
Abstract
Background
The optimal treatment strategy for the surgical management of femur fractures and non-unions remains unknown. The aim of this study is to assess union rates, complications and outcome after femoral double plating. Treatment of shaft, distal, periprosthetic fractures and pathological proximal femur fractures as well as femoral non-unions with double plating were evaluated.
Methods
A systematic review according to the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) statement was conducted. Published literature reporting on the treatment and clinical outcome of femoral fractures and non-unions with double plating was identified. In total, 24 studies with 436 cases of double plating, 64 cases of single plating, 84 cases of intramedullary nailing (IM), and 1 interfragmentary screw treatment met the inclusion criteria of this systematic review. The evaluated literature was published between 1991 and 2020.
Results
Double plating of femoral fractures achieved high healing rates and few complications were reported. It displayed significantly less intraoperative haemorrhage, shorter surgery time reduced risk of malunion in polytraumatised patients when compared to IM. Fracture healing rate of double-plating distal femoral fractures was 88.0%. However, there were no significant differences regarding fracture healing, complication or functional outcome when compared to single plating. Treatment of periprosthetic fractures with double plating displayed high healing rates (88.5%). Double plating of non-unions achieved excellent osseous union rates (98.5%).
Conclusions
The literature provides evidence for superior outcomes when using double plating in distal femoral fractures, periprosthetic fractures and femoral non-unions. Some evidence suggests that the use of double plating of femoral fractures in polytraumatised patients may be beneficial over other types of fracture fixation.
Level of evidence
IV.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Double plating is performed by adding a second implant for fracture treatment increasing stability and providing advantages of fracture fixation in regions with high bending forces and intra-articular metaphyseal fractures [1]. Due to these biomechanical advantages, there are several indications for double plating of the femur including femoral fractures, pathological fractures of the proximal femur, periprosthetic femoral fractures and femoral non-unions [2,3,4].
In general, the treatment of femoral shaft fractures with intramedullary nailing (IM) or single-plate fixation can achieve high union rates [5]. However, some evidence in the literature shows a 24% rate of complications, including non-union, implant failure and infection [6]. Particularly in polytraumatised patients, plate fixation of the femoral shaft can provide a successful treatment option [7]. Plate fixation is recommended in patients with lung injuries unsuitable for IM [7, 8].
A further indication for double plating of the femur is distal femoral fractures. These injuries occur in young patients after high-energy or much more frequently in the older patients after low-energy trauma. Fractures of the distal femur account for 3–6% of all femoral fractures [9, 10]. Plating and IM are discussed in the literature as treatment options, with plating used predominating. Furthermore, biomechanical studies report better results with plating compared to other fixation methods [11]. A recent meta-analysis displayed a non-union rate of approximately 5% after fixation of distal femur fractures using a single locking compression plate or retrograde intramedullary nailing [12].
In addition, periprosthetic fractures of the femur can be treated successfully with double plating. Periprosthetic fractures following hip or knee arthroplasty are difficult to treat because they are associated with poor bone quality and distal fragments of insufficient length for adequate fixation [13].
Treatment options for pathological proximal femur fractures include intramedullary nailing (IM) [14], endoprosthetic reconstruction [15] and plating with and without augmentation of bone cement [16]. The compound osteosynthesis has been developed for these pathological fractures [17, 18]. The reconstruction of the proximal femur and fixation using a condylar plate together with an intramedullary placed narrow small fragment plate achieves a great amount of stability [17, 19] and is more stable compared to intramedullary nailing [18, 20, 21]. Furthermore, functional results of double plating are superior compared to primary endoprosthetic replacement [22].
Another indication for double plating of the femur is the treatment of non-unions. The overall rate of femoral non-union is approximately 14% [23]. Non-union of the femur can result from severe open fracture or segmental bone loss, infection or failure of the previous implants. Non-union in the lower extremities is associated with axial malalignment, loss of ambulatory function, decreased range of motion, chronic pain and reduced quality of life [24].
Given that fracture healing varies between diaphyseal and metaphyseal bone or pathological fractures and that accompanying injuries as well as comorbidities and injuries of the soft tissues between polytraumatised patients and the elderly patient suffering from periprosthetic fractures are different, the most important common denominator of this review are the surgical technique of double plating and the anatomical femoral region.
Endpoints of the present study were union rates and complication rates for double plating of femoral shaft fractures, distal femoral fractures, periprosthetic femoral fractures, pathological fractures of the proximal femur and femoral non-unions. When possible, comparison to other fixation procedures was to be performed. It was hypothesised that double plating of the femur for each indication mentioned above achieves high union rates with low complication rates and that double plating is a successful alternative compared to other fixation procedures.
Materials and methods
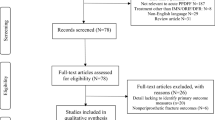
Electronic database was searched to identify all published literature addressing the treatment of fractures and non-unions of the femur. This study was conducted in accordance with the 2009 preferred reporting items for systematic review and meta-analysis (PRISMA) statement (Fig. 1) [25]. The search was performed using PubMed in November 2020. According to the predefined selection criteria, studies that had been published from the database inception until November 30, 2020 were searched using both MeSH (Medical Subject Headings) terms and keywords. The search terms were ”femoral fracture AND dual plating”, “femoral fracture AND double plating”, “fracture of the femur AND dual plating”, “fracture of the femur AND double plating”, “periprosthetic femoral fracture AND dual plating”, “periprosthetic femoral fracture AND double plating”, “periprosthetic fracture of the femur AND dual plating”, “periprosthetic fracture of the femur AND double plating”.

PRISMA flow chart showing the path from identification to inclusion of relevant literature
Two investigators independently reviewed the titles, abstracts and texts from all included articles. Selection for inclusion was determined by examining the title and abstract of all articles obtained from the search (Fig. 1). The citations in the included studies were manually checked to identify potentially eligible studies. Full-text articles were examined for review to allow further assessment of inclusion and exclusion criteria (Fig. 1).
A study was included when it (1) assessed the treatment of fractures or non-unions of the femur with two plates, with two plates compared to a single plate or compared to IM and (2) consisted of a cohort of seven or more patients. A study was excluded when it (1) consisted of a cohort of less than seven patients, (2) was basic science or editorial articles or surgical technique descriptions or (3) was an animal or biomechanical study. The present study was conducted with language limitation to English, French and German.
The retrieved studies were populated in Citavi (version 6 Swiss Academic Software and Citavi, Wädenswil, Switzerland,) and then exported to Microsoft software (Microsoft 365 Business Standard, Redmond, WA USA). Following the exclusion of duplicate results, the study selection was performed.
Two reviewers independently extracted the key information from the included studies comprising the names of the authors, year of publication, level of evidence, number of patients, treatment, mean follow-up, fracture healing, complications and functional outcome at final follow-up. Descriptive analysis was performed with Excel. The level of evidence was assigned according to the classification as specified by Wright et al. [26]. In addition, studies were evaluated according the Coleman methodology score (CMS) [27].
Results
A total of 24 studies, published between 1991 and 2020, met the inclusion criteria of this systematic review. Studies were level III or IV according to Wright et al. [26].
Femoral shaft fractures in polytraumatised patients
One study examined outcomes of double plating of femoral shaft fractures [8]. A second study compared outcomes of double plating versus IM [28]. In total, 141 patients and 141 femoral shaft fractures were included (Table 1). Double plating was performed in 57 cases and IM in 84 cases. The mean follow-up was 16.5 months. Fracture healing was achieved in 138 cases (97.9%). The mean healing time was 8.8 months. The study comparing IM and double plating reported significantly less intraoperative haemorrhage when double plating was used for fixation of femoral shaft fractures [28]. Furthermore, a significantly shorter surgery time and a significantly reduced risk for malunion was observed [28]. All 141 cases were polytraumatised patients [8] or patients with an Injury Severity Score (ISS) ≥ 18 [28]. The overall complication rate was 35% among the 141 patients. The complication rate of double plating was 28% (16 complications in 57 cases), while that of IM was 40% (34 complications in 84 cases) (Table 1). Pulmonary complications were observed in 26 cases of the IM group (31%) and in 10 cases of the double-plating group (18%). However, there were no significant differences between the IM and the double-plating groups regarding function scores, fracture union rate, overall pulmonary complication rate or in-hospitality mortality [28]. The mean Coleman methodology score was 48 (Table 2).
-
n = 1 delayed union (0.7%)
-
n = 1 superficial wound infection (0.7%)
-
n = 36 pulmonary complications (25.5%) (n = 26 IM group, n = 10 double-plating group)
-
n = 5 multiple organ failure (3.6%)
-
n = 7 mortality during hospitalisation (5.0%).
Distal femoral fracture
Six studies described outcomes of case series with double plating of distal femoral fractures [2, 29,30,31,32,33]. A total of 156 distal femoral fractures (AO [Arbeitsgemeinschaft für Osteosynthesefragen] 33 A–B and 33-C2 and 33-C3 fractures) were included (Table 3). Of these 156 cases, 108 distal femoral fractures were treated with double plating which achieved healing in 95 cases (88.0%). Bai et al. (2018) compared lateral plating in 48 cases and double plating in 12 cases of distal femoral fractures. No significant differences in the mean operation time, intraoperative haemorrhage or fracture-healing time were observed. Good to excellent knee function 1 year postoperatively was found [29]. While fracture healing was achieved in all cases in the double-plating group, there was one non-union in the single-plating group [29]. Summarising all 108 cases, the overall complication rate was 33.3%. The mean Coleman methodology score was 41.5 (Table 4).
-
n = 9 infection (8.3%)
-
n = 10 non-union (9.3%)
-
n = 2 mortality during hospitalisation (1.9%)
-
n = 3 mild pain at the iliac grafting donor site (2.8%)
-
n = 2 arthrolysis under general anaesthesia at 3 weeks after surgery because of a clear delay in rehabilitation response and fear of development of arthrofibrosis (1.9%)
-
n = 2 delayed tibial tuberosity osteotomy healing for more than 12 weeks (1.9%)
-
n = 2 delayed wound healing (1.9%)
-
n = 1 deep-vein thrombosis (0.9%)
-
n = 6 screw breakage or cut-out in one of the plate fixations with no loss of reduction (5.6%).
Periprosthetic femoral fracture
Five studies reported outcomes of case series with double plating of periprosthetic femoral fractures. Periprosthetic fractures around total hip and knee arthroplasty and femoral shaft were included [3, 34,35,36,37]. A total of 106 patients (109 cases) with 68 periprosthetic and 38 femur fractures, including 2 non-unions and 1 open fracture, were analysed (Table 5). Of these 109 cases, 96 cases were treated with double plating. The fractures contained type A3 and C3 fractures according to AO/OTA-classification. Very low supracondylar fractures and periprosthetic fractures around total hip and total knee arthroplasty (Vancouver classification B1 and C, Su et al. [38] Su2 and Su3) were included. Müller et al. [3] evaluated double plating of ten periprosthetic fracture cases following hip or knee arthroplasty: six periprosthetic fractures after total hip arthroplasty, three periprosthetic fractures after total knee arthroplasty and one interprosthetic fracture after total hip and knee arthroplasty. Seven patients were included in the final follow-up. Fracture healing was achieved in all cases [3]. The mean follow-up was 34.5 months (Table 5). Two patients passed away because of non-surgery related events before the follow-up [3]. Park et al. [36] analysed periprosthetic fractures around knee arthroplasty (Su type 3). Of 21 patients, 20 achieved union at an average of 14 weeks postoperatively and the mean Knee Society knee and function scores were 94 and 89.5 [36]. Bologna et al. [37] showed in their retrospective study that double plating of complex distal femoral fractures (AO/OTA 33-C2/33-C3) or periprosthetic fractures led to significantly higher union rates compared to single plating. It is to highlight that of 13 cases treated with single plating only, there were 6 non-unions and 4 delayed unions (76.9% impaired bone healing).
Overall, healing was achieved in 85 of 96 cases fractures treated with double plating (88.5%) [3, 34,35,36,37]. The complication rate was 21.9%. The mean Coleman methodology score was 46.2 (Table 6).
-
n = 1 non-union (1.0%)
-
n = 2 implant failure (2.1%)
-
n = 3 delayed union (3.1%)
-
n = 6 superficial wound infection (6.3%)
-
n = 1 reduction loss (1.0%)
-
n = 1 deep infection (1.0%)
-
n = 4 complication in soft tissue healing (4.2%)
-
n = 2 significant knee stiffness (2.1%)
-
n = 2 mild anterolateral heterotopic ossification (2.1%)
Pathological fractures of the proximal femur
Two studies analysed double-plate compound osteosynthesis for treatment of pathological fractures of the proximal femur (Table 7) [16, 18]. Merckaert et al. [18] reported that double-plate compound osteosynthesis is superior compared to other fixation techniques. Comparing the double-plate compound osteosynthesis and the single-plate compound osteosynthesis Kinkel et al. [16] showed that the double-plate technique is more stable and associated with a higher survival probability after 5 years. The mean Coleman methodology score was 49 (Table 8).
Non-union of the femur
Nine studies reported outcomes of case series with double plating of femoral non-unions including the proximal femur, femoral shaft and distal femur [4, 24, 39,40,41,42,43,44,45]. Pydisetty et al. [42] analysed 10 patients with revision surgery for non-union of bisphosphonate-related subtrochanteric fractures. After removal of failed implants and resection of the non-union, bone grafting and double plating with a lateral dynamic compression screw (DCS) plate and anterior locking compression plate were performed achieving bone union in all the cases. However, one patient was lost to follow-up and complication rate was high in these complex fracture patterns [42]. Both, Lu et al. [43] and Mardani-Kivi et al. [44] reported that double plating and bone grafting achieved a healing rate of 100% for the treatment of atrophic distal femur non-union with bone defect and non-union of femoral supracondylar, subtrochanteric, and shaft fractures, respectively. There were no differences between double plating, single plate and interfragmentary screw in the only study comparing different fixation techniques [39]. A total of 193 non-unions were included (Table 9). Fracture healing was achieved in 190 cases (98.5%). Reported postoperative complications occurred with an overall rate of 25.9%. The mean Coleman methodology score was 44.2 (Table 10).
-
n = 4 infection (2.1%)
-
n = 1 sacral sore (0.5%)
-
n = 2 postoperative seroma (1.0%)
-
n = 4 blood transfusion (2.1%)
-
n = 1 HDU admission (0.5%)
-
n = 1 periprosthetic fracture (0.5%)
-
n = 2 fatigue failure (1.0%)
-
n = 1 malunion (0.5%)
-
n = 1 persistent non-union (0.5%)
-
n = 1 loss of motion of one knee (0.5%)
-
n = 12 movement limitation (6.2%)
-
n = 9 muscle atrophy (4.7%)
-
n = 2 failure of attachment of the greater trochanter (1.0%)
-
n = 7 symptomatic hardware (3.6%)
-
n = 1 breakdown of the posterior iliac crest harvest site (0.5%)
-
n = 1 deep-vein thrombosis (0.5%)
-
n = 1 pulmonary embolism (0.5%).
Discussion
The most important observations of this systematic review were (1) that double plating displayed significantly less intraoperative haemorrhage, a significantly shorter surgery time and a significantly reduced risk for malunion compared to IM in polytraumatised patients and thus it is reported to be a successful alternative to nailing, (2) that double plating of distal femoral fractures achieved very high healing rates (88.0%) with a reported overall complication rate (33.3%), (3) that double plating of periprosthetic femoral fractures displayed very high healing rates (88.5%) with a moderate overall complication rate of 21.9% and (4) that the treatment of femoral non-union with double plating achieved excellent osseous union rates (98.5%) with a reported overall complication rate of 25.9%.
Application of an external fixator in femoral fractures showed non-union rates of 0–12% [46]. Plate fixation of femoral fractures displayed non-union rates ranging from 1.6 to 8% [47,48,49]. The results of the present systematic review showed a 97.9% fracture-healing rate after double plating of femoral shaft fractures in polytraumatised patients. Moreover, better surgical parameters were observed. These findings might lead to an increase in the clinical use of double plating for the treatment of femoral shaft fractures in polytraumatised patients. Further studies are necessary to evaluate the possible benefits. According to current literature, treating femoral shaft fractures in polytraumatised patients with double plating is superior to IM.
Distal femur fractures occur in older patients after low-energy trauma and result from high-energy trauma in younger patients causing comminution, unstable fractures and bone loss [31]. Due to poor bone quality, treatment of distal femur fractures in older patients is difficult. Limitations of treatment with the condylar blade plate and supracondylar nailing are the reduction of the articular surface and fixation [31]. Furthermore, there is a high incidence of loss of fixation and varus collapse [2, 10]. Double plating of distal shaft fractures in other anatomical regions like the distal humerus is already a standard procedure [1]. According to biomechanical studies, a parallel arrangement of the plates appears to be best, however, there is no evidence for the optimal arrangement in clinical data [1]. In the examined case series, fracture healing was achieved in almost all patients treated with double plating, which might be advantageous over other fixation types. Compared to the results of the meta-analysis of Yoon et al. [12] showing a non-union rate of 5% after single-plate fixation or retrograde intramedullary nailing the results of the present study provide that double plating is a surgical treatment option. This systematic review shows that there is a lack of clinical studies comparing single versus double plating and other fixation techniques. According to the current literature examining double plating of the lower extremity, further clinical studies examining the best treatment options for the elderly patients are necessary.
Surgical treatment of periprosthetic fractures of the femur is challenging. Current literature reports high union rates (88.5%) of double plating of distal femoral and periprosthetic fractures following hip or knee arthroplasty. Considering the high mean age of 76.2 years of the patients, double plating is a valid treatment option. The present study reveals that double plating of periprosthetic fractures leads to a moderate rate of complications [3, 34]. Furthermore, double locking plating of osteoporotic periprosthetic supracondylar femur fractures resulted in reduction of complication rates, reduction loss and implant failure and allows early mobilisation and rehabilitation and earlier weight bearing [35]. However, currently there are predominantly level IV studies in the literature. One retrospective level III study showed significant better results for double plating compared to single plating [37]. In comparison to other fixation techniques, more clinical data are necessary to further evaluate the benefit of double plating of periprosthetic fractures. The potential advantages of full weight bearing after double plating and thus preventing complications, including pneumonia and thrombosis, needs further evaluation.
It is reported that using the double-plate compound osteosynthesis superior biomechanical characteristics and a higher survival probability can be achieved. However, due to a lack of consistency of reporting in the literature, more clinical data are necessary to underline the possible advantages of double plating for these fracture patterns.
Non-unions of the femur occur after open fractures and metaphyseal comminution [50]. The present systematic review shows union rates of 98.5% using double plating and bone grafting for the treatment of femoral shaft non-unions. Therefore, double plating for the treatment of femoral shaft union is a viable treatment option.
Supracondylar non-unions are serious complications and there is no treatment standard [39, 51]. The present study shows that a high proportion of patients with distal femoral non-unions can be treated successfully with double plating and autogenous bone grafting. Moreover, compared to other studies, the use of dual plating and bone grafting for the treatment of supracondylar femoral non-unions can achieve higher healing rates [24, 39, 52].
Stabilisation of the greater trochanter in the revision of total hip arthroplasty is a major challenge. Non-union rates using multibraided metallic cables range from 20 to 31% [40, 53, 54]. Operative techniques for the reattachment of the greater trochanter are cable fixation, single-plate devices and dual plating [40]. Current literature shows that double plating leads to considerably higher union rates than other fixation techniques [55,56,57]. According to current literature, a 100% union rate can be achieved when the trochanter is attached to the femur with good contact and double plating [40]. Superior results when performing double plating of non-union of the greater trochanter need to be confirmed. Current literature shows that double plating might be superior.
A limitation of the present study is that the included studies—with one exception being level III evidence based—are level IV evidence based and that the overall mean Coleman methodology score was only 45.8. Major areas of methodological deficiencies were study size and type of study [27]. There is a need for more prospective clinical studies comparing double plating to other fixation techniques with greater study sizes. Whereas there was consistency in the literature regarding the definition of bone union, the reported complication rates vary in part substantially due to the different study designs.
Regarding the endpoints of the present study double plating of femoral shaft fractures, distal femoral fractures, periprosthetic femoral fractures, pathological fractures of the proximal femur and femoral non-unions achieves high union rates with moderate complication rates. The hypothesis that double plating of femoral fractures and non-unions can achieve high union rates with low complication rates is confirmed. The hypothesis that double plating of femoral fractures and non-unions can provide a successful alternative to other fixation procedures is also supported by the findings of the present systematic review.
Conclusions
The current literature contains evidence for high healing rates and superior outcomes when using double plating in distal femoral fractures, periprosthetic fractures and femoral non-unions. Some evidence suggests that the use of double plating of femoral fractures in polytraumatised patients may be beneficial over other types of fracture fixation.
References
Katthagen JC, Schliemann B, Michel PA, Heilmann LF, Dyrna F, Raschke MJ (2020) Clinical application and outcomes of upper extremity double plating. Zeitschrift fur Orthopadie und Unfallchirurgie 158:227–237
Sanders R, Swiontkowski M, Rosen H, Helfet D (1991) Double-plating of comminuted, unstable fractures of the distal part of the femur. J Bone Jt Surg Am Vol 73:341–346
Müller FJ, Galler M, Füchtmeier B (2014) Clinical and radiological results of patients treated with orthogonal double plating for periprosthetic femoral fractures. Int Orthop 38:2469–2472
Maimaitiyiming A, Amat A, Rehei A, Tusongjiang M, Li C (2015) Treatment of the femoral shaft nonunion with double plate fixation and bone grafting: a case series of 14 patients. Injury 46:1102–1107
Winquist RA, Hansen ST, Clawson DK (1984) Closed intramedullary nailing of femoral fractures. A report of five hundred and twenty cases. J Bone Jt Surg Am Vol 66:529–539
Loomer RL, Meek R, de Sommer F (1980) Plating of femoral shaft fractures: the vancouver experience. J Trauma 20:1038–1042
Apivatthakakul T, Chiewcharntanakit S (2009) Minimally invasive plate osteosynthesis (MIPO) in the treatment of the femoral shaft fracture where intramedullary nailing is not indicated. Int Orthop 33:1119–1126
Cheng T, Xia R, Yan X, Luo C (2018) Double-plating fixation of comminuted femoral shaft fractures with concomitant thoracic trauma. J Int Med Res 46:440–447
Court-Brown CM, Caesar B (2006) Epidemiology of adult fractures: a review. Injury 37:691–697
Gwathmey FW, Jones-Quaidoo SM, Kahler D, Hurwitz S, Cui Q (2010) Distal femoral fractures: current concepts. J Am Acad Orthop Surg 18:597–607
Ehlinger M, Ducrot G, Adam P, Bonnomet F (2013) Distal femur fractures. Surgical techniques and a review of the literature. Orthop Traumatol Surg Res OTSR 99:353–360
Yoon B-H, Park IK, Kim Y, Oh H-K, Choo SK, Sung Y-B (2020) Incidence of nonunion after surgery of distal femoral fractures using contemporary fixation device: a meta-analysis. Arch Orthop Trauma Surg
Meneghini RM, Keyes BJ, Reddy KK, Maar DC (2014) Modern retrograde intramedullary nails versus periarticular locked plates for supracondylar femur fractures after total knee arthroplasty. J Arthroplast 29:1478–1481
Tanaka T, Imanishi J, Charoenlap C, Choong PFM (2016) Intramedullary nailing has sufficient durability for metastatic femoral fractures. World J Surg Oncol 14:80
Lane JM, Sculco TP, Zolan S (1980) Treatment of pathological fractures of the hip by endoprosthetic replacement. J Bone Jt Surg Am Vol 62:954–959
Kinkel S, Stecher J, Gotterbarm T, Bruckner T, Holz U (2009) Compound osteosynthesis for osteolyses and pathological fractures of the proximal femur. Orthopedics 32:403
Friedl W (1992) Die Doppelplattenverbundosteosynthese. Ein Verfahren zur primär belastungsstabilen Versorgung von Problemverletzungen des subtrochanteren bis suprakondylären Femurbereiches. Aktuelle Traumatologie 22:189–196
Merckaert SR, Fontanellaz-Castiglione CD, Fornari ED, Tannast M (2020) Double-plate compound osteosynthesis for pathological fractures of the proximal femur: high survivorship and low complication rate. Arch Orthop Trauma Surg 140:1327–1338
Ganz R, Isler B, Mast J (1984) Internal fixation technique in pathological fractures of the extremities. Arch Orthop Trauma Surg 103:73–80
Friedl W, Ruf W, Mischkowsky T (1986) Die Doppelplattenverbundosteosynthese bei subtrochanteren pathologischen Frakturen. Eine klinische und experimentelle Untersuchung. Der Chirurg; Zeitschrift fur alle Gebiete der operativen Medizen. 57:713–718
Schöttle H, Sauer HD, Jungbluth KH (1977) Stabilitätsmessungen bei Osteosynthesen am proximalen Femur. Archiv fur orthopadische und Unfall-Chirurgie 89:87–100
Rompe JD, Eysel P, Hopf C, Heine J (1994) Metastatic instability at the proximal end of the femur. Comparison of endoprosthetic replacement and plate osteosynthesis. Arch Orthop Trauma Surg 113:260–264
Zura R, Xiong Z, Einhorn T, Watson JT, Ostrum RF, Prayson MJ, Della Rocca GJ, Mehta S, McKinley T, Wang Z et al (2016) Epidemiology of fracture nonunion in 18 human bones. JAMA Surg 151:e162775
Holzman MA, Hanus BD, Munz JW, O’Connor DP, Brinker MR (2016) Addition of a medial locking plate to an in situ lateral locking plate results in healing of distal femoral nonunions. Clin Orthop Relat Res 474:1498–1505
Moher D, Liberati A, Tetzlaff J, Altman DG (2010) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int J Surg (Lond, Engl) 8:336–341
Wright JG, Swiontkowski MF, Heckman JD (2003) Introducing levels of evidence to the journal. J Bone Jt Surg Am 85:1–3
Coleman BD, Khan KM, Maffulli N, Cook JL, Wark JD (2000) Studies of surgical outcome after patellar tendinopathy: clinical significance of methodological deficiencies and guidelines for future studies. Victorian Institute of Sport Tendon Study Group. Scand J Med Sci Sports 10:2–11
Cheng T, Xia R-G, Dong S-K, Yan X-Y, Luo C-F (2019) Interlocking intramedullary nailing versus locked dual-plating fixation for femoral shaft fractures in patients with multiple injuries: a retrospective comparative study. J Invest Surg Off J Acad Surg Res 32:245–254
Bai Z, Gao S, Hu Z, Liang A (2018) Comparison of clinical efficacy of lateral and lateral and medial double-plating fixation of distal femoral fractures. Sci Rep 8:4863
Imam MA, Torieh A, Matthana A (2018) Double plating of intra-articular multifragmentary C3-type distal femoral fractures through the anterior approach. Eur J Orthop Surg Traumatol Orthop Traumatol 28:121–130
Khalil AE-S, Ayoub MA (2012) Highly unstable complex C3-type distal femur fracture: can double plating via a modified Olerud extensile approach be a standby solution? J Orthop Traumatol Off J Italian Soc Orthop Traumatol 13:179–188
Ziran BH, Rohde RH, Wharton AR (2002) Lateral and anterior plating of intra-articular distal femoral fractures treated via an anterior approach. Int Orthop 26:370–373
Metwaly RG, Zakaria ZM (2018) Single-incision double-plating approach in the management of isolated, closed osteoporotic distal femoral fractures. Geriatr Orthop Surg Rehabil 9:2151459318799856
Steinberg EL, Elis J, Steinberg Y, Salai M, Ben-Tov T (2017) A double-plating approach to distal femur fracture: a clinical study. Injury 48:2260–2265
Çiçek H, Tuhanioğlu Ü, Oğur HU, Seyfettinoğlu F, Bozkurt M (2018) An alternative treatment for osteoporotic Su Type III periprosthetic supracondylar femur fractures: double locking plate fixation. Acta orthopaedica et traumatologica turcica 52:92–96
Park K-H, Oh C-W, Park K-C, Kim J-W, Oh J-K, Kyung H-S, Kim H-J, Yoon Y-C (2020) Excellent outcomes after double-locked plating in very low periprosthetic distal femoral fractures. Arch Orthop Trauma Surg
Bologna MG, Claudio MG, Shields KJ, Katz C, Salopek T, Westrick ER (2020) Dual plate fixation results in improved union rates in comminuted distal femur fractures compared to single plate fixation. J Orthop 18:76–79
Su ET, DeWal H, Di Cesare PE (2004) Periprosthetic femoral fractures above total knee replacements. Am Acad Orthop Surg 12:12–20
Chapman MW, Finkemeier CG (1999) Treatment of supracondylar nonunions of the femur with plate fixation and bone graft. J Bone Jt Surg Am Vol 81:1217–1228
Laflamme GY, Leduc S, Petit Y (2012) Reattachment of complex femoral greater trochanteric nonunions with dual locking plates. J Arthroplast 27:638–642
Peng Y, Ji X, Zhang L, Tang P (2016) Double locking plate fixation for femoral shaft nonunion. Eur J Orthop Surg Traumatol Orthop Traumatol 26:501–507
Nagy MT, Pydisetty G, Kwaees TA, Saldanha K (2020) Outcome of revision surgery for bisphosphonate related subtrochanteric fracture non-union following failed intramedullary nailing. Injury
Lu J, Guo S-C, Wang Q-Y, Sheng J-G, Tao S-C (2020) J-bone graft with double locking plate: a symphony of mechanics and biology for atrophic distal femoral non-union with bone defect. J Orthop Surg Res 15:144
Mardani-Kivi M, Karimi Mobarakeh M, Keyhani S, Azari Z (2020) Double-plate fixation together with bridging bone grafting in nonunion of femoral supracondylar, subtrochanteric, and shaft fractures is an effective technique. Musculoskelet Surg 104:215–226
Sun L, Li Z, Ma T, Xue H-Z, Wang Q, Lu D-G, Lu Y, Ren C, Li M, Zhang K (2019) Treatment of atrophic nonunion via autogenous ilium grafting assisted by vertical fixation of double plates: a case series of patients. J Int Med Res 47:1998–2010
Alonso J, Geissler W, Hughes JL (1989) External fixation of femoral fractures. Indications and limitations. Clin Orthop Relat Res 1989:83–88
Geissler WB, Powell TE, Blickenstaff KR, Savoie FH (1995) Compression plating of acute femoral shaft fractures. Orthopedics 18:655–660
Rüedi TP, Lüscher JN (1979) Results after internal fixation of comminuted fractures of the femoral shaft with DC plates. Clin Orthop Relat Res 1979:74–76
Riemer BL, Butterfield SL, Burke CJ, Mathews D (1992) Immediate plate fixation of highly comminuted femoral diaphyseal fractures in blunt polytrauma patients. Orthopedics 15:907–916
Ebraheim NA, Martin A, Sochacki KR, Liu J (2013) Nonunion of distal femoral fractures: a systematic review. Orthop Surg 5:46–50
Chan DB, Jeffcoat DM, Lorich DG, Helfet DL (2010) Nonunions around the knee joint. Int Orthop 34:271–281
Moore TJ, Watson T, Green SA, Garland DE, Chandler RW (1987) Complications of surgically treated supracondylar fractures of the femur. J Trauma 27:402–406
Barrack RL, Butler RA (2005) Current status of trochanteric reattachment in complex total hip arthroplasty. Clin Orthop Relat Res 441:237–242
Takahira N, Itoman M, Uchiyama K, Takasaki S, Fukushima K (2010) Reattachment of the greater trochanter in total hip arthroplasty: the pin-sleeve system compared with the Dall-Miles cable grip system. Int Orthop 34:793–797
Koyama K, Higuchi F, Kubo M, Okawa T, Inoue A (2001) Reattachment of the greater trochanter using the Dall-Miles cable grip system in revision hip arthroplasty. J Orthop Sci Off J Japn Orthop Assoc 6:22–27
Ritter MA, Eizember LE, Keating EM, Faris PM (1991) Trochanteric fixation by cable grip in hip replacement. J Bone Jt Surg Br Vol 73:580–581
Hamadouche M, Zniber B, Dumaine V, Kerboull M, Courpied JP (2003) Reattachment of the ununited greater trochanter following total hip arthroplasty. The use of a trochanteric claw plate. J Bone Jt Surg Am Vol 85:1330–1337
Acknowledgements
The authors thank Dr. Robert Blakytny (MA, DPhil, Oxford) for his language editing. The authors maintained complete control over the direction and content of the manuscript.
Funding
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
The idea for the article was conceived by Katthagen JC. All the authors contributed to the study conception and design. Conceptualization: JCK, MFL, MJR, JSS, JE, and SR. Methodology: JCK, MFL, JSS, JE, and SR. Literature search and data analysis were performed by MFL and JCK. The first draft of the manuscript was written by MFL, and all the authors commented on previous versions of the manuscripts. Writing—original draft preparation: MFL. Writing—review and editing: JCK, JSS, JE, SR, and MJR. Supervision: JCR and MJR. All the authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no known competing financial interests, non-financial interests or personal relationships that could have appeared to influence the work reported in this paper. The authors did not receive support from any organisation for the submitted work. No funding was received to assist with the preparation of this manuscript. No funding was received for conducting this study. No funds, grants, or other support was received. The authors have no relevant financial or non-financial interests to disclose. The authors have no conflicts of interest to declare that are relevant to the content of this article. All the authors certify that they have no affiliations with or involvement in any organisation or entity with any financial interest or non-financial interest in the subject matter or materials discussed in this manuscript. The authors have no financial or proprietary interests in any material discussed in this article.
Ethical approval
This is an observational study. No ethical approval is required.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Lodde, M.F., Raschke, M.J., Stolberg-Stolberg, J. et al. Union rates and functional outcome of double plating of the femur: systematic review of the literature. Arch Orthop Trauma Surg 142, 1009–1030 (2022). https://doi.org/10.1007/s00402-021-03767-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-021-03767-6