
Abstract
Purpose
To assess the association between nut and seed consumption, both combined and separately, and metabolic syndrome and its components, including fasting glucose, triglycerides, high-density lipoprotein (HDL) cholesterol, central obesity, and blood pressure.
Methods
This cross-sectional analysis used data from 22,687 adults (aged ≥ 18 years) involved in seven cycles (2005–2018) of the National Health and Nutrition Examination Survey (NHANES). Habitual nut and seed intakes were estimated by the Multiple Source Method using data from two 24-h dietary recalls. Metabolic syndrome was ascertained using biochemical data and self-reported medication use. Sex-specific effect estimates were obtained using logistic and linear regressions adjusting for lifestyle and socioeconomic confounders.
Results
Compared to non-consumers, female, but not male, habitual consumers of either nuts or seeds had lower odds of having metabolic syndrome (OR: 0.83, 95% CI 0.71, 0.97). Both nut intake alone and seed intake alone were inversely associated with high fasting glucose and low HDL-cholesterol in females compared to non-consumers. When restricted to habitual consumers only, the combined intake of nuts and seeds at 6 g/day was associated with the lowest triglycerides and highest HDL-cholesterol in females. Combined consumption of nuts and seeds up to one ounce-equivalent (15 g) per day, but not in higher intake levels, was inversely associated with metabolic syndrome, high fasting glucose, central obesity, and low HDL-cholesterol in females.
Conclusions
Nut and seed consumption, both separately or combined, below 15 g/day was inversely associated with metabolic syndrome and its component conditions in females but not males.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Metabolic syndrome is a condition that involves the co-occurrence of multiple metabolic abnormalities, including high fasting glucose, dyslipidemia, high blood pressure, and/or central obesity [1]. It is estimated that 20 to 30% of the global population has metabolic syndrome [2,3,4,5] and individuals with this condition have a higher risk of developing type 2 diabetes [6], cardiovascular diseases [7], and a higher mortality rate [8]. Although dietary-based interventions are considered an important strategy for the management of metabolic syndrome [9], many questions remain as to which modifiable dietary factors may play a role to reduce the risk of or manage metabolic syndrome.
Nuts and seeds are considered an important component of a healthy diet in dietary guidelines in several countries [10,11,12] and this is attributed to their plant-based origin while being a source of high quality protein, as well as containing high amounts of mono- and poly-unsaturated fats, dietary fiber, micronutrients, and phytochemicals with antioxidative properties [13]. Habitual nut consumption has been associated with improved weight management [14] and a lower risk of cardiovascular and all-cause mortality [15, 16], but the association with the risk of metabolic syndrome has been inconsistent [17, 18]. Furthermore, few studies have investigated the health benefits of seeds alone even though they have comparable nutrient profiles to nuts and belong to the same food group within dietary guidelines. Due to the similarities in nutritional profiles, nuts and seeds are hypothesized to provide similar health benefits [19]. However, current evidence surrounding the metabolic health benefits of seeds alone is limited to randomized controlled trials [20,21,22,23]. For instance, flaxseed intake decreased blood pressure and sesame seeds intake lowered fasting blood glucose [20, 23]. However, results regarding the effect of flaxseed intake on fasting blood glucose were inconsistent [21], and no significant changes in metabolic syndrome markers were observed with chia seeds consumption [22]. Nonetheless, high heterogeneity in the characteristics of participants and the results was noted in all systematic reviews [20,21,22,23], thus the quality of evidence was generally considered low or very low based on the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) approach. More importantly, the association between the intake of seeds, either alone or together with nuts as a food group, and metabolic syndrome has not been assessed before. Therefore, the aim of this study was two-fold: (1) to assess the difference in the odds of metabolic syndrome and its related components [high fasting glucose, high triglycerides, central obesity, high blood pressure, and low high-density lipoprotein cholesterol (HDL-cholesterol)] between consumers and non-consumers of nuts and/or seeds, and (2) to examine the presence of a dose–response association between nut and/or seed consumption and metabolic syndrome.
Methods
Study population
This study used data collected from males and females aged 18 years and over that participated in the National Health and Nutrition Examination Survey (NHANES), which used a multistage probability sampling procedure to obtain nationally representative estimates of the health and nutritional status of noninstitutionalized residents in the United States [24]. In each survey, participants provided information regarding demographics, socioeconomic status, diet, and health in an interview, underwent medical and physiological examinations, and provided fasted blood samples in which various biomarkers were measured. In this analysis, we included participants aged 18 years or older from seven cycles (2005–2006, 2007–2008, 2009–2010, 2011–2012, 2013–2014, 2015–2016, 2017–2018). The survey protocols for NHANES 2005–2018 (Protocol #2005–06, Protocol #2011–17, and Protocol #2018–01) were approved by the National Centre for Health Statistics (NCHS) Research Ethics Review Board, and all participants provided their informed consent. Further inclusion criteria were that participants had to have completed two reliable 24-h recalls, and have complete data on relevant covariates (age, sex, ethnicity, ratio of family income to poverty, smoking status, alcohol intake, Healthy Eating Index 2015 (HEI 2015), physical activity z-score, and prior cardiovascular event).
Nut and seed intake
Nut and seed intake data were obtained using two 24-h dietary recalls that were carried out on non-consecutive days using the Automated Multiple Pass Method (AMPM), the details of which were previously published [25]. In this analysis, nuts and seeds included the following: (1) nuts: almonds, almond butter, Brazil nuts, cashews, cashew butter, hazelnuts, macadamias, pecans, pine nuts, pistachios, walnuts, peanuts, and peanut butter, and (2) seeds: pumpkin seeds, flaxseeds, sesame seeds, sesame butter, sunflower seeds, psyllium seeds, and chia seeds [26]. In addition to those eaten alone, nuts and seeds that were a component of a meal or an ingredient of food products were also included by searching the Food Commodity Intake Database (FCID), containing recipes for composite food products [27]. Only 24-h recalls that were reliable and met the minimum criteria established by NHANES were used in this study [24]. The usual nut and seed intake were then estimated using the Multiple Source Method (MSM) [28], which is a statistical method for estimating usual dietary intake for episodically consumed foods in individuals and was validated in a large epidemiological study [29]. We included age, sex, product of age and sex, and days of recall (weekday/weekend) as covariates when estimating usual nut and seed intake in this study. Furthermore, we categorized the combined intake of nuts and seeds using cut-offs informed by our previous study: non-consumers (0 g/day), 0.1–15.0 g/day, 15.1–29.9 g/day, and 30.0 g/day or above [26]. Based on the U.S dietary guidelines 2020 [10], an ounce-equivalent of nuts and seeds is defined as ½ oz, which translates to approximately 15 g, hence further justifying the application for the intake group cut-offs used in this study. The intake cut-off at 15 g per day also aligned with the results from a global study where daily nut and seed intake below the optimal range (16–25 g/day) was associated with higher all-cause mortality [30].
Metabolic syndrome and the component conditions
Metabolic syndrome was ascertained using the criteria published by Alberti et al. [1]. This set of criteria was chosen because it is the most updated criteria for defining metabolic syndrome. Participants meeting the criteria for any three of the following conditions were defined as having metabolic syndrome: high fasting plasma glucose (FPG) (≥ 100 mg/dL or using insulin or taking medication for hyperglycemia), high triglycerides (≥ 150 mg/dL or taking medication for dyslipidemia), central obesity (waist circumference ≥ 102 cm in men and ≥ 88 cm in women), high blood pressure (systolic pressure ≥ 130 mmHg, diastolic pressure ≥ 85 mmHg, or taking medication for high blood pressure), and low HDL-cholesterol (< 40 mg/dL in men or < 50 mg/dL for women, or taking medication for dyslipidemia). Fasting blood samples were collected from participants and analyzed using methods detailed elsewhere [31], while medication use was self-reported by the participants. The data for FPG and triglycerides were adjusted using regression equations provided in the NHANES data documentation of the 2015–2016 and 2017–2018 cycles to account for variations in the analysis method [24].
Demographic factors and covariates
Covariates considered in this analysis included age, sex, ethnicity (Mexican American, Other Hispanic, Non-Hispanic White, Non-Hispanic Black, and other races), family income to poverty ratio, smoking status, HEI 2015, physical activity, alcohol intake, and history of a cardiovascular event. The family income to poverty ratio was used to depict socioeconomic status and was calculated by dividing family or individual income by the poverty guidelines specific to each survey cycle and varying by family size and geographic location [24]. Smoking status was self-reported and categorized into non-smoker, former smoker, and current smoker. The HEI 2015 was used to assess adherence to the 2015–2020 Dietary Guidelines for Americans. With a range from 0 to 100, a higher score depicts a higher adherence and thus a better diet quality [32]. Physical activity was reported as a z-score based on self-reported frequency and duration of leisure-time physical activity, which were collected from participants using different questionnaires across the seven cycles of NHANES as reported in previous studies [33, 34]. The calculation of the z-score is described elsewhere [26]. Daily alcohol intake was calculated by averaging alcohol intake from the two 24-h recalls. History of a cardiovascular event, which included congestive heart failure, angina/angina pectoris, heart attack, and/or stroke, was self-reported by participants.
Statistical analyses
This analysis utilized sampling strata, clusters, and weights in line with the NHANES analytical guidelines ensuring the results could be generalized to the US population [24]. Two-year sample weights for each NHANES cycle were combined to provide 14-year weights for the 2005–2018 survey period. The two-day dietary recall weights were used for all outcomes.
We tested for age and sex interactions in the association between the combined intake of nuts and seeds and metabolic syndrome using a multivariate model adjusted for ethnicity, family income to poverty ratio, daily alcohol intake, smoking status, HEI 2015, physical activity, and history of a cardiovascular event. While we did not find evidence of age interaction (p = 0.39), the sex interaction was statistically significant (p = 0.005), thus all subsequent analyses were conducted separately for males and females. Since approximately 50% of participants reported zero consumption of nuts and seeds, we adopted a two-part modeling approach to assess the association between nut and/or seed intake (intake of nuts alone, seeds alone, and the combined intake of nuts and seeds) and metabolic syndrome, its components, and the measurements used to define metabolic syndrome. First, we assess if consuming any amount of nuts and/or seeds was associated with differences in outcomes compared with not consuming any. Second, we investigate if the outcomes changed with the amount of nut and/or seed consumed among consumers.
For the first part of the approach, we modeled the associations using nut and/or seed intake as binary exposure variables (0 g/day vs > 0 g/day), with non-consumers being the reference group. Logistic regression analyses (odds ratios with 95% CI) were used for binary outcomes (metabolic syndrome, high fasting glucose, high triglycerides, central obesity, high blood pressure, and low HDL-cholesterol) and covariates included age, family income to poverty ratio, ethnicity (Mexican American, Non-Hispanic White, Non-Hispanic Black, Other Hispanic, and other races), smoking status (non-smoker, former smoker, current smoker), daily alcohol intake, HEI 2015, experienced a cardiovascular event (yes/no), and physical activity z-scores. Linear regression analyses (beta coefficients with 95% CI) were used for continuous outcomes (FPG, triglycerides, waist circumference, systolic blood pressure, and HDL-cholesterol) with the same covariates as used in logistic regression, but with the addition of medications used for managing levels of corresponding biomarkers (e.g. use of insulin and medication for hyperglycemia was adjusted for when the outcome was fasting glucose). When we modeled the associations for nut or seed intake alone, both variables were included in the same model to account for intakes of one another.
For the second part of the approach, continuous outcomes and binary outcomes were analyzed differently. For continuous outcomes, linear regression models were used to assess the linear associations between nut and/or seed intake and all continuous outcomes among consumers only, including the same set of covariates as those in the first part. Results were presented as estimated changes in unit of measurement per one-gram additional consumption of nuts and seeds. We further investigated the presence of non-linear associations between nut and/or seed intake (among consumers only) and the continuous outcomes using linear regression models with restricted cubic splines for the exposure variables, with five knots placed at the 5th, 27.5th, 50th, 72.5th, and 95th percentiles, adjusting for the same set of covariates as in the linear association models. Model fit of linear and non-linear models of each exposure and outcome pair were then compared using likelihood-ratio tests. Whenever a non-linear model showed a better fit over the linear model (likelihood-ratio test p < 0.05), the non-linear associations were also reported. For binary variables, logistic regression models were used to assess the associations between categories of combined intake of nuts and seeds (0 g/day, 0.1–15.0 g/day, 15.1–29.9 g/day, 30.0 g/day or above) and all binary outcomes with 0 g/day as the reference group and the same set of covariates used in the first part. The presence of linear trends across categories of combined intake of nuts and seeds was assessed using logistic regressions with the median value of each category as the independent variable and the same set of covariates was included.
All analyses were performed in R (version 4.1.1) [35] using packages “survey” [36] and “rms” [37] while nonlinear plots were produced using the “effects” package [38]. Statistical significance was set at two-sided p < 0.05.
Results
Participant characteristics
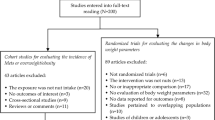
A total of 22,687 participants were included in the main analysis. The inclusion flowchart is shown in Fig. 1 and the demographic characteristics are shown in Table 1. The proportion of participants who were habitual consumers of either nuts or seeds was greater in females than in males, while male consumers had a higher median intake of nuts and seeds combined than female consumers. Similar results were observed when considering nut intake alone. Around 20% females and 17% males reported to be habitual seed consumers and the median daily intake among consumers was 4 g/day in both sexes. Females were more likely to be non-smokers while males were more likely to be former smokers. Females also consumed less alcohol, had a better diet based on the HEI 2015, had lower physical activity levels, and were less likely to have a history of a cardiovascular event when compared to males. The prevalence of metabolic syndrome was approximately 50% and was similar between sexes. Males were more likely to have high fasting glucose and high triglycerides while females were more likely to have central obesity.

Participant exclusion flowchart for all outcomes. HDL, high-density-lipoprotein. NHANES, National Health and Nutrition Examination Survey. *Numbers of individual variables do not add up as participants could have missing data in more than one variable
Associations with metabolic syndrome and its components between consumers vs. non-consumers of nuts and/or seeds
To investigate if any amount of nut and/or seed consumption was associated with metabolic syndrome and its components compared to not consuming any, we assessed the associations between consumers and non-consumers of nuts and/or seeds and all outcomes and the results are shown in Table 2. In females, after adjusting for all covariates, habitual consumption of either nuts or seeds, as well as nuts alone, were both associated with lower odds of metabolic syndrome, high fasting glucose, central obesity, and low HDL-cholesterol. Seed intake alone in females was also associated with lower odds of high fasting glucose and low HDL-cholesterol. In males, no statistically significant associations were found, except that nut consumers had lower odds of high fasting glucose compared to non-consumers.
Regarding clinical measurements used to define metabolic syndrome, habitual consumption of either nuts or seeds was inversely associated with waist circumference in females and positively associated with HDL-cholesterol in males compared to non-consumers. Habitual nut consumption alone was inversely associated with waist circumference in females and higher HDL-cholesterol in both sexes. No statistically significant associations were observed between habitual seed intake and any of the clinical measurements in both sexes.
Associations with measurements used to define metabolic syndrome among nut and/or seed consumers only
To explore if the measurements used to define metabolic syndrome changed with the amount of nut and/or seed consumed, we modeled the association between habitual nut and/or seed consumption with FPG, triglycerides, waist circumference, systolic blood pressure, and HDL-cholesterol among consumers only and the results are shown in Table 3. Per-gram increase in the combined intake of nuts and seeds among consumers was positively associated with waist circumference in females but not males and no statistically significant associations were observed for other outcomes. Per-gram increase in nut intake alone was positively associated with waist circumference in both males and females; whereas a per-gram increase in seed intake alone was positively associated with triglycerides and waist circumference in females, and negatively associated with systolic blood pressure in males.
We observed evidence of non-linear associations for the following exposure and outcome pairs (pnon-linear < 0.05, Table 3): combined intake of nuts and seeds and triglycerides in females (p = 0.049), combined intake of nuts and seeds and systolic blood pressure in males (p = 0.028), nut intake alone and systolic blood pressure in males (p = 0.048), and combined intake of nuts and seeds and HDL-cholesterol in females (p = 0.019). The plot of the estimated non-linear association indicated that triglycerides decreased with combined nut and seed intake in females (Supplemental Figure 1 ), reaching the lowest point at approximately 6 g/day. Triglycerides then increased and plateaued at intake beyond 25 g/day, although the levels remained lower than the near-zero intake level. Systolic blood pressure in males increased with combined intake of nuts and seeds until 10 g/day (Supplemental Figure 2), followed by a decrease until 30 g/day and tended to go up at higher intake. This trend was also observed with nut intake alone in males (Supplemental Figure 3), although the range of fluctuation in systolic blood pressure was within 4 mmHg for both associations. Estimated HDL-cholesterol increased with combined nut and seed intake in females (Supplemental Figure 4), peaking at 6 g/day, then slightly decreased and finally plateauing at intake beyond 12 g/day at a level higher than near-zero intake levels.
Association between categories of nut and seed intake and metabolic syndrome and its components
To investigate if the odds of metabolic syndrome and its components change with the amount of nuts and seeds consumed, we modeled the associations between pre-specified categories of combined intake of nuts and seeds and metabolic syndrome and its components. After adjusting for all covariates, female participants consuming 0.1–15.0 g nuts and seeds per day had lower odds of having metabolic syndrome, high FPG, central obesity, and low HDL cholesterol than non-consumers. At the same level of intake, males had higher odds of having high triglycerides (Table 4). No statistically significant association was observed in all higher intake categories and both sexes, except for lower odds of high blood glucose in females at the 15.1–29.9 g/day category, and higher odds of high blood pressure in males at the 30 g/day and above category. No significant linear trend across intake categories of nuts and seeds was observed for any outcomes.
Discussion
In this nationally representative sample of US adults, we found that nut and seed consumers had lower odds of having metabolic syndrome and some of its components (e.g. high fasting glucose, central obesity, low HDL cholesterol) than non-consumers, but these associations were seen only in females. Congruent results were observed when nut and seed intake were considered separately, although the associations were less consistent in seed intake alone. Our analyses further demonstrated that the lower odds of metabolic syndrome and its components in females were the most pronounced at the nut and seed intake level of 0.1–15.0 g/day when compared with non-consumers (Table 4). Our study also showed for the first time in an epidemiological analysis that consumption of seeds was associated with a better metabolic profile in females i.e. a lower likelihood of having high fasting glucose and low HDL-cholesterol.
The finding that habitual nut consumption in females being inversely associated with metabolic syndrome compared to non-consumers is consistent with a cohort study involving Spanish university graduates, which observed that consuming two serves of nuts per week at baseline was inversely associated with the prevalence of metabolic syndrome after six years in females but not males [39]. This sex-specific relationship between nut consumption and metabolic benefits has also been observed in previous analyses using data from European and South Korean populations of a similar age or older [40, 41]. In support of our findings, one study that analyzed data from adult NHANES participants observed significant trends of reduction in fasting glucose and waist circumference, as well as increasing HDL-cholesterol, with the combined intake of nuts and seeds in females but not males [26]. This study also found that nut and seed consumption at all levels were inversely associated with the risk of having non-alcoholic fatty liver disease (NAFLD) in females, while this association was only observed in males with moderate nut and seed intake (15.1–30.0 g/day) [26]. This difference in NAFLD risk between male and female could possibly explain our observations in this study as NAFLD was known to be a cause of metabolic syndrome [42]. Another possible explanation is a variation in the time of nut and seed ingestion during the day, as it was previously shown that the preference in number and timing of meals, which have profound influence on metabolic health [43], could be different between sexes [44]. Similarly, a recent meta-analysis of randomized controlled trials found that the timing of nut intake during the day could affect energy expenditure in human subjects [45]. Nonetheless, we acknowledge that a mechanistic explanation is yet to be offered and this difference in the association between sexes should be verified in future randomized controlled studies and longitudinal studies.
The effect estimates for nut intake alone observed in this study were similar in direction and magnitude to those of combined intake of nuts and seeds, while the findings related to seed intake were less pronounced. This suggests that nut intake was the main contributor to the findings associated with the combined intake of nuts and seeds observed in this study, which is expected given the higher consumption of nuts compared to seeds among the included participants. Despite the weaker associations observed with seed intake, we were able to observe consistencies in results between consumption of nuts alone and seeds alone, especially the inverse associations with high fasting glucose and low HDL-cholesterol. Together with the fact that nuts and seeds had comparable nutrient content [19], our results provide support, from an epidemiological perspective, to encourage intake of these two food types for better metabolic health, supporting their combination in the same food group in the dietary guidelines. The similarities in nutrient content between nuts and seeds also imply that they can be used complimentarily or as a substitution (in the case of nut allergy) in the habitual diet. The call for consuming both nuts and seeds for optimal metabolic health is further supported by evidence that dietary patterns involving higher amount of both nuts and seeds, such as the Mediterranean diet and the plant-based Dietary Portfolio [46], were associated with lower incidence of type 2 diabetes and cardiovascular diseases [47, 48]. Interestingly, nut and seed intake was associated with improvement in overall diet quality in a previous study [49] and while this is not captured by our study design, it remains to be another possible mechanism contributing to metabolic benefits. Nonetheless, it is important to note that the clinical markers between habitual seed consumers and non-consumers were not significantly different (Table 2), which could be due to the small amount of seeds consumed (mean intake: 4 g/day) among included participants, as opposed to the high doses used in previous RCTs (usually ≥ 20 g/day). Therefore, the associations of habitual seed intake at this level with metabolic health should be further assessed in future longitudinal studies and randomized controlled trials.
Although our results supported a more favorable metabolic profile in habitual nut and seed consumers compared to non-consumers, these associations did not appear to be dose-dependent. The non-linear associations between combined intake of nuts and seeds and triglycerides and HDL cholesterol in females showed that optimum benefits were achieved at an intake of approximately 6 g/day (Table 3), while the combined intake of nuts and seeds above 15 g/day had no association with metabolic syndrome (Table 4). This was in line with the results from a meta-analysis of prospective cohort studies, which found that changes in the incidence of central obesity plateaued after nut intake exceeded 5 g/day [14], while a recently published cohort study involving Iranian adults also observed an inverse association with metabolic syndrome incidence in the second quantile of nut consumption but not in higher quantiles [50]. These findings suggested that the benefits of nut and/or seed intake on metabolic syndrome could be achieved at low levels (i.e. ≤ 15 g/day). Our findings align with the recommendation of having an ounce-equivalent (i.e. 15 g) of nuts and seeds on most days of a week [10], although the current recommendation was developed based on results of food pattern modeling [51] to ensure adequate nutrient intakes across different life stages. On the other hand, the possibility that inadequate data points at higher nut and seed intake precluding associations to be detected could not be excluded. Studies conducted using data from populations with higher nut and seed intake, such as those following the Mediterranean diet, may be able to address this limitation.
The strengths of this study include the use of a large nationally representative sample and dietary data collected using a validated method [52]. Furthermore, we estimated the habitual intake of nuts and seeds, which is an episodically consumed food group, using the MSM to account for intra-individual variation. In addition, we considered nuts and seeds in different forms, including in the whole form, as an ingredient, and in butter form, to obtain a more precise estimate of nut and seed intake. As per the guidance of the American Nutrition Society, we provided effect estimates together with 95% CI for all results [53]. On the other hand, several limitations should be considered when interpreting the findings. First, the results might be affected by reverse causation and residual confounding due to the cross-sectional nature of this study. Second, with metabolic syndrome being the primary outcome of this study, multiple secondary outcomes were analyzed and the p-values in this study should be interpreted carefully. Third, the intake of seeds was very low among the included participants, thereby limiting the ability of this analysis in detecting significant associations. Finally, caution must be exercised when attempting to generalize the results of this study to other populations.
Conclusion
Intake of nuts and seeds, both combined and separately, was inversely associated with metabolic syndrome and its component conditions in females, with the associations being the most pronounced at 0.1–15.0 g/day and higher intake was not associated with lower odds. Nut consumption seemed to be the main driver of these relationships, with seed consumption showing consistent associations. Future studies should investigate the longitudinal relationships between habitual nut and/or seed intake with metabolic health outcomes, as well as reasons for the sex-dependent associations found in this study.
Data availability
The data that support the findings of this study is available from the corresponding author upon reasonable request.
References
Alberti KGMM, Eckel Robert H, Grundy Scott M, Zimmet Paul Z, Cleeman James I, Donato Karen A, Fruchart J-C, James WPT, Loria Catherine M, Smith Sidney C (2009) Harmonizing the metabolic syndrome. Circulation 120(16):1640–1645. https://doi.org/10.1161/CIRCULATIONAHA.109.192644
Hirode G, Wong RJ (2020) Trends in the Prevalence of Metabolic Syndrome in the United States, 2011–2016. JAMA 323(24):2526–2528. https://doi.org/10.1001/jama.2020.4501
Tanamas SK, Magliano DJ, Lynch B, Sethi P, Willenberg L, Polkinghorne KR, Chadban S, Dunstan D, Shaw JE (2013). AusDiab 2012. The Australian Diabetes, Obesity and Lifestyle Study. Baker IDI Heart and Diabetes Institute, Melbourne. Available at https://www.baker.edu.au/-/media/documents/impact/ausdiab/reports/ausdiabreport-2012.pdf?la=en
Scuteri A, Laurent S, Cucca F, Cockcroft J, Cunha PG, Mañas LR, Raso FUM, Muiesan ML, Ryliškytė L, Rietzschel E, Strait J, Vlachopoulos C, Völzke H, Lakatta EG, Nilsson PM, for the Metabolic S, Arteries Research C (2015) Metabolic syndrome across Europe: different clusters of risk factors. Eur J Prevent Cardiol 22(4):486–491. https://doi.org/10.1177/2047487314525529
Liu B, Chen G, Zhao R, Huang D, Tao L (2021) Temporal trends in the prevalence of metabolic syndrome among middle-aged and elderly adults from 2011 to 2015 in China: the China health and retirement longitudinal study (CHARLS). BMC Public Health 21(1):1045. https://doi.org/10.1186/s12889-021-11042-x
DeBoer MD, Filipp SL, Gurka MJ (2018) Use of a metabolic syndrome severity <em>Z</em> score to track risk during treatment of prediabetes: an analysis of the diabetes prevention program. Diabetes Care 41(11):2421. https://doi.org/10.2337/dc18-1079
Mottillo S, Filion KB, Genest J, Joseph L, Pilote L, Poirier P, Rinfret S, Schiffrin EL, Eisenberg MJ (2010) The metabolic syndrome and cardiovascular risk: a systematic review and meta-analysis. J Am Coll Cardiol 56(14):1113–1132. https://doi.org/10.1016/j.jacc.2010.05.034
Shi TH, Wang B, Natarajan S (2020) The influence of metabolic syndrome in predicting mortality risk among US Adults: importance of metabolic syndrome even in adults with normal weight. Prev Chronic Dis 2020(17):17
Castro-Barquero S, Ruiz-León AM, Sierra-Pérez M, Estruch R, Casas R (2020) Dietary strategies for metabolic syndrome: a comprehensive review. Nutrients. https://doi.org/10.3390/nu12102983
U.S. Department of Agriculture and U.S. Department of Health and Human Services (2020) Dietary Guidelines for Americans, 2020–2025, 9th Edition. Available at https://DietaryGuidelines.gov
National Health and Medical Research Council (2013) Australian Dietary Guidelines. National Health and Medical Research Council. https://www.health.gov.au/sites/default/files/australian-dietary-guidelines.pdf.
Public Health England (2016) The Eatwell Guide. Helping you eat a healthy, balanced diet. Public Health England. https://www.gov.uk/government/publications/the-eatwell-guide.
Alasalvar C, Bolling BW (2015) Review of nut phytochemicals, fat-soluble bioactives, antioxidant components and health effects. Br J Nutr 113(S2):S68–S78. https://doi.org/10.1017/S0007114514003729
Nishi SK, Viguiliouk E, Blanco Mejia S, Kendall CWC, Bazinet RP, Hanley AJ, Comelli EM, Salas Salvadó J, Jenkins DJA, Sievenpiper JL (2021) Are fatty nuts a weighty concern? A systematic review and meta-analysis and dose–response meta-regression of prospective cohorts and randomized controlled trials. Obesity Rev. https://doi.org/10.1111/obr.13330
Coates AM, Hill AM, Tan SY (2018) Nuts and cardiovascular disease prevention. Curr Atheroscler Rep 20(10):48. https://doi.org/10.1007/s11883-018-0749-3
de Souza RJ, Dehghan M, Mente A, Bangdiwala SI, Ahmed SH, Alhabib KF, Altuntas Y, Basiak-Rasała A, Dagenais G-R, Diaz R, Amma LI, Kelishadi R, Khatib R, Lear SA, Lopez-Jaramillo P, Mohan V, Poirier P, Rangarajan S, Rosengren A, Ismail R, Swaminathan S, Wentzel-Viljoen E, Yeates K, Yusuf R, Teo KK, Anand SS, Yusuf S, investigators Ps (2020) Association of nut intake with risk factors, cardiovascular disease, and mortality in 16 countries from 5 continents: analysis from the Prospective Urban and Rural Epidemiology (PURE) study. Am J Clin Nutr 112(1):208–219. https://doi.org/10.1093/ajcn/nqaa108
O’Neil CE, Fulgoni VL, Nicklas TA (2015) Tree Nut consumption is associated with better adiposity measures and cardiovascular and metabolic syndrome health risk factors in US adults: NHANES 2005–2010. Nutr J. https://doi.org/10.1186/s12937-015-0052-x
Ibarrola-Jurado N, Bulló M, Guasch-Ferré M, Ros E, Martínez-González MA, Corella D, Fiol M, Wärnberg J, Estruch R, Román P, Arós F, Vinyoles E, Serra-Majem L, Pintó X, Covas M-I, Basora J, Salas-Salvadó J (2013) Cross-sectional assessment of nut consumption and obesity. The PREDIMED Study. PLOS ONE, Metabolic syndrome and other cardiometabolic risk factors. https://doi.org/10.1371/journal.pone.0057367
George ES, Daly RM, Tey SL, Brown R, Wong THT, Tan S-Y (2022) Perspective: is it time to expand research on “nuts” to include “seeds”? Advances in nutrition, Justifications and key considerations. https://doi.org/10.1093/advances/nmac028
Sohouli MH, Haghshenas N, Hernández-Ruiz Á, Shidfar F (2022) Consumption of sesame seeds and sesame products has favorable effects on blood glucose levels but not on insulin resistance: a systematic review and meta-analysis of controlled clinical trials. Phytother Res. https://doi.org/10.1002/ptr.7379
Ntzouvani A, Antonopoulou S, Nomikos T (2019) Effects of nut and seed consumption on markers of glucose metabolism in adults with prediabetes: a systematic review of randomised controlled trials. Br J Nutr 122(4):361–375. https://doi.org/10.1017/S0007114519001338
Teoh SL, Lai NM, Vanichkulpitak P, Vuksan V, Ho H, Chaiyakunapruk N (2018) Clinical evidence on dietary supplementation with chia seed (Salvia hispanica L.): a systematic review and meta-analysis. Nutr Rev 76(4):219–242. https://doi.org/10.1093/nutrit/nux071
Ursoniu S, Sahebkar A, Andrica F, Serban C, Banach M (2016) Effects of flaxseed supplements on blood pressure: A systematic review and meta-analysis of controlled clinical trial. Clin Nutr 35(3):615–625. https://doi.org/10.1016/j.clnu.2015.05.012
Centers for Disease Control and Prevention (CDC), National Center for Health Statistics (NCHS) (2021) National Health and Nutrition Examination Survey Data. Department of Health and Human Services, Centers for Disease Control and prevention. https://www.cdc.gov/nchs/nhanes/index.htm.
Raper N, Perloff B, Ingwersen L, Steinfeldt L, Anand J (2004) An overview of USDA’s dietary intake data system. J Food Compos Anal 17(3):545–555. https://doi.org/10.1016/j.jfca.2004.02.013
Cardoso BR, Tan S-Y, Daly RM, Via JD, Georgousopoulou EN, George ES (2021) Intake of nuts and seeds is associated with a lower prevalence of nonalcoholic fatty liver disease in US adults: findings from 2005–2018 NHANES. J Nutr 151(11):3507–3515. https://doi.org/10.1093/jn/nxab253
U.S. Environmental Protection Agency Food Commodity Intake Database. What We Eat in America. https://fcid.foodrisk.org/.
Harttig U, Haubrock J, Knüppel S, Boeing H, on behalf of the EC (2011) The MSM program: web-based statistics package for estimating usual dietary intake using the multiple source method. Eur J Clin Nutr 65(1):S87–S91. https://doi.org/10.1038/ejcn.2011.92
Haubrock J, Nöthlings U, Volatier J-L, Dekkers A, Ocké M, Harttig U, Illner A-K, Knüppel S, Andersen LF, Boeing H, on behalf of the European Food Consumption Validation C (2011) Estimating usual food intake distributions by using the multiple source method in the EPIC-potsdam calibration study. J Nutr 141(5):914–920. https://doi.org/10.3945/jn.109.120394
Afshin A, Sur PJ, Fay KA, Cornaby L, Ferrara G, Salama JS, Mullany EC, Abate KH, Abbafati C, Abebe Z, Afarideh M, Aggarwal A, Agrawal S, Akinyemiju T, Alahdab F, Bacha U, Bachman VF, Badali H, Badawi A, Bensenor IM, Bernabe E, Biadgilign SKK, Biryukov SH, Cahill LE, Carrero JJ, Cercy KM, Dandona L, Dandona R, Dang AK, Degefa MG, El Sayed ZM, Esteghamati A, Esteghamati S, Fanzo J, Farinha CSES, Farvid MS, Farzadfar F, Feigin VL, Fernandes JC, Flor LS, Foigt NA, Forouzanfar MH, Ganji M, Geleijnse JM, Gillum RF, Goulart AC, Grosso G, Guessous I, Hamidi S, Hankey GJ, Harikrishnan S, Hassen HY, Hay SI, Hoang CL, Horino M, Ikeda N, Islami F, Jackson MD, James SL, Johansson L, Jonas JB, Kasaeian A, Khader YS, Khalil IA, Khang Y-H, Kimokoti RW, Kokubo Y, Kumar GA, Lallukka T, Lopez AD, Lorkowski S, Lotufo PA, Lozano R, Malekzadeh R, März W, Meier T, Melaku YA, Mendoza W, Mensink GBM, Micha R, Miller TR, Mirarefin M, Mohan V, Mokdad AH, Mozaffarian D, Nagel G, Naghavi M, Nguyen CT, Nixon MR, Ong KL, Pereira DM, Poustchi H, Qorbani M, Rai RK, Razo-García C, Rehm CD, Rivera JA, Rodríguez-Ramírez S, Roshandel G, Roth GA, Sanabria J, Sánchez-Pimienta TG, Sartorius B, Schmidhuber J, Schutte AE, Sepanlou SG, Shin M-J, Sorensen RJD, Springmann M, Szponar L, Thorne-Lyman AL, Thrift AG, Touvier M, Tran BX, Tyrovolas S, Ukwaja KN, Ullah I, Uthman OA, Vaezghasemi M, Vasankari TJ, Vollset SE, Vos T, Vu GT, Vu LG, Weiderpass E, Werdecker A, Wijeratne T, Willett WC, Wu JH, Xu G, Yonemoto N, Yu C, Murray CJL (2019) Health effects of dietary risks in 195 countries, 1990–2017: a systematic analysis for the global burden of disease study 2017. Lancet 393(10184):1958–1972. https://doi.org/10.1016/S0140-6736(19)30041-8
Centers for Disease Control and Prevention (CDC) (2017) National Health and Nutrition Examination Survey (NHANES). MEC Laboratory Procedures Manual. https://wwwn.cdc.gov/nchs/data/nhanes/2017-2018/manuals/2017_MEC_Laboratory_Procedures_Manual.pdf.
Krebs-Smith SM, Pannucci TE, Subar AF, Kirkpatrick SI, Lerman JL, Tooze JA, Wilson MM, Reedy J (2018) Update of the healthy eating index: HEI-2015. J Acad Nutr Diet 118(9):1591–1602. https://doi.org/10.1016/j.jand.2018.05.021
Loprinzi PD (2015) Dose–response association of moderate-to-vigorous physical activity with cardiovascular biomarkers and all-cause mortality: Considerations by individual sports, exercise and recreational physical activities. Prev Med 81:73–77. https://doi.org/10.1016/j.ypmed.2015.08.014
Resciniti NV, Lohman MC, Wirth MD, Shivappa N, Hebert JR (2019) Dietary inflammatory index, pre-frailty and frailty among older US adults: evidence from the national health and nutrition examination survey, 2007–2014. J Nutr Health Aging 23(4):323–329. https://doi.org/10.1007/s12603-019-1164-3
R Core Team (2021) R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. Available online at https://www.R-project.org/
Lumley T (2021) Analysis of complex survey samples version 4.1–1. J Stat Soft 9(8). Available at https://cran.r-project.org/web/packages/survey/survey.pdf
Harrell Jr F (2021) rms: Regression Modeling Strategies. https://CRAN.R-project.org/package=rms.
Fox J, Weisberg S (2019) An R companion to applied regression, 3rd edn. Sage publications, Thousand Oaks, CA
Fernández-Montero A, Bes-Rastrollo M, Beunza JJ, Barrio-Lopez MT, de la Fuente-Arrillaga C, Moreno-Galarraga L, Martínez-González MA (2013) Nut consumption and incidence of metabolic syndrome after 6-year follow-up: the SUN (Seguimiento Universidad de Navarra, University of Navarra Follow-up) cohort. Public Health Nutr 16(11):2064–2072. https://doi.org/10.1017/S1368980012004442
Julibert A, del Mar BM, Gallardo-Alfaro L, Abbate M, Martínez-González MÁ, Salas-Salvadó J, Corella D, Fitó M, Martínez JA, Alonso-Gómez ÁM, Wärnberg J, Vioque J, Romaguera D, Lopez-Miranda J, Estruch R, Tinahones FJ, Lapetra J, Serra-Majem L, Cano-Ibañez N, Martín-Sánchez V, Pintó X, Gaforio JJ, Matía-Martín P, Vidal J, Vázquez C, Daimiel L, Ros E, Sayon-Orea C, Becerra-Tomás N, Gimenez-Alba IM, Castañer O, Abete I, Tojal-Sierra L, Pérez-López J, Notario-Barandiaran L, Colom A, Garcia-Rios A, Castro-Barquero S, Bernal R, Santos-Lozano JM, Fernández-Lázaro CI, Hernández-Alonso P, Saiz C, Zomeño MD, Zulet MA, Belló-Mora MC, Basterra-Gortari J, Canudas S, Goday A, Tur JA, investigators P-P (2020) Metabolic syndrome features and excess weight were inversely associated with nut consumption after 1-year follow-up in the PREDIMED-plus study. J Nutr 150(12):3161–3170. https://doi.org/10.1093/jn/nxaa289
Jung JY, Park SK, Oh C-M, Choi J-M, Ryoo J-H, Kim J, Kim MK (2019) The association between metabolic syndrome and peanuts, pine nuts, almonds consumption: the ansan and ansung study. Endocrine 65(2):270–277. https://doi.org/10.1007/s12020-019-01980-3
Yki-Järvinen H (2014) Non-alcoholic fatty liver disease as a cause and a consequence of metabolic syndrome. Lancet Diabetes Endocrinol 2(11):901–910. https://doi.org/10.1016/S2213-8587(14)70032-4
Asher G, Sassone-Corsi P (2015) Time for food: the intimate interplay between nutrition, metabolism, and the circadian clock. Cell 161(1):84–92. https://doi.org/10.1016/j.cell.2015.03.015
Monrroy H, Pribic T, Galan C, Nieto A, Amigo N, Accarino A, Correig X, Azpiroz F (2019) Meal enjoyment and tolerance in women and men. Nutrients. https://doi.org/10.3390/nu11010119
Nikodijevic CJ, Probst YC, Tan S-Y, Neale EP (2023) The effects of tree nut and peanut consumption on energy compensation and energy expenditure: a systematic review and meta-analysis. Adv Nutr 14(1):77–98. https://doi.org/10.1016/j.advnut.2022.10.006
Jenkins DJA, Kendall CWC, Faulkner D, Vidgen E, Trautwein EA, Parker TL, Marchie A, Koumbridis G, Lapsley KG, Josse RG, Leiter LA, Connelly PW (2002) A dietary portfolio approach to cholesterol reduction: Combined effects of plant sterols, vegetable proteins, and viscous fibers in hypercholesterolemia. Metabol Clin Exp 51(12):1596–1604. https://doi.org/10.1053/meta.2002.35578
Glenn AJ, Lo K, Jenkins DJA, Boucher BA, Hanley AJ, Kendall CWC, Manson JE, Vitolins MZ, Snetselaar LG, Liu S, Sievenpiper JL (2021) Relationship between a plant-based dietary portfolio and risk of cardiovascular disease: findings from the women’s health initiative prospective cohort study. J Am Heart Assoc. https://doi.org/10.1161/JAHA.121.021515
Salas-Salvadó J, Guasch-Ferré M, Lee C-H, Estruch R, Clish CB, Ros E (2016) Protective effects of the mediterranean diet on type 2 diabetes and metabolic syndrome. J Nutr 146(4):920S-927S. https://doi.org/10.3945/jn.115.218487
Dikariyanto V, Berry SE, Pot GK, Francis L, Smith L, Hall WL (2020) Tree nut snack consumption is associated with better diet quality and CVD risk in the UK adult population: national diet and nutrition survey (NDNS) 2008–2014. Public Health Nutr 23(17):3160–3169. https://doi.org/10.1017/S1368980019003914
Hassannejad R, Mohammadifard N, Kazemi I, Mansourian M, Sadeghi M, Roohafza H, Sarrafzadegan N (2019) Long-term nuts intake and metabolic syndrome: a 13-year longitudinal population-based study. Clin Nutr 38(3):1246–1252. https://doi.org/10.1016/j.clnu.2018.05.006
Dietary Guidelines Advisory Committee (2020) Scientific report of the 2020 dietary guidelines advisory committee: advisory report to the secretary of agriculture and the secretary of health and human services. U.S. Department of Agriculture, Agricultural Research Service, Washington, DC. Available at https://www.dietaryguidelines.gov/sites/default/files/2020-07/ScientificReport_of_the_2020DietaryGuidelinesAdvisoryCommittee_first-print.pdf
Moshfegh AJ, Rhodes DG, Baer DJ, Murayi T, Clemens JC, Rumpler WV, Paul DR, Sebastian RS, Kuczynski KJ, Ingwersen LA, Staples RC, Cleveland LE (2008) The US department of agriculture automated multiple-pass method reduces bias in the collection of energy intakes. Am J Clin Nutr 88(2):324–332. https://doi.org/10.1093/ajcn/88.2.324
Sorkin JD, Manary M, Smeets PAM, MacFarlane AJ, Astrup A, Prigeon RL, Hogans BB, Odle J, Davis TA, Tucker KL, Duggan CP, Tobias DK (2021) A guide for authors and readers of the American society for nutrition journals on the proper use of P values and strategies that promote transparency and improve research reproducibility. Am J Clin Nutr 114(4):1280–1285. https://doi.org/10.1093/ajcn/nqab223
Acknowledgements
The authors’ responsibilities were as follows—TWHT, ESG, and S-YT designed research; ESG, ENG, and S-YT extracted nut and seed intake data and conducted the HEI 2015 calculation; TWHT performed statistical analysis with assistance from GA; TWHT, ESG, GA, RMD, and S-YT interpreted the results. TWHT and S-YT drafted the paper with critical advice from ESG, GA, RMD, and ENG. All authors have read and approved the final manuscript. TWHT and S-YT had primary responsibility for the final content.
Funding
Open Access funding enabled and organized by CAUL and its Member Institutions.
Author information
Authors and Affiliations
Contributions
S-YT was involved in clinical studies that were funded by the Almond Board of California and the Californian Walnut Commission. S-YT, RMD, and ESG have received research grants from the International Nut and Dried Fruit Council. THTW, GA, and ENG report no conflicts of interest.
Corresponding author
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Wong, T.H.T., George, E.S., Abbott, G. et al. Nut and seed consumption is inversely associated with metabolic syndrome in females but not males: findings from the 2005–2018 NHANES data. Eur J Nutr 62, 2415–2427 (2023). https://doi.org/10.1007/s00394-023-03157-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00394-023-03157-1