
Abstract
Motor abnormalities occur in the majority of persons with schizophrenia but are generally neglected in clinical care. Psychiatric diagnostics fail to include quantifiable motor variables and few assessment tools examine full-body movement. We assessed full-body movement during gait of 20 patients and 20 controls with motion capture technology, symptom load (PANSS, BPRS) and Neurological Soft Signs (NSS). In a data-driven analysis, participants’ motion patterns were quantified and compared between groups. Resulting movement markers (MM) were correlated with the clinical assessment. We identified 16 quantifiable MM of schizophrenia. While walking, patients and controls display significant differences in movement patterns related to posture, velocity, regularity of gait as well as sway, flexibility and integration of body parts. Specifically, the adjustment of body sides, limbs and movement direction were affected. The MM remain significant when controlling for medication load. They are systematically related to NSS. Results add assessment tools, analysis methods as well as theory-independent MM to the growing body of research on motor abnormalities in schizophrenia.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Genuine motor abnormalities (GMA) can be observed in up to 80% of all patients with schizophrenia and in 66% of first-episode, antipsychotic-naive patients [1,2,3,4,5]. To a lesser degree, they have been observed in individuals considered at ultra-high risk (UHR) and in unaffected first-degree relatives with a genetic risk for schizophrenia [3, 6, 7]. Some researchers accordingly consider GMA a prognostic biomarker for neurodevelopmental alterations contributing to a vulnerability to the illness [3, 8]. However, acquiring a comprehensive overview of GMA related to schizophrenia is difficult. Descriptions and categorizations vary largely with the conceptual framework and the assessment means of the respective researchers [3, 9,10,11,12]. Hirjak et al. [3] for example, categorize four groups of GMA: (a) neurological soft signs (NSS)—externally observable impairments in sensory integration, motor coordination, balance, and sequencing of complex motor acts [1, 13], (b) hyperkinetic abnormal involuntary movements (AIMS), such as dyskinesia, dystonia, akathisia or hyperkinesia, (c) hypokinetic AIMS, such as spontaneous parkinsonism, and (4) catatonic phenomena, which can present as a hyperkinetic (e.g. mannerisms, stereotypy) or a hypokinetic (e.g. stupor, rigidity, immobility) movement disorder.
Pavlidou and Walter [9] in turn, name six distinct categories of GMA: (a) Dyskinesia—AIMS, (b) parkinsonism (c) akathisia—including restlessness and inner tension, (d) NSS (e) catatonia, and (f) psychomotor slowing, affecting fine and gross movements, such as writing or walking. The lack of conceptual clarity also applies to GMA rating scales which, additionally, rely on raters’ subjective observation. They are thus prone to observer bias, depend on rater training for accuracy and are not designed to detect subclinical abnormalities [4, 6, 14,15,16,17,18,19].
The most established neurobiological findings on GMA originate from studies on NSS [3, 10, 20]. Besides being a sign for the risk of developing schizophrenia (trait factors), they can be used to monitor disease progression (state factors) [20, 21]. They are not only related to psychopathological symptoms of schizophrenia [22] but also to poor cognitive and social functioning of patients. Cuesta and colleagues found strong associations of NSS with impaired performance in attention tasks, speed of processing, verbal and visual memory in first-episode patients [23, 24]. The most frequently reported NSS category in patients with schizophrenia is motor incoordination, comprising the inability to perform rapid alternating movements and difficulties in simple coordination tasks, such as the tandem walk or finger-nose tapping [25,26,27]. Impaired motor or interlimb coordination has been found to discriminate best between high-risk children and controls, and between patients with schizophrenia or a mood disorder [26, 27].
Recently formed task forces, such as the European collaboration on movement and sensorimotor/psychomotor functioning in schizophrenia and other psychoses (ECSP), attempt a consensus on GMA definitions and underline the great advantages (e.g. sensitivity, linearly related results) of an increased implementation of instrumental assessment [6, 19]. Additionally, researchers from different academic backgrounds have begun experimenting with modern technology to create innovative paradigms for the systematic assessment of GMA in schizophrenia. They include accelerometers in smartphones to study tremor, pressure sensitive foot switches for step analysis, or actigraphy to assess restlessness and overall activity of individuals [28,29,30,31,32,33,34,35,36,37,38,39]. Despite disturbances in interlimb and motor coordination being one of the motor symptoms most specific to schizophrenia, most studies focus on fine motor performance or movement of the upper limbs [10, 39]. Very few studies examine full-body movement, and if they do, they analyze highly reduced (stride length, cadence) or very broad (overall activity) variables [39,40,41]. The most detailed assessment of human motion has been done with motion capture (MoCap) technologies [42], showing that the mere movement qualities of anonymized walkers (abstracted to point-light displays) reveal information about their gender, age and affective state [43,44,45,46,47]. To our knowledge, within the psychiatric context full-body MoCap has only been applied in one study to analyze movement patterns with relevance to diagnostics: Michalak et al. [48] compared gait patterns of patients with depression to controls and found a reduced walking speed, arm swing, vertical movement, a slumped posture of the upper body, and an increased lateral sway in patients. Effect sizes ranged between d = 0.8 and 1.3.
Taken together, despite various instrumental attempts to quantify GMA [18, 28,29,30,31,32,33,34,35,36,37,38,39], current diagnostics fail to systematically include the objective evaluation of subtle and overt motor behavior [10]. Available assessment means do not analyze detailed full-body movement or interlimb coordination. Hence, with our study, we aimed at
-
(a)
piloting an assessment protocol, which allows for a detailed, three-dimensional, full-body gait analysis, and
-
(b)
defining theory-independent full-body movement markers (MM) for schizophrenia.
To navigate around the lack of conceptual clarity regarding GMA and to facilitate a truly objective assessment, we chose a data-driven approach for the first step, and only in the second step related its results to existing symptom definitions. We are not aware of any other study on schizophrenia applying such an approach. The following hypotheses were addressed:
H1 The mere MoCap data will reveal significantly different movement characteristics for patients and controls, from which full-body Movement Markers (MM) can be extracted by controlling for confounding variables (medication load, weight).
H2 Full-body MM are similar to but expand the movement characteristics of individuals with depression found by Michalak et al. [48].
H3 Particularly interlimb coordination is affected.
H4 Pronounced MM are associated with pronounced NSS (especially subscale motor coordination, and sensory integration).
H5 Patients with pronounced negative symptoms display pronounced MM.
Methods
The study was conducted as part of the collaborative research project “Schizophrenia and the Moving Body” [Center for Psychosocial Medicine (CPM), Heidelberg Center for Motion Research (HCMR), BioMotionLab]. It was embedded in a series of studies on movement of individuals with schizophrenia and conducted in accordance with the declaration of Helsinki [49]. The ethics committee of Heidelberg University’s Medical Faculty approved the study before recruitment start.
Recruitment procedure
Participants with a diagnosis of schizophrenia were consecutively (2019–2020) recruited from one of four wards (three in-patient, one out-patient ward) of the CPM. Included patients were (1) able to consent, (2) between 18 and 60 years old, (3) diagnosed with a schizophrenia spectrum disorder (ICD-10: F20.0-F20.9) prior to study inclusion by senior psychiatrists unrelated to the study and (4) stable on antipsychotic medication for at least 2 weeks. Exclusion criteria were: (1) acute psychosis (ICD-10: F23), (2) diagnosis with a catatonic or schizoaffective subtype (ICD-10: F20.2, F25.0-F25.9), (3) history of brain trauma, neurological or internal diseases, heavy fractions or prostheses (4) visible tremor, (5) strong visual impairment (6) alcohol/substance abuse or dependency within the past 12 months or a substance-induced psychosis (ICD-10: F19.5), (7) an IQ < 70, (8) an SAS score above 4, (9) pronounced language barriers. Controls were recruited through postings and the University’s website. Exclusion criteria resembled the patients’ ones with one addition: history of psychosis or schizophrenia, personal or in first-degree relatives. All participants gave informed consent prior to participation, were clinically assessed at the CPM and then motion captured at HCMR. A priori power analyses (g*power) suggested a total sample size between 23 and 55 for the detection of medium to large effects (d = 0.5–0.8), when assuming an alpha-level of p < 0.05. Because previous studies [48] found large effect sizes, we targeted a sample size of at least 40 participants.
Clinical assessment
Patients were assessed with the Positive and Negative Syndrome Scale (PANSS) [50], the Heidelberger NSS Scale [17], the Brief Psychiatric Rating Scale (BPRS) [51], and the Simpson-Angus Scale (SAS) [52, 53] (parkinsonoid). Controls were assessed with the Heidelberger NSS Scale.
Movement assessment
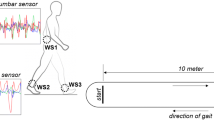
Lab equipment and functionality were explained to prevent psychotic triggers. A set of 49 infrared-reflective markers was attached to the participants skin and skintight sportswear (see C-Motion [54] for the detailed marker set). 8 Oqus500 cameras (Qualisys, Goeteborg, Sweden) tracked participants’ movements. An additional fixed video camera filmed the experiment. Participants were requested to walk back and forth on a path (7 m × 0.70 m) marked with white tape. They performed a series of other movement, balance and coordination tasks (details and results are discussed elsewhere). Walking was chosen, because it is a habituated full-body movement not requiring much cognitive attention but a complex interplay of sensory, motor and balance processes, and a fine-tuning of all limbs. To ensure a natural, “un-performed” walk, participants were asked to walk for a while to “find their most comfortable speed” (at least 3 min) before the actual recording began without further notice. At least 50 steps (8 times through the MoCap volume) were recorded.
Data analysis
Data were first analyzed algorithm-driven and then following a one-factorial, controlled between-group design. We performed three steps of analyis using different software for the various types of data: (1) By matching the groups for certain characteristics, we aimed at minimizing the influence of confounding variables (see Sect. 2.2.1). (2) We then quantified all visible group differences in movement (movement features, see Sect. 2.2.2), and (3) finally defined movement markers for schizophrenia from the pool of movement features (see Sect. 2.2.3).
Step 1: Sample characteristics and propensity score matching
Sample characteristics were analyzed and groups matched in R (Version 4.0.2) [55]. Daily medication load was converted into olanzapine equivalents (OPZ) following the classical mean dose method by Leucht and colleagues [56]. To match an equal-sized subgroup of controls to the available patients, we performed propensity score matching with five variables inherently correlated with gait: (a) gender, (b) age, (c) height, (d) weight, (e) BMI. We chose logistic regression for the estimation of propensity scores and created a matched sample using the one-to-one approach [57,58,59]. Except for the variable gender (exact matching), we chose nearest-neighbor matching. Matching was successful in reducing covariate imbalance for all variables except weight and, consequently, BMI. Hence, we based all further analysis on the matched and reduced sample and controlled for weight within the data-based exploration of movement patterns and the auxiliary analysis. See the supplementary material for details on matching.
Step 2: Data-driven analysis of movement patterns (movement features)
The MoCap data were analyzed with Qualisys Track Manager (Version 2018) and Matlab (Version R2020a). To avoid artifacts in the motion data, first and last centimeters of the walks were excluded from the analysis. For the quantification of movement features, we followed Troje’s [44, 60] computational framework. Due to space limitations, we can only give an overview of the algorithm. See [44] for a detailed description of the single computational steps. First, we computed the locations of 15 joint centers from the 49 marker trajectories. See Fig. 1 for a visualization of the joint center locations and [61,62,63,64] for the definition of the bone landmarks. With the help of Fourier Decomposition (FD), the joint center locations were linearized and redundancy was reduced.

Visualization of the joint centers (JC). They are located at the center of the head (HEDO), the sternum (TRXO), the shoulders (LSJC, RSJC), elbows (LEJC, REJC), wrists (LWJC, RWJC), the center of the pelvis (BMLPEL), hips (LHJC, RHJC), knees (LKJC, RKJC), and the ankles (LAJC, RAJC). The figure displays a film still of the average walker, derived from the entire sample. It can be viewed from the front (left picture) and rotated along all three axes (right picture). It is the basis for the discriminant walker, which is visualized as increments of the average walker. Axes: x = walking direction, y = lateral direction, z = vertical direction
We then computed a principal component analysis (PCA) across all Fourier-decomposed walkers to reduce dimensionality of the linear walker space [44, 47] (ten principal components, see [44, p. 10] for the decision on the amount of components of the PCA). To create linear classifiers, we computed a linear discriminant function (LDF), regressing the class indicator (patients, controls) on the walkers’ projections in the low-dimensional Eigenwalker space. To account for group differences in weight, we repeated the LDF computation, regressing the weight on the Eigenwalkers. By multiplying the second LDF (weight) with the transpose of the original LDF (patients, controls), we extracted components that can be explained by weight differences. We subtracted those components from the original LDF. Using the coefficients of the rectified LDF and the Eigenwalkers of the PCA, we created a discriminant walker (DW), an animated visualization of the set of movement patterns that the LDF extracted as classifiers [44]: see https://www.biomotionlab.ca/martin2022/. LDF classifiers, however, remain on data-level, meaning they essentially refer to moving dots in space. To quantify visible movement features, which could be compared statistically, amplitudes and visualizations of the DW were repeatedly examined and rated by different members of the research team. Visible differences were gathered, categorized and computed for each participant on the basis of the FD data for one gait cycle. We aimed at a comprehensive mathematical description of the groups’ dynamic, full-body movement differences (no structural differences: e.g. body size or hip width). Hence, for some movement differences, we propose multiple quantification options (movement features), which either follow Troje or Michalak [44, 48, 65] by capturing body parts’ amount of movement in space, or biomechanical recommendations, by quantifying the extent of motion in a respective joint (“Utilized Range of Motion” (URM)). See Table 1 in the supplementary material for computational details on all movement features.
Step 3: Determination of movement markers (MM) and correlations with clinical scales
Group comparisons of movement features and correlations were computed with IBM SPSS (Version 27.0.0.0). To determine MM for schizophrenia, all movement features were tested for significance. First, we computed t tests (two-sided, independent groups). We applied Bonferroni correction (p < 0.0003 = 0.05/154) for multiple testing but due to the explorative nature of our study also acknowledged initially significant variables not withstanding the correction. We again controlled for the weight of participants in an ANCOVA. In an auxiliary analysis, we assessed the influence of the medication load, by (a) correlating significant movement features with OPZ, and (b) splitting the patient group into a high and low dosage group and comparing significant movement features with second t tests. Movement features which proved significant in the main t tests and the ANCOVA and non-significant in the auxiliary analysis were defined as MM. Furthermore, we chose movement features which could be summarized for both body sides. Finally, we correlated the defined MM with the clinical scales PANSS, BPRS and NSS. Correlations with PANSS and BPRS, being schizophrenia-specific, were calculated for the patient group only. We correlated the MM with the conventional three factor model of the PANSS (Positive, Negative, Global) [50] as well as with the five-factor model of van der Gaag et. al (Positive, Negative, Disorganized, Excitement, Emotional Distress) [66, 67]. Correlations with NSS were calculated for the entire sample. We correlated the MM with gait specific items of the NSS scale (Station and Gait, Tandem Walk) as well as with its five subscales (Motor Coordination, Sensory Integration, Complex Motor Tasks, Right/Left Spatial Orientation, Hard Signs) [17].
Results
Sample characteristics
We screened over 140 and included 50 participants (22 patients, 28 controls). Due to drop out and propensity score matching, we analyzed the data of 40 individuals: 20 patients, 20 controls. See Table 1 for detailed sample characteristics.
Data-based movement markers
Results of the group comparison are shown in Table 2. Due to space limitations, it only contains movement features, which display significant group differences (see results of all t tests in Table 2 of the supplementary material). Features which withstood Bonferroni correction are marked bold.
-
(a)
Basic features patients and controls walked with significantly different speed (Mean velocity) resulting from a smaller stride or step length, not from a significantly different cadence (CA, SF see Table 2 supplementary material). They differed significantly in modeling power (Mean Power), indicating a less regular walk in the patient group, and varied more in their modeling power across moves (Standard Deviation of Power). It generally seems harder to model patients’ walk with FD.
-
(b)
Of all postural features (see Tables 1 and 2 in the supplementary material), only the angle between clavicle and head (head angle) was significantly different between the groups. Heads of patients “hang” more than those of controls.
-
(c)
Sway of body parts patients displayed a significantly reduced 3D, horizontal and anterior–posterior (AP) arm sway, a significantly reduced 3D elbow and knee sway, and a significantly increased lateral body sway..
-
(d)
Interplay of limb movement (interlimb coordination) patients displayed a significantly increased ratio of left and right arm or wrist movement, indicating lesser adjustment of the two body sides. Furthermore, we found significant differences in relational movement of the wrists and elbows (Ratio Wrist Elbow, Difference Wrist Elbow). Patients not only move wrists and elbows less in general, but they also move their wrists much less in relation to their own elbows, indicating stiffer arm movements. Similarly, we found significant differences in the relational movement of the arms and legs (Ratio Leg Arm, Difference Leg Arm) and shoulders and hips (Ratio Shoulder Hip, Difference Shoulder Hip). Patients do not adjust arm to leg movement (significantly more leg movement in relation to arm movement) or shoulder and hip movement to each other. Controls use their hips flexibly, patients walk with rather stiff hips, in a pendulum-like manner (twice as much lateral shoulder than hip movement).
-
(e)
Utilized range of motion we found significant differences between the groups of URM in AP and lateral direction, both of the upper and lower, left and right arm (URM Left Arm AP − URM Right Elbow lateral). Analyzing physicality-independent, biomechanical measures, we can confirm the finding that patients generally use upper and lower arms less than controls. Furthermore, the 3D angle inside the elbow changes significantly less for patients within one gait cycle (URM Left and Right Elbow 3D), indicating a rather stiff usage of the arms. We also could replicate significant differences in LBS by looking at changes in the lateral movement of the thorax in relation to the entire body (URM Thorax lateral).
-
(f)
Relational URM calculating the ratio of arm movement in AP and lateral direction, we found that movement in walking direction is more dominant in controls than in patients (Ratio URM Left and Right Arm, Difference URM Left and Right Arm). The strong expression of the control group’s arm movement in walking direction can be interpreted as a goal directedness of the arms or as less “unnecessary” movement in lateral directions. This result is supported by similar group differences concerning the shoulders: patients move their shoulders more in lateral direction, controls move them almost with the same amount in AP and lateral direction (Ratio URM Left and Right Shoulder, Difference URM Left and Right Shoulder). Furthermore, patients show smaller differences in AP and lateral movement of their upper and lower arms. They move their arms in a stiffer or less flexible way (Ratio Left Elbow Left Arm AP − Difference Right Elbow Right Arm lateral). This result replicates and refines the finding of a decreased URM in the elbow joint of patients.
-
(g)
All sway velocity measures are significantly different between the groups.
-
(h)
Patients display significantly more pronounced ratios of knee and elbow velocities.
Effect sizes are considerably large (d = 0.6–1.5). None of the auxiliary correlations and t tests were statistically significant (see Tables 3 and 4 in the supplementary material) indicating that movement features are indeed independent of medication. Applying the definition rules mentioned above (see also the auxiliary ANCOVA—Table 5 in the supplementary material), we defined 16 full-body MM for schizophrenia. Table 3 summarizes the MM, their manifestation within the groups and ways to quantify them (movement features). Except for a decreased vertical body sway, we found similar MM in patients with schizophrenia, which Michalak and colleagues [48] found in individuals with depression. Additionally, we found a reduced step length, a reduced regularity of gait and various MM indicating a reduced ability to integrate the movement of body sides and limbs. Following Bonferroni adjustment, significance was maintained for the regularity of the gait, the arm and elbow sway, the flexibility of arm movement, the goal directedness of the shoulder movement and arm and elbow sway velocities. Hence, we can confirm H1 to H3.
Correlations with clinical scales
Table 4 displays the correlations of the MM with the clinical scales. We can confirm H4. Almost all MM (except Lateral Body Sway and Knee Sway) are significantly correlated with total NSS scores and especially with the subscales Motor Coordination, Sensory Integration and Complex Motor Tasks. The correlations indicate that a stronger manifestation of the respective MM is associated with a stronger manifestation of NSS in general, specifically with coordination and integration related NSS. Furthermore, all objectively measured MM (except Lateral Body Sway and Goal Directedness of Movement) are significantly related to the subjectively rated NSS item “Station and Gait”. Again, and in all cases, a stronger manifestation of the respective MM is related to more disturbances in station and gait. Contrary to this, only some specific MM are correlated with the NSS item “Tandem Walk”: Head Posture, Variation of Gait Regularity, Arm and Elbow Sway, Flexibility of Limb Movement and Arm Sway Velocity.
We can not confirm H5: none of the correlation patterns with the positive, negative, global (PANSS) and overall symptom load (BPRS) are significant. This holds true when looking at van der Gaag’s five-factor model of the PANSS [67]: Except for the MM Goal directedness, which is positively related to the patients’ disorganisation, none of the correlations become significant. The positive correlation of the patients’ goal directedness with the disorganisation subscore contradicts the correlation patterns with NSS scores indicating a stronger manifestation of disorganisation when movements are more goal directed. Some MM display a correlational trend with the PANSS and BPRS. e.g. in the sense that less of an arm sway is related to an increase in positive, negative, disorganisational, excitement related and overall symptoms (e.g. rAS3, PANSS:Pos). Correlations of integration related features with the symptom load do not show a systematic pattern. Furthermore, we could not find a systematic difference between the interaction of the MM with positive or with negative symptoms.
Discussion
Our study revealed three major results. First, movement features extracted and quantified instrumentally from basic walking are able to differentiate between individuals with a diagnosis of schizophrenia and without. Second, the MM of schizophrenia are mainly related to the integration and adjustment of body sides, limbs or the direction of movement. Third, most of the MM are associated with increased NSS, particularly motor coordination and sensory-motor integration.
Our theory-independent MM are in line with results of the few previous studies analyzing posture and gait disturbances in people with schizophrenia [39,40,41, 48, 68, 69]: Cristiano et al. [69] identified forward head tilt as the most common postural feature in early and late-stage schizophrenia and found associations of postural changes with disease severity. Similarly, we identified the head posture as only significant posture marker and found associations of an increased “hanging” of the head with higher levels of NSS items “Station and Gait”, “Tandem Walk” and NSS subscales “Motor Coordination” and “Sensory Integration”. Like Putzhammer and colleagues [41], we identified a significantly decreased gait velocity in patients compared to controls, which can be ascribed to a shorter stride length, not to a decreased cadence. Similarly to Lallart and colleagues [40], who compared the stride-to-stride variability of patients and controls in a “walk alone” and in dual-task conditions and found significant differences in the dual-task conditions only, we did not find group differences concerning the variation of cadence in simple walking. An increased intraindividual variability in kinematic indices such as peak velocity and peak acceleration was also found by Jahn et al., who developed a device to analyse repetitive pronation/supination for subtle kinematic changes [70, 71]. Although pronation/supination, which is generally considered to be a typical NSS for schizophrenia [71], refers to fine motor performance of the hands, Jahn’s finding corresponds to our finding of an increased variation in gait regularity across moves (walks through the MoCap volume). Together with Lallart’s finding, it suggests that schizophrenia is characterized not merely by motor retardation but particularly by motor variability [71].
The fact that gait regularity was the only MM in our study which varied across moves might be related to the simplicity of our movement task. A dual-task condition was part of the above-mentioned additional movement tasks and will be analyzed in forthcoming publications. The striking differences of Lallart’s participants’ stride-to-stride variability while dual-tasking raises the assumption that the identified MM might be augmented by a dual-task. Additionally, Boks et al. [26] identified impaired motor coordination as most specific to patients with schizophrenia when comparing them to patients with a mood disorder; and Schiffman and colleagues [27] identified coordination deficits at the age of 10–13 as predictors of schizophrenia spectrum disorder at the age of 31–33. Although Schiffman and Boks as well restricted their analysis to fine motor performance and did not examine full-body movement, their results coincide with the many relational markers and variability differences we found. The relational features are particularly interesting, because they touch on the idea derived from embodied cognition that a disorganized mind is related to a disorganized body in the sense of a missing intrabodily and sensorimotor integration. Within the field of embodied cognition, the search for underlying brain alterations of schizophrenia is complemented by the analysis of interplay between mind, body and environment [72,73,74]. Schizophrenia is understood as a form of disembodiment, a missing integration and adjustment of sensorimotor loops, which results in an alienation of somatosensory perception, a lack of emotional expression, and a dissolution of the Gestalt units of movement and action [75, 76]. Successive movements (like one step after the other in walking) are described to lose their relatedness, smooth transition and “grace” [77, 78].
Tsakiris et al. [79] review studies on the sense of body-ownership (“It is my body, which is moving”) and the sense of agency (“I control my movements”) as two basic aspects of an embodied self-experience: while multisensory afferent signals suffice to create a sense of body ownership, it takes the integration of efferent motoric (self-initiated movement) and subsequent afferent sensory signals (multisensory integration) to create a sense of agency and finally a coherent experience of one’s own embodied self. On one hand, the fact that most MM are not only correlated with deficits in “Motor Coordination” but also with deficits in “Sensory Integration” can be seen as further evidence for disembodiment or a lack of multisensory integration in the patients [76]. On the other hand, the consistent relations of the MM with NSS total scores, which not only include motor but also sensory NSS, correspond to the transidagnostic nature of NSS and raises the question if our MM are of transdiagnostic value as well. NSS have been observed in other severe neuropsychiatric conditions such as bipolar disorder, Alzheimer disease or HIV-associated cognitive disorder and are understood by some researchers as signs for neurocognitive impairment in general [20, 80, 81]. While the fact that Michalak et al. [48] did not identify movement patterns related to the adjustment of limbs or body sides in patients with depression suggests the possibility of using MM for the prediction and differential diagnosis of schizophrenia, it remains to be tested if and which MM can be found in patients with other neuropsychiatric diagnoses.
Finally, relating the MM to gait specific NSS items allows for a preliminary validation. While almost all MM were associated with the item “station and gait”, only specific MM (Head Posture, Variation of Gait Regularity, Arm and Elbow Sway, Flexibility of Limb Movement and Arm Sway Velocity) were related to the NSS rating of the tandem walk. This makes sense, since the Tandem Walk—other than simple walking—is a highly coordinated, less habituated movement, which requires a straight posture, flexible limb and dextereous arm usage.
Limitations and future directions
This was an exploratory study with a relatively small sample size. Non-significant correlations of MM with clinical scales might be a consequence. Hertzog [82] reviews the precision of estimates in pilot studies and appraises samples of 10–20 as sufficient for clinical contexts, given the possibility to specify expected group differences in an a priori power analysis. Our sample size was an interdisciplinary compromise taking into account previous studies, power calculations and the availability of the motion lab. The replication of this study with a larger sample might lead to a systematic association of MM with positive and negative symptoms. Another reason for non-systematic relations of MM with PANSS scores could be the ongoing controversy in the literature about which factor model of the PANSS yields the most useful research results [83].
By conducting a data-driven, comprehensive mathematical description of the groups’ dynamic movement differences, we arrived at a very large amount of movement features, which overlap and correlate. To correct for multiple statistical testing we applied the Bonferroni correction. Streiner and Norman [84] discuss different correction types and arrive at the conclusion that the conservative Bonferroni method might lead to an overcorrection in explorative studies which aim at defining promising leads. Hence, we followed the researchers’ advice against correction in the definition of “areas”, in our case MM, that need follow-up in later studies [84]. In future analyses, we aim at a substantiation of the MM by conducting a factor analysis on the movement features and a multiple regression analysis.
Due to uncertainties concerning the reaction of vulnerable participants to the instrumental assessment, we exclusively examined individuals with a stable second-generation antipsychotic. To control for medication, we did auxiliary statistical analyses. Previous studies found no differences regarding GMA in never-medicated individuals and participants taking second-generation antipsychotics [41] and demonstrated that NSS vary in the course of the illness with psychopathological symptoms [21]. This includes a decline under neuroleptic treatment and speaks against an induction of GMA by medication. However, to entirely rule out the influence of medication on the identified MM, it would be beneficial to examine never-medicated or UHR individuals. This, and the longitudinal measurement of MM might answer the question to what extent behavioral MM can serve as predictors of a transition from a prodromal state to an acute psychosis or as indicators of disease progression. Since recent studies suggest that GMA gradually intensify on a continuum from prodrome to acute psychosis and that NSS improve with medication [1, 3, 20, 21] and since we found significant correlations of our MM with NSS, it is highly probable that a similar continuum can be established for the objectively assessed MM of this study and that the MM are primal symptoms of schizophrenia, which are independent of medical side effects.
Future studies should also assess the neuropathology underlying the identified MM. Recent neuroimaging studies support the hypothesis that GMA are linked to a disrupted “cortico-cerebellar-thalamic-cortical circuit” [1, 3, 10, 85]. However, studies on the neurological mechanisms underlying full-body gait disturbances in schizophrenia are scarce. On the way to defining a distinct motor domain for schizophrenia the present study should be expanded with a portable, neurological assessment, ideally guided by the current Mobile brain/Body imaging (MoBi) approach [86].
Finally, to integrate instrumental assessment into daily clinical practice, less expensive MoCap techniques (e.g. Kinect) should be explored. Prior to recruitment, we experimented with and found great bias in tools which base the motion tracking on inertial measurement units. Hence, we decided to establish subtle MM first and then transfer their mathematical and statistical evaluation to less detailed MoCap data. A greater accessibility and comprehensibility of MoCap data and its analysis might serve a systematic integration of motion assessment into clinical practice, generate great amounts of data and provide the missing link of GMA to the patients’ subjective experience.
Conclusion
Long-standing negligence of the moving body in schizophrenia research has left us with a diagnostic system heavily weighing positive and cognitive symptoms and underestimating motor abnormalities. The systematic and continuous assessment and staging of MM as well as their correlation with self-experience and subjective well-being could substantially improve early and differential diagnosis of schizophrenia. At length, not only diagnostics but also treatment of schizophrenia would benefit from a systematic staging of MM. While various studies underline the overall beneficiary effects of embodied therapies [75, 87,88,89], their underlying mechanisms are far from clear. With the help of external cues, Putzhammer et al. [41] could dissolve stride length differences between patients and controls. This is highly encouraging evidence for the beneficiary effect of identifying individual MM of patients and treating them with specifically targeted therapy.
Abbreviations
- GMA:
-
Genuine motor abnormalities
- NSS:
-
Neurological soft signs
- UHR:
-
Ultra high risk
- CPM:
-
Center for Psychosocial Medicine
- HMR:
-
Heidelberg center for motion research
- MoCap:
-
Motion capture
- FD:
-
Fourier decomposition
- LDF:
-
Linear discriminant function
- MM:
-
Movement markers
- MF:
-
Movement features
- URM:
-
Utilized range of motion
References
Hirjak D, Thomann PA, Kubera KM, Wolf ND, Sambataro F, Wolf RC (2015) Motor dysfunction within the schizophrenia-spectrum: a dimensional step towards an underappreciated domain. Schizophr Res 169(1–3):217–233
Peralta V, Cuesta MJ (2001) Motor features in psychotic disorders. I. Schizophr Res 47(2):107–116
Hirjak D, Meyer-Lindenberg A, Kubera KM, Thomann PA, Wolf RC (2018) Motor dysfunction as research domain in the period preceding manifest schizophrenia: a systematic review. Neurosci Biobehav Rev 87:87–105
Walther S, Strik W (2012) Motor symptoms and schizophrenia. Neuropsychobiology 66(2):77–92
Peralta V, Campos MS, De Jalón EG, Cuesta MJ (2010) Motor behavior abnormalities in drug-naïve patients with schizophrenia spectrum disorders. Mov Disord 25(8):1068–1076
van Harten PN, Walther S, Kent JS, Sponheim SR, Mittal VA (2017) The clinical and prognostic value of motor abnormalities in psychosis, and the importance of instrumental assessment. Neurosci Biobehav Rev 80:476–487
Mittal VA, Neumann C, Saczawa M, Walker EF (2008) Longitudinal progression of movement abnormalities in relation to psychotic symptoms in adolescents at high risk of schizophrenia. Arch Gen Psychiatry 56(2):165–171
Hirjak D, Kubera MK, Thomann PA, Wolf RC (2017) Motor dysfunction as an intermediate phenotype across schizophrenia and other psychotic disorders: progress and perspectives. Schizophr Res 200:26–34
Pavlidou A, Walther S (2021) Using virtual reality as a tool in the rehabilitation of movement abnormalities in schizophrenia. Front Psychol 11:3733
Walther S, Mittal VA (2017) Motor system pathology in psychosis. Curr Psychiatry Rep 19(12):1–9
Morita K, Miura K, Fujimoto M, Yamamori H, Yasuda Y, Kudo N, Azechi H, Okada N, Koshiyama D, Ikeda M, Kasai K, Hashimoto R (2019) Eye movement abnormalities and their association with cognitive impairments in schizophrenia. Schizophr Res 209:255
Dowiasch S, Backasch B, Einhäuser W, Leube D, Kircher T, Bremmer F (2016) Eye movements of patients with schizophrenia in a natural environment. Eur Arch Psychiatry Clin Neurosci 266(1):43–54
Bombin I, Arango C, Buchanan RW (2005) Significance and meaning of neurological signs in schizophrenia: two decades later. Schizophr Bull 31(4):962–977
Bombin I, Arango C, Buchanan RW (2003) Assessment tools for soft signs. Psychiatr Ann 33:170–176
Buchanan RW, Heinrichs DW (1989) The neurological evaluation scale (NES): a structured instrument for the assessment of neurological signs in schizophrenia. Psychiatry Res 27(3):335–350
Chen EYH, Shapleske J, Luque R, McKenna PJ, Hodges JR, Calloway SP, Hymas NFS, Dening TR, Berrios GE (1995) The Cambridge Neurological Inventory: a clinical instrument for assessment of soft neurological signs in psychiatric patients. Psychiatry Res 56(2):183–204
Schröder J, Niethammer R, Geider F-J, Reitz C, Binkert M, Jauss M, Sauer H (1991) Neurological soft signs in schizophrenia. Schizophr Res 6(1):25–30
Walther S, Koschorke P, Horn H, Strik W (2009) Objectively measured motor activity in schizophrenia challenges the validity of expert ratings. Psychiatry Res 169(3):187–190
Walther S, van Harten PN, Waddington JL, Cuesta MJ, Peralta V, Dupin L, Foucher JR, Sambataro F, Morrens M, Kubera KM, Pieters LE, Stegmayer K, Strik W, Wolf RC, Hirjak D (2020) Movement disorder and sensorimotor abnormalities in schizophrenia and other psychoses—European consensus on assessment and perspectives. Eur Neuropsychopharmacol 38:25–39
Schröder J, Toro P (2020) Neurological soft signs predict outcomes in schizophrenia. Nat Rev Neurol 16(12):659–660
Bachmann S, Schröder J (2018) Neurological soft signs in schizophrenia: an update on the state-versus trait-perspective. Front Psych 8:272
Jahn T, Hubmann W, Karr M, Mohr F, Schlenker R, Heidenreich T, Cohen R, Schröder J (2006) Motoric neurological soft signs and psychopathological symptoms in schizophrenic psychoses. Psychiatry Res 142(2–3):191–199
Cuesta MJ, Moreno-Izco L, Ribeiro M, Lecumberri P, Cabada T, Lorente-Omenaca R, Sánchez-Torres A, Goméz MS, Peralta V (2018) Motor abnormalities and cognitive impairment in first-episode psychosis patients, their unaffected siblings and healthy controls. Schizophr Res 200:50–55
Cuesta MJ, de Jalón EG, Campos MS, Moreno-Izco L, Lorente-Omeñaca R, Sánchez-Torres AM, Peralta V (2018) Motor abnormalities in first-episode psychosis patients and long-term psychosocial functioning. Schizophr Res 200:79
Boks MPM, Liddle PF, Burgerhof JGM, Knegtering R, van den Bosch RJ (2004) Neurological soft signs discriminating mood disorders from first episode schizophrenia. Acta Psychiatr Scand 110(1):29–35
Boks MPM, Russo S, Knegtering R, van den Bosch RJ (2000) The specificity of neurological signs in schizophrenia: a review. Schizophr Res 43(2):109–116
Schiffman J, Sorensen HJ, Maeda J, Mortensen EL, Victoroff J, Hayashi K, Michelsen NM, Ekstrom M, Mednick S (2009) Childhood motor coordination and adult schizophrenia spectrum disorders. Am J Psychiatry 166(9):1041–1047
Kalampratsidou V, Torres EB (eds) (2017) Body-brain-avatar interface: a tool to study sensory-motor integration and neuroplasticity. In: Fourth international symposium on movement and computing, MOCO
Dumas G, de Guzman GC, Tognoli E, Kelso JS (2014) The human dynamic clamp as a paradigm for social interaction. Proc Natl Acad Sci 111(35):E3726–E3734
Torres EB, Brincker M, Isenhower RW III, Yanovich P, Stigler KA, Nurnberger JI Jr, Metaxas DN, José JV (2013) Autism: the micro-movement perspective. Front Integr Neurosci 7:32
Zapata-Fonseca L, Martin L, Froese T, Fuchs T (2021) Operationalizing disembodied interaction: the perceptual crossing experiment in schizophrenia research. Phenomenol Mind 21:112–125
Caligiuri MP, Lohr JB, Rotrosen J, Adler L, Lavori P, Edson R, Tracy K (1997) Reliability of an instrumental assessment of tardive dyskinesia: results from VA Cooperative Study# 394. Psychopharmacology 132(1):61–66
Dean DJ, Teulings HL, Caligiuri M, Mittal VA (2013) Handwriting analysis indicates spontaneous dyskinesias in neuroleptic naive adolescents at high risk for psychosis. Journal of visualized experiments: JoVE 81
Janno S, Holi MM, Tuisku K, Wahlbeck K (2008) Neuroleptic-induced movement disorders in a naturalistic schizophrenia population: diagnostic value of actometric movement patterns. BMC Neurol 8(1):1–8
Senova S, Querlioz D, Thiriez C, Jedynak P, Jarraya B, Palfi S (2015) Using the accelerometers integrated in smartphones to evaluate essential tremor. Stereotact Funct Neurosurg 93(2):94–101
Kupper Z, Ramseyer F, Hoffmann H, Kalbermatten S, Tschacher W (2010) Video-based quantification of body movement during social interaction indicates the severity of negative symptoms in patients with schizophrenia. Schizophr Res 121(1–3):90–100
Walther S, Horn H, Razavi N, Koschorke P, Müller TJ, Strik W (2009) Quantitative motor activity differentiates schizophrenia subtypes. Neuropsychobiology 60(2):80–86
Walther S, Mittal VA (2016) Why we should take a closer look at gestures. Schizophr Bull 42(2):259–261
Putzhammer A, Heindl B, Broll K, Pfeiff L, Perfahl M, Hajak G (2004) Spatial and temporal parameters of gait disturbances in schizophrenic patients. Schizophr Res 69(2–3):159–166
Lallart E, Jouvent R, Herrmann FR, Perez-Diaz F, Lallart X, Beauchet O, Allali G (2014) Gait control and executive dysfunction in early schizophrenia. J Neural Transm 121(4):443–450
Putzhammer A, Perfahl M, Pfeiff L, Hajak G (2005) Gait disturbances in patients with schizophrenia and adaptation to treadmill walking. Psychiatry Clin Neurosci 59(3):303–310
van der Kruk E, Reijne MM (2018) Accuracy of human motion capture systems for sport applications; state-of-the-art review. Eur J Sport Sci 18(6):806–819
Fuchs T, Koch SC (2014) Embodied affectivity: on moving and being moved. Front Psychol 5:508
Troje NF (2008) Retrieving information from human movement patterns. In: Shipley TF, Zacks JM (eds) Understanding events: from perception to action. Oxford University Press, Oxford
Dittrich WH, Troscianko T, Lea SE, Morgan D (1996) Perception of emotion from dynamic point-light displays represented in dance. Perception 25(6):727–738
Atkinson AP, Dittrich WH, Gemmell AJ, Young AW (2004) Emotion perception from dynamic and static body expressions in point-light and full-light displays. Perception 33(6):717–746
Troje NF (2002) Decomposing biological motion: a framework for analysis and synthesis of human gait patterns. J Vis 2(5):2
Michalak J, Troje NF, Fischer J, Vollmar P, Heidenreich T, Schulte D (2009) Embodiment of sadness and depression—gait patterns associated with dysphoric mood. Psychosom Med 71(5):580–587
World Medical Association (2013) World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA 310(20):2191–2194
Kay SR, Flszbein A, Opfer LA (1987) The positive and Negative Syndrome Scale (PANSS) for schizophrenia. Schizophr Bull 13(2):261–276
Overall JE, Gorham DR (1962) The brief psychiatric rating scale. Psychol Rep 10(3):799–812
Simpson GM, Angus JWS (1970) A rating scale for extrapyramidal side effects. Acta Psychiatr Scand 45(Suppl 212):11–19
Janno S, Holi M, Tuisku K, Wahlbeck K (2005) Validity of Simpson-Angus Scale (SAS) in a naturalistic schizophrenia population. BMC Neurol 5(1):5
C-Motion. Marker Set Guidelines https://www.c-motion.com/v3dwiki/index.php?title=Marker_Set_Guidelines. Accessed 5 Oct 2021
RStudio Team (2019) RStudio: integrated development for R. RStudio Inc, Boston
Leucht S, Samara M, Heres S, Patel MX, Furukawa T, Cipriani A, Geddes J, Davis JM (2015) Dose equivalents for second-generation antipsychotic drugs: the classical mean dose method. Schizophr Bull 41(6):1397–1402
Harris H, Horst SJ (2016) A brief guide to decisions at each step of the propensity score matching process. Pract Assess Res Eval 21(1):4
Caliendo M, Kopeinig S (2008) Some practical guidance for the implementation of propensity score matching. J Econ Surv 22(1):31–72
Ejdemyr S (2020) R Tutorial 8: propensity score matching https://sejdemyr.github.io/. Accessed 19 Oct 2021
Troje NF (2002) The little difference: Fourier based synthesis of gender-specific biological motion. Dynam Percept:115–120
Rab G, Petuskey K, Bagley A (2002) A method for determination of upper extremity kinematics. Gait Posture 15(2):113–119
Cappozzo A, Catani F, Leardini A, Benedetti MG, Della CU (1996) Position and orientation in space of bones during movement: experimental artefacts. Clin Biomech 11(2):90–100
Leardini A, Sawacha Z, Paolini G, Ingrosso S, Nativo R, Benedetti MG (2007) A new anatomically based protocol for gait analysis in children. Gait Posture 26(4):560–571
C-Motion. Coda Pelvis https://www.c-motion.com/v3dwiki/index.php?title=Coda_Pelvis. Accessed 20 Aug 2021
Michalak J, Rohde K, Troje NF (2015) How we walk affects what we remember: gait modifications through biofeedback change negative affective memory bias. J Behav Ther Exp Psychiatry 46:121–125
van der Gaag M, Cuijpers A, Hoffman T, Remijsen M, Hijman R, de Haan L, van Meijel B, van Harten PN, Valmaggia L, de Hert M, Wiersma D (2006) The five-factor model of the Positive and Negative Syndrome Scale I: confirmatory factor analysis fails to confirm 25 published five-factor solutions. Schizophr Res 85(1):273–279
van der Gaag M, Hoffman T, Remijsen M, Hijman R, de Haan L, van Meijel B, van Harten PN, Valmaggia L, de Hert M, Cuijpers A, Wiersma D (2006) The five-factor model of the Positive and Negative Syndrome Scale II: a ten-fold cross-validation of a revised model. Schizophr Res 85(1):280–287
Feldman R, Schreiber S, Pick CG, Been E (2020) Gait, balance and posture in major mental illnesses: depression, anxiety and schizophrenia. Austin Med Sci 5(1):1039
Cristiano VB, Vieira Szortyka MF, Lobato MI, Ceresér KM, Belmonte-de-Abreu P (2017) Postural changes in different stages of schizophrenia is associated with inflammation and pain: a cross-sectional observational study. Int J Psychiatry Clin Pract 21(2):104–111
Jahn T, Cohen R, Mai N, Ehrensperger M, Marquardt C, Nitsche N, Schrader S (1995) Untersuchung der fein- und grobmotorischen Dysdiadochokinese schizophrener Patienten: Methodenentwicklung und erste Ergebnisse einer computergestützten Mikroanalyse. Z Klin Psychol 24:300–315
Schröder J, Essig M, Baudendistel K, Jahn T, Gerdsen I, Stockert A, Schad LR, Knopp MV (1999) Motor dysfunction and sensorimotor cortex activation changes in schizophrenia: a study with functional magnetic resonance imaging. Neuroimage 9(1):81–87
Merleau-Ponty M (1962) Phenomenology of perception. Routledge, New York
Fuchs T, Schlimme JE (2009) Embodiment and psychopathology: a phenomenological perspective. Curr Opin Psychiatry 22(6):570–575
Gallagher S (2005) How the body shapes the mind. Oxford University Press, Oxford
Martin L, Koch S, Hirjak D, Fuchs T (2016) Overcoming disembodiment: the effect of movement therapy on negative symptoms in schizophrenia—a multicenter randomized controlled trial. Front Psychol
Fuchs T (2005) Corporealized and disembodied minds: a phenomenological view of the body in melancholia and schizophrenia. Philos Psychiatry Psychol 12(2):95–107
Fuchs T (2000) Psychopathologie von Leib und Raum: Melancholie und Schizophrenie. Springer, Berlin, pp 99–184
Kraepelin E (1987) Dementia praecox. In: Shepherd JCM (ed) The clinical roots of the schizophrenia concept: translations of seminal European contributions on schizophrenia. Cambridge University Press, New York, pp 13–24
Tsakiris M, Schütz-Bosbach S, Gallagher S (2007) On agency and body-ownership: phenomenological and neurocognitive reflections. Conscious Cogn 16(3):645–660
Toro P, Ceballos ME, Pesenti J, Inostroza M, Valenzuela D, Henríquez F, Forno G, Herold C, Schröder J, Calderón J (2018) Neurological soft signs as a marker of cognitive impairment severity in people living with HIV. Psychiatry Res 266:138–142
Urbanowitsch N, Degen C, Toro P, Schröder J (2015) Neurological soft signs in aging, mild cognitive impairment, and Alzheimer’s disease—the impact of cognitive decline and cognitive reserve. Front Psych 6:12
Hertzog MA (2008) Considerations in determining sample size for pilot studies. Res Nurs Health 31(2):180–191
Jerrell JM, Hrisko S (2013) A comparison of the PANSS Pentagonal and Van Der Gaag 5-factor models for assessing change over time. Psychiatry Res 207(1):134–139
Streiner DL, Norman GR (2011) Correction for multiple testing: is there a resolution? Chest 140(1):16–18
Bernard JA, Russell CE, Newberry RE, Goen JR, Mittal VA (2017) Patients with schizophrenia show aberrant patterns of basal ganglia activation: evidence from ALE meta-analysis. NeuroImage Clin 14:450–463
Jungnickel E, Gehrke L, Klug M, Gramann K (2019) MoBI—Mobile brain/body imaging. In: Ayaz H, Dehais F (eds) Neuroergonomics—the brain at Work2019, pp 59–63
Martin L, Pohlmann V, Koch SC, Fuchs T (2016) Back into life: effects of embodied therapies on patients with schizophrenia. Eur Psychother:179–194
Röhricht F, Priebe S (2006) Effect of body-oriented psychological therapy on negative symptoms in schizophrenia: a randomized controlled trial. Psychol Med 36(05):669–678
Priebe S, Savill M, Wykes T, Bentall R, Reininghaus U, Lauber C, Bremner S, Eldridge S, Röhricht F (2015) Effectiveness of group body psychotherapy as a treatment for negative symptoms of schizophrenia - a multi-centre randomised controlled trial. Br J Psychiatry 13:1
Acknowledgements
We would like to thank all participants for taking part in the experiments as well as Saeed Ghorbani and Tina Sedaghat for their help in data analysis and animation.
Funding
Open Access funding enabled and organized by Projekt DEAL. Foundation of German Economy, doctoral scholarship. Graduate Academy of Heidelberg University (heiDOCS-beCULT), expense allowance of participants.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have declared that there are no competing interest in relation to the subject of this study.
Animations
Visualization of discriminant walker: https://www.biomotionlab.ca/martin2022/
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Martin, L., Stein, K., Kubera, K. et al. Movement markers of schizophrenia: a detailed analysis of patients’ gait patterns. Eur Arch Psychiatry Clin Neurosci 272, 1347–1364 (2022). https://doi.org/10.1007/s00406-022-01402-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00406-022-01402-y