23:2239–2256
Cauley JA, Chalhoub D, Kassem AM, Fuleihan GEH (2014) Geographic and ethnic disparities in osteoporotic fractures. Nat Rev Endocrinol 10(6):338–351.
Kjeldgaard HK, Meyer HE, O'Flaherty M et al (2022) Impact of total hip replacements on the incidence of hip fractures in Norway during 1999–2019. A NOREPOS study. J Bone Miner Res. 37(10):1936–1943
Hagen G, Magnussen J, Tell G, Omsland T (2020) Estimating the future burden of hip fractures in Norway. A NOREPOS study. Bone 131:115156
Kanis JA, Cooper C, Rizzoli R, Reginster JY (2019) European guidance for the diagnosis and management of osteoporosis in postmenopausal women. Osteoporos Int 30:3–44
Sakshaug S (2018) (red) Legemiddelforbruket i Norge 2013–2017 [Drug Consumption in Norway 2013–2017], Legemiddelstatistikk 2018:1. Folkehelseinstituttet, Oslo
Finnes TE, Syversen U, Høiberg M, Pretorius M, Eriksen EF, Olsen AL, Balasuriya C, Grimnes G, Tazmini K, Arsetøy H (2022) Osteoporose. In: Jørgensen AP, Tazmini K (eds) Nasjonal veileder i endokrinologi [National guideline in endocrinology]. https://metodebok.no/endokrinologi. Accessed 28 Oct 2022
Rosen HN (2022) Bisphosphonate therapy for the treatment of osteoporosis. In: Rosen CJ SK, Rubinow K (ed) UpToDate. https://www.uptodate.com/contents/bisphosphonate-therapy-for-the-treatment-of-osteoporosis?search=osteoporosis&source=search_result&selectedTitle=4~150&usage_type=default&display_rank=3#H53. Accessed 2 Nov 2022
Crandall CJ, Newberry SJ, Diamant A, Lim YW, Gellad WF, Booth MJ, Motala A, Shekelle PG (2014) Comparative effectiveness of pharmacologic treatments to prevent fractures: an updated systematic review. Ann Intern Med 161:711–723
Viswanathan M, Reddy S, Berkman N, Cullen K, Middleton JC, Nicholson WK, Kahwati LC (2018) Screening to prevent osteoporotic fractures: updated evidence report and systematic review for the US Preventive Services Task Force. JAMA 319:2532–2551
Barrionuevo P, Kapoor E, Asi N et al (2019) Efficacy of pharmacological therapies for the prevention of fractures in postmenopausal women: a network meta-analysis. J Clin Endocrinol Metab 104:1623–1630
Cummings SR, San Martin J, McClung MR et al (2009) Denosumab for prevention of fractures in postmenopausal women with osteoporosis. N Engl J Med 361:756–765
Iconaru L, Baleanu F, Charles A, Mugisha A, Benoit F, Surquin M, Karmali R, Body JJ, Bergmann P (2021) Which treatment to prevent an imminent fracture? Bone Rep 15:101105
Reyes C, Pottegård A, Schwarz P, Javaid MK, Van Staa TP, Cooper C, Diez-Perez A, Abrahamsen B, Prieto-Alhambra D (2016) Real-life and RCT participants: alendronate users versus FITs’ trial eligibility criterion. Calcif Tissue Int 99:243–249
Olsen KR, Hansen C, Abrahamsen B (2013) Association between refill compliance to oral bisphosphonate treatment, incident fractures, and health care costs—an analysis using national health databases. Osteoporos Int 24:2639–2647
Kanis JA, Norton N, Harvey NC, Jacobson T, Johansson H, Lorentzon M, McCloskey EV, Willers C, Borgström F (2021) SCOPE 2021: a new scorecard for osteoporosis in Europe. Arch Osteoporos 16:82
Hoff M, Skurtveit S, Meyer HE, Langhammer A, Sogaard AJ, Syversen U, Skovlund E, Abrahamsen B, Forsmo S, Schei B (2018) Anti-osteoporosis drug use: too little, too much, or just right? The HUNT study, Norway. Osteoporos Int 29:1875–1885
Ström O, Lauppe R, Ljunggren Ö, Spångéus A, Ortsäter G, O’Kelly J, Åkesson K (2020) Real-world effectiveness of osteoporosis treatment in the oldest old. Osteoporos Int 31:1525–1533
Yusuf AA, Cummings SR, Watts NB, Feudjo MT, Sprafka JM, Zhou J, Guo H, Balasubramanian A, Cooper C (2018) Real-world effectiveness of osteoporosis therapies for fracture reduction in post-menopausal women. Arch Osteoporos 13:33
Bourrion B, Souty C, Fournier L, Vilcu AM, Blanchon T, Böelle PY, Hanslik T, François M (2021) Bisphosphonate use and hospitalization for hip fractures in women: an observational population-based study in France. Int J Environ Res Public Health 18(16):8780
Furu K (2009) Establishment of the nationwide Norwegian Prescription Database (NorPD) – new opportunities for research in pharmacoepidemiology in Norway. Norsk Epidemiologi 18(2)
WHO collaborating Centre for drug statistics methodology. https://www.whocc.no/. Accessed 14 Feb 2022
Holvik K, Hjellvik V, Karlstad Ø, Gunnes N, Hoff M, Tell GS, Meyer HE (2022) Contribution of an extensive medication-based comorbidity index (Rx-Risk) in explaining the excess mortality after hip fracture in older Norwegians: a NOREPOS cohort study. BMJ Open 12:e057823
Søgaard AJ, Meyer HE, Emaus N, Grimnes G, Gjesdal CG, Forsmo S, Schei B, Tell GS (2014) Cohort profile: Norwegian Epidemiologic Osteoporosis Studies (NOREPOS). Scand J Public Health 42:804–813
The Norwegian pharmaceutical product compendium (Felleskatalogen AS) (n.d.). https://www.felleskatalogen.no/medisin/. Accessed 31 Jan 2022
Black DM, Schwartz AV, Ensrud KE et al (2006) Effects of continuing or stopping alendronate after 5 years of treatment: the Fracture Intervention Trial Long-term Extension (FLEX): a randomized trial. JAMA 296:2927–2938
Statistics Norway (2003) Norwegian standard classification of education revised 2000. Statistics Norway, Oslo/Kongsvinger. https://www.ssb.no/a/english/publikasjoner/pdf/nos_c751_en/nos_c751_en.pdf. Accessed 10 Oct 2022
Solbakken SM, Magnus JH, Meyer HE et al (2019) Urban-rural differences in hip fracture mortality: a nationwide NOREPOS study. JBMR Plus 3:e10236
Lambert PC, Royston P (2009) Further development of flexible parametric models for survival analysis. Stand Genomic Sci 9:265–290
Johnell O, Kanis JA, Oden A et al (2005) Predictive value of BMD for hip and other fractures. J Bone Miner Res 20:1185–1194
Kanis JA, Johnell O, Oden A, Jonsson B, De Laet C, Dawson A (2000) Risk of hip fracture according to the World Health Organization criteria for osteopenia and osteoporosis. Bone 27:585–590
Pedersen AB, Heide-Jørgensen U, Sørensen HT, Prieto-Alhambra D, Ehrenstein V (2019) Comparison of risk of osteoporotic fracture in denosumab vs alendronate treatment within 3 years of initiation. JAMA Netw Open 2:e192416
Søgaard AJ, Holvik K, Meyer HE, Tell GS, Gjesdal CG, Emaus N, Grimnes G, Schei B, Forsmo S, Omsland TK (2016) Continued decline in hip fracture incidence in Norway: a NOREPOS study. Osteoporos Int 27:2217–2222
Harper KD, Weber TJ (1998) Secondary osteoporosis. Diagnostic considerations. Endocrinol Metab Clin North Am 27:325–348
Stein E, Shane E (2003) Secondary osteoporosis. Endocrinol Metab Clin North Am 32:115–134 (vii)
Hoff M, Skovlund E, Meyer HE, Langhammer A, Søgaard AJ, Syversen U, Holvik K, Abrahamsen B, Schei B (2021) Does treatment with bisphosphonates protect against fractures in real life? The HUNT study, Norway. Osteoporos Int 32:1395–1404
Kanis JA, Harvey NC, Johansson H, Liu E, Vandenput L, Lorentzon M, Leslie WD, McCloskey EV (2020) A decade of FRAX: how has it changed the management of osteoporosis? Aging Clin Exp Res 32:187–196
O’Kelly J, Bartsch R, Kossack N, Borchert J, Pignot M, Hadji P (2022) Real-world effectiveness of osteoporosis treatments in Germany. Arch Osteoporos 17:119
Landfeldt E, Ström O, Robbins S, Borgström F (2012) Adherence to treatment of primary osteoporosis and its association to fractures–the Swedish Adherence Register Analysis (SARA). Osteoporos Int 23:433–443
Black DM, Thompson DE, Bauer DC, Ensrud K, Musliner T, Hochberg MC, Nevitt MC, Suryawanshi S, Cummings SR (2000) Fracture risk reduction with alendronate in women with osteoporosis: the Fracture Intervention Trial. FIT Research Group. J Clin Endocrinol Metab 85:4118–4124
Cummings SR, Ferrari S, Eastell R et al (2018) Vertebral fractures after discontinuation of denosumab: a post hoc analysis of the randomized placebo-controlled FREEDOM trial and its extension. J Bone Miner Res 33:190–198
Everts-Graber J, Reichenbach S, Ziswiler HR, Studer U, Lehmann T (2020) A single infusion of zoledronate in postmenopausal women following denosumab discontinuation results in partial conservation of bone mass gains. J Bone Miner Res 35:1207–1215
Tutaworn T, Nieves JW, Wang Z, Levin JE, Yoo JE, Lane JM (2023) Bone loss after denosumab discontinuation is prevented by alendronate and zoledronic acid but not risedronate: a retrospective study. Osteoporos Int 34:573–584
Stone KL, Seeley DG, Lui LY, Cauley JA, Ensrud K, Browner WS, Nevitt MC, Cummings SR (2003) BMD at multiple sites and risk of fracture of multiple types: long-term results from the Study of Osteoporotic Fractures. J Bone Miner Res 18:1947–1954
Funding
Open access funding provided by University of Oslo (incl Oslo University Hospital)
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical approval
This study involves human participants and was approved by the Regional Committee for Medical and Health Research Ethics in Norway (REC South East A, reference number: 15538). The research is based on national health registries to which reporting is mandatory. The research project has obtained exemption from confidentiality from the Regional Committee for Medical and Health Research Ethics, on the basis of the Norwegian Act on medical and health research (the Health Research Act). The data were handled in accordance with the General Data Protection Regulation, and a Data Protection Impact Assessment has been conducted.
Conflicts of interests
None.
Disclaimer
Data from the Norwegian Patient Registry have been used in this publication. The interpretation and reporting of these data are the sole responsibility of the authors, and no endorsement by the Norwegian Directorate of Health is intended nor should be inferred.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Riska, B.S.L., Gunnes, N., Stigum, H. et al. Time-varying exposure to anti-osteoporosis drugs and risk of first-time hip fracture: a population wide study within the Norwegian Epidemiologic Osteoporosis Studies (NOREPOS). Osteoporos Int 34, 1369–1379 (2023). https://doi.org/10.1007/s00198-023-06752-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-023-06752-4