
Abstract
Purpose
Parastomal hernia is a complication with high morbidity that affects the patient’s quality of life. The aim of this study was to assess the cumulative incidence of parastomal hernia in patients who have undergone colorectal cancer surgery and to identify potential risk factors that could predispose to the development of this type of hernia in a large population-based cohort over a long follow-up period.
Methods
The Swedish Colorectal Cancer Registry and the National Patient Register were used to collect study cohort data between January 2007 and September 2013. All patients undergoing colorectal cancer surgery including a permanent stoma were included in the study group.
Results
A total of 39,984 patients were registered during the study period. Of these, 7649 received a permanent stoma. Multivariate proportional hazard analysis, based on 6329 patients for whom all covariates could be retrieved, showed that the only independent risk factor for developing a parastomal hernia was BMI ≥ 30 (HR 1.49; 95% CI 1.02–2.17; p < 0.037). A slightly elevated hazard ratio was found for preoperative radiotherapy (HR 1.36; 95% CI 0.96–1.91; p < 0.070). The cumulative incidence of patients diagnosed or surgically treated for parastomal hernia over a follow-up period of 5 years was 7.7% (95% CI 6.1–9.2%).
Conclusions
The cumulative incidence of parastomal hernia causing symptoms or requiring surgery after 5 years was at least 7.7%. Obesity increases the risk of developing parastomal hernia.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The creation of a stoma for temporary or permanent deviation of the bowel is a common procedure in colorectal surgery. When used as a temporary solution, the intent is to reverse the stoma and close the aperture in the abdominal wall. This is usually performed a minimum of 6 months after the index surgical procedure in order to let the tissue and anastomoses heal properly. Nevertheless, many of these patients never undergo the reversal procedure. A permanent stoma may be an integral part of the index surgical procedure itself, or an active strategy decided preoperatively in selected groups of patients (i.e., elderly or frail), or a measure determined by situations related to the cancer or comorbidity.
Living with a stoma implies coping with changes in body appearance and functional ability, which demands several lifestyle adjustments [1,2,3]. Unfortunately, stomal complications are not unusual and may add to an already strained situation for the patient. Complications range from minor such as skin irritation and leakage, dehydration from high output stomas, and cosmetically poor results with difficulties finding clothes that fit, to more serious problems such as prolapse, bowel obstruction, and parastomal hernia causing recurrent episodes of abdominal pain and the risk of bowel strangulation. All these factors lead to impaired quality of life.
A parastomal hernia is an incisional hernia defined as a herniation of abdominal contents through the trephine in the abdominal wall alongside the enterostomy [4, 5]. The risk for developing a parastomal hernia has been found to be high. Some, in fact, would describe this complication as a more or less inevitable long-term outcome. In previous studies, the cumulative incidence of parastomal hernia varies between 5 and 50% [4, 6,7,8]. The diversity of results in the literature is partly due to differences in defining parastomal hernia. Distinguishing criteria between stomal hernia and prolapse are also lacking. Some studies define parastomal hernia based solely on clinical signs such as bulging adjacent to the stoma or palpable defect in the abdominal wall, while others complement this with a radiological definition [9,10,11,12,13]. Cohort size and follow-up period also differ considerably. It is known from studies on ventral hernia that the rate of herniation increases with time, which is probably also true for parastomal hernia. All in all, this makes it difficult to compare and estimate the true rate of parastomal hernia from previously published studies. Whatever the criteria used, clinically the most important hernias are those that cause complications, symptoms, or problems to the patient that warrant surgical repair [9].
Among risk factors mentioned in the literature are those related to the surgical technique such as the diameter of the aperture in the abdominal wall and the location of the stoma, through the rectus abdominis muscle or lateral to it [4, 14]. There are also patient-related risk factors, including old age, chronic respiratory disorder, corticosteroid use, obesity, wound infection, and malnutrition [15,16,17,18].
In this study on a large population-based cohort of adult patients with permanent stoma and with long-term follow-up, our aim was to assess the cumulative incidence of parastomal hernia requiring surgical repair or causing symptoms in patients who have undergone colorectal cancer surgery, and to identify risk factors that could predispose to the development of this type of hernia.
Materials and methods
Study design
Data were retrieved from the Swedish Colorectal Cancer Registry (SCRCR), originally the Swedish Rectal Cancer Registry (SRCR) founded in 1995, and since 2007 including the Swedish Colon Cancer Registry (SCCR). It is compulsory for every healthcare provider in Sweden to report patients diagnosed with cancer to the Swedish Cancer Registry (SCR) [19]. Together with the SCR, the SCRCR approaches 100% coverage or all patients diagnosed with colorectal cancer in Sweden [20,21,22]. The other database used was the National Patient Register (NPR) [23] to which all Swedish healthcare providers report. Since 1987, this registry has included all in-patient care, and from the year 2001 even outpatient visits to both private and public healthcare provider except visits to primary healthcare physicians, and has been shown to have a high reliability [23, 24]. The SCRCR and the NPR were cross-matched using the patient’s Swedish personal identity number: a 10-digit number unique to each resident [25]. The personal identity number makes it possible to follow every individual over time.
Inclusion and exclusions criteria
In this study, all patients who underwent surgery for colorectal cancer in Sweden between January 1, 2007 and September 3, 2013 were identified in the SCRCR. From this cohort, procedures that included a permanent stoma were selected. Data on gender, age, BMI, tumor staging based on TNM-classification [26], preoperative radiochemotherapy, and index surgical procedures were also obtained from the SCRCR.
Information on development of parastomal hernia during the postoperative period, identified by International Classification of Diseases codes (ICD-10 codes K43, K45, or K46 or procedure codes JAR10-81), was obtained from the NPR until November 7, 2014, which was the limit of the follow-up period. These specific ICD codes enabled us to include all known parastomal hernias causing symptoms great enough for patients to bring it to the attention of their physician. Whereas minor asymptomatic hernias would not have been detected, the vast majority of stomal hernias found at clinical examination or diagnosed by radiological imaging, as well as hernias requiring surgical treatment were registered in the NPR during the period of the study.
The NPR also provided all diagnoses from admissions and visits prior to the index surgical procedure. These were scrutinized for relevant comorbidity including cardiovascular disease, connective tissue disorders, liver cirrhosis, kidney failure, diabetes, chronic obstructive lung disease, and chronic inflammatory conditions, i.e. conditions mentioned in the literature as possible risk factors for developing a hernia.
Statistical methods
Cox proportional hazard analysis was performed to identify the impact of each risk factor and to estimate the cumulative incidence of parastomal hernia. The analyses were performed with IBM SPSS Statistics for Windows, Version 22.0.
Results
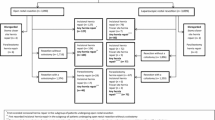
A total of 39,984 patients were registered in the SCRCR during the period 2007 until 2013. Of these, 7649 received a permanent stoma. Patients with data lacking on any variables in the multivariate analysis were excluded and the final study group consisted of 6,329 patients (Fig. 1). Baseline characteristics of the total cohort are shown in Table 1. There was a predominance of men receiving a permanent stoma at the index surgical procedure (4430 male patients (57.9%) compared to 3219 female patients (42.1%)). The mean age was 71.7 years. The follow-up time was equivalent to the registry period 2007–2013, with data from the NPR up to November 7, 2014. Altogether 3,276 patients (42,8% of the total cohort) died during the period of study. In Cox proportional hazard analysis, death was treated as a censored event.

Flow chart of cohort assembly
Some 65% of the patients had advanced stage tumors. Tumors infiltrating muscularis propria, i.e., T2, constituted almost 18% of the cohort. Categories T0-T1, corresponding to the least invasive tumors, accounted for 6.8% of the patients receiving a permanent stoma. In approximately 10% of the patients, the T-category was not known. Almost half of the patients had no spread to nearby lymph nodes and 72.5% had no distant spread.
Abdominoperineal resection (APR) was the most common surgical procedure in the cohort (43.9%). Anterior resection (AR) used for carcinoma situated in the upper or middle part of rectum where an oncologic safe distal margin could be achieved, leaving the rectal sphincter intact and allow for an anastomosis, was combined with a permanent stoma in 2.1% of the cases. Some 30.6% of the patients underwent resection of the sigmoid colon, in most cases registered as Hartmann’s procedure with a permanent stoma. Of the patients operated with resection of other parts of the colon (ascending, transverse, or descending colon), or when total colectomy was performed, 9.6% of cases had a permanent stoma. Of all surgical procedures resulting in a permanent stoma, 12.5% were performed as an emergency procedure.
In the statistical analyses, obesity (BMI ≥ 30) was found to be the only independent risk factor for developing a parastomal hernia. Multivariate Cox proportional hazard analysis showed a hazard ratio of 1.49, 95% CI 1.02–2.17, for BMI ≥ 30 (Table 2). None of the other potential risk factors, including TNM-categories, were statistically significant in predicting development of a stomal hernia. There was a slightly elevated hazard ratio of 1.36 (95% CI 0.96–1.91) for preoperative radiotherapy.
The cumulative incidence in this population-based cohort of patients diagnosed or surgically treated for parastomal hernia after a follow-up period of 5 years was 7.7%, 95% CI 6.1–9.2% (Fig. 2).

Cumulative incidence of parastomal hernia by BMI
Discussion
In the present study, the cumulative incidence of stomal hernia requiring surgery or causing symptoms was 7.7% over a 5-year follow-up period. Although this figure is lower than reported from previous studies using more sensitive methods and other criteria for determining the presence of stomal hernia [9, 27,28,29], the outcome in the present study focused on clinically relevant hernias.
Previous studies have shown obesity to be a risk factor for parastomal hernia [29, 30]. This should be considered when creating a stoma in obese patients. To some extent, the risk for future stomal hernia may be minimized by appropriate choice of stomal site, aperture diameter, and perhaps by reinforcing the stoma with mesh [31, 32].
As shown in Fig. 2, the incidence of stomal hernia requiring repair does not level off. This probably depicts the natural course, with pressure and distention of the tissues around the stoma. In the early period, tissues around the stoma usually retain their tensile strength. However, over time, the fascia becomes distended and loses its tensile strength resulting in distention of the tissues that progresses as time goes by [6].
The present study has some limitations. The primary endpoint was defined by the diagnoses and interventions registered in the NPR or SCRCR by the surgeons responsible for the patients. Although both registers are population-based and have national coverage, stomal hernias are only registered if the surgeon finds it relevant. This probably explains the relatively low incidence of stomal hernia seen in the present study. It is possible that there were some patients with a large stomal hernia causing problem who were not considered candidates for surgery due to comorbidity or because of anatomical conditions related to the hernia or previous abdominal surgery. Furthermore, no clear distinction between stomal hernia and stoma prolapse was made.
The SCRCR does not include data on measures taken to prevent the development of stomal hernia, and thus, we know nothing of what was done intraoperatively to reduce this risk. Type of stoma is not registered more specifically than stating whether it is intended for protective and temporary or permanent use, nor is there any information on the placement of the stoma site or the size of the aperture in the abdominal wall in the SCRCR. Also in this context, mesh reinforcement is of particular concern. Most of the procedures, however, were performed before mesh reinforcement became routine. Over the last decade, a large number of studies on mesh reinforcement have been published, with conflicting results [31,32,33,34,35,36]. In a Cochrane review based on 10 studies, the risk for stomal hernia was found to be halved if the stoma is reinforced with a mesh [37].
According to the European Hernia Society guidelines on stomal hernia prevention, the evidence regarding measures to prevent stomal hernias is insufficient [38]; thus, patient characteristics and specific preference should be taken into account when creating a stoma. Reinforcement with a mesh may be an option but should only be performed after assessing the specific circumstances in each case, including expected survival, the likelihood of stoma reversal, the risks associated with reoperation, and the risk of developing a stomal hernia. Whereas prevention of a stomal hernia may be high on the priority list of some patients, the side effects and risks associated with a permanent mesh may outweigh the potential benefit. Based on the results of the present study, obesity is one of the most important risk factors that must be considered when deciding on mesh reinforcement.
Conclusions
This population-based study showed that the cumulative incidence of clinically relevant parastomal hernia causing symptoms or requiring surgery after a follow-up period of 5 years was at least 7.7%. The only risk factor associated with stomal hernia was BMI ≥ 30. Our findings also suggest that the cumulative incidence increased with BMI over time, with higher risk for patients with a BMI greater than the median. In our opinion, this risk factor should be taken into consideration when deciding on measures to prevent stomal hernia, such as the use of mesh reinforcement.
References
Näsvall P, Dahlstrand U, Löwenmark T, Rutegård J, Gunnarsson U, Strigård K (2017) Quality of life in patients with a permanent stoma after rectal cancer surgery. Qual Life Res 26:55–64
van Dijk SM, Timmermans L, Deerenberg EB, Lamme B, Kleinrensink GJ, Jeekel J, Lange JF (2015) Parastomal hernia: impact on quality of life? World J Surg 39:2595–2601
Ripoche J, Basurko C, Fabbro-Perray P, Prudhomme M (2011) Parastomal hernia. A study of the French federation of ostomy patients. J Visc Surg 148:e435–e441
Israelsson LA (2008) Parastomal hernias. Surg Clin North Am 88:113–125
Śmietański M, Szczepkowski M, Alexandre JA, Berger D, Bury K, Conze J, Hansson B, Janes A, Miserez M, Mandala V, Montgomery A, Morales Conde S, Muysoms F (2014) European hernia society classification of parastomal hernias. Hernia 18:1–6
Londono-Schimmer EE, Leong AP, Phillips RK (1994) Life table analysis of stomal complications following colostomy. Dis Colon Rectum 37:916–920
North J (2014) Early intervention, parastomal hernia and quality of life: a research study. Br J Nurs 23(Suppl 5):S14–S18
Carne PWG, Robertson GM, Frizelle FA (2003) Parastomal hernia. Br J Surg 90:784–793
Jänes A, Weisby L, Israelsson LA (2011) Parastomal hernia: clinical and radiological definitions. Hernia 15:189–192
Gurmu A, Gunnarsson U, Strigård K (2011) Imaging of parastomal hernia using three-dimensional intrastomal ultrasonography. Br J Surg 98:1026–1029
Gurmu A, Matthiessen P, Nilsson S, Påhlman L, Rutegård J, Gunnarsson U (2011) The inter-observer reliability is very low at clinical examination of parastomal hernia. Int J Color Dis 26:89–95
Strigård K, Gurmu A, Näsvall P, Påhlman P, Gunnarsson U (2013) Intrastomal 3D ultrasound; an inter- and intra-observer evaluation. Int J Color Dis 28:43–47
Näsvall P, Wikner F, Gunnarsson U, Rutegård J, Strigård K (2014) A comparison between intrastomal 3D ultrasonography, CT scanning and findings at surgery in patients with stomal complaints. Int J Color Dis 29:1263–1266
Hardt J, Meerpohl JJ, Metzendorf MI, Kienle P, Post S, Herrle F (2013) Lateral pararectal versus transrectal stoma placement for prevention of parastomal herniation. Cochrane Database Syst Rev 22:CD009487
Parmar KL, Zammit M, Smith A, Kenyon D, Lees NP (2011) A prospective audit of early stoma complications in colorectal cancer treatment throughout the Greater Manchester and Cheshire colorectal cancer network. Color Dis 13:935–938
Ahn BK (2012) Risk factors for incisional hernia and parastomal hernia after colorectal surgery. J Korean Soc Coloproctol 28:280–281
Osborne W, North J, Williams J (2018) Using a risk assessment tool for parastomal hernia prevention. Br J Nurs 27:15–19
Hong SY, Oh SY, Lee JH, Kim DY, Suh KW (2013) Risk factors for parastomal hernia: based on radiological definition. J Korean Surg Soc 84:43–47
Barlow L, Westergren K, Holmberg L, Talbäck M (2009) The completeness of the Swedish Cancer Register, a sample survey for year 1998. Acta Oncol 48:27–33
Påhlman L, Bohe M, Cedermark B, Dahlberg M, Lindmark G, Sjödahl R, Ojerskog B, Damber L, Johansson R (2007) The Swedish rectal cancer registry. Br J Surg 94:1285–1292
Jörgren F, Johansson R, Damber L, Lindmark G (2013) Validity of the Swedish Rectal Cancer Registry for patients treated with major abdominal surgery between 1995 and 1997. Acta Oncol 52:1707–1714
Kodeda K, Nathanaelsson L, Jung B, Olsson H, Jestin P, Sjövall A, Glimelius B, Påhlman L, Syk I (2013) Population-based data from the Swedish Colon Cancer Registry. Br J Surg 100:1100–1107
Ludvigsson JF, Andersson E, Ekbom A, Feychting M, Kim JL, Reuterwall C, Heurgren M, Olausson PO (2011) External review and validation of the Swedish national inpatient register. BMC Public Health 11:450
Forsberg L, Rydh H, Jacobson A, Nygvist K, Heurgren M (2009) Kvalitet och innehåll i patientregistret. Discharge from inpatient treatment 1964–2007 and visits to specialist outpatient care (excluding primary care visits) 1997–2007 [quality and content of the patient register]. National Board of Health and Welfare, Stockholm
Ludvigsson JF, Otterblad-Olausson P, Pettersson BU, Ekbom A (2009) The Swedish personal identity number: possibilities and pitfalls in healthcare and medical research. Eur J Epidemiol 24:659–667
Sobin LH, Gospodarowicz MK, Wittekind C (2011) TNM classification of malignant tumours, 7th edn. John Wiley & Sons, New York
Andersen RM, Klausen TW, Danielsen AK, Vinther A, Gögenur I, Thomsen T (2018) Incidence and risk factors for parastomal bulging in patients with ileostomy or colostomy: a register-based study using data from the Danish stoma database capital region. Color Dis 20:331–340
Temple B, Farley T, Popik K, Ewanyshyn C, Beyer E, Dufault B (2016) Prevalence of parastomal hernia and factors associated with its development. J Wound Ostomy Continence Nurs 43:489–493
Sohn YJ, Moon SM, Shin US, Jee SH (2012) Incidence and risk factors of parastomal hernia. J Korean Soc Coloproctol 28:241–246
Funahashi K, Suzuki T, Nagashima Y, Matsuda S, Koike J, Shiokawa H, Ushigome M, Arai K, Kaneko T, Kurihara A, Kaneko H (2014) Risk factors for parastomal hernia in Japanese patients with permanent colostomy. Surg Today 44:1465–1469
Brandsma HT, Hansson BME, Aufenacker TJ, van Geldere D, van Lammeren FM, Mahabier C, Steenvoorde P, de Vries Reilingh TS, Wiezer RJ, de Wilt JHW, Bleichrodt RP, Rosman C (2016) Prophylactic mesh placement to prevent parastomal hernia, early results of a prospective multicenter randomized trial. Hernia 20:535–541
Odensten C1, Strigård K, Rutegård J, Dahlberg M, Ståhle U, Gunnarsson U, Näsvall P (2017) Use of prophylactic mesh when creating a colostomy does not prevent parastomal hernia: a randomized controlled trial-STOMAMESH. Ann Surg 269:427–431. https://doi.org/10.1097/SLA.0000000000002542
López-Cano M, Pereira JA, Armengol-Carrasco M, García-Alamino J (2018) To prevent parastomal hernia after Stomal surgery, a prophylactic mesh does work. Cir Esp 96:62–63
López-Cano M, Pereira Rodriguez JA (2018) Parastomal hernia prevention with mesh in the context of laparoscopic approach: an opinion based on current literature. Front Surg 5:19. https://doi.org/10.3389/fsurg.2018.00019
Cross AJ, Buchwald PL, Frizelle FA, Eglinton TW (2017) Meta-analysis of prophylactic mesh to prevent parastomal hernia. Br J Surg 104:179–186
Jänes A, Cengiz Y, Israelsson LA (2009) Preventing parastomal hernia with a prosthetic mesh: a 5-year follow-up of a randomized study. World J Surg 33:118–121
Jones HG, Rees M, Aboumarzouk OM, Brown J, Cragg J, Billings P, Carter B, Chandran P (2018) Prosthetic mesh placement for the prevention of parastomal herniation. Cochrane Database Syst Rev. https://doi.org/10.1002/14651858.CD008905
Antoniou SA, Agresta F, Garcia Alamino JM, Berger D, Berrevoet F, Brandsma HT, Bury K, Conze J, Cuccurullo D, Dietz UA, Fortelny RH, Frei-Lanter C, Hansson B, Helgstrand F, Hotouras A, Jänes A, Kroese LF, Lambrecht JR, Kyle-Leinhase I, López-Cano M, Maggiori L, Mandalà V, Miserez M, Montgomery A, Morales-Conde S, Prudhomme M, Rautio T, Smart N, Śmietański M, Szczepkowski M, Stabilini C, Muysoms FE (2018) European Hernia Society guidelines on prevention and treatment of parastomal hernias. Hernia 22:183–198
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Financial disclosures
No funding was provided for this work.
Ethical approval
The study received approval from the Regional ethics review board in Stockholm, ref. number 2014/1351-31/5.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Tivenius, M., Näsvall, P. & Sandblom, G. Parastomal hernias causing symptoms or requiring surgical repair after colorectal cancer surgery—a national population-based cohort study. Int J Colorectal Dis 34, 1267–1272 (2019). https://doi.org/10.1007/s00384-019-03292-4
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00384-019-03292-4