
Abstract
Purposes
To investigate longitudinally (1) the contribution of morphological covariates to explaining the development of maximum cardiac output (\({\dot{\text{Q}}}\) max) and maximum arteriovenous oxygen difference (a-vO2 diff max), (2) sex differences in \({\dot{\text{Q}}}\) max and a-vO2 diff max once age, maturity status, and morphological covariates have been controlled for, and, (3) the contribution of concurrent changes in morphological and cardiovascular covariates to explaining the sex-specific development of peak oxygen uptake (\(\dot{{V}}{\mathrm{O}}_{2}\)).
Methods
Fifty-one (32 boys) 11–13-year-olds had their peak \(\dot{{V}}{\mathrm{O}}_{2}\), maximum heart rate (HR max), \({\dot{\text{Q}}}\) max, and a-vO2 diff max determined during treadmill running on three annual occasions. The data were analysed using multilevel allometric modelling.
Results
There were no sex differences in HR max which was not significantly (p > 0.05) correlated with age, morphological variables, or peak \(\dot{{V}}{\mathrm{O}}_{2}\). The best-fit models for \({\dot{\text{Q}}}\) max and a-vO2 diff max were with fat-free mass (FFM) as covariate with age, maturity status, and haemoglobin concentration not significant (p > 0.05). FFM was the dominant influence on the development of peak \(\dot{{V}}{\mathrm{O}}_{2}\). With FFM controlled for, the introduction of either \({\dot{\text{Q}}}\) max or a-vO2 diff max to multilevel models of peak \(\dot{{V}}{\mathrm{O}}_{2}\) resulted in significant (p < 0.05) additional contributions to explaining the sex difference.
Conclusions
(1) With FFM controlled for, there were no sex differences in \({\dot{\text{Q}}}\) max or a-vO2 diff max, (2) FFM was the dominant influence on the development of peak \(\dot{{V}}{\mathrm{O}}_{2}\), and (3) with FFM and either \({\dot{\text{Q}}}\) max or a-vO2 diff max controlled for, there remained an unresolved sex difference of ~ 4% in peak \(\dot{{V}}{\mathrm{O}}_{2} .\)
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Peak oxygen uptake (\({\dot{\text{V}}\text{O}}_{2}\)), the highest \({\dot{\text{V}}\text{O}}_{2}\) elicited during an incremental exercise test to exhaustion, is internationally recognized as the ‘gold standard’ measure of youth cardiorespiratory fitness. Peak \({\dot{\text{V}}\text{O}}_{2}\) is probably the most researched physiological variable in paediatric exercise science (Falk et al. 2018), but the vast majority of investigations have been cross-sectional with data analyses clouded by inappropriate ratio scaling of peak \({\dot{\text{V}}\text{O}}_{2}\) with body mass (BM) and interpretation of youth peak \({\dot{\text{V}}\text{O}}_{2}\) in mL kg−1 min−1 (Welsman and Armstrong 2019). Even when interpreted appropriately, cross-sectional studies only provide a ‘snapshot’ of a continuous process and there are remarkably few rigorously analysed longitudinal studies of youth cardiorespiratory fitness. The influence of concurrent changes in morphological and physiological covariates on the development of peak \({\dot{\text{V}}\text{O}}_{2}\) during childhood and adolescence remains to be elucidated (Armstrong and McManus 2017).
Multilevel allometric modelling (Rasbash et al. 2018) allows the effects of age, maturity status, morphological covariates, and physiological covariates to be partitioned concurrently within an allometric framework to provide a sensitive interpretation of the development of peak \(\dot{{V}}{\mathrm{O}}_{2}\). The application of multilevel allometric modelling has provided new insights into the role of morphological covariates in the development of cardiorespiratory fitness during childhood and adolescence (Armstrong and Welsman 2019a, b; Nevill et al. 1998). Recent studies have explored the influence of age- and maturity status-driven changes in BM and fat-free mass (FFM) on the development of peak \({\dot{\text{V}}\text{O}}_{2}\) from 10 to 18 years. Peak \({\dot{\text{V}}\text{O}}_{2}\) was demonstrated to be ergometer-specific but regardless of exercise modality (i.e., running or cycling) and in both sexes, with age and BM controlled for, maturity status made a positive contribution to explaining peak \(\dot{{V}}{\mathrm{O}}_{2}\). However, when FFM was introduced to the multilevel allometric models in place of BM, the independent effects of maturity status were negated, and the models provided significantly (p < 0.05) better statistical fits to the data. However, even with FFM controlled for, an unexplained sex difference in peak \({\dot{\text{V}}\text{O}}_{2}\) remained with boys’ values significantly (p < 0.05) higher than those of girls (Armstrong and Welsman 2019a, b).
It is consistently reported that pulmonary ventilation does not limit the peak \({\dot{\text{V}}\text{O}}_{2}\) of healthy youth (Fawkner 2007; McManus and Armstrong 2017; Nixon 2018), so the unexplained sex difference in peak \(\dot{{V}}{\mathrm{O}}_{2}\) is likely to be influenced by differences in cardiovascular variables at peak \(\dot{{V}}{\mathrm{O}}_{2}\). Cardiovascular components of \(\dot{{V}}{\mathrm{O}}_{2}\) are described by the Fick equation where \( \dot{{V}}{\mathrm{O}}_{2}\) = cardiac output × arteriovenous oxygen difference and cardiac output is a function of heart rate and stroke volume. Both cross-sectional and longitudinal studies of heart rate at peak \(\dot{{V}}{\mathrm{O}}_{2}\) (HR max) have reported that HR max is independent of age, maturity status, peak \(\dot{{V}}{\mathrm{O}}_{2}\), and sex during childhood and early adolescence (Bailey et al. 1978; McNarry et al. 2014; Rowland et al. 1997b; Rutenfranz et al. 1981). In contrast, there are few cross-sectional studies of cardiac output at peak \(\dot{{V}}{\mathrm{O}}_{2}\) (\({\dot{\text{Q}}}\) max), stroke volume at peak \(\dot{{V}}{\mathrm{O}}_{2}\) (SV max), or arteriovenous oxygen difference at peak \(\dot{{V}}{\mathrm{O}}_{2}\) (a-vO2 diff max) (Rowland 2017; Turley 1997; Winsley 2007). Prior to the present study, no studies had investigated longitudinally the contribution of concurrent changes in morphological and cardiovascular variables to the development of peak \(\dot{{V}}{\mathrm{O}}_{2}\).
Understanding the responses of cardiovascular variables to maximum exercise is limited by ethical and methodological challenges and no direct measurements of heathy children’s \({\dot{\text{Q}}}\) max or a-vO2 diff max have been reported. Several indirect methods of estimating \({\dot{\text{Q}}}\) during exercise have been developed and Doppler echocardiography, bioimpedance cardiography, and carbon dioxide (CO2) rebreathing have been demonstrated to be safe and reliable methods of estimating \({\dot{\text{Q}}}\) in paediatric exercise studies (Patterson et al. 1982; Warburton et al. 2008; Welsman et al. 2005). There are, however, no ‘gold standard’ reference values of \({\dot{\text{Q}}}\) max or a-vO2 diff max as all techniques suitable for use with healthy children are subject to varying degrees of error. Measures of cardiovascular variables should, therefore, only be compared within methodologies although trends are consistent across methodologies (Driscoll et al. 1989; Warburton and Breder 2018; Washington 1993).
Cross-sectional studies consistently show young adults to have higher absolute values of \({\dot{\text{Q}}}\) max (i.e., expressed in L·min−1) than children but when \({\dot{\text{Q}}}\) max is expressed in ratio with body surface area (BSA) (i.e. in L min−1 m−2) as the cardiac index values are similar (Nottin et al. 2002; Rowland et al. 1997a, 2000b). In childhood and early adolescence, cross-sectional studies suggest that boys’\({\dot{\text{Q}}}\) max is typically larger than similar aged girls’\({\dot{\text{Q}}}\) max and remains larger when expressed as the cardiac index (Rowland 2005; Vinet et al. 2003; Winsley 2007). However, ratio scaling \({\dot{\text{Q}}}\) max with BSA clouds understanding of its development.
Scaling \({\dot{\text{Q}}}\) max in ratio with BSA is convenient and traditional, but 70 years ago, Tanner (1949) unequivocally established that ratio scaling of cardiac data with BSA was fallacious. It has, subsequently, been demonstrated that the most appropriate method of scaling \({\dot{\text{Q}}}\) max is with a curvilinear allometric model (Batterham et al. 1997, 1999; Rowland 2017) and once it has been allometrically scaled with BSA neither age nor maturity status influence \({\dot{\text{Q}}}\) max (McNarry et al. 2014; Rowland 2017). \({\dot{\text{Q}}}\) max is, however, more closely matched to metabolic demand than body size and should be considered in relation to active muscle mass rather than BSA. Determining young people’s active muscle mass is experimentally challenging, and FFM has emerged as a pragmatic and appropriate morphological variable with which to scale \({\dot{\text{Q}}}\) max in developmental exercise physiology.
It has been compellingly argued that \({\dot{\text{Q}}}\) max is best expressed in relation to FFM raised to an empirically derived allometric scaling exponent calculated from the participants in a study (Batterham et al. 1997, 1999; Rowland 2017). In a well-designed cross-sectional study, Vinet et al. (2003) demonstrated that when \({\dot{\text{Q}}}\) max was expressed relative to FFM0.76, there were no longer \({\dot{\text{Q}}}\) max differences between 10 to 12-year-old boys and girls. However, appropriately modelled longitudinal studies are required to elucidate the development of \({\dot{\text{Q}}}\) max and its influence on the development of peak \(\dot{{V}}{\mathrm{O}}_{2}\) during childhood and adolescence.
In a longitudinal investigation with the same participants as in the present study, we reported that with FFM controlled for, there was no significant (p > 0.05) sex difference in SV max. Moreover, with FFM controlled for, a ~ 5% sex difference in peak \(\dot{{V}}{\mathrm{O}}_{2}\) was present and the introduction of SV max to the multilevel allometric model revealed that SV max made a significant (p < 0.05) additional contribution to explaining the development of peak \(\dot{{V}}{\mathrm{O}}_{2}.\) However, a residual ~ 4% sex difference remained (Armstrong and Welsman 2019c).
There are few reports of a-vO2 diff max in children and early adolescents with data from girls particularly sparse. As a-vO2 diff max is normally calculated from \({\dot{\text{Q}}}\) max and peak \(\dot{{V}}{\mathrm{O}}_{2}\), measures of a-vO2 diff max have similar limitations to those for \({\dot{\text{Q}}}\) max. Cross-study comparisons of data must, therefore, be made with caution. Within studies, a-vO2 diff max has consistently been reported to be higher in young adult men than in boys (Nottin et al. 2002; Rowland et al. 1997a), but data from studies focused on children and early adolescents indicate that a-vO2 diff max is not influenced by age (Gilliam et al. 1977; Rowland 2005; Yamaji and Miyashita 1977), sex (Obert et al. 2003; Rowland et al. 2000a; Vinet et al. 2003), or maturity status (McNarry et al. 2011, 2014; Rowland 2017). Significant associations between a-vO2 diff max and peak \(\dot{{V}}{\mathrm{O}}_{2}\) have not been identified in children and adolescents (Rowland 2017; Rowland et al. 1999b).
In summary, changes in FFM have been demonstrated to be the dominant morphological influence on the development of peak \(\dot{{V}}{\mathrm{O}}_{2}\) in both sexes (Armstrong and Welsman 2019a, b). SV max makes a small, additional contribution to FFM in explaining sex differences in the development of peak \(\dot{{V}}{\mathrm{O}}_{2}\) (Armstrong and Welsman 2019c) and HR max appears to be independent of peak \(\dot{{V}}{\mathrm{O}}_{2}\) and sex (Rowland 2017). The longitudinal development of \({\dot{\text{Q}}}\) max, and a-vO2 diff max and their influence on the development of peak \(\dot{{V}}{\mathrm{O}}_{2}\) have not been rigorously explored using appropriate models in which covariates are partitioned concurrently within an allometric framework. The purposes of the present study are, therefore, to use multilevel allometric modelling to investigate in children and early adolescents: (1) the contribution of morphological covariates to explaining the development of \({\dot{\text{Q}}}\) max and a-vO2 diff max, (2) sex differences in \({\dot{\text{Q}}}\) max and a-vO2 diff max once age, maturity status, and morphological covariates have been controlled for, and (3) the contribution of concurrent changes in morphological and cardiovascular covariates to explaining the sex-specific development of peak \(\dot{{V}}{\mathrm{O}}_{2}.\)
Methods
Participants
Fifty-one (32 boys) 11–13-year-olds participating in a longitudinal study of cardiorespiratory fitness and short-term power output (Armstrong and Welsman 2019a, d) volunteered to have their maximum cardiovascular responses to exercise determined on three annual occasions. The SV max data have been published (Armstrong and Welsman 2019c), but complementary data on HR max, \({\dot{\text{Q}}}\) max, and a-vO2 diff max have not previously been analysed or reported.
Experimental procedures
Determination of resting variables
Participants were well habituated to the laboratory environment, to the laboratory personnel, and to the experimental procedures. Age was computed from date of birth and date of test. Anthropometric measures were taken as described by the International Biological Programme (Weiner and Lourie 1981) and apparatus was calibrated according to the manufacturers’ instructions. BM was assessed using Avery balance scales (Avery, Birmingham, UK), stature was measured using a Holtain stadiometer (Holtain, Crmych, Dyfed, UK), and skinfold thicknesses over the triceps and subscapular regions were measured using Holtain skinfold callipers. Maturity status was visually assessed by the Research Centre nurse using the indices for pubic hair (PH) development described by Tanner (1962). FFM was estimated from skinfolds, BM, and maturity status using the youth-specific equations developed by Slaughter et al. (1988). Haemoglobin (Hb) concentration was determined as the mean value from duplicate fingertip blood samples which were immediately assayed using a Hemo Cue photometer (Clandon Scientific, Farnborough, UK).
Determination of exercise variables
Participants attended the Research Centre annually on two consecutive mornings to complete the required exercise protocols. Peak \(\dot{{V}}{\mathrm{O}}_{2}\) and HR at peak \(\dot{{V}}{\mathrm{O}}_{2}\) were determined on day one, and at a similar time, the following morning SV max was determined. All exercise tests were preceded by a standardized warm-up. Peak \(\dot{{V}}{\mathrm{O}}_{2}\) was determined during a discontinuous, incremental exercise test to voluntary exhaustion on a motorized treadmill (Woodway, Cranlea Medical, Birmingham, UK). HR was monitored using an electrocardiograph (Rigel, Morden, UK) and expired respiratory gases were monitored continuously using an Oxycon Sigma on-line gas-analysis system (Cranlea Medical) which was calibrated prior to each test using gases of verified concentration and an appropriate range of flow rates using a Hans Rudolph calibration syringe (Cranlea Medical). The tests began at a treadmill belt speed of 1.94 m s−1 (7 km h−1) which was increased by 0.28 m s−1 (1 km h−1) every 3 min until a speed of 2.78 m s−1 (10 km h−1) was reached. Subsequently, belt speed was held constant and the gradient was incrementally increased by 2.5% every 3 min until voluntary exhaustion. A 1 min rest period separated the exercise stages. The highest 30 s \(\dot{{V}}{\mathrm{O}}_{2}\) attained was accepted as a maximal index if clear signs of intense exertion (e.g., hyperpnea, facial flushing unsteady gait, and profuse sweating) were demonstrated and supported by a respiratory exchange ratio greater than 1.00 and an HR which was levelling-off over the final stages of the test at a value within 5% of the mean peak HR that we have previously reported for large groups of similar aged young people using the same test protocol (Armstrong et al. 1991). All participants reported in this study satisfied these criteria.
On the following morning, using the same apparatus including the \({\dot{\text{Q}}}\) determination facility of the Oxycon Sigma \(\dot{{V}}{\mathrm{O}}_{2}\), HR, and \({\dot{\text{Q}}}\) were determined during the final minute of 3 min treadmill running at 2.50 m s−1 (9 km h−1). \({\dot{\text{Q}}}\) was determined using the CO2 rebreathing technique in accord with the methodology recommended by Jones (1997). The partial pressure of CO2 in arterial blood (PaCO2) was estimated from the end-tidal CO2. The partial pressure of mixed venous CO2 (PvCO2) was estimated from the rebreathing equilibrium. The downstream correction was applied to the partial pressure of the equilibration CO2 to adjust for alveolar to blood partial pressure differences. The CO2 content of venous and arterial blood was calculated from PvCO2 and PaCO2 using the McHardy curve adjusted for the effect of individual differences in Hb (McHardy et al. 1967). The volume of gas in the rebreathing bag was calculated to be 1.5 times the mean of three previous tidal breaths and the bag CO2 concentration, which varied from 9 to 13%, was calculated based on the \(\dot{{V}}{\mathrm{O}}_{2}\) and the end-tidal partial pressure of CO2. The size of the rebreathing bag was selected individually to accommodate the gas volume but without being so large as to prevent appropriate CO2 equilibrium. Only tests which demonstrated a CO2 equilibrium were included in the data (Jones 1997).
Data analysis
Data were stored and analysed using SPSS version 25 (IBM, SPSS statistics, Portsmouth, UK). In a preliminary study, we confirmed with these students that SV reaches its maximal value and plateaus during progressive treadmill running above moderate-exercise intensities. We reported no significant (p > 0.05) change (~ 2–3%) in SV running at 2.22 m s−1 (8 km h−1), 2.50 m s−1 (9 km h−1) and 2.78 m s−1 (10 km h−1) despite a significant (p < 0.05) ~ 16–17% increase in \(\dot{{V}}{\mathrm{O}}_{2}\) (Armstrong and Welsman 2019c). SV as determined herein was, therefore, recorded as SV max. Individual values of \({\dot{\text{Q}}}\) max were determined by multiplying SV max by HR max and a-vO2 diff max was calculated by re-arranging the Fick equation (i.e., a-vO2 diff max = peak \(\dot{{V}}{\mathrm{O}}_{2}\)/\({\dot{\text{Q}}}\) max). Longitudinal relationships between BM and FFM, respectively, and cardiovascular variables and between cardiovascular variables and peak \(\dot{{V}}{\mathrm{O}}_{2}\) were graphed, and Pearson product-moment correlation coefficients computed with significance set at p < 0.05.
Longitudinal data were analysed using multilevel regression modelling (MLWin v3.02, Centre for Multilevel Modeling, University of Bristol, UK). In contrast to traditional methods that require a complete longitudinal data set, both the number of observations per individual and the temporal spacing of the observations can vary within a multilevel analysis. Longitudinal changes in \({\dot{\text{Q}}}\) max, a-vO2 diff max, and peak \(\dot{{V}}{\mathrm{O}}_{2}\) were analysed using the multiplicative, allometric approach introduced to paediatric exercise physiology by Nevill et al. (1998) and implemented in subsequent longitudinal analyses of youth exercise performance (e.g., Armstrong and Welsman 2019a, b, c, d; Armstrong et al. 2019) as in Eqs. 1 and 2:
where y = \({\dot{\text{Q}}}\) max, a-vO2 diff max, or peak \(\dot{{V}}{\mathrm{O}}_{2}\).
Log transformation linearizes the model as in Eqs. 3 and 4 forming the starting point for analyses:
where y = \({\dot{\text{Q}}}\) max, a-vO2 diff max, or peak \(\dot{{V}}{\mathrm{O}}_{2}\).
All parameters were fixed with the exception of the constant (a) which was allowed to vary randomly at level 2 (between individuals) and the multiplicative error ratio (ε) which also varied randomly at level 1 (within individuals) as denoted by the subscripts i (level 1 variation) and j (level 2 variation). Age was centred on the group mean. Other factors associated with the dependent variable were explored either as additional covariates or through the calculation of dummy variables (e.g., setting the boys’ constant as baseline and investigating any departure from this for girls and setting PH stage 1 as the baseline from which effects of PH stages 2, 3, 4, and 5 could be explored) or interaction terms allowing for different relationships between covariates and sex to be examined.
Parameter estimates were considered significant (p < 0.05) where their value exceeded 2 × the standard error (SE). Where more than one model was investigated, a comparison of the goodness of fit of the different models was obtained from the change in the deviance statistic (− 2 × log-likelihood) with reference to the number of fitted parameters. The model with the smallest log-likelihood reflects that with the best fit for the same number of fitted parameters. Additional parameters contribute to improved fit from the change in the log-likelihood according to a chi-squared statistic for additional degrees of freedom added.
Results
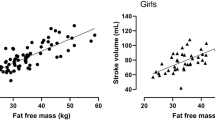
Longitudinal relationships by sex between HR max, \({\dot{\text{Q}}}\) max, and a-vO2 diff max, respectively, with BM and with FFM are illustrated in Figs. 1 and 2. \({\dot{\text{Q}}}\) max in boys was significantly (p < 0.01) and strongly correlated with both BM and FFM with moderate, significant (p < 0.01) correlations in girls. Significant (p < 0.01) but weak correlations between a-vO2 diff max and morphological variables were apparent in both sexes. HR max was not significantly (p > 0.05) correlated with BM or FFM, in either boys or girls. Figure 3 describes the relationships between HR max, \({\dot{\text{Q}}}\) max, and a-vO2 diff max, respectively, and peak \(\dot{{V}}{\mathrm{O}}_{2}\), and shows no significant (p > 0.05) correlations between HR max and peak \(\dot{{V}}{\mathrm{O}}_{2}\). \({\dot{\text{Q}}}\) max was significantly (p < 0.01) and strongly correlated with peak \(\dot{{V}}{\mathrm{O}}_{2}\) in both sexes. a-vO2 diff max was also significantly (p < 0.01) correlated with peak \(\dot{{V}}{\mathrm{O}}_{2}\) in both sexes, but with weak-to-moderate strength coefficients.

Maximum heart rate, maximum cardiac output, and maximum arteriovenous oxygen difference in relation to body mass

Maximum heart rate, maximum cardiac output, and maximum arteriovenous oxygen difference in relation to fat-free mass

Peak oxygen uptake in relation to maximum heart rate, maximum cardiac output, and maximum arteriovenous oxygen difference
As HR max was not significantly (p > 0.05) related to BM, FFM, or peak \(\dot{{V}}{\mathrm{O}}_{2,}\) the multilevel allometric analyses presented herein are focused on \({\dot{\text{Q}}}\) max and a-vO2 diff max. Table 1 presents multilevel allometric models for loge\({\dot{\text{Q}}}\) max and loge a-vO2 diff max with loge BM or loge FFM as covariates. In model 1.1, loge BM was revealed as a significant (p < 0.05) covariate of loge\({\dot{\text{Q}}}\) max with a significant (p < 0.05) negative sex term showing boys’ values to be higher than those of girls. In Model 1.2 with loge FFM replacing loge BM in the model, there was no significant (p > 0.05) sex difference in loge\({\dot{\text{Q}}}\) max. Model 1.2 provided a significantly (p < 0.05) better statistical fit with loge\({\dot{\text{Q}}}\) max increasing proportionally to FFM0.69. Model 1.3 shows loge BM as a significant (p < 0.05) covariate of loge a-vO2 diff max, but model 1.4 with loge FFM replacing loge BM provided a significantly (p < 0.05) better statistical fit. With either loge BM or loge FFM controlled for, there were no significant (p > 0.05) sex differences in loge a-vO2 diff max. Once either loge BM or loge FFM had been controlled for, the introduction of age, maturity status, or Hb concentration into any model in Table 1 was not significant (p > 0.05).
Table 2 describes multilevel allometric models for loge peak \(\dot{{V}}{\mathrm{O}}_{2}\). Model 2.1 shows, with loge FFM controlled for, a significant (p < 0.05) sex difference of ~ 5% in loge peak \(\dot{{V}}{\mathrm{O}}_{2}\). Models 2.2 and 2.4 show with either loge\({\dot{\text{Q}}}\) max or loge a-vO2 diff max, respectively, controlled for, no significant (p > 0.05) sex differences in loge peak \(\dot{{V}}{\mathrm{O}}_{2}\). Model 2.1 is a significantly (p < 0.05) better statistical fit for loge peak \(\dot{{V}}{\mathrm{O}}_{2}\) than either Model 2.2 or 2.4. Model 2.3 shows that with loge FFM controlled for, loge\({\dot{\text{Q}}}\) max was an additional and significant (p < 0.05) covariate of loge peak \(\dot{{V}}{\mathrm{O}}_{2}\) with a significant (p < 0.05) sex difference in loge peak \(\dot{{V}}{\mathrm{O}}_{2}\) of ~ 4%. Model 2.3 provides a significantly (p < 0.05) better fit than both Model 2.1 and Model 2.2. Similarly, Model 2.5 shows that with loge FFM controlled for, loge a-vO2 diff max was an additional and significant (p < 0.05) covariate of loge peak \(\dot{{V}}{\mathrm{O}}_{2}\) with a significant (p < 0.05) sex difference in loge peak \(\dot{{V}}{\mathrm{O}}_{2}\) of ~ 4%. Model 2.5 provides a significantly (p < 0.05) better fit than both Model 2.1 and Model 2.4. The introduction of age, maturity status, or Hb concentration into any model in Table 2 was not significant (p > 0.05).
Discussion
Directly comparing values of \({\dot{\text{Q}}}\) max and a-vO2 diff max data across methodologies must be done with extreme caution (Warburton and Breder 2018), but the present data are in accord with values from cross-sectional studies which used CO2 rebreathing with similarly aged children and adolescents (Gilliam et al. 1977; Miyamura and Honda 1973: Yamaji and Miyashita 1977). Cross-sectional studies of similarly aged young people have reported HR max and a-vO2 diff max to be independent of sex but boys’ \({\dot{\text{Q}}}\) max to be higher than girls’ \({\dot{\text{Q}}}\) max (Armstrong et al. 1991; Miyamura and Honda 1973; Obert et al. 2003; Rowland et al. 2000a; Vinet et al. 2003; Winsley et al. 2009). However, growth and maturation are continuous processes driven by individual biological clocks and cross-sectional ‘snapshots’ of paediatric exercise data provide limited insights into developmental exercise physiology (Armstrong 2019; Baxter-Jones 2017; Malina et al. 2004). There are no longitudinal studies with which to compare the descriptive relationships described in Figs. 1, 2, and 3. The figures nicely describe the data, but as discussed earlier, provide few meaningful insights into the development of \({\dot{\text{Q}}}\) max, a-vO2 diff max, or peak \(\dot{{V}}{\mathrm{O}}_{2}\). In contrast, multilevel allometric modelling describes the underlying mean response as individual growth trajectories are modelled.
Model 1.1 (Table 1) shows that \({\dot{\text{Q}}}\) max increased in proportion to BM0.63 with a significant (p < 0.05) sex difference of ~ 8%. However, \({\dot{\text{Q}}}\) max is dependent on metabolic demand and more closely related to the volume of metabolically active tissue than to total BM. Data indicate that cardiac dimensions are closely associated with FFM and suggestive of a potential relationship between skeletal and cardiac muscularity (Batterham et al. 1997, 1999; George et al. 1991). As quantifying actively contracting muscle mass during maximum exercise in childhood and adolescence is extremely challenging, FFM has become established as an appropriate surrogate marker of active muscle (Batterham et al. 1999; Rowland 2017; Vinet et al. 2003). Model 1.2 shows that \({\dot{\text{Q}}}\) max increases in proportion to FFM0.69 and provides a model with no significant (p > 0.05) sex differences and a significantly (p < 0.05) better fit than Model 1.1. With FFM controlled for, neither age nor maturity status were significant (p > 0.05) explanatory variables, but this may have been influenced by the limited age range and population of maturity stages in the present data. There are no comparative longitudinal data on cardiovascular variables, but it has been demonstrated that when FFM replaces BM in a multilevel modelling analysis of the development of peak \(\dot{{V}}{\mathrm{O}}_{2}\) from 10 to 18 years, the effects of maturity status are negated in both boys and girls (Armstrong and Welsman 2019a).
In childhood and adolescence, HR max is independent of body size. \({\dot{\text{Q}}}\) max and SV max should, therefore, relate to morphological variables by similar exponents. This is the case with the present data with SV max increasing in relation to BM0.64 with a significant (p < 0.05) sex difference of ~ 9% and in relation to FFM0.70 with no significant (p > 0.05) sex difference. The FFM exponents of both \({\dot{\text{Q}}}\) max and SV max fall within the 95% confidence limits of previous cross-sectional studies (Rowland et al. 2000a; Vinet et al. 2003). (SV max models are not presented herein as multilevel allometric models of the development of the SV max of these participants have been analysed in Armstrong and Welsman 2019c).
Models 1.3 and 1.4 show that a-vO2 diff max increases in relation to BM0.26 and FFM0.29, but Model 1.4 with FFM as covariate presents a significantly (p < 0.05) better fit than Model 1.3. With either BM or FFM controlled for, age, maturity status, Hb concentration, and sex were not significant (p > 0.05). Comparative data on boys and girls are sparse, but there is no compelling evidence to support sex differences in a-vO2 diff max during childhood and early adolescence (Obert et al. 2003; Rowland 2005, 2017; Vinet et al. 2003). a-vO2 diff max represents the difference at peak \(\dot{{V}}{\mathrm{O}}_{2}\) between the arterial oxygen content of blood approaching the muscles and the venous oxygen content as it leaves. Arterial oxygen content is primarily dependent on Hb concentration and, consistent with cross-sectional data on similar aged students from elsewhere (Armstrong et al. 1991; Obert et al. 2003; Vinet et al. 2003), Hb concentration was not a significant (p > 0.05) covariate in the present study. There is no persuasive empirical evidence to suggest sex differences in peripheral factors which are likely to influence venous oxygen content and, therefore, peak \(\dot{{V}}{\mathrm{O}}_{2}\). Potential influences on muscle oxygen utilization include blood flow distribution, muscle capillarization, mitochondrial density, muscle fibre types, muscle activation, and muscle aerobic enzyme activity, but experimental exploration in developmental exercise physiology awaits the emergence and application of appropriate non-invasive technology (Armstrong et al. 2017; Dotan et al. 2012; Malina et al. 2004; Rowland 2005).
It has been demonstrated that age and maturity status-driven changes in FFM provide the most powerful morphological influence on peak \(\dot{{V}}{\mathrm{O}}_{2}\) in 10–18 year-olds of both sexes and account for much of the increasing sex difference in the development of youth cardiorespiratory fitness (Armstrong and Welsman 2019a, b). Over the 10–18 years age range, FFM increases by ~ 105% and ~ 55% in boys and girls, respectively, and with BM controlled for, there is a ~ 16% sex difference in peak \(\dot{{V}}{\mathrm{O}}_{2}\) which falls to ~ 10% with FFM controlled for, in place of BM (Armstrong 2019; Armstrong and Welsman 2019a). Increases in peak \(\dot{{V}}{\mathrm{O}}_{2}\) during youth are driven by gains in either oxygen delivery to or oxygen utilization by the active muscles, or both. Growth and development of active muscle mass, reflected by FFM, not only enhance muscle oxygen utilization during exercise but, through the peripheral muscle pump, also augment venous return, boost \({\dot{\text{Q}}}\) max, and, therefore, increase oxygen delivery to the muscles (Armstrong and McManus 2017; Armstrong et al. 2017; Rowland 2017).
From 11 to 13 years, FFM rises on average, by ~ 28% and ~ 26% in boys and girls, respectively, but with wide individual variations as it is driven not only by chronological age but by the timing and tempo of biological maturation. FFM increases by ~ 60% and ~ 30% in boys and girls, respectively, from 1 year prior to 1 year post peak height velocity (Armstrong 2019; Baxter-Jones et al. 2003). In the present data set with children and early adolescents, there was a ~ 12% sex difference in peak \(\dot{{V}}{\mathrm{O}}_{2}\) with BM controlled for and Model 2.1 (Table 2) illustrates that with sex-specific changes in FFM controlled for, there was a smaller but still significant (p < 0.05) ~ 5% sex difference in peak \(\dot{{V}}{\mathrm{O}}_{2}\).
Model 2.2 shows that peak \(\dot{{V}}{\mathrm{O}}_{2}\) increases in relation to \({\dot{\text{Q}}}\) max0.88 and Model 2.4 shows that peak \(\dot{{V}}{\mathrm{O}}_{2}\) increases in relation to a-vO2 diff max0.74. In both cases, once either \({\dot{\text{Q}}}\) max or a-vO2 diff max were controlled for, there was no significant (p > 0.05) sex difference in peak \(\dot{{V}}{\mathrm{O}}_{2}\). However, Model 2.1 with FFM controlled for shows a significant (p < 0.05) sex difference in the development of peak \(\dot{{V}}{\mathrm{O}}_{2}\) and provides a significantly (p < 0.05) better statistical fit than either Model 2.2 with \({\dot{\text{Q}}}\) max controlled for, or Model 2.4 with a-vO2 diff max controlled for.
Models 2.3 and 2.5, respectively, show that with FFM controlled for, both \({\dot{\text{Q}}}\) max and a-vO2 diff max are additional, independent and significant (p > 0.05) covariates of peak \(\dot{{V}}{\mathrm{O}}_{2}\) with, in each case, a significant (p < 0.05) ~ 4% sex difference in peak \(\dot{{V}}{\mathrm{O}}_{2}.\) The models including FFM and either \({\dot{\text{Q}}}\) max (Model 2.3) or a-vO2 diff max (Model 2.5) provide significantly (p < 0.05) better statistical fits than Model 2.1. This finding agrees with our earlier publication in which with FFM controlled for, the introduction of SV max provided a significantly (p < 0.05) better fit model of peak \(\dot{{V}}{\mathrm{O}}_{2}\) than FFM alone, with a similar ~ 4% sex difference (Armstrong and Welsman 2019c).
Collectively, the data show that age- and maturity status-driven changes in FFM are the dominant morphological influences on the development of 11–13-year-olds’ \({\dot{\text{Q}}}\) max and a-vO2 diff max, and that with FFM controlled for, there are no significant sex differences in either \({\dot{\text{Q}}}\) max or a-vO2 diff max. FFM is also the dominant influence on the development of peak \(\dot{{V}}{\mathrm{O}}_{2}\) but, even with FFM controlled for, there remains a ~ 5% sex difference in peak \(\dot{{V}}{\mathrm{O}}_{2}\). Concurrent changes in FFM and either \({\dot{\text{Q}}}\) max or a-vO2 diff max provide a better fit model of peak \(\dot{{V}}{\mathrm{O}}_{2}\) than FFM alone, but a residual and unexplained ~ 4% sex difference in peak \(\dot{{V}}{\mathrm{O}}_{2}\) remains.
Strengths and limitations
A potential criticism of the present study is using CO2 rebreathing to monitor SV at ~ 83% (girls) and ~ 74% (boys) of peak \(\dot{{V}}{\mathrm{O}}_{2},\) extrapolating it to represent SV max and using it with HR max to calculate \({\dot{\text{Q}}}\) max. However, this SV response is one of the most consistently observed responses in cardiac exercise physiology and has been reliably demonstrated in healthy, untrained children and adolescents using a range of methodologies including CO2 rebreathing (Rowland 2017; Warburton and Bredin 2018; Washington 1993). Values of exercise SV above ~ 50% of peak \(\dot{{V}}{\mathrm{O}}_{2}\) have been reported to reflect SV max and be characteristic of individuals as well as group means (Rowland et al. 1999a, 2000c; Rowland 2005). A unique strength of the present study is that despite an increase in exercise intensity resulting in a rise in \(\dot{{V}}{\mathrm{O}}_{2}\) of ~ 16–17%, a SV plateau within ~ 2–3% was demonstrated in all participants. Moreover, SV data were collected as close to peak \(\dot{{V}}{\mathrm{O}}_{2}\) as reasonable for the young participants, many of whom found CO2 rebreathing unpleasant at high exercise intensities (Armstrong and Welsman 2019c).
The estimation of FFM from BM and skinfold thicknesses rather than its direct measurement using more sophisticated technology can be criticised, but this methodology is well established in paediatric exercise physiology (Slaughter et al. 1988) and ‘direct’ measures of the body fat of 12–14-year-olds have recently been shown to vary widely across laboratory techniques (Ferri-Morales et al. 2018). Regardless of assessment, FFM includes tissues not involved in exercise and ideally active muscle mass would be directly determined on each test occasion, but this is not currently feasible in paediatric exercise studies.
With three annual measurement occasions, the study only partially covers childhood and adolescence and potential effects of age and maturity status might have been limited by the small age range. The study does, however, provide for the first time longitudinal insights into the development of \({\dot{\text{Q}}}\) max and a-vO2 diff max and on their influence both individually and with concurrent changes in FFM, on the development of the peak \(\dot{{V}}{\mathrm{O}}_{2}\) of healthy, untrained children, and early adolescents. Moreover, collectively, the present study and a parallel study on the same students (Armstrong and Welsman 2019c) provide insights into the development of all components of the Fick equation and their effect on the development of peak \(\dot{{V}}{\mathrm{O}}_{2}\). A major strength of the study lies in using multiplicative allometric modelling analyses in which individual growth trajectories are modelled and morphological and cardiovascular covariates are partitioned concurrently within an allometric framework to provide sensitive interpretations of the development of, \({\dot{\text{Q}}}\) max, a-vO2 diff max, and peak \(\dot{{V}}{\mathrm{O}}_{2}.\)
Conclusions
\({\dot{\text{Q}}}\) max and a-vO2 diff max increase in proportion to FFM0.69 and FFM0.29, respectively. Once FFM has been controlled for, multilevel allometric models demonstrate that, in accord with SV max, there are no sex differences in either the \({\dot{\text{Q}}}\) max or a-vO2 diff max of children and early adolescents. Changes in age- and maturity status-driven FFM are the dominant influences on the development of peak \(\dot{{V}}{\mathrm{O}}_{2}\), but with FFM controlled for, there remains a ~ 5% sex difference. With FFM controlled for, concurrent changes in either \({\dot{\text{Q}}}\) max or a-vO2 diff max make additional, independent and significant contributions to explaining the development of peak \(\dot{{V}}{\mathrm{O}}_{2}\), but a residual ~ 4% sex difference remains unresolved in each case. The data clearly demonstrate that rigorous exploration of the development of cardiorespiratory fitness during growth and maturation requires longitudinal studies which include analyses of the influence of concurrent changes in both morphological and physiological covariates.
Abbreviations
- a-vO2 diff:
-
Arteriovenous oxygen difference
- BM:
-
Body mass
- BSA:
-
Body surface area
- CO2 :
-
Carbon dioxide
- \({\dot{\text{Q}}}\) :
-
Cardiac output
- FFM:
-
Fat-free mass
- Hb:
-
Haemoglobin
- HR:
-
Heart rate
- max:
-
Maximum
- \(\dot{{V}}{\mathrm{O}}_{2}\) :
-
Oxygen uptake
- PaCO2 :
-
Partial pressure of CO2 in arterial blood
- PvCO2 :
-
Partial pressure of mixed venous CO2
- PH:
-
Pubic hair
- SV:
-
Stroke volume
References
Armstrong N (2019) Development of the youth athlete. Routledge, Oxford
Armstrong N, McManus AM (2017) Aerobic fitness. In: Armstrong N, Mechelen W (eds) Oxford textbook of children’s sport and exercise medicine, 3rd edn. Oxford University Press, Oxford, pp 161–180
Armstrong N, Welsman J (2019a) Sex-specific longitudinal modeling of youth aerobic fitness. Pediatr Exerc Sci 31:204–212
Armstrong N, Welsman J (2019b) Development of peak oxygen uptake from 11–16 years determined using both treadmill and cycle ergometry. Eur J Appl Physiol 119:801–812
Armstrong N, Welsman J (2019c) Multilevel allometric modelling of maximal stroke volume and peak oxygen uptake in 11–13-year-olds. Eur J Appl Physiol 119:2629–2639
Armstrong N, Welsman J (2019d) Sex-specific longitudinal modeling of short-term power in 11- to 18-year-olds. Med Sci Sports Exerc 51:1055–1063
Armstrong N, Williams J, Balding J, Gentle P, Kirby B (1991) Peak oxygen uptake of British children with reference to age, sex and sexual maturity. Eur J Appl Physiol 62:369–375
Armstrong N, Barker AR, McManus AM (2017) Muscle metabolism during exercise. In: Armstrong N, Mechelen W (eds) Oxford textbook of children’s sport and exercise medicine, 3rd edn. Oxford University Press, Oxford, pp 69–87
Armstrong N, Welsman J, Bloxham SR (2019) Development of 11–16 year-olds’ short-term power output determined using both treadmill and cycle ergometry. Eur J Appl Physiol 119:1565–1580
Bailey DA, Ross WD, Mirwald RL, Weese C (1978) Size dissociation of maximal aerobic power during growth in boys. Med Sport Sci 11:140–151
Batterham AM, George KP, Mullineaux DR (1997) Allometric scaling of left ventricular mass by body dimensions in males and females. Med Sci Sports Exerc 29:181–186
Batterham AM, George KP, Whyte G, Sharma S, McKenna W (1999) Scaling cardiac structural data by body dimensions: a review of theory, practice and problems. Int J Sports Med 20:495–502
Baxter-Jones ADG (2017) Growth and maturation. In: Armstrong N, Mechelen W (eds) Oxford textbook of children’s sport and exercise medicine, 3rd edn. Oxford University Press, Oxford, pp 13–24
Baxter-Jones ADG, Mirwald RL, McKay HA, Bailey D (2003) A longitudinal analysis of sex differences in bone mineral accrual in healthy 8–19-year-old boys and girls. Ann Hum Biol 30:160–175
Dotan R, Mitchell C, Cohen R, Klentrou P, Gabriel D, Falk B (2012) Child-adult differences in muscle activation—a review. Pediatr Exerc Sci 24:2–21
Driscoll DJ, Staats BA, Beck KC (1989) Measurement of cardiac output in children during exercise: a review. Pediatr Exerc Sci 1:102–115
Falk B, Klentrou P, Armstrong N, Rowland TW, Kemper HCG (2018) A brief history of pediatric exercise physiology. Pediatr Exerc Sci 30:1–10
Fawkner SG (2007) Pulmonary function. In: Armstrong N (ed) Paediatric exercise physiology. Churchill Livingstone, Edinburgh, pp 119–138
Ferri-Morales A, Nascimento-Ferreira MV, Vlachopoulos D et al (2018) Agreement between standard body composition methods to estimate percentage of body fat in young male athletes. Pediatr Exerc Sci 30:402–410
George KP, Wolfe LA, Burggraf GW (1991) The ‘athletic heart syndrome’: a critical review. Sports Med 11:300–331
Gilliam TB, Sady S, Thorland WG, Weltman AL (1977) Comparison of peak performance measures in children ages 6 to 8, 9 to 10, and 11 to 13 years. Res Quart 48:695–702
Jones NL (1997) Clinical exercise testing, 4th edn. WB Saunders Company, Philadelphia, pp 109–123
Malina RM, Bouchard C, Bar-Or O (2004) Growth, maturation and physical activity, 2nd edn. Human Kinetics, Champaign
McHardy GJR, Jones NL, Campbell EJM (1967) Graphical analysis of carbon dioxide transport during exercise. Clin Sci 32:289–298
McManus AM, Armstrong N (2017) Pulmonary function. In: Armstrong N, Mechelen W (eds) Oxford textbook of children’s sport and exercise medicine, 3rd edn. Oxford University Press, Oxford, pp 133–146
McNarry MA, Welsman JR, Jones AM (2011) Influence of training and maturity status on the cardiopulmonary responses to ramp incremental cycle and upper body exercise in girls. J Appl Physiol 110:375–381
McNarry MA, Mackintosh KA, Stoedefalke K (2014) Longitudinal investigation of training status and cardiopulmonary responses in pre- and early-pubertal children. Eur J Appl Physiol 114:1573–1780
Miyamura M, Honda Y (1973) Maximum cardiac output related to sex and age. Jpn J Physiol 23:645–656
Nevill AM, Holder RL, Baxter-Jones A, Round JM, Jones DA (1998) Modelling developmental changes in strength and aerobic power in children. J Appl Physiol 84:963–970
Nixon PA (2018) Pulmonary function. In: Rowland TW (ed) Cardiopulmonary exercise testing in children and adolescents. Human Kinetics, Champaign, pp 127–138
Nottin S, Vinet A, Stecken N, Nguyen L-D, Ounissi F, Lecoq A-M, Obert P (2002) Central and peripheral cardiovascular adaptations during maximal cycle exercise in boys and men. Med Sci Sports Exerc 33:456–463
Obert P, Mandigout S, Nottin S, Vinet A, Nguyen L-D, Lecoq A-M (2003) Cardiovascular response to endurance training in children: effect of gender. Eur J Clin Investig 33:199–208
Patterson DH, Cunningham DA, Plyley MJ, Blimkie CJR, Donner A (1982) The consistency of cardiac output measurement (CO2 rebreathe) in children during exercise. Eur J Appl Physiol 49:37–44
Rasbash J, Steele F, Browne WJ, Goldstein H (2018) A user’s guide to MLwiN Version 3.02. University of Bristol Centre for Multilevel Modelling, Bristol
Rowland TW (2005) Children’s exercise physiology, 2nd edn. Human Kinetics, Champaign
Rowland TW (2017) Cardiovascular function. In: Armstrong N, Mechelen W (eds) Oxford textbook of children’s sport and exercise medicine, 3rd edn. Oxford University Press, Oxford, pp 147–159
Rowland T, Popowski B, Ferrone L (1997a) Cardiac responses to maximal upright cycle exercise in healthy boys and men. Med Sports Sci Exerc 29:1146–1151
Rowland T, Vanderburgh P, Cunningham L (1997b) Body size and the growth of maximal aerobic power in children: a longitudinal analysis. Pediatr Exerc Sci 9:262–274
Rowland T, Goff D, Martel L, Ferrone L (1999a) Estimation of maximal stroke volume from submaximal values (abstract). Pediatr Exerc Sci 11:279
Rowland T, Kline G, Goff D, Martel L, Ferrone L (1999b) Physiological determinants of maximal aerobic power in healthy 12-year-old boys. Pediatr Exerc Sci 11:317–326
Rowland T, Goff D, Martel L, Ferrone L (2000a) Influence of cardiac functional capacity on gender differences in maximal oxygen uptake in children. Chest 17:629–635
Rowland T, Miller K, Vanderburgh P, Goff D, Martel L, Ferrone L (2000b) Cardiovascular fitness in premenarcheal girls and young women. Int J Sports Med 21:117–121
Rowland T, Potts J, Potts T, Sandor G, Goff D, Ferrone L (2000c) Cardiac responses to progressive exercise in normal children: a synthesis. Med Sci Sports Exerc 32:253–259
Rutenfranz J, Andersen KL, Seliger V, Klimmer F, Berndt I, Ruppel M (1981) Maximum aerobic power and body composition during the puberty growth period: similarities and differences between children of two European countries. Eur J Pediatr 136:122–133
Slaughter MH, Lohman TG, Boileau RA, Horswill CA, Stillman RJ, Van Loan MD, Bemben DA (1988) Skinfold equations for estimation of body fatness in children and youth. Hum Biol 60:709–723
Tanner JM (1949) Fallacy of per-weight and per-surface area standards and their relation to spurious correlation. J Appl Physiol 2:1–15
Tanner JM (1962) Growth at adolescence, 2nd edn. Blackwell, Oxford, pp 28–39
Turley KR (1997) Cardiovascular responses to exercise in children. Sports Med 24:241–257
Vinet A, Mandigout S, Nottin S, Nguyen LD, Lecoq A-M, Courteix D, Obert P (2003) Influence of body composition, hemoglobin concentration, and cardiac size and function on gender differences in maximal oxygen uptake in prepubertal children. Chest 124:1494–1499
Warburton DER, Bredin SSD (2018) Cardiac output measurement techniques. In: Rowland TW (ed) Cardiopulmonary exercise testing in children and adolescents. Human Kinetics, Champaign, IL, pp 107–118
Warburton DER, Nettlefold L, McGuire KA, Bredin SSD (2008) Cardiovascular function. In: Armstrong N, Mechelen W (eds) Paediatric exercise science and medicine, 2nd edn. Oxford University Press, Oxford, pp 77–95
Washington RL (1993) Measurement of cardiac output. In: Rowland TW (ed) Pediatric laboratory exercise testing. Human Kinetics, Champaign, pp 131–140
Weiner JS, Lourie JA (1981) Practical human biology. Academic Press, London, pp 33–51
Welsman J, Armstrong N (2019) Interpreting aerobic fitness in youth: the fallacy of ratio scaling. Pediatr Exerc Sci 31:184–190
Welsman JR, Bywater K, Farr C, Welford D, Armstrong N (2005) Reliability of peak VO2 and maximal cardiac output assessed using thoracic bioimpedance in children. Eur J Appl Physiol 94:228–234
Winsley RJ (2007) Cardiovascular function. In: Armstrong N (ed) Paediatric exercise physiology. Churchill Livingstone, Edinburgh, pp 139–160
Winsley RJ, Fulford J, Roberts AC, Welsman JR, Armstrong N (2009) Sex difference in peak oxygen uptake in prepubertal children. J Sci Med Sport 12:647–657
Yamaji K, Miyashita M (1977) Oxygen transport system during exhaustive exercise in Japanese boys. Eur J Appl Physiol 36:93–99
Acknowledgements
We gratefully acknowledge the commitment of the participants, the logistic support of Exeter schools, and the technical assistance of the Children’s Health and Exercise Research Centre team.
Funding
This study was funded by the British Heart Foundation.
Author information
Authors and Affiliations
Contributions
NA and JW jointly conceived and designed the research, led the research team, and analysed the data. Both authors contributed to the drafting of the manuscript; both authors reviewed and approved the final version.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki Declaration and its later amendments or comparable standards.
Informed consent
Written informed consent was obtained from all individual participants included in the study and from their legal guardians.
Additional information
Communicated by I. Mark Olfert.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Armstrong, N., Welsman, J. Multilevel allometric modelling of maximum cardiac output, maximum arteriovenous oxygen difference, and peak oxygen uptake in 11–13-year-olds. Eur J Appl Physiol 120, 527–537 (2020). https://doi.org/10.1007/s00421-020-04300-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-020-04300-0