
Abstract
Exposure to heatwaves may result in adverse human health impacts. Heat alerts in South Africa are currently based on defined temperature-fixed threshold values for large towns and cities. However, heat-health warning systems (HHWS) should incorporate metrics that have been shown to be effective predictors of negative heat-related health outcomes. This study contributes to the development of a HHWS for South Africa that can potentially minimize heat-related mortality. Distributed lag nonlinear models (DLNM) were used to assess the association between maximum and minimum temperature and diurnal temperature range (DTR) and population-adjusted mortality during summer months, and the effects were presented as incidence rate ratios (IRR). District-level thresholds for the best predictor from these three metrics were estimated with threshold regression. The mortality dataset contained records of daily registered deaths (n = 8,476,532) from 1997 to 2013 and data for the temperature indices were for the same period. Maximum temperature appeared to be the most statistically significant predictor of all-cause mortality with strong associations observed in 40 out of 52 districts. Maximum temperature was associated with increased risk of mortality in all but three of the districts. Our results also found that heat-related mortality was influenced by regional climate because the spatial distribution of the thresholds varied according to the climate zones across the country. On average, districts located in the hot, arid interior provinces of the Northern Cape and North West experienced some of the highest thresholds compared to districts located in temperate interior or coastal provinces. As the effects of climate change become more significant, population exposure to heat is increasing. Therefore, evidence-based HHWS are required to reduce heat-related mortality and morbidity. The exceedance of the maximum temperature thresholds provided in this study could be used to issue heat alerts as part of effective heat health action plans.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Climate change is projected to intensify the adverse health impacts of extreme heat by increasing their frequency, severity, and duration of heatwave events (Ebi et al. 2021; Zhao et al. 2022). Several record-breaking heatwaves have been reported in many parts of the world. In the summer of 2003, for example, Europe experienced its hottest heatwave in 500 years; studies showed that heat-related excess deaths during the 2003 European summer exceeded 70,000 (Luterbacher et al. 2004; Trigo et al. 2009; Christoph and Gerd 2004; Robine et al. 2008; Fouillet et al. 2006). Similarly, in 2010, Russia experienced its worst heatwave since records began that resulted in an estimated 55,000 deaths (Hoag 2014; Grumm 2011). In 2006 in the USA, California (which was the most affected state) recorded 655 heat-related deaths over 2 weeks (Coumou and Rahmstorf 2012; Knowlton et al. 2012, 2008). Devasting heatwaves which were associated with high numbers of deaths and illnesses have also been reported in Australia and India (Nitschke et al. 2011; Azhar et al. 2014; Mazdiyasni et al. 2017).
It is evident that research on health-related impacts of heatwaves is unevenly distributed as the majority of studies are concentrated in mid-latitude temperate regions including North America, Europe, eastern China, and Australia while lacking in lower middle-income settings such as Africa and South America (Campbell et al. 2018). For example, South Africa has experienced prolonged, intense heatwaves in recent years; however, there are no published articles that present the health effects of these events leading to an underestimation of the risks. Most reports about health outcomes attributed to extreme heat in the country are from media sources, such as recent media releases that revealed eight people, most of them farm workers, died from heatstroke in the Northern Cape province of the country during a heatwave in late January 2023 (AfricaNews 2023).
Given the severity of the impacts of extreme heat events, several countries (mainly in Europe and North America) have implemented heat-health warning systems (HHWS) to reduce heat-related morbidity and mortality (Casanueva et al. 2019; Kotharkar and Ghosh 2022). According to recommended methodologies, the development of HHWS should be based on knowledge of cause-effect relationships between temperature and the health of a given population (Kim et al. 2006; Montero et al. 2010). This information can then be used to estimate thresholds to trigger heat warning alerts (McGregor et al. 2015). However, the South African Weather Service (SAWS) currently issues heat warnings using city/town-specific absolute threshold values that are not associated with a negative human response (SAWS 2017).
Although recent South African studies have found strong associations between hot days and mortality especially in children and older adults (Wichmann 2017; Scovronick et al. 2018), these analyses were not restricted to summer months to model heat effects only. Furthermore, the methods used in these studies did not account for population size, which is an important confounder considering that previous studies show heat extremes often have substantially higher impacts when they occur in highly populated areas (Chebana et al. 2013; Harrington and Otto 2018).
Stakeholder participation at local level is necessary to ensure sustainability and effectiveness of HHWS (Climate-ADAPT 2023). In South Africa, there are three tiers of government, namely, national, provincial, and local. Local government comprises 52 districts nationally, and this administrative level is responsible for coordinating development and service delivery. The South African Heat Health Guidelines acknowledge that district municipalities play a crucial role in reducing the burden of disease due to heat exposure (Department of Health 2020). Therefore, districts should be incorporated in the design and implementation heat health action plans such as HHWSs.
Here, we used distributed lag nonlinear models (DLNM) using quasi-Poisson regression models to identify the most statistically significant temperature metric between maximum and minimum temperature and diurnal temperature range (DTR) while adjusting for population in each of the 52 districts in South Africa. We further estimated district-level heat thresholds for the most statistically significant temperature metric. This study enables recommendations for an appropriate exposure metric and the associated location-specific thresholds to issue heat alerts to contribute towards the development of a health-outcome evidenced HHWS for South Africa.
Methods
Mortality and population data
Statistics South Africa provided the mortality data for 1997–2013, which contains all deaths registered and collated through the South African civil registration system maintained by the Department of Home Affairs. A data quality assessment conducted by Statistics South Africa estimated that adult (15 years and older) death registrations were ~ 89% complete early on in the study period, increasing to ~ 94% completion by 2013, while the child death records had not been sufficiently reported (Stats SA 2014; Scovronick et al. 2018). Records with missing or incomplete information about location of death (district) and/or date of death were excluded from the dataset used for analysis. This study used all-cause mortality similar to most epidemiological studies because temperature-related mortality is often misclassified and underestimated (Hajat and Kosatky 2010; Alahmad et al. 2019). District-level population estimates for the study period were also obtained from Statistics South Africa.
Temperature data
Data for maximum and minimum temperature were provided by the National Oceanographic and Atmospheric Administration (NOAA) and South Africa’s Agricultural Research Council (ARC). This dataset comprised daily minimum and maximum temperatures for each of the country’s 52 district municipalities. The NOAA dataset comprised daily data covering 30 district municipalities, while the ARC dataset covered 50 districts except the City of Johannesburg and Nelson Mandela Bay. Using the most complete datasets from the two sources, the final dataset consisted of temperature data from ARC for 34 district municipalities and NOAA data from 18 district municipalities. In-depth quality control was conducted on the dataset to exclude invalid values resulting from instrument error or human error during data uploading and capturing. The collation, quality control procedures, and processing of the temperature dataset are described in more detail in Scovronick et al. (2018). Daily DTR was calculated as the difference between maximum and minimum temperature.
Heat-related mortality studies often limit temperature data to summer months because this excludes the effects of cold temperature (Li et al. 2012; Basu 2009). Therefore, this study limits its temperature data from October to March, which are considered “summer” months in South Africa due to the warmer temperatures compared to the rest of the year.
Statistical analysis
To explore the association between maximum temperature and minimum temperature and DTR on all-cause mortality, a distributed lag nonlinear model (DLNM) using a quasi-Poisson regression model was implemented to express the nonlinear exposure-lag-response relationship. This was performed separately for each district due to heterogeneity between the locations. The model was adjusted to account for the population of each district, and results are reported as IRR (incidence risk ratio) per 10,000 people. The R package “dlnm” was used to carry out the DLNM analysis (Gasparrini 2011).
To determine the threshold values for the significant temperature metrics for each district, threshold regression was used. Threshold regression models are a class of models where the predictors are believed to impact the outcome at different change points or thresholds. Threshold regression extends linear regression to allow coefficients to vary across different regions (Fong et al. 2017). These regions are identified as either being above or below a threshold value. The threshold parameter can be thought of as a change point, and the model provides an easy to interpret method of describing nonlinear relationships between an outcome and predictors (Fong et al. 2017). A model is fitted to obtain an estimate of the threshold and the coefficients on either side of it. The two regions are defined by a threshold value γ with (Gonzalo and Pitarakis 2002)
where \({y}_{t}\) is the dependent variable, \({x}_{t}\) is a \(1\times {\text{k}}\) vector of covariates, \(\beta\) is a \(k\times 1\) vector of region-invariant parameters, \({\varepsilon }_{t}\) is an IID error with mean 0 and variance \({\sigma }^{2}\), \({z}_{t}\) is a vector of exogenous variables with region-specific coefficient vectors \({\delta }_{1}\) and \({\delta }_{2}\), and \({\omega }_{t}\) is a threshold variable that may be one of the variables in \({x}_{t}\) or \({z}_{t}\). The conditional least squares function is used to estimate the parameters of the threshold regression model for each district. Stata version 15.1 was used for the threshold regression analysis (StataCorp 2017).
Results
Descriptive statistics
The descriptive statistics of mortality and temperature metrics are illustrated in Supplementary Tables S1. Total warm-season mortality in South Africa from 1997 to 2013 was 4,066,276. As illustrated in Table S1, the eThekwini district (number 19) had the highest number of reported deaths for all causes (n = 284,598), and the Central Karoo district (number 8) recorded the lowest number of deaths (n = 6547). Both the highest maximum and lowest minimum temperatures of 47.3 and 0.84 °C, respectively, were observed in districts of KwaZulu-Natal province across all study years.
DLNM
Maximum temperature was the most statistically significant temperature metric in 40 (77%) districts out 52 (Table 1). A majority of the districts showed a significant association (p < 0.05) with maximum temperature. Minimum temperature was second (7 districts, 13%) followed by DTR (3 districts, 6%). Maximum temperature was associated with increased risk of mortality per 10,000 people ranging from 3 to 164% (IRR = 1.03, coefficient = 0.03, 95% CI = − 0.93–0.98, not statistically significant and IRR = 2.64, coefficient = 0.97, 95% CI = − 31.69–33.63, not statistically significant), respectively. However, three district municipalities, namely, Buffalo City (Eastern Cape), Cape Winelands (Western Cape), and Ekurhuleni (Gauteng), showed that max temperature led to a reduction of 26%, 5%, and 6% in risk of mortality per 10,000 people, respectively.
Threshold regression
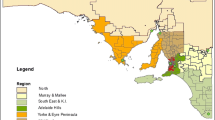
Maximum temperature was found to be the most important predictor of mortality. Threshold regression was used to determine district-level threshold values for maximum temperature during the summer months, above which daily mortality increases. The spatial distribution of the thresholds varies according to the climate zones across the country (Fig. 1). It resembles the distribution of climatic regions defined by the Köppen-Geiger classification system (Fig. 2). This is one of the most widely used approaches to classify regions into zones based on temperature and precipitation characteristics. The results of the threshold regression for each district are presented in Table S2. Figure 1 shows that, on average, districts located in the hot arid interior provinces of the Northern Cape and the North West had the highest thresholds (provincial average of 33.31 and 33.05) compared to districts located in the temperate interior (Mpumalanga province) and along the coast (Eastern Cape province) 27.92 and 26.37, respectively. These are among the hottest provinces in the country, and they have experienced several significant heatwaves that have impacted human health in recent years (Marue 2016; Mbokodo et al. 2020; van der Walt and Fitchett 2021).

Maximum thresholds (in °C) for mortality for each of the 52 districts in South Africa estimated from threshold regression

a Köppen-Geiger map of the climate zones in South Africa (Beck, Zimmermann et al. 2018). b Map depicting provinces of South Africa
Discussion
Our aim was to identify which temperature metric is the most important predictor of mortality during summer months. This metric can then be considered as an exposure outcome towards the development of a HHWS for South Africa. The temperature metrics included in this study were maximum and minimum temperature and DTR. We also calculated district-level thresholds for the most significant metric that can be used to issue heat warnings. An important component of HHWS involves choosing a temperature metric that is most appropriate in terms of prediction for adverse heat-related health outcomes. However, the SAWS definition of extreme heat events does not incorporate the association between an exposure metric and a health outcome. Therefore, our study aimed to provide recommendations based on heat-health evidence.
Based on our analysis of the relationship between three daily temperature metrics and mortality during summer months, maximum temperature was found to be the best predictor of mortality across the country. Daily maximum represents the maximum thermal stress experienced by the human body and is therefore commonly used as an exposure metric in heat-mortality studies (Tan et al. 2007). This has been corroborated by studies that have found strong associations between maximum temperature and mortality (Davis et al. 2016). For example, a study conducted in India, a country with hot summers that has experienced several fatal heatwaves over the years, found high correlations between daily mortality and maximum temperatures during the hottest months of the year (April, May, and June) and all were statistically significant (Azhar et al. 2014). Also, a study in Australia, a region with a climate similar to South Africa, found that maximum temperature had a significant effect on mortality with a 10 °C increase in daily maximum temperature resulting in an increase of 4.5–12.1% in mortality (Vaneckova et al. 2008). In addition, operational HHWS in several countries use the exceedance of a maximum temperature threshold to issue heat alerts (Nogueira 2005; Basarin et al. 2020; NHS 2020; Wu et al. 2020). This supports the feasibility of recommending maximum temperature as a meteorological index for high temperature warnings in South Africa.
We also found spatial variation in the distribution of maximum temperature thresholds related to the climate conditions in local regions. Provinces in hot arid regions experienced high district-level average maximum temperature thresholds. Findings from previous studies suggest that populations living in hotter climates cope better in extreme heat and therefore temperature thresholds for heat-related mortality are higher for warm regions compared to cooler areas (Kenny et al. 2019; Kalkstein et al. 2011). An analysis of daily summer temperatures and mortality across the ten government regions of England and Wales found that regions with hotter climates had higher thresholds for mean temperature compared to colder climates (Armstrong et al. 2011). In a study across seven regions in China, minimum mortality temperature was found to be higher in regions with warmer climates compared to those with cooler climates (Ma et al. 2015). More evidence of the geographical variation of the temperature-mortality relationship was found in a multi-country study where heat thresholds were higher in cities with hotter summers (McMichael et al. 2008).
The findings of our study relating to the high maximum temperature thresholds for hot regions indicate population adaptation to local climate. Previous studies conducted across the world also reported similar observations that support this hypothesis. For example, the national heat index threshold of 40.1 °C used by the US National Weather Service to issue heat alerts was found to be ineffective in the desert communities of California. The threshold was regularly exceeded in these communities, but residents are well adapted to extreme heat (Guirguis et al. 2014). In Croatia, the analysis of mortality and meteorological data over a 26-year period found that thresholds for maximum temperature were higher in continental parts of the country compared to cooler, coastal areas (Zaninović and Matzarakis 2014). Another study that compared temperature and mortality associations in the UK and Australia found that relative risk attributed to the exceedance of heat thresholds was lower in Australian cities than in the UK (Vardoulakis et al. 2014). Some of the suggested reasons were the physiological acclimatization and behavioral adaptation of the population of Australia due to the warmer climate (Vardoulakis et al. 2014).
The World Meteorological Organization and World Health Organization guidance on the development of HHWS acknowledges that there is no preferred meteorological variable or exposure metric that is recommended for use in HHWS (McGregor et al. 2015). Indicators that are used in operational HHWS across the world include maximum temperature, minimum temperature, mean temperature, apparent temperature, and air mass (calculated by combining air temperature, dewpoint temperature, total cloud cover, sea level pressure, windspeed, and wind direction). However, for increased effectiveness, heat indicators in HHWS should be based on variables that are easy to forecast with a certain level of confidence to ensure accurate prediction of heat events. According to Pascal et al. (2006), temperature forecasts up to 5 days in advance are within the acceptance level of confidence for heat early warnings. SAWS can forecast minimum and maximum temperature up to 3 days in advance with a high level of confidence; therefore, our study used maximum and minimum temperature and DTR as input variables. For future research, we recommend that the performance of maximum temperature on forecasted data should also be tested to ensure its effectiveness in a HHWS.
Several limitations were considered during this study. Firstly, we used all-cause mortality and not exposure to excessive natural heat (ICD-10 code X30). Although using heat-specific death would increase reliability of results, heat-related deaths are often misclassified as deaths due to heart attacks, cardiovascular disease, and respiratory disease (Basu and Samet 2002). According to the mortality dataset, there were about 10 deaths per year recorded as being heat-related across South Africa from 1997 to 2013 which suggests gross underreporting (Stats SA 2014). The study also did not account for air pollution (particles, ozone, nitrogen dioxide, sulfur dioxide, and carbon monoxide), rainfall, or humidity which are potential confounder of the temperature–mortality relationship. High temperatures have been associated with increased levels of air pollution which also increases risk of mortality (Hu et al. 2022). Therefore, our results could have potentially overestimated the effect of heat on mortality due to the lack of adjustment for air pollution variables. Lastly, our study used mortality as a health outcome; however, hospitalizations (including emergency department visits) and ambulance callouts have been found to capture heat-related health outcomes more accurately (Bishop-Williams et al. 2015; Li et al. 2015). Unfortunately, these data are difficult to obtain for South Africa due to controlled access to data, the slow pace of migration from hard copy record keeping to computerized records, and challenges with data quality.
Conclusions
Effective and efficient HHWS require that threshold values be informed by epidemiological studies assessing temperature–mortality relationship. The results of our analysis suggest that the development and implementation of HHWS should be country specific, taking the local climate into account in order to reduce heat-related mortality and morbidity. This study investigated which temperature index (maximum and minimum temperature or a combination of both) has the potential to be incorporated into a HHWS design that takes associations with a health outcome (in this case, mortality) into consideration. Maximum temperature was the most robust predictor of all-cause mortality, and thresholds varied across the country depending on the local climate. Based on the findings, this study recommends a HHWS incorporating district-level maximum temperature thresholds to issue heat alerts.
Data Availability
The data that support the findings of this study are available from Statistics South Africa, the National Oceanographic and Atmospheric Administration (NOAA), and South Africa’s Agricultural Research Council (ARC) but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the authors upon reasonable request and with permission of data custodians.
References
AfricaNews. 2023. https://www.africanews.com/2023/01/25/heatwave-kills-eight-in-south-africa-govt/. Accessed 22 Oct 2023
Alahmad B, Shakarchi A, Alseaidan M, Fox M (2019) The effects of temperature on short-term mortality risk in Kuwait: a time-series analysis. Environ Res 171:278–284
Armstrong BG, Chalabi Z, Fenn B, Hajat S, Kovats S, Milojevic Ai, Wilkinson P (2011) Association of mortality with high temperatures in a temperate climate: England and Wales. J Epidemiol Community Health 65:340–345
Azhar GS, Mavalankar D, Nori-Sarma A, Rajiva A, Dutta P, Jaiswal A, Sheffield P, Knowlton K, Hess JJ (2014) Heat-related mortality in India: excess all-cause mortality associated with the 2010 Ahmedabad heat wave. PLoS ONE 9:e91831
Azhar, Gulrez Shah, Dileep Mavalankar, Amruta Nori-Sarma, Ajit Rajiva, Priya Dutta, Anjali Jaiswal, Perry Sheffield, Kim Knowlton, Jeremy J Hess, and Ahmedabad HeatClimate Study Group. 2014. 'Heat-related mortality in India: excess all-cause mortality associated with the 2010 Ahmedabad heat wave', PloS one, 9
Basarin B, Lukić T, Matzarakis A (2020) Review of biometeorology of heatwaves and warm extremes in Europe. Atmosphere 11:1276
Basu R (2009) High ambient temperature and mortality: a review of epidemiologic studies from 2001 to 2008. Environ Health 8:40
Basu R, Samet JM (2002) Relation between elevated ambient temperature and mortality: a review of the epidemiologic evidence. Epidemiol Rev 24(2):190–202
Beck HE, Zimmermann NE, McVicar TR , Vergopolan N, Berg A, Wood EF (2018) Present and future Köppen-Geiger climate classification maps at 1-km resolution. Sci Data 5(1):1–12
Beck HE, Zimmermann NE, McVicar TR , Vergopolan N, Berg A, Wood EF (2020) Publisher Correction: Present and future Köppen-Geiger climate classification maps at 1-km resolution. Sci Data 7
Bishop-Williams KE, Berke O, Pearl DL, Kelton DF (2015) A spatial analysis of heat stress related emergency room visits in rural Southern Ontario during heat waves. BMC Emerg Med 15:1–9
Campbell S, Remenyi TA, White CJ, Johnston FH (2018) Heatwave and health impact research: a global review. Health Place 53:210–218
Casanueva A, Burgstall A, Kotlarski S, Messeri A, Morabito M, Flouris AD, Nybo L, Spirig C, Schwierz C (2019) Overview of existing heat-health warning systems in Europe. Int J Environ Res Public Health 16:2657
Chebana F, Martel B, Gosselin P, Giroux J-X, Ouarda TBMJ (2013) A general and flexible methodology to define thresholds for heat health watch and warning systems, applied to the province of Québec (Canada). Int J Biometeorol 57:631–644
Christoph S, Gerd J (2004) Hot news from summer 2003. Nature 432:559–560
Climate-ADAPT. 2023. 'Establishment of early warning systems', The European Climate Adaptation Platform Climate-ADAPT. Available athttps://climate-adapt.eea.europa.eu/en/metadata/adaptation-options/establishment-of-early-warning-systems
Coumou D, Rahmstorf S (2012) A decade of weather extremes. Nat Clim Chang 2:491–496
Davis RE, Hondula DM, Patel AP (2016) Temperature observation time and type influence estimates of heat-related mortality in seven US cities. Environ Health Perspect 124:795–804
Department of Health. 2020. 'National Heat Health Action Guidelines for South Africa ', National heat health action guidelines for South Africa developed by the National Department of Health. Available athttps://www.health.gov.za/wp-content/uploads/2022/06/National-Heat-Health-Action-Guidelines.pdf
Ebi KL, Vanos J, Baldwin JW, Bell JE, Hondula DM, Errett NA, Hayes K, Reid CE, Saha S, Spector J (2021) Extreme weather and climate change: population health and health system implications. Annu Rev Public Health 42:293–315
Fong Y, Huang Y, Gilbert PB, Permar SR (2017) chngpt: threshold regression model estimation and inference. BMC Bioinformatics 18:1–7
Fouillet A, Rey G, Laurent F, Pavillon G, Bellec S, Guihenneuc-Jouyaux C, Clavel J, Jougla E, Hémon D (2006) Excess mortality related to the August 2003 heat wave in France. Int Arch Occup Environ Health 80:16–24
Gasparrini A (2011) Distributed lag linear and non-linear models in R: the package dlnm. J Stat Softw 43:1
Gonzalo J, Pitarakis J-Y (2002) Estimation and model selection based inference in single and multiple threshold models. J Econ 110:319–352
Grumm RH (2011) The central European and Russian heat event of July–August 2010. Bull Am Meteor Soc 92:1285–1296
Guirguis K, Gershunov A, Tardy A, Basu R (2014) The impact of recent heat waves on human health in California. J Appl Meteorol Climatol 53:3–19
Hajat S, Kosatky T (2010) Heat-related mortality: a review and exploration of heterogeneity. J Epidemiol Community Health 64:753–760
Harrington Luke J, Otto FEL (2018) Changing population dynamics and uneven temperature emergence combine to exacerbate regional exposure to heat extremes under 15 C and 2 C of warming. Environ Res Lett 13:034011
Hoag H (2014) Russian summer tops ‘universal’heatwave index. Nature 16(4):636
Hu X, Han W, Wang Y, Aunan K, Pan X, Huang J, Li G (2022) Does air pollution modify temperature-related mortality? A systematic review and meta-analysis. Environ Res 210:112898
Kalkstein LS, Greene S, Mills DM, Samenow J (2011) An evaluation of the progress in reducing heat-related human mortality in major US cities. Nat Hazards 56:113–129
Kenny GP, Flouris AD, Yagouti A, Notley SR (2019) Towards establishing evidence-based guidelines on maximum indoor temperatures during hot weather in temperate continental climates. Temperature 6:11–36
Kim Ho, Ha J-S, Park J (2006) High temperature, heat index, and mortality in 6 major cities in South Korea. Arch Environ Occup Health 61:265–270
Knowlton K, Rotkin-Ellman M, King G, Margolis HG, Smith D, Solomon G, Trent R, English P (2008) The 2006 California heat wave: impacts on hospitalizations and emergency department visits. Environ Health Perspect 117:61–67
Knowlton K, Chen LJ, Kalkstein L (2012) Killer summer heat: projected death toll from rising temperatures in America due to climate change. NRDC Issue Brief
Kotharkar R, Ghosh A (2022) Progress in extreme heat management and warning systems: a systematic review of heat-health action plans (1995–2020). Sustain Cities Soc 76:103487
Li Bo, Sain S, Mearns LO, Anderson HA, Kovats S, Ebi KL, Bekkedal MYV, Kanarek MS, Patz JA (2012) ’The impact of extreme heat on morbidity in Milwaukee. Wis Clim Chang 110:959–976
Li M, Gu S, Bi P, Yang J, Liu Q (2015) Heat waves and morbidity: current knowledge and further direction-a comprehensive literature review. Int J Environ Res Public Health 12:5256–5283
Luterbacher J, Dietrich D, Xoplaki E, Grosjean M, Wanner H (2004) European seasonal and annual temperature variability, trends, and extremes since 1500. Science 303:1499–1503
Ma W, Wang L, Lin H, Liu T, Zhang Y, Rutherford S, Luo Y, Zeng W, Zhang Y, Wang X (2015) The temperature–mortality relationship in China: an analysis from 66 Chinese communities. Environ Res 137:72–77
Marue, Katlego. 2016. 'Northern Cape heat wave claims at least 17. Available at https://health-e.org.za/2016/02/04/northern-cape-heat-wave-claims-at-least-17/. Accessed 17 September 2020
Mazdiyasni O, AghaKouchak A, Davis SJ, Madadgar S, Mehran A, Ragno E, Sadegh M, Sengupta A, Ghosh S, Dhanya CT (2017) Increasing probability of mortality during Indian heat waves. Sci Adv 3:e1700066
Mbokodo I, Bopape M-J, Chikoore H, Engelbrecht F, Nethengwe N (2020) Heatwaves in the future warmer climate of South Africa. Atmosphere 11:712
McGregor GR, Bessemoulin P, Ebi K, Menne B (2015) Heatwaves and health: guidance on warning-system development. World Meteorological Organization World Health Organization. Available at https://ghhin.org/wp-content/uploads/WMO_WHO_Heat_Health_Guidance_2015.pdf. Accessed 17 Jul 2020
McMichael AJ, Paul Wilkinson R, Kovats S, Pattenden S, Hajat S, Armstrong B, Vajanapoom N, Niciu EM, Mahomed H, Kingkeow C (2008) International study of temperature, heat and urban mortality: the ‘ISOTHURM’project. Int J Epidemiol 37:1121–1131
Montero JC, Mirón IJ, Criado JJ, Linares C, Díaz J (2010) Comparison between two methods of defining heat waves: a retrospective study in Castile-La Mancha (Spain). Sci Total Environ 408:1544–1550
NHS. 2020. 'Heatwave plan for England. Available at https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/888668/Heatwave_plan_for_England_2020.pdf. Accessed 21 August 2020
Nitschke M, Tucker GR, Hansen AL, Williams S, Zhang Y, Bi P (2011) Impact of two recent extreme heat episodes on morbidity and mortality in Adelaide, South Australia: a case-series analysis. Environ Health 10:42
Nogueira PJ (2005) Examples of heat health warning systems: Lisbon’s ICARO’s surveillance system, summer of 2003. Extreme weather events and public health responses 141–159
Pascal M, Laaidi K, Ledrans M, Baffert E, Caserio-Schönemann C, Le Tertre A, Manach J, Medina S, Rudant J, Empereur-Bissonnet P (2006) France’s heat health watch warning system. Int J Biometeorol 50:144–153
Robine J-M, Siu Lan K, Cheung SL, Roy HV, Oyen CG, Michel J-P, Herrmann FR (2008) Death toll exceeded 70,000 in Europe during the summer of 2003. CR Biol 331:171–178
SAWS. 2017. South African Weather Service. http://www.weathersa.co.za/learning/weather-questions/346-what-is-a-heat-wave. Accessed 17 Mar 2020
Scovronick N, Sera F, Acquaotta F, Garzena D, Fratianni S, Wright CY, Gasparrini A (2018) The association between ambient temperature and mortality in South Africa: a time-series analysis. Environ Res 161:229–235
StataCorp (2017) StataCorp. 2001. Statistical Software: Release 15.0. College Station, TX: Stata Corporation
Stats SA. 2014. 'Statistics South Africa statistical release: mortality and causes of death in South Africa, 2014: Findings from death notification. Available http://ipasa.co.za/wp-content/uploads/2016/03/Stats-SA-mortality-and-death-causes-in-south-africa-2014-findings-from-death-notification.pdf. Accessed 29 May 2019
Tan J, Zheng Y, Song G, Kalkstein LS, Kalkstein AJ, Tang Xu (2007) Heat wave impacts on mortality in Shanghai, 1998 and 2003. Int J Biometeorol 51:193–200
'The European Climate Adaptation Platform Climate-ADAPT, https://climate-adapt.eea.europa.eu/en/mission/knowledge-and-data/regional-adaptation-support-tool/step-2-assessing-climate-change-risks-and-vulnerabilities'
Trigo RM, Ramos AM, Nogueira PJ, Santos FD, Garcia-Herrera R, Gouveia C, Santo FE (2009) Evaluating the impact of extreme temperature based indices in the 2003 heatwave excessive mortality in Portugal. Environ Sci Policy 12:844–854
van der Walt AJ, Fitchett JM (2021) Exploring extreme warm temperature trends in South Africa: 1960–2016. Theoret Appl Climatol 143:1341–1360
Vaneckova P, Beggs PJ, de Dear RJ, McCracken KWJ (2008) Effect of temperature on mortality during the six warmer months in Sydney, Australia, between 1993 and 2004. Environ Res 108:361–369
Vardoulakis S, Dear K, Hajat S, Heaviside C, Eggen B, McMichael AJ (2014) Comparative assessment of the effects of climate change on heat-and cold-related mortality in the United Kingdom and Australia. Environ Health Perspect 122:1285
Wichmann J (2017) Heat effects of ambient apparent temperature on all-cause mortality in Cape Town, Durban and Johannesburg, South Africa: 2006–2010. Sci Total Environ 587–588:266–272
Wu Y, Wang X, Jingyan Wu, Wang R, Yang S (2020) Performance of heat-health warning systems in Shanghai evaluated by using local heat-related illness data. Sci Total Environ 715:136883
Zaninović K, Matzarakis A (2014) Impact of heat waves on mortality in Croatia. Int J Biometeorol 58:1135–1145
Zhao Qi, Pei Yu, Mahendran R, Huang W, Gao Y, Yang Z, Ye T, Wen Bo, Yao Wu, Li S (2022) Global climate change and human health: Pathways and possible solutions. Eco-Environ Health 1:53–62
Funding
Open access funding provided by South African Medical Research Council. TK and CYW receive research funding from the SAMRC. TK also receives funding from the National Research Foundation (NRF) of South Africa.
Author information
Authors and Affiliations
Contributions
TK, CYW, and MG were involved in developing the methodology. TK and NA were involved in data analysis. TK wrote the first draft of the manuscript. All authors contributed to the writing of subsequent versions of the manuscript and approved the final version.
Corresponding author
Ethics declarations
Ethics approval
Research ethics clearance was granted by the Research Ethics Committee of the Faculty of Natural and Agricultural Sciences at the University of Pretoria, Reference Number: EC180126-169.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kapwata, T., Abdelatif, N., Scovronick, N. et al. Identifying heat thresholds for South Africa towards the development of a heat-health warning system. Int J Biometeorol 68, 381–392 (2024). https://doi.org/10.1007/s00484-023-02596-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00484-023-02596-z