
Abstract
Purpose
This umbrella review aimed to assess whether dietary protein intake with regard to quantitative (higher vs. lower dietary protein intake) and qualitative considerations (total, plant-based or animal-based protein intake) affects body weight (BW), fat mass (FM) and waist circumference (WC).
Methods
A systematic literature search was conducted in PubMed, Embase and Cochrane Database of Systematic Reviews for systematic reviews (SRs) with and without meta-analyses of prospective studies published between 04 October 2007 and 04 January 2022. Methodological quality and outcome-specific certainty of evidence of the retrieved SRs were assessed by using AMSTAR 2 and NutriGrade, respectively, in order to rate the overall certainty of evidence using predefined criteria.
Results
Thirty-three SRs were included in this umbrella review; 29 were based on randomised controlled trials, a few included cohort studies. In studies without energy restriction, a high-protein diet did not modulate BW, FM and WC in adults in general (all “possible” evidence); for older adults, overall certainty of evidence was “insufficient” for all parameters. Under hypoenergetic diets, a high-protein diet mostly decreased BW and FM, but evidence was “insufficient” due to low methodological quality. Evidence regarding an influence of the protein type on BW, FM and WC was “insufficient”.
Conclusion
“Possible” evidence exists that the amount of protein does not affect BW, FM and WC in adults under isoenergetic conditions. Its impact on the reduction in BW and FM under hypoenergetic conditions remains unclear; evidence for an influence of protein type on BW, FM and WC is “insufficient”.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Obesity is a chronic disease worldwide; its prevalence almost tripled between 1975 and 2016 [1]. Android obesity is of great concern due to the increased risk of obesity-associated diseases, such as type 2 diabetes mellitus, hypertension, cardiovascular diseases, and many types of cancer [2,3,4]. To prevent obesity, energy intake has to be adapted to the individual energy requirement. However, this is challenging as the availability of energy-dense foods [5] and physical inactivity have increased [6].
Diets rich in protein may be beneficial for the prevention and treatment of obesity as protein exerts a higher diet-induced thermogenesis than carbohydrates (CHO) and fat. Moreover, protein can maximise lean body mass retention during weight loss, which in turn may counteract a decrease in resting energy expenditure [7]. Furthermore, dietary protein stimulates the release of intestinal peptide hormones (e.g., glucagon like peptide-1, peptide YY) with anorexigenic properties, which may increase satiety, thereby reducing food consumption and energy intake [7]. Overall, high protein intake might favour a negative energy balance by increasing energy expenditure and decreasing energy intake; both might contribute to normalisation of body weight (BW) [7].
In addition, protein quality (digestibility, content of indispensable/essential amino acids [EAA], particularly leucine as key stimulus in muscle protein synthesis, availability of amino acids for muscle protein synthesis) may also be relevant for the prevention and treatment of obesity [8]. For example, whey protein has a higher protein quality (rapid digestion, high content of EAA) than casein. Moreover, amino acids from whey protein and casein are less catabolised than soya protein, thus increasing their availability for muscle protein synthesis [8]. Soya protein is digested rapidly, but contains less EAA than whey protein. Therefore, whey protein may be beneficial during weight loss since a higher preservation of lean body mass (or muscle mass) can be expected [8]. Moreover, whey protein and casein have higher effects on satiety than other proteins, which could promote weight loss by a stronger suppression of hunger sensations [8, 9].
International recommendations on protein intake are around 0.8 g/kg BW/day for healthy adults [10]. This corresponds to a mean daily intake of 11% of energy (EN%) for an adult with a reference BW of 70 kg and a total energy requirement of 2200 kcal/day. The recommendations on protein intake apply to people with normal weight; for people with under- or overweight or obesity, it is recommended to adjust the BW to the reference weight. In European countries, average protein intake of adults ranged from 67 to 114 g/day for men and 59 to 102 g/day for women, which corresponds to an average intake of 0.8–1.25 g/kg BW/day or 12–20 EN% [11].
The German Nutrition Society is currently developing an evidence-based guideline for protein intake regarding the impact of protein amount and type on several outcomes in the general adult population, namely bone health [12], kidney health [13], blood pressure, cancer, cardiovascular diseases, muscle health, type 2 diabetes mellitus and BW and related outcomes [14]. The current manuscript focuses on the latter. The collection of evidence for each outcome will form the basis for the overall conclusion of the guideline [14].
The key question behind this umbrella review was to assess the overall certainty of evidence whether dietary protein intake with regard to quantitative (higher vs. lower dietary protein intake) and qualitative (total, plant-based or animal-based protein intake) considerations affects BW, fat mass (FM) and waist circumference (WC).
Methods
We conducted an umbrella review (PROSPERO: CRD42018082395) following the methodology published by Kroke et al. [14]. Two authors each independently conducted the literature search, selection of systematic reviews (SRs), data extraction, assessment of methodological quality and outcome-specific certainty of evidence (AMA, JH, AL, AS), as well as the grading of the overall certainty of evidence (SE, SEg). Any disagreements were resolved by discussion and consensus [14].
Data sources and searches
The systematic literature search was performed in PubMed, Embase and Cochrane Database of Systematic Reviews for SRs with or without meta-analyses (MA) published between 04.10.2007 and 04.01.2022. The date of 10/2007 originates from the decision to cover a 10-year period, i.e. the initial database search was conducted in 10/2017, and the last update in 01/2022. The search strategies are presented in Supplementary Material 1. In addition to the database search, the reference lists of the included SRs were reviewed.
Selection of systematic reviews
Titles and/or abstracts of retrieved records were screened according to the pre-defined inclusion/exclusion criteria to identify potentially eligible publications. The full texts of potentially relevant publications were assessed for eligibility. It was tolerated that some of the primary studies were incorporated more than once into different SRs, the overlap of primary studies was documented and the percentage of overlapping was assessed by calculating the corrected cover area according to Pieper et al. [15].
Publications were included if they met the following criteria: (i) evaluated the association between protein intake and BW, FM and WC in the general adult population including older adults and recreational athletes, (ii) SR with or without MA of prospective studies in humans, i.e. randomised controlled trials (RCTs), prospective cohort studies, case-cohort studies or nested case–control studies. Inclusion of case–control studies was tolerated if another study type was predominant, (iii) manuscript was written in English or German.
Exclusion criteria were as follows: (i) study populations consisted exclusively of children, pregnant and/or lactating women and/or top athletes, (ii) not investigating the specific effect of protein, (iii) not investigating relevant protein–outcome relationships, (iv) conference proceedings or abstracts, (v) individual studies (RCTs, cohort studies, other primary studies), and (vi) umbrella reviews.
Data extraction
The following data from each included SR were extracted into a standardised form: the first author’s surname, year of publication, study type, duration range of primary studies, study population, intervention/exposure(s), outcome(s), effect estimate(s) including 95% confidence interval, P-value(s) and heterogeneity estimate(s). In case of missing data, corresponding authors were contacted.
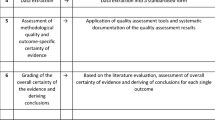
Assessment of methodological quality and outcome-specific certainty of evidence
The methodological quality of each retrieved SR was assessed by a modified version of the “A Measurement Tool to Assess Systematic Reviews 2” tool (AMSTAR 2) [16] (Supplementary Material 2). SRs were rated on a scale from “high” to “critically low” quality. SRs graded as “critically low” by AMSTAR 2 were excluded from the current work.
The NutriGrade scoring tool was used to rate the outcome-specific certainty of evidence of included SRs [17] by means of a numerical scoring system as high, moderate, low, or very low (Supplementary Material 3). The NutriGrade scoring tool was modified for the assessment of SRs without MA, as described by Kroke et al. [14]. If an SR reported more than one relevant outcome, each outcome-specific certainty of evidence was assessed separately.
Grading of the overall certainty of the evidence
After summarising the available evidence, two authors (SE and SEg) graded the overall certainty of evidence based on the criteria outlined in our protocol [14] and in Table 1. This rating was double-checked by staff members of the German Nutrition Society (AMA and JH) and thereafter reviewed and approved by all co-authors.
Results
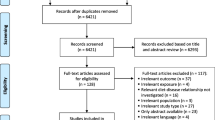
The process of study selection is outlined in Fig. 1. The literature search identified 7111 potentially relevant records. After removal of duplicates, 5206 records were excluded by screening on the basis of title and/or abstract. Thereafter, 107 records were excluded after assessing the full text. A total of 33 SRs were finally included in the present umbrella review [18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50]. These SRs were published between 07/2009 and 03/2022. A list of excluded records after full-text assessment including justifications for exclusion is provided in Supplementary Material 4.

Flow diagram
Study characteristics
Among these 33 SRs, 29 included solely RCTs [18,19,20,21,22,23,24,25,26,27,28,29, 31, 32, 35,36,37,38,39,40,41,42, 44,45,46,47,48,49,50]. One SR considered solely cohort studies [30] and three SRs additionally addressed RCTs [33, 34, 43]. In total, 26 SRs conducted an MA [20,21,22,23,24,25,26,27,28,29, 32, 35,36,37,38,39,40,41,42, 44,45,46,47,48,49,50] and seven SRs were without MA [18, 19, 30, 31, 33, 34, 43]. One SR with MA analysed dose–response relationships [35]. Some of the primary studies were incorporated more than once into different SRs, but overall there was only a “slight” overlap of primary studies of 2.2%, determined as corrected covered area according to Pieper et al. [15], see Supplementary Material 5. BW was addressed in 29 SRs [18,19,20, 22, 23, 26,27,28,29,30,31,32,33,34,35, 37,38,39,40,41,42,43,44,45,46,47,48,49,50], FM in 21 SRs [18, 23,24,25, 27, 29, 32,33,34, 36,37,38,39,40,41,42,43, 45, 46, 49, 50] and WC in 13 SRs [18, 21, 30, 32,33,34,35, 40, 42, 43, 48,49,50].
Most SRs investigated the effect/association of total protein [18, 21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42, 44,45,46,47,48,49,50], and five compared different types of protein (e.g., soya vs. whey protein) [19, 20, 25, 40, 43]. Protein intake differed highly between the SRs, but the amount in the control group reached at least the recommended protein intake for adults (0.8 g/kg BW/day for adults < 65 years, 1.0 g/kg BW/day for adults > 65 years, which corresponds to an intake about 10% EN under isoenergetic conditions) (Table 2). Dietary intervention of included RCTs ranged from two to 208 weeks; the duration of included cohort studies ranged from one to seven years (Table 2). In three SRs, the study durations of included studies were not mentioned or remained unclear [33, 34, 48]. Six SRs focused on the effects of protein and/or different protein types in older adults [22, 23, 28, 29, 36, 41]. All SRs except one [27] were based on studies with men and women. The included SRs contained healthy participants [18, 25, 27, 33, 45] and subjects with risk factors of cardiometabolic diseases [20, 21, 23, 26, 29, 36, 42, 48], one SR focused on nursing home residents [22] and another on older adults with frailty [29]. In most SRs, specific restrictions on the participants’ health status were lacking [19, 22, 24, 28, 30,31,32, 34, 35, 37,38,39,40,41, 43, 44, 46, 47, 49, 50].
Methodological quality
Overall scores of AMSTAR 2 for each included SR are summarised in Table 2. Supplementary Material 6 provides a more detailed overview showing the assessments of each individual item. Methodological quality of the included SRs as assessed with AMSTAR 2 was high for eight SRs, moderate for ten SRs, and low for 15 SRs. One SR rated as “critically low” by AMSTAR 2 was excluded from the current work (Fig. 1).
Associations/effects of protein intake and outcome-specific certainty of the evidence
The impact of total protein intake on BW-related outcomes was investigated in 29 RCTs [18,19,20,21,22,23,24,25,26,27,28,29, 31, 32, 35,36,37,38,39,40,41,42, 44,45,46,47,48,49,50]; study characteristics are shown in Table 2. Four SRs included cohort studies [30, 33, 34, 43]; the results are shown in Table 2. Out of the 98 NutriGrade ratings of outcome-specific certainty of evidence, twelve were rated very low, 61 low and 25 moderate, respectively; none was ranked as high. Overall scores of NutriGrade for each SR are summarised in Table 2. Supplementary Material 7 provides a more detailed account showing the assessments of each individual NutriGrade item.
(1) Effects of the amount of protein intake on BW, FM and WC in studies without energy restrictions
The effect of the amount of protein intake on BW, FM and/or WC in adults under predominantly isoenergetic conditions was investigated in 16 SRs, among them 13 SRs with MA [21, 24, 25, 27, 32, 35, 40, 42, 45,46,47,48,49] and 3 SRs without MA [18, 30, 33] (Table 2). SRs with MA defined different inclusion criteria on protein intake: ≥ 25 EN% vs. ≤ 20 EN% [32], differences of ≥ 3 EN% [49] and ≥ 5 EN% [35] between both treatments, respectively, or supplemental protein intake of 20–50 g/day [42], 0.3–1.35 g/kg BW/day [40] and 6–48 g/day [27]. Five SRs with MA did not consider the amount of protein as inclusion criteria [24, 45,46,47,48]. In seven out of 13 SRs with MA, the duration of protein intervention was defined as inclusion criteria with ≥ 2 weeks [21, 42], ≥ 4 weeks [25, 40, 49], ≥ 6 weeks [24] and ≥ 12 months [32]. Intervention was conducted by supplementation with whey protein [18, 21, 24, 27, 40, 42, 46], soya protein [45, 46, 48], beef protein [25] or dietary proteins without further specification [32, 33, 35, 47, 49].
Four out of 10 SRs with MA of RCTs showed a reduction of BW [35, 42, 47, 49], whereas six did not find any effects [27, 32, 40, 45, 46, 48] (Table 2). The impact on FM was investigated in nine SRs with MA. Again, most of them did not find an effect of the quantity of protein consumed on FM [24, 25, 27, 32, 40, 45, 46]. However, Vogtschmidt et al. [49] and Wirunsawanya et al. [42] found a decrease in FM after higher protein consumption (Table 2). Seven SRs with MA considered WC; five of them found no effects [32, 40, 42, 48, 49], whereas two found a decrease in WC by protein intervention [21, 35]. A multivariable meta-regression analysis did not show a dose–response relationship between the additional protein intake by intervention and the changes in BW as well as WC taking into account differences in the intake of protein (EN%), total energy and in CHO (EN%) between intervention and control groups [35].
To sum up, most SRs with MA did not find an effect of the amount of protein on BW, FM and WC in studies without energy restriction. For BW, FM and WC, the majority of the included SRs with and without MA reached at least a low outcome-specific certainty of evidence, and the majority of all included SRs reached at least a methodological quality of moderate (Table 2). Therefore, the overall certainty of evidence was graded as “possible” that the amount of protein intake does not affect BW, FM and WC in adults under isoenergetic conditions.
(2) Effects of the amount of protein intake on BW, FM and WC in studies without energy restrictions in the subgroup of older adults
The impact of the amount of protein intake on BW under predominantly isoenergetic study conditions in older adults was investigated in five SRs with MA [22, 23, 28, 29, 41]; four considered FM [23, 29, 36, 41] (Table 2). WC was not investigated by any SR. Only Donaldson et al. [22] defined protein intake as inclusion criterion, which had to be at least 10 g/day higher in the protein intervention group compared to the control group. The period of intervention was not an inclusion criterion in any SR except Hidayat et al. [41], which included only RCTs with an intervention duration of more than twelve weeks. Intervention was performed for 3 to 6 months [28], 12 to 72 weeks [41], 8 to 24 weeks [36] and up to 9 months [22, 29]. Intervention was conducted by supplementation of milk protein [28, 41] or by intake of non-meat protein and mixture of (dietary) protein types except meat [29, 36] (Table 2). Two SRs with MA did not provide any details on the type of protein [22, 23].
Five SRs with MA investigated the effect of the amount of protein intake on BW; three of them found an increase in BW in older adults [22, 28, 29], whereas two did not detect an effect [23, 41] (Table 2). The impact on FM was investigated in four SRs with MA. Three of them did not find an effect on FM [23, 29, 41]. Only Liao et al. [36] found a decrease in FM (Table 2).
To sum up, most SRs with MA in older adults found an increase in BW due to a higher protein intake without modulating FM. However, the majority of the included SRs reached only a low outcome-specific certainty of evidence and had only low methodological quality (Table 2). Consequently, the overall certainty of evidence was graded as “insufficient” that the amount of protein ingested may increase BW without affecting FM in older adults under isoenergetic conditions. Since no SR was identified for WC, evidence was also “insufficient”.
(3) Effects of the amount of protein intake on BW, FM and WC in studies with energy restriction
The effect of the amount of protein intake on BW under hypoenergetic study conditions was investigated in six SRs with MA [27, 35, 37,38,39, 50] and in one SR without MA [31]; the effect on FM was studied in six SRs with MA [23, 27, 37,38,39, 50] (Table 2). Two SRs with MA investigated WC [35, 50]. Protein intervention and study duration differed strongly between SRs (Table 2). For example, in the SR with MA of Wycherley et al. [39] protein intake differed at least by 10 EN% between energy-restricted diet with high vs. standard-protein content with an intervention of ≥ 4 weeks. In the SR with MA of Kim et al. [37], protein intake was > 25 EN% (or > 1.0 g/kg BW/day) vs. < 25 EN% (or < 1.0 g/kg BW/day) for at least 8 weeks (Table 2). Intervention was conducted with a mixture of (dietary) protein types as part of a whole diet approach (Table 2).
Four out of six SRs with MA found a decrease in BW in response to a higher protein intake under hypoenergetic conditions [35, 38, 39, 50], whereas two did not observe an effect of the protein intervention [27, 37]. FM was investigated by six SRs with MA as outcome [23, 27, 37,38,39, 50], and five of them found a decrease in FM [23, 37,38,39, 50]. WC decreased in the MA of Santesso et al. [35], but did not change in the MA of Zhang et al. [50] (Table 2).
To sum up, the majority of SRs with MA found a stronger decrease in BW by a higher intake of protein under hypoenergetic conditions, but most of the included SRs reached a low outcome-specific certainty of evidence and a low methodological quality. Therefore, the overall certainty of evidence for an impact of protein intake on BW under hypoenergetic conditions was rated as “insufficient”. In most SRs with MA, FM decreased in response to a higher intake of protein under energy restriction, but the majority of included SRs reached only a low outcome-specific certainty of evidence and a low methodological quality. Hence, the overall certainty of evidence that a protein-rich hypoenergetic diet affects FM is “insufficient”. For WC, the effect of protein intake was also judged to be “insufficient” as consistent risk associations/effects were lacking (Table 2).
(4) Effects of the amount of protein intake on maintenance of BW, FM and WC after BW reduction in subjects with overweight/obesity
Effects of the amount of protein intake on the maintenance of BW after a previous weight loss in adults with overweight or obesity through an energy-restricted diet were investigated in three SRs, two of them with MA [26, 44] and one without MA [34]. We did not identify any SRs with FM as outcome parameter. One SR without MA investigated the effects on WC [34]. As shown in Table 2, all SRs considered studies with highly different protein intakes (e.g., addition of 30–48 g/day or addition of 10–15 EN%) with a duration of 3 to 12 months [26], 3 months to 3 years [44] or ≥ 6 months [34].
Both SRs with MA found a further decrease in BW with higher protein intake compared to lower intake after initial weight loss [26, 44]. In the SR without MA, total protein intake did not show consistent associations with changes in BW or WC [34] (Table 2).
To sum up, a further decrease in BW after BW reduction was found in both SRs with MA, which may contribute to long-term weight maintenance. Yet, as most SRs reached a very low outcome-specific certainty of evidence and a low methodological quality, the overall certainty of evidence was graded as “insufficient” that a higher protein intake prevents a regain of BW in adults with overweight or obesity after achieving weight loss by means of an energy-restricted diet. Due to the lack of SRs on FM, the overall certainty of evidence for an association between the amount of protein intake and FM was “insufficient”. For WC, only a single SR without MA is available showing different associations with protein intake on the basis of two cohort studies. Therefore, the overall certainty of evidence was judged as “insufficient” without considering the grading criteria.
(5) Effects of the type of protein on BW, FM and WC
The effects of the type of protein on BW were investigated in four SRs. Two of them included an MA and were based on RCTs [20, 40]. Two SRs without MA included intervention studies [19, 43], Chalvon-Demersay et al. [43] additionally included cohort studies. FM was investigated in two SRs with MA [25, 40] and two SRs without MA [19, 43]. WC was investigated in one SR with MA [40] and in two SRs without MA [19, 43]. The participants were mostly healthy [25, 40, 43], partly with metabolic impairment [43], or they suffered from hypercholesterolaemia [20]. Two SRs with MA compared the effect of plant vs. animal protein for 4 to 24 weeks [20] and 5 to 7 years [43], respectively. Another SR with MA studied the effect of whey protein vs. other proteins [40]. SRs without MA compared a variety of plant proteins (mostly soya) with protein of animal origin (mostly casein) [43] or alternative plant proteins (e.g., lupine, pea, fava bean, rice, oat, hemp, lentil) with milk protein [19] (Table 2).
Neither of the SRs with MA found an effect of the type of protein on BW [20, 40]; the results of SRs without MA are consistent since most of the included RCTs did not report different effects of animal and plant protein on BW [19, 43]. Valenzuela et al. [25] compared the intake of beef protein and whey protein on FM in healthy adults, mostly athletes, but did not find differences in these types of protein. Miller et al. [40] examined whey protein vs. other proteins, but did not find a specific effect of whey protein. Supplementation of whey protein did not affect WC compared to other proteins [40]. Most RCTs in SRs without MA did not find an effect of the protein type on WC [19, 43]. Results from cohort studies are unclear [43] (Table 2).
To sum up, neither of the SRs with MA showed an effect of protein type on BW, FM and WC. The results from SRs without MA on these parameters remain unclear. As the majority of included SRs reached a low methodological quality and a low outcome-specific certainty of evidence for each outcome, the overall certainty of evidence that the type of protein may influence BW, FM and WC was considered to be “insufficient”.
Discussion
The aim of this umbrella review was to assess whether the amount and type of protein may affect BW, FM and WC in adults with consideration of the overall certainty of evidence. To our knowledge, this umbrella review is the first to provide a summary evidence assessment of previous SRs. Our major finding is that there is “possible” evidence that under isoenergetic study conditions the amount of protein did not affect BW, FM and WC in the general adult population. For further settings, such as (i) older adults, (ii) hypoenergetic diets, and (iii) diets following weight reduction, the overall certainty of evidence was graded as “insufficient”. Moreover, the evidence for an influence of the type of protein on BW, FM and WC was also “insufficient”.
Our finding that the amount of protein did not affect BW and related parameters in studies without intended energy restriction may be explained by the combination of several factors, such as methodological limitations (e.g., ad libitum food consumption in free-living subjects, which is determined by a couple of exogeneous factors; high variation in the duration of interventions). Furthermore, the assumed physiological effect of a high protein intake (e.g., thermogenic effect) seems to be negligible in settings without energy restriction.
For older adults, albeit with “insufficient” evidence, most of the considered SRs with MA found an increase in BW in response to higher protein intakes (under isoenergetic conditions), which could not be explained by an increase in FM. This suggests that older people may benefit from a high-protein diet since the observed increase in BW may be partly explained by fat-free mass. Some nutrition societies (e.g., German Nutrition Society, ESPEN) recommend a higher protein intake (e.g., 1.0 vs. 0.8 g/kg BW/day) for older adults to combat age-related losses of muscle mass and muscle strength [51, 52]. In five out of six SRs, the higher protein intake was achieved via administration of milk protein including whey protein [22, 28, 29, 36, 41] (Table 2), which was mostly combined with physical activity [22, 23, 29, 36, 41]. Whey protein has been discussed to be an optimal protein source to support muscle protein synthesis at rest and following resistance training to induce muscle hypertrophy and strength gains. The anabolic effect of whey protein is explained by its amino acid content (high EAA, branched-chain amino acids, particularly leucine), rapid digestibility, and high availability within the plasma and muscle tissue upon consumption to induce muscle protein synthesis [8].
Under hypoenergetic study conditions, most of the SRs with MA showed that a higher protein intake lowers BW and FM more than a lower protein intake under free-living conditions. The overall certainty of evidence was only rated as “insufficient” as the demands on methodological quality were not fulfilled. Protein intake with a high-protein diet was > 1.0 g/kg BW/day in two SRs of RCTs [23, 37]. Effects attributed to protein, such as increased diet-induced thermogenesis and hunger suppression/satiety, seem to be especially relevant under the setting of energy restriction and weight reduction [53, 54].
Whether the origin of protein, e.g., from animal vs. plants, has an impact on BW, FM and WC remains unclear due to “insufficient” evidence. Current dietary guidelines recommend plant-based diets. In addition to vegetables, fruit and cereals, this also implies a regular consumption of protein sources of plant origin, such as legumes and nuts [55]. Due to the great importance of plant-based foods as part of a healthy and sustainable diet, further studies on the role of the protein type on BW, FM and WC are needed.
Currently, a lot of SRs are available on the impact of protein quantity on BW and associated parameters in different settings. This allows differentiated statements on the impact of protein amount on BW, FM and WC. Considering the type of protein, however, only a few SRs could be found; these investigated quite different questions (e.g., animal vs. plant protein; whey vs. other protein). Moreover, the investigation of the effects of protein type requires an isonitrogeneous diet, which is difficult to implement if natural foods are used. This is only practicable by using protein supplements or isolates/concentrates. If natural food is used as a protein source, nutrient composition and energy density of the diets may be different. This might affect hunger and satiety, thereby influencing energy balance and thus BW in the longer term. This point concerns studies on protein type, but also on the amount of protein. An increased intake of dietary protein requires a simultaneous decrease in either CHO or fat intake to ensure an equal supply of energy. This aspect of energy substitution is important, and it is rather questionable whether this was considered in all SRs included. This problem might have been resolved by stricter criteria for the selection of SRs, but this would have considerably reduced the number of relevant SRs. Our search and selection strategy can also be critically questioned with regard to the study collective. The aim of our umbrella review was to investigate the health-promoting effects of the protein. Some SR included both healthy adults and also subjects at risk of obesity-associated diseases (Table 2). A further limitation could be that the literature search was last updated in 01/2022, and thus, it cannot be ruled out that any very recently published SR regarding the effect of protein intake on health outcomes have not been included in the present umbrella review.
About one-fourth of all SRs of RCTs defined the additional protein intake by intervention or the difference in protein intake compared to control treatment as criteria for eligibility [22, 32, 35, 37, 39, 49], whereas most SRs did not [18,19,20,21, 23,24,25,26,27,28,29, 31, 33, 34, 36, 38, 40,41,42,43,44,45,46,47,48, 50]. The protein intake by intervention was mostly given in grammes per day [18, 19, 21, 22, 25, 27,28,29, 36, 41,42,43,44,45,46, 48] and partly in grammes per kg BW [21, 23, 36, 37, 39,40,41, 45, 50]. Sometimes, total protein intake for both treatments was provided in EN% [31,32,33,34,35, 37,38,39, 44, 47, 49]. In two SRs, data on protein intake were completely missing [20, 24]. These differences make it difficult to compare the different SRs with each other to derive a specific amount of protein associated with a preventive effect on BW.
We included the results of all relevant SRs, regardless of overlap as our purpose was to present and describe the current body of SR evidence. Having assessed the extent of primary study overlap between the SRs, bias due to multiple inclusion of the same primary studies in different SRs is unlikely, as the primary study overlap is only small at 2.2%.
In conclusion, it is rather unlikely that the amount of protein may affect BW, FM and WC in adults under isoenergetic conditions. The impact of a high-protein diet concerning body composition and the reduction of BW under hypoenergetic conditions remains unclear. In addition, the evidence for an influence of the type of protein on BW, FM and WC is “insufficient”. Thus, further SRs of RCTs with high methodological quality are mandatory. This also implies a sufficient number of well-controlled and well-designed RCTs.
Abbreviations
- AMSTAR 2:
-
A Measurement Tool to Assess Systematic Reviews 2
- BW:
-
Body weight
- CHO:
-
Carbohydrates
- EAA:
-
Essential amino acids
- EN%:
-
Percentage of energy intake
- FM:
-
Fat mass
- MA:
-
Meta-analysis/meta-analyses
- RCT(s):
-
Randomised controlled trial(s)
- SR(s):
-
Systematic review(s)
- WC:
-
Waist circumference
References
WHO (2021) Obesity and overweight. https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight
Powell-Wiley TM, Poirier P, Burke LE, Despres JP, Gordon-Larsen P, Lavie CJ, Lear SA, Ndumele CE, Neeland IJ, Sanders P, St-Onge MP, American Heart Association Council on L, Cardiometabolic H, Council on C, Stroke N, Council on Clinical C, Council on E, Prevention, Stroke C (2021) Obesity and cardiovascular disease: a scientific statement from the American Heart Association. Circulation 143(21):e984–e1010. https://doi.org/10.1161/CIR.0000000000000973
Ross R, Neeland IJ, Yamashita S, Shai I, Seidell J, Magni P, Santos RD, Arsenault B, Cuevas A, Hu FB, Griffin BA, Zambon A, Barter P, Fruchart JC, Eckel RH, Matsuzawa Y, Despres JP (2020) Waist circumference as a vital sign in clinical practice: a Consensus Statement from the IAS and ICCR Working Group on Visceral Obesity. Nat Rev Endocrinol 16(3):177–189. https://doi.org/10.1038/s41574-019-0310-7
Lauby-Secretan B, Scoccianti C, Loomis D, Grosse Y, Bianchini F, Straif K, International Agency for Research on Cancer Handbook Working G (2016) Body fatness and cancer-viewpoint of the IARC Working Group. N Engl J Med 375(8):794–798. https://doi.org/10.1056/NEJMsr1606602
Grill HJ (2020) A Role for GLP-1 in treating hyperphagia and obesity. Endocrinology. https://doi.org/10.1210/endocr/bqaa093
Guthold R, Stevens GA, Riley LM, Bull FC (2018) Worldwide trends in insufficient physical activity from 2001 to 2016: a pooled analysis of 358 population-based surveys with 1.9 million participants. Lancet Glob Health 6(10):e1077–e1086. https://doi.org/10.1016/S2214-109X(18)30357-7
Moon J, Koh G (2020) Clinical evidence and mechanisms of high-protein diet-induced weight loss. J Obes Metab Syndr 29(3):166–173. https://doi.org/10.7570/jomes20028
Devries MC, Phillips SM (2015) Supplemental protein in support of muscle mass and health: advantage whey. J Food Sci 80(Suppl 1):A8–A15. https://doi.org/10.1111/1750-3841.12802
Simonson M, Boirie Y, Guillet C (2020) Protein, amino acids and obesity treatment. Rev Endocr Metab Disord 21(3):341–353. https://doi.org/10.1007/s11154-020-09574-5
Hruby A, Jacques PF (2021) Protein intake and human health: implications of units of protein intake. Adv Nutr 12(1):71–88. https://doi.org/10.1093/advances/nmaa097
EFSA (2012) Scientific opinion on dietary reference values for protein. EFSA J 10(2):2557. https://doi.org/10.2903/j.efsa.2012.2557
Zittermann A, Schmidt A, Haardt J, Kalotai N, Lehmann A, Egert S, Ellinger S, Kroke A, Lorkowski S, Louis S, Schulze MB, Schwingshackl L, Siener R, Stangl GI, Volkert D, Watzl B, Bischoff-Ferrari HA on behalf of the German Nutrition Society (2023) Protein intake and bone health: an umbrella review of systematic reviews for the evidence-based guideline of the German Nutrition Society. Osteoporos Int. https://doi.org/10.1007/s00198-023-06709-7
Remer T, Kalotai N, Amini AM, Lehmann A, Schmidt A, Bischoff-Ferrari HA, Egert S, Ellinger S, Kroke A, Kuhn T, Lorkowski S, Nimptsch K, Schwingshackl L, Zittermann A, Watzl B, Siener R on behalf of the German Nutrition Society (2023) Protein intake and risk of urolithiasis and kidney diseases: an umbrella review of systematic reviews for the evidence-based guideline of the German Nutrition Society. Eur J Nutr 62(5):1957–1975. https://doi.org/10.1007/s00394-023-03143-7
Kroke A, Schmidt A, Amini AM, Kalotai N, Lehmann A, Haardt J, Bauer JM, Bischoff-Ferrari HA, Boeing H, Egert S, Ellinger S, Kuhn T, Louis S, Lorkowski S, Nimptsch K, Remer T, Schulze MB, Siener R, Stangl GI, Volkert D, Zittermann A, Buyken AE, Watzl B, Schwingshackl L on behalf of the German Nutrition Society (2022) Dietary protein intake and health-related outcomes: a methodological protocol for the evidence evaluation and the outline of an evidence to decision framework underlying the evidence-based guideline of the German Nutrition Society. Eur J Nutr 61(4):2091–2101. https://doi.org/10.1007/s00394-021-02789-5
Pieper D, Antoine SL, Mathes T, Neugebauer EA, Eikermann M (2014) Systematic review finds overlapping reviews were not mentioned in every other overview. J Clin Epidemiol 67(4):368–375. https://doi.org/10.1016/j.jclinepi.2013.11.007
Shea BJ, Reeves BC, Wells G, Thuku M, Hamel C, Moran J, Moher D, Tugwell P, Welch V, Kristjansson E, Henry DA (2017) AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 358:j4008. https://doi.org/10.1136/bmj.j4008
Schwingshackl L, Knuppel S, Schwedhelm C, Hoffmann G, Missbach B, Stelmach-Mardas M, Dietrich S, Eichelmann F, Kontopantelis E, Iqbal K, Aleksandrova K, Lorkowski S, Leitzmann MF, Kroke A, Boeing H (2016) Perspective: NutriGrade: a scoring system to assess and judge the meta-evidence of randomized controlled trials and cohort studies in nutrition research. Adv Nutr 7(6):994–1004. https://doi.org/10.3945/an.116.013052
Blair M, Kellow NJ, Dordevic AL, Evans S, Caissutti J, McCaffrey TA (2020) Health benefits of whey or colostrum supplementation in adults ≥35 years; a systematic review. Nutrients 12(2):299. https://doi.org/10.3390/nu12020299
Lonnie M, Laurie I, Myers M, Horgan G, Russell WR, Johnstone AM (2020) Exploring health-promoting attributes of plant proteins as a functional ingredient for the food sector: a systematic review of human interventional studies. Nutrients 10(3):360. https://doi.org/10.3390/nu12082291
Zhao H, Song A, Zheng C, Wang M, Song G (2020) Effects of plant protein and animal protein on lipid profile, body weight and body mass index on patients with hypercholesterolemia: a systematic review and meta-analysis. Acta Diabetol 57(10):1169–1180. https://doi.org/10.1007/s00592-020-01534-4
Badely M, Sepandi M, Samadi M, Parastouei K, Taghdir M (2019) The effect of whey protein on the components of metabolic syndrome in overweight and obese individuals; a systematic review and meta-analysis. Diabetes Metab Syndr 13(6):3121–3131. https://doi.org/10.1016/j.dsx.2019.11.001
Donaldson AIC, Smith TO, Alder S, Johnstone AM, De Roos B, Aucott LS, Gordon AL, Myint PK (2019) Effect of nonmeat, high-protein supplementation on quality of life and clinical outcomes in older residents of care homes: a systematic review and meta-analysis. Nutr Rev 77(2):116–127. https://doi.org/10.1093/nutrit/nuy061
Hsu KJ, Liao CD, Tsai MW, Chen CN (2019) Effects of exercise and nutritional intervention on body composition, metabolic health, and physical performance in adults with sarcopenic obesity: a meta-analysis. Nutrients 11(9):2163. https://doi.org/10.3390/nu11092163
Li M, Liu F (2019) Effect of whey protein supplementation during resistance training sessions on body mass and muscular strength: a meta-analysis. Food Funct 10(5):2766–2773. https://doi.org/10.1039/c9fo00182d
Valenzuela PL, Mata F, Morales JS, Castillo-Garcia A, Lucia A (2019) Does beef protein supplementation improve body composition and exercise performance? A systematic review and meta-analysis of randomized controlled trials. Nutrients 11(6):1429. https://doi.org/10.3390/nu11061429
van Baak MA, Mariman ECM (2019) Dietary strategies for weight loss maintenance. Nutrients 11(8):1916. https://doi.org/10.3390/nu11081916
Bergia RE 3rd, Hudson JL, Campbell WW (2018) Effect of whey protein supplementation on body composition changes in women: a systematic review and meta-analysis. Nutr Rev 76(7):539–551. https://doi.org/10.1093/nutrit/nuy017
Dewansingh P, Melse-Boonstra A, Krijnen WP, van der Schans CP, Jager-Wittenaar H, van den Heuvel E (2018) Supplemental protein from dairy products increases body weight and vitamin D improves physical performance in older adults: a systematic review and meta-analysis. Nutr Res 49:1–22. https://doi.org/10.1016/j.nutres.2017.08.004
Liao CD, Lee PH, Hsiao DJ, Huang SW, Tsauo JY, Chen HC, Liou TH (2018) Effects of protein supplementation combined with exercise intervention on frailty indices, body composition, and physical function in frail older adults. Nutrients 10(12):1916. https://doi.org/10.3390/nu10121916
Summerbell CD, Douthwaite W, Whittaker V, Ells LJ, Hillier F, Smith S, Kelly S, Edmunds LD, Macdonald I (2009) The association between diet and physical activity and subsequent excess weight gain and obesity assessed at 5 years of age or older: a systematic review of the epidemiological evidence. Int J Obes (Lond) 33(Suppl 3):S1-92. https://doi.org/10.1038/ijo.2009.80
Lepe M, Bacardi Gascon M, Jimenez Cruz A (2011) Long-term efficacy of high-protein diets: a systematic review. Nutr Hosp 26(6):1256–1259. https://doi.org/10.1590/S0212-16112011000600010
Schwingshackl L, Hoffmann G (2013) Long-term effects of low-fat diets either low or high in protein on cardiovascular and metabolic risk factors: a systematic review and meta-analysis. Nutr J 12:48. https://doi.org/10.1186/1475-2891-12-48
Pedersen AN, Kondrup J, Borsheim E (2013) Health effects of protein intake in healthy adults: a systematic literature review. Food Nutr Res 57. https://doi.org/10.3402/fnr.v57i0.21245
Fogelholm M, Anderssen S, Gunnarsdottir I, Lahti-Koski M (2012) Dietary macronutrients and food consumption as determinants of long-term weight change in adult populations: a systematic literature review. Food Nutr Res. https://doi.org/10.3402/fnr.v56i0.19103
Santesso N, Akl EA, Bianchi M, Mente A, Mustafa R, Heels-Ansdell D, Schunemann HJ (2012) Effects of higher- versus lower-protein diets on health outcomes: a systematic review and meta-analysis. Eur J Clin Nutr 66(7):780–788. https://doi.org/10.1038/ejcn.2012.37
Liao CD, Tsauo JY, Wu YT, Cheng CP, Chen HC, Huang YC, Chen HC, Liou TH (2017) Effects of protein supplementation combined with resistance exercise on body composition and physical function in older adults: a systematic review and meta-analysis. Am J Clin Nutr 106(4):1078–1091. https://doi.org/10.3945/ajcn.116.143594
Kim JE, O’Connor LE, Sands LP, Slebodnik MB, Campbell WW (2016) Effects of dietary protein intake on body composition changes after weight loss in older adults: a systematic review and meta-analysis. Nutr Rev 74(3):210–224. https://doi.org/10.1093/nutrit/nuv065
Clifton PM, Condo D, Keogh JB (2014) Long term weight maintenance after advice to consume low carbohydrate, higher protein diets–a systematic review and meta analysis. Nutr Metab Cardiovasc Dis 24(3):224–235. https://doi.org/10.1016/j.numecd.2013.11.006
Wycherley TP, Moran LJ, Clifton PM, Noakes M, Brinkworth GD (2012) Effects of energy-restricted high-protein, low-fat compared with standard-protein, low-fat diets: a meta-analysis of randomized controlled trials. Am J Clin Nutr 96(6):1281–1298. https://doi.org/10.3945/ajcn.112.044321
Miller PE, Alexander DD, Perez V (2014) Effects of whey protein and resistance exercise on body composition: a meta-analysis of randomized controlled trials. J Am Coll Nutr 33(2):163–175. https://doi.org/10.1080/07315724.2013.875365
Hidayat K, Chen GC, Wang Y, Zhang Z, Dai X, Szeto IMY, Qin LQ (2018) Effects of milk proteins supplementation in older adults undergoing resistance training: a meta-analysis of randomized control trials. J Nutr Health Aging 22(2):237–245. https://doi.org/10.1007/s12603-017-0899-y
Wirunsawanya K, Upala S, Jaruvongvanich V, Sanguankeo A (2018) Whey protein supplementation improves body composition and cardiovascular risk factors in overweight and obese patients: a systematic review and meta-analysis. J Am Coll Nutr 37(1):60–70. https://doi.org/10.1080/07315724.2017.1344591
Chalvon-Demersay T, Azzout-Marniche D, Arfsten J, Egli L, Gaudichon C, Karagounis LG, Tome D (2017) A systematic review of the effects of plant compared with animal protein sources on features of metabolic syndrome. J Nutr 147(3):281–292. https://doi.org/10.3945/jn.116.239574
Johansson K, Neovius M, Hemmingsson E (2014) Effects of anti-obesity drugs, diet, and exercise on weight-loss maintenance after a very-low-calorie diet or low-calorie diet: a systematic review and meta-analysis of randomized controlled trials. Am J Clin Nutr 99(1):14–23. https://doi.org/10.3945/ajcn.113.070052
Saboori SF, Falahi E, Rad EY, Asbaghi O, Khosroshahi MZ, Clark CCT, Jafarnejad S (2019) Does soy protein supplementation affect body composition in healthy exerciser adults? A systematic review and meta-analysis of clinical trials. Obesity Med 14:100083
Piri Damaghi M, Mirzababaei A, Moradi S, Daneshzad E, Tavakoli A, Clark CCT, Mirzaei K (2022) Comparison of the effect of soya protein and whey protein on body composition: a meta-analysis of randomised clinical trials. Br J Nutr 127(6):885–895. https://doi.org/10.1017/S0007114521001550
Hansen TT, Astrup A, Sjodin A (2021) Are dietary proteins the key to successful body weight management? A systematic review and meta-analysis of studies assessing body weight outcomes after interventions with increased dietary protein. Nutrients 13(9):3193. https://doi.org/10.3390/nu13093193
Mohammadifard N, Sajjadi F, Haghighatdoost F (2021) Effects of soy consumption on metabolic parameters in patients with metabolic syndrome: a systematic review and meta-analysis. EXCLI J 20:665–685. https://doi.org/10.17179/excli2021-3348
Vogtschmidt YD, Raben A, Faber I, de Wilde C, Lovegrove JA, Givens DI, Pfeiffer AFH, Soedamah-Muthu SS (2021) Is protein the forgotten ingredient: effects of higher compared to lower protein diets on cardiometabolic risk factors. A systematic review and meta-analysis of randomised controlled trials. Atherosclerosis 328:124–135. https://doi.org/10.1016/j.atherosclerosis.2021.05.011
Zhang Y, Chen X, Allison DB, Xun P (2022) Efficacy and safety of a specific commercial high-protein meal-replacement product line in weight management: meta-analysis of randomized controlled trials. Crit Rev Food Sci Nutr 62(3):798–809. https://doi.org/10.1080/10408398.2020.1829539
Richter M, Baerlocher K, Bauer JM, Elmadfa I, Heseker H, Leschik-Bonnet E, Stangl G, Volkert D, Stehle P on behalf of the German Nutrition Society (2019) Revised Reference Values for the Intake of Protein. Ann Nutr Metab 74(3):242–250. https://doi.org/10.1159/000499374
Volkert D, Beck AM, Cederholm T, Cruz-Jentoft A, Goisser S, Hooper L, Kiesswetter E, Maggio M, Raynaud-Simon A, Sieber CC, Sobotka L, van Asselt D, Wirth R, Bischoff SC (2019) ESPEN guideline on clinical nutrition and hydration in geriatrics. Clin Nutr 38(1):10–47. https://doi.org/10.1016/j.clnu.2018.05.024
Westerterp-Plantenga MS, Lemmens SG, Westerterp KR (2012) Dietary protein - its role in satiety, energetics, weight loss and health. Br J Nutr 108(Suppl 2):S105-112. https://doi.org/10.1017/S0007114512002589
Westerterp-Plantenga MS (2020) Challenging energy balance—during sensitivity to food reward and modulatory factors implying a risk for overweight—during body weight management including dietary restraint and medium-high protein diets. Physiol Behav 221:112879. https://doi.org/10.1016/j.physbeh.2020.112879
Camara M, Giner RM, Gonzalez-Fandos E, Lopez-Garcia E, Manes J, Portillo MP, Rafecas M, Dominguez L, Martinez JA (2021) Food-based dietary guidelines around the world: a comparative analysis to update AESAN scientific committee dietary recommendations. Nutrients 13(9):3131. https://doi.org/10.3390/nu13093131
Alonso-Coello P, Schünemann HJ, Moberg J et al (2016) GRADE Evidence to Decision (EtD) frameworks: a systematic and transparent approach to making well informed healthcare choices. 1: Introduction. BMJ 353:i2016. https://doi.org/10.1136/bmj.i2016
Acknowledgements
The following scientists deserve special thanks for providing helpful remarks on the evidence-based guideline for protein intake: Jürgen M. Bauer, Heiner Boeing, Nicole Kalotai and Thomas Remer.
Funding
This research was funded by the German Federal Ministry of Food and Agriculture. The funder had no role in the decisions about data collection, analyses, interpretation of data, in the writing of the report nor in the decision to submit the article for publication.
Author information
Authors and Affiliations
Consortia
Contributions
AMA, JH, AL and AS conducted the literature search, study selection, data extraction and AMSTAR 2 and NutriGrade evaluations. SE and SEg evaluated the evidence and graded the overall certainty of evidence, which was finalised after discussion with all authors. SE, SEg, AMA and AS prepared the manuscript. HBF, AEB, AK, TK, SL, SLo, KN, MBS, LS, RS, GIS, DV, AZ and BW provided critical feedback for revision. All authors read and approved the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
A list of any possible conflicts of interest is provided in Supplementary Material 8.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ellinger, S., Amini, A.M., Haardt, J. et al. Protein intake and body weight, fat mass and waist circumference: an umbrella review of systematic reviews for the evidence-based guideline on protein intake of the German Nutrition Society. Eur J Nutr 63, 3–32 (2024). https://doi.org/10.1007/s00394-023-03220-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00394-023-03220-x