
Abstract
Purpose
To evaluate the uptake and effect of RENEW, a 12-week exercise referral programme for young adult cancer survivors delivered by Trekstock, a UK-based cancer charity.
Methods
The RENEW programme provides one-to-one individually tailored support from a level-4 cancer-rehabilitation-qualified gym instructor, free gym membership and access to information resources online. Objective and self-report data on cardiorespiratory function, strength, body composition, fatigue, sleep quality and general health-related quality of life (HRQoL) was collected from participants before the programme (week 0), immediately after (week 12) and 1 month later (week 16).
Results
Forty-eight young adults (83% female; mean age, 29 years) with a history of cancer took part within the 12-week programme and completed the evaluation measures. Physical activity (PA) levels significantly increased following the programme and remained raised at follow-up. Improvements in physical function were significant: peak expiratory flow (mean change, 30.96, p = 0.003), sit-and-reach test (mean change, 6.55 ± 4.54, p < 0.0001), and 6-mine-walk test (mean change, 0.12 ± 0.04, p < 0.0001). No significant changes in BMI, weight or muscle mass were observed. Improvements in fatigue, sleep and HRQoL were observed across the programme and at follow-up (mean change, weeks 0–16; 8.04 ± 1.49 p < 0.01; 1.05 ± 0.49 p < 0.05; and − 0.9 ± 0.46 p = 0.051, respectively). Changes in self-efficacy to exercise and motivations to exercise were not observed at 12 weeks or at follow-up.
Conclusions
Results suggest that the RENEW exercise referral programme has a positive impact upon some domains of physical function and well-being among young adult cancer survivors.
Implication for cancer survivors
Exercise referral programmes delivered by charity organisations are one means by which PA behaviour change support may be widely disseminated to young adult cancer survivors. Health professionals and charitable bodies specialising in the care of young adults with cancer should look to address factors which prevent engagement and uptake of ‘real-world’ PA interventions such as the RENEW programme.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
Systematic reviews and meta-analyses of high-quality randomised controlled trials demonstrate physical activity (PA) has a positive effect on a number of clinical, physical and psychosocial outcomes among cancer survivors [1,2,3]. Given the benefits of exercise for individuals with cancer, the World Cancer Research Fund (WCRF), American Cancer Society and American College of Sports Medicine (ACSM) recommend that cancer survivors reduce their sedentary time and aim to accumulate 150 min/week of moderate-intensity aerobic exercise (or 75 min/week of vigorous intensity aerobic exercise) and two strength training sessions per week. However, at present, the vast majority of studies have been conducted in controlled clinical environments (hospitals/academic institutions) among cancer survivors over the age of 50 diagnosed with breast, prostate or colorectal cancer [4, 5]. There is increasing recognition that PA plays a role in reducing cancer recurrence risk and mortality among young adult cancer survivors [4, 6]. and that efforts need to be made to translate PA interventions into real-world practice [7].
The term ‘young adult cancer survivor’ typically refers to an individual who is 18–39 years of age who has had a diagnosis of cancer [8]. This age range is distinct from a physiological and psychosocial perspective: young adults have passed puberty but have not yet experienced the effects of hormonal decline, immune response deterioration or organ dysfunction associated with older age and chronic health conditions [9]. Given that young adult cancer survivors will experience many decades more of survivorship than older adults, it has been widely acknowledged that sustainable and practical evidence-based survivorship programmes for young adult cancer survivors are required [10, 11].
Trekstock is a London-based charity which provides information and support programmes to help cancer survivors in their 20s and 30s deal with the emotional and physical impact of cancer. Based upon the evidence that physical activity is a means to enhance physical and psychosocial outcomes among individuals with cancer, Trekstock programmes predominantly centre around physical activity promotion. To address young adult cancer survivors’ need and desire for structured physical activity support [12, 13], Trekstock developed a 12-week exercise programme (RENEW) consisting of personal training support from a qualified level-4 cancer-rehabilitation instructor within a community-based setting, free gym membership and support materials available online via the Trekstock website. The delivery of an individually tailored yet structured physical activity support programme by a charitable organisation in a community-based gym setting is novel and addresses young adult cancer survivors need for PA interventions which foster independence and autonomy away from primary treatment centres [13].
The purpose of this evaluation is to investigate the effect of the RENEW exercise programme upon the health and well-being of young adult cancer survivors. The primary objective was to assess rates of uptake of and adherence to the programme. The secondary objective was to determine the effect of the programme on the (i) physical health and function, (ii) quality of life, sleep and fatigue, (iii) PA behaviour; and (iv) self-efficacy for, and motivation to, exercise.
Methods
Participants and recruitment
Participants were service users of Trekstock defined as young adults between the age of 18 and 39 years who have had a cancer diagnosis at any point within their lifetime. Between August 2018 and May 2019, advertisements for the RENEW programme were shared through the Trekstock network and in London-based cancer centres specialising in the treatment and care of young adults. If interested in taking part in the RENEW programme, participants were asked to complete a self-referral form via the Trekstock website. Trekstock then linked the participant to a level-4 cancer-rehabilitation personal trainer to commence the programme at a time convenient to themselves. To ensure safety of delivery, if a participant was in active cancer treatment, clearance from their medical team was required before they were linked with a personal trainer.
RENEW exercise programme
Trekstock linked each participant to a level-4 cancer-rehabilitation personal trainer at the Central YMCA gym in London. Participants met with the personal trainer at 4 time points across the 12-week programme. At baseline (week 0, initial meeting), trainers worked with each participant to develop a tailored programme based on their age, cancer type and any comorbidities. Hour-long personal training sessions were held at time points selected by the participants and trainers. All sessions began with a warm-up, followed by aerobic and strength training exercise before a cool-down. The total cost incurred by Trekstock to deliver the programme in partnership with YMCA was £200 per person.
Evaluation design
A quasi-experimental pre- and post-test design was adopted to evaluate the programme. It was not compulsory for young adults with cancer who were taking part in the RENEW programme to take part in the evaluation. Self-report data on physical activity behaviour, health related quality of life, sleep, fatigue, motivation and self-efficacy to exercise were collected at 3 time points pre-programme (baseline, week 0), immediately following delivery of the exercise programme (T1, week 12) and 1 month later (T2, week 16). Objective measures of physical health were taken by the personal trainer at baseline (week 0) and post-programme (T1, week 12). There was no incentive or compensation provided to participants for taking part in the programme or for completing the evaluation measures. Ethical approval for the evaluation was granted by the Queen Mary University Research Ethics Committee (reference: QMREC2018/48/006).
Measures
Demographic and health characteristics
Self-report data on age, ethnicity and educational/employment status was collected alongside data on current health status and cancer history (diagnosis, age at diagnosis, treatment received and current treatment status). Weight, height, resting blood pressure, resting heart rate, body fat mass and muscle mass data were collected by personal trainers who deliver the RENEW programme at baseline and post-programme. Body fat mass and muscle mass were assessed using bioelectrical impedance analysis (YMCA, body composition scanner).
Functional health
Data on peak expiratory flow (PEF), sit-and-reach performance and 6-min walk test (6MWT) performance were collected by personal trainers who deliver the RENEW programme. These are valid, reliable field based measures of lung function, flexibility and cardiorespiratory fitness [14, 15]. The 6MWT is considered a valid measure of cardiorespiratory fitness, correlation coefficient = 0.67 between 6MWT and oxygen consumption (VO2) peak [16].
Physical activity and sedentary behaviour
The Godin Leisure Time Exercise Questionnaire (GLTEQ) was used to assess physical activity. Participants were asked to report the frequency and duration of mild, moderate and strenuous exercise they engage in over typical week. The GLTEQ has been used in similar studies of TYA cancer survivors [17, 18] and has previously demonstrated reliability and validity within the oncology research setting [19]. A single item from the International Physical Activity Questionnaire (IPAQ) regarding the amount of time spent sitting down in the last week and two items taken from the National Health and Nutrition Examination Survey (NHANES) [20] were used to assess computer and television viewing as proxy measures of sedentary behaviour.
Self-efficacy and self-determined motivation to exercise
Physical activity self-efficacy was measured using the Self-Efficacy for Exercise (SEE) scale [21] a revision of McAuley’s (1990) self-efficacy barriers to exercise measure, which is made up of 13 items relating to the ability to continue exercising in the face of barriers to exercise. These were rated on an 11-point scale (0 = not confident, 10 = very confident). The information gathered by this standardised subjective measure is descriptive of participants’ level of confidence to be active with a higher score indicating greater self-efficacy. The Behavioural Regulation in Exercise Questionnaire (BREQ) was used to assess participants’ motivation to exercise [22]. The BREQ2 measures external, introjected, identified and intrinsic forms of regulation of exercise behaviour based on Deci and Ryan’s (1985, 1991) hierarchical model of extrinsic and intrinsic motivation. Each domain of the BREQ was scored on a scale of 1–6 with a high score indicating more dominance of that domain of motivation. Physical activity self-efficacy was measured using the Self-Efficacy for Exercise (SEE) scale [21] which is made up of thirteen items relating to the ability to continue exercising in the face of barriers to exercise. These were rated on an 11-point scale (0 = not confident, 10 = very confident). The information gathered by this standardised subjective measure is descriptive of participants’ level of confidence to be active with a higher score indicating greater self-efficacy. The Behavioural Regulation In Exercise Questionnaire (BREQ) was used to assess participants’ motivation to exercise [22]. The BREQ2 measures external, introjected, identified and intrinsic forms of regulation of exercise behaviour. Each domain of the BREQ was scored on a scale of 1–6 with a high score indicating more dominance of that domain of motivation.
Health-related quality of life
Health-related quality of life (HRQoL) was measured using the five-item EuroQoL-5, a valid (Cronbachs alpha = 0.71) and reliable (r > 0.7) measure of health status commonly used in cancer research [23]. The five-item questionnaire assesses mobility, self-care, daily activities, pain and anxiety/depression on a 5-point Likert scale. Each item is scored to provide a global score ranging from 5 to 25; higher scores indicate poorer HQQoL. The EuroQoL-5 has previously been used among TYA cancer survivors [24].
Fatigue
Fatigue was measured using the Functional Assessment of Chronic Illness Therapy Fatigue (FACIT-F) questionnaire which assess fatigue and its’ impact on physical and psychosocial well-being using 13 items on a 5-point Likert scale. The FACIT-F is widely used among cancer patients [25] and has previously been used in studies of TYA cancer survivors [24]. Scoring of the FACIT-F measure obtains a global score ranging from zero to 52, with a higher score indicating better quality of life [26].
Sleep quality
The Pittsburgh Sleep Quality Index (PSQI) was used to assess seven dimensions of global sleep quality over the previous month. The PSQI is a 19-item self-report measure which identifies subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, sleep medication and daytime function. The PSQI has been validated for use among cancer patients (Cronbach’s α = 0.81) and shows good reliability (r = 0.85) [27]. A combined global sleep score was calculated for each participant ranging from 0 to 21, with greater scores indicating poorer sleep quality.
Statistical analyses
Descriptive statistics (M, SD, n, %) were calculated in order to summarise this data on participant characteristics, programme retention and attrition. Continuous data are presented as means and standard deviation; nominal and ordinal data are presented as frequencies and percentages. All data were checked for distribution and evaluated for normality using the Shapiro-Wilk test. Paired sample t tests were used to examine changes in physical function and health variables from baseline to post-programme. For non-normally distributed variables, non-parametric Wilcoxon Signed Rank tests were used. To examine differences over time repeated measures analyses of variance (rANOVAs) were calculated with factors time (baseline vs. T1 vs. T2). Prior to these analyses, missing data values were imputed using the Markov-Chain Monte-Carlo (MCMC) multiple imputation method. All statistical analysis was conducted using SPSS software (version 25.0) with statistical significance set at p < 0.05.
Results
Rate of uptake and adherence to the programme
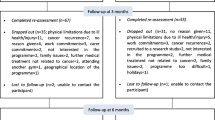
As displayed in Fig. 1, a total of 98 participant referrals to the RENEW programme were made. Of these, 76 proceeded to commence the programme of whom 48 opted to take part in the evaluation. Ten participants who took part in the evaluation did not complete the 12-week programme for reasons listed within the figure. Of the 38 participants who provided data at T1, 15 provided data at T2. No adverse events were recorded during the RENEW programme among either those who chose to take part in the evaluation (n = 48) or those who took part in the programme in general (n = 76).

Flow of participants. Data provided in brackets refers to those who completed the evaluation outcome measures
Participant characteristics
Table 1 summarises participant demographic and health characteristics. The majority of participants (n = 48, mean age, 29 years) were female (83%, n = 40), white (81%, n = 39) and educated to a minimum of a bachelor’s degree (58%, n = 28). The most common cancer diagnosis was lymphoma (18%, n = 9) followed by breast cancer (16%, n = 8) and leukaemia (12%, n = 6). Most had completed their main cancer treatment (66%, n = 32) but were within the first 12 months of survivorship or undergoing active surveillance (37%, n = 18). At baseline, 2 participants were classified as underweight (BMI < 18.5), eight as overweight (BMI 25–30) and seven as obese (BMI > 30).
Effect on physical function and health
Table 2 displays pre- and post-changes in physical function following the RENEW programme. Significant improvements in lung function (mean PEF change, 49.03 ± 8.44; p < 0.000) fitness (6MWT distance, 0.13 ± 0.03; p = 0.00) and flexibility (mean S&R change, 6.67 ± 0.95, p = 0.00) were observed. Overall no significant change was observed in the weight status, fat mass, muscle mass, resting blood pressure or resting HR of participants.
Change in physical activity
Change in physical activity levels are show in Table 3. At baseline, 79% (n = 38) of participants were classed as active (GLTEQ Score > 24). There was a significant increase in GLTEQ score from baseline to post-programme (mean change T0–T1, 18.40 ± 3.25; mean change T0–T2, 22.05 ± 3.34; p < 0.01). Frequency of mild, moderate and vigorous intensity exercise increased across the programme and remained stable at follow-up.
Effect on self-efficacy and motivation to exercise
Changes in self-efficacy and motivation are displayed in Table 4. Overall there was no significant change in self-efficacy or self-determined exercise motivation from baseline to follow-up (p < 0.05). A small decrease in external regulation was observed and small increase in intrinsic regulation was observed across the 12-week programme.
Change in sleep, fatigue and health-related quality of life
Changes in sleep, fatigue and HRQoL are shown in Table 5. There was a significant improvement in participant fatigue scores across the programme from baseline to follow up (mean change T0–T2: 8.04 ± 1.49; p < 0.05). Fatigue scores significantly improved throughout the 12 week intervention period (T0–T1, 10.1 ± 1.45; p < 0.005) and plateaued at follow-up (T1–T2, 2.1 ± 1.27; p = 0.100) HRQoL and sleep quality significantly improved throughout the programme (mean change T0–T2, 0.9 ± 0.46; p < 0.05 and 1.05 ± 0.49; p = 0.051 respectively).
Discussion
There is increasing evidence that remaining active during and after treatment has a number of physical and psychosocial benefits for cancer patients and survivors. However, there are very few tailored interventions available to support young adult cancer survivors aged between 18 and 39 years to either increase or maintain their activity levels following a cancer diagnosis. The RENEW programme delivered by Trekstock was found to be effective in improving the PA levels, fitness, physical function, HRQoL, sleep quality and fatigue levels of young adult diagnosed with cancer. Benefits were observed among both cancer patient (those receiving treatment) and survivors (those who had completed treatment).
Interest in programme participation was high with 98 young adults expressing interest in the 9-month recruitment window; 77% of young adults who signed up for the RENEW programme attended at least one exercise session with 61% of these young adults completing the full 12-week programme. This rate of uptake is notably higher than many exercise intervention studies conducted in the hospital setting or academic setting among similar age groups [28, 29]. It is likely that the delivery of the programme by a trusted charity organisation, the ease of the referral process and the guarantee of personally tailored exercise support alongside free gym membership underpinned young adults’ interest in enrolling. However, 22% of young adults who came forward as being interested in the RENEW exercise programme did not initiate the programme; the primary reason for drop out either prior to the programme or during the 12-week RENEW period was illness. Whilst no negative adverse events were recorded during the RENEW programme and the ACSM exercise guidelines state medical assessment for cancer survivors before initiating an exercise programme is unnecessary due to the high benefit/low risk [30], the finding that illness was the primary cause of drop-out reiterates the importance of qualified exercise professionals adapting programmes to suit the health status of each individual cancer patient/survivor. Akin to existing intervention studies within the literature, the majority of individuals who enrolled to the RENEW programme were female, white British and highly educated. This suggests that effort need to be made to ensure that advertisements and access to the RENEW programme reach all young adults with cancer who require support. User engagement studies are currently being carried out to investigate young adult male cancer survivors’ viewpoint of Trekstock services.
The RENEW programme demonstrated a positive impact on the physical activity levels of young adult cancer survivors. Total amount of physical activity and frequency of mild, moderate and vigorous exercise generally increased across the programme duration. This is encouraging and supports the UK National Institute for Health and Care Excellence position that structured exercise referral schemes delivered and developed by qualified professionals (such as L4 Cancer Rehab trainers) can address inactivity among people with chronic disease [31]. Thought towards different models of exercise programme delivery for young adults with cancer, especially those living in rural areas without easy access to gym facilities, is required. Whilst digital interventions conducted among adolescent and young adult cancer survivors have demonstrated promising outcomes, there is currently little evidence of the economic value of implementing digital interventions on a wide-scale in AYA cancer services [32].
Significant improvements were observed in some domains of physical function (lung function, fitness and flexibility). This is promising and reflective of existing data from intervention studies conducted among adolescent and childhood cancer survivors of a similar age [28, 29, 33, 34]. The improvements in chronic fatigue scores, sleep quality and HRQoL are also encouraging and reiterate the benefit of physical activity upon the psychosocial health and well-being of young adults with cancer [35, 36].
Among adult cancer survivors, high self-efficacy to exercise has been found to predict better quality of life, lower levels of cancer-related fatigue and higher exercise intervention adherence [37, 38]. Data from the Wellspring Cancer Exercise Programme in Ontario, Canada demonstrate that self-efficacy to exercise can affect exercise programme outcomes with those who have higher levels of self-efficacy demonstrating greater improvements in HRQoL and fatigue [38]. Participants within this study demonstrated high levels of exercise self-efficacy and motivation to exercise at baseline indicating that the RENEW programme failed to reach those who lack the confidence to engage in or commit to an exercise programme. In accordance with existing research [38], advertising and highlighting the features of the RENEW programme which are known to improve self-efficacy to exercise (e.g. personalised exercise plan, autonomy to choose exercise modality and positive feedback upon progress) may nudge some young adults to engage in the programme. Providing young adults cancer survivors with the opportunity to see other cancer survivors of a similar age who have similar physical limitations complete exercise successfully is a further solution by which young adults with low self-efficacy and motivation to exercise may be better engaged. Data from the evaluation of the Trekstock Meet and Move programme confirm this notion and indicate that 1-day events which provide an opportunity for young adults with cancer to meet others are effective at improving confidence to be active [39].
Strengths and limitations
A major strength of this work is that it is one of very few evaluations of community-based exercise programmes delivered by a charitable organisation which uses objective outcome measures. Despite the strengths of the RENEW evaluation (e.g. prospective repeated measures design, independent data collection and participant retention) several limitations must be noted when interpreting the results of the data presented. First, the generalisability of the results is limited due to the prevalence of highly educated white females within the sample. Secondly, there is a high likelihood that response bias in that young adults who participated in the programme are likely to report different outcomes (specifically for self-efficacy and motivation) than those who elected not to enrol. Although the sample within the study is comparable with other physical activity intervention studies conducted among young adult cancer survivors (e.g. [40]), it is likely that there was inadequate power to detect a significant difference between time-points for some outcome measures.
Implications and future directions
Advancements in the field of exercise oncology have resulted in a growing body of evidence demonstrating physical activity and exercise interventions conducted among cancer survivors have a positive effect. As a result, there are increasing calls from cancer patients, survivors and health professionals for exercise programmes to be translated into community health and fitness settings [4]. Traditionally, participation in exercise oncology research includes rigorous assessment of study eligibility, medical screening, and no participant autonomy regarding the frequency, intensity, type and total duration of physical activity undertaken during the intervention period. Exercise programmes conducted within the community naturally overcome these issues and provide a real-world alternative to clinically delivered exercise interventions. However, such programmes must undergo rigorous evaluation in order to establish the effect of the programme and provide insight towards factors which limit accessibility and benefit. Established principles of knowledge-to-action translation and evaluation frameworks should be applied to better determine features of exercise programmes which make them successful and sustainable [41]. As first crucial step to ensuring community based exercise programmes for young adults with cancer are accessible efforts to make health professionals aware of existing lifestyle resources and exercise programmes should be made [42].
It is important that future work looks to evaluate the dose-response effect of exercise programmes conducted among young adult cancer survivors and establish the optimal number of exercise sessions per week or intensity of exercise required to have benefit. In addition, both cancer patients (those receiving treatment) and survivors (those who had completed treatment) were included within the intervention and grouped within the analyses. Future work should look to evaluate whether the effects of exercise during active cancer treatment differ to the effects observed post-treatment. This would provide some insight on whether early rehabilitation interventions initiated during the active treatment phase lead to better patient outcomes than interventions delivered in the survivorship phase once treatment has ended. To prevent loss-to-follow-up, greater insight towards geographical, psychosocial and socioeconomic determinants of programme uptake and attrition is required alongside studies evaluating the maintenance of PA behaviour change over time.
Conclusion
The findings of the current study provide evidence of the physical and psychological benefits of the RENEW exercise programme delivered by Trekstock. The high uptake and engagement with the programme, combined with the data on patient reported outcomes, support the implementation of the RENEW exercise referral scheme across other cities within the UK. Given the growing body of evidence demonstrating exercise programmes can improve the length and quality of cancer survival [43], reduce co-morbidities associated with cancer treatment and foster resilience among cancer survivors, programmes such as RENEW have the potential to address some of the most pressing issues facing young people living with cancer.
References
Speck RM, Courneya KS, Mâsse LC, Duval S, Schmitz KH (2010) An update of controlled physical activity trials in cancer survivors: a systematic review and meta-analysis. J Cancer Surviv 4(2):87–100
Fong DYT et al (2012) Physical activity for cancer survivors: meta-analysis of randomised controlled trials. BMJ 344
Ballard-Barbash R, Friedenreich CM, Courneya KS, Siddiqi SM, McTiernan A, Alfano CM (2012) Physical activity, biomarkers, and disease outcomes in cancer survivors: a systematic review. J Natl Cancer Inst 104(11):815–840
Wurz A, Daeggelmann J, Albinati N, Kronlund L, Chamorro-Viña C, Culos-Reed SN (2019) Physical activity programs for children diagnosed with cancer: an international environmental scan. Support Care Cancer 27(4):1153–1162
PATEL AV et al (2019) American College of Sports Medicine roundtable report on physical activity, sedentary behavior, and cancer prevention and control. Med Sci Sports Exerc 51(11):2391–2402
Hjorth M, Febbraio MA (2018) Exercise as medicine for survivors of paediatric cancer. Nat Rev Endocrinol 14(9):506–508
Santa Mina D et al (2018) Connecting people with cancer to physical activity and exercise programs: a pathway to create accessibility and engagement. Curr Oncol 25(2)
Barr RD, Ferrari A, Ries L, Whelan J, Bleyer WA (2016) Cancer in adolescents and young adults: a narrative review of the current status and a view of the future. JAMA Pediatr 170(5):495–501
Sender L, Zabokrtsky KB (2015) Adolescent and young adult patients with cancer: a milieu of unique features. Nat Rev Clin Oncol 12(8):465–480
Pugh G, Gravestock HL, Hough RE, King WM, Wardle J, Fisher A (2016) Health behavior change interventions for teenage and young adult cancer survivors: a systematic review. J Adolesc Young Adult Oncol 5(2):91–105
Rabin C, Politi M (2010) Need for health behavior interventions for young adult Cancer survivors. Am J Health Behav 34(1):70–76
Pugh G, Hough RE, Gravestock HL, Jackson SE, Fisher A (2017) The health behavior information needs and preferences of teenage and young adult Cancer survivors. Journal of Adolescent and Young Adult Oncology 6(2):318–326
Pugh G (2017) et al. The lifestyle information and intervention preferences of teenage and young adult cancer survivors: a qualitative study, Cancer Nurs
Schumacher AN et al (2019) Validation of the 6-min walk test for predicting peak VO2 in cancer survivors. Med Sci Sports Exerc 51(2):271–277
Mayorga-Vega D, Merino-Marban R, Viciana J (2014) Criterion-related validity of sit-and-reach tests for estimating hamstring and lumbar extensibility: a meta-analysis. J Sports Sci Med 13(1):1–14
Schmidt K et al (2012) Validity and reproducibility of the 6-minute walk test in cancer patients. Med Sci Sports Exerc 44:188–188
Wright M et al (2013) Physical activity in adolescents following treatment for cancer: influencing factors. Leuk Res Treat 2013:592395
Gilliam MB, Madan-Swain A, Whelan K, Tucker DC, Demark-Wahnefried W, Schwebel DC (2012) Social, demographic, and medical influences on physical activity in child and adolescent cancer survivors. J Pediatr Psychol 37(2):198–208
Amireault S, Godin G, Lacombe J, Sabiston CM (2015) Validation of the Godin-Shephard leisure-time physical activity questionnaire classification coding system using accelerometer assessment among breast cancer survivors. J Cancer Surviv 9(3):532–540
Hagstromer M, Oja P, Sjostrom M (2006) The international physical activity questionnaire (IPAQ): a study of concurrent and construct validity. Public Health Nutr 9(6):755–762
Resnick B, Jenkins LS (2000) Testing the reliability and validity of the self-efficacy for exercise scale. Nurs Res 49(3):154–159
Markland D, Tobin V (2004) A modification to the behavioural regulation in exercise questionnaire to include an assessment of amotivation. J Sport Exerc Psychol 26:191–196
Noyes J, Edwards RT (2011) EQ-5D for the assessment of health-related quality of life and resource allocation in children: a systematic methodological review. Value Health 14(8):1117–1129
Fortmann J, Fisher A, Hough R, Gregory A, Pugh G (2018) Sleep quality, fatigue, and quality of life among teenage and young adult cancer survivors. Journal of Adolescent and Young Adult Oncology 7(4):465–471
Butt Z, Lai JS, Rao D, Heinemann AW, Bill A, Cella D (2013) Measurement of fatigue in cancer, stroke, and HIV using the functional assessment of chronic illness therapy—fatigue (FACIT-F) scale. J Psychosom Res 74(1):64–68
Webster K, Cella D, Yost K (2003) The functional assessment of chronic illness therapy (FACIT) measurement system: properties, applications, and interpretation. Health Qual Life Outcomes 1:79–79
Beck SL et al (2004) Psychometric evaluation of the Pittsburgh sleep quality index in cancer patients. J Pain Symptom Manag 27(2):140–148
Munsie C, Ebert J, Joske D, Ackland T (2019) The benefit of physical activity in adolescent and young adult cancer patients during and after treatment: a systematic review. J Adolesc Young Adult Oncol 8(5):512–524
Brunet J, Wurz A, Shallwani SM (2018) A scoping review of studies exploring physical activity among adolescents and young adults diagnosed with cancer. Psycho-Oncology 27(8):1875–1888
Schmitz KH, Courneya KS, Matthews C, Demark-Wahnefried W, Galvão DA, Pinto BM, Irwin ML, Wolin KY, Segal RJ, Lucia A, Schneider CM, von Gruenigen V, Schwartz AL, American College of Sports Medicine (2010) American College of Sports Medicine roundtable on exercise guidelines for cancer survivors. Med Sci Sports Exerc 42(7):1409–1426
NICE (2014) Physical activity: exercise referral schemes. N.I.o.C.E, London
McCann L, McMillan KA, Pugh G (2019) Digital interventions to support adolescents and young adults with cancer: systematic review. JMIR Cancer 5(2):e12071
Grimshaw SL, Taylor NF, Shields N (2016) The feasibility of physical activity interventions during the intense treatment phase for children and adolescents with cancer: a systematic review. Pediatr Blood Cancer 63(9):1586–1593
Braam KI et al (2013) Physical exercise training interventions for children and young adults during and after treatment for childhood cancer. Cochrane Database Syst Rev 4:Cd008796
Barnett M et al (2016) Psychosocial outcomes and interventions among cancer survivors diagnosed during adolescence and young adulthood (AYA): a systematic review. J Cancer Surviv 10(5):814–831
van Dijk-Lokkart EM et al (2016) Effects of a combined physical and psychosocial intervention program for childhood cancer patients on quality of life and psychosocial functioning: results of the QLIM randomized clinical trial. Psycho-Oncology 25(7):815–822
Courneya KS, Friedenreich CM, Sela RA, Quinney HA, Rhodes RE, Jones LW (2004) Exercise motivation and adherence in cancer survivors after participation in a randomized controlled trial: an attribution theory perspective. Int J Behav Med 11(1):8–17
Brunet J et al (2019) Predictors of cancer survivors’ response to a community-based exercise program. Psychol Sport Exerc
Pugh G et al (2019) Trekstock meet & move: the impact of one-day health and well-being events for young adults with cancer. J Adolesc Young Adult Oncol. https://doi.org/10.1089/jayao.2019.0108
Valle CG, Tate DF, Mayer DK, Allicock M, Cai J (2013) A randomized trial of a Facebook-based physical activity intervention for young adult cancer survivors. J Cancer Surviv 7(3):355–368
Glasgow RE, Vogt TM, Boles SM (1999) Evaluating the public health impact of health promotion interventions: the RE-AIM framework. Am J Public Health 89(9):1322–1327
Pugh G et al (2017) Lifestyle advice provision to teenage and young adult cancer patients: the perspective of health professionals in the UK. Support Care Cancer
Loprinzi PD, Nooe A (2019) Objectively measured physical activity and all-cause mortality among cancer survivors: National Prospective Cohort Study. South Med J 112(4):234–237
Aldiss S, Fern LA, Phillips RS, Callaghan A, Dyker K, Gravestock H, Groszmann M, Hamrang L, Hough R, McGeachy D, Morgan S, Smith S, Upadhyaya S, Veitch H, Veitch L, Williamson M, Whelan JS, Gibson F (2019) Research priorities for young people with cancer: a UK priority setting partnership with the James Lind Alliance. BMJ Open 9(8):e028119
Acknowledgements
The authors acknowledge the support of YMCA gyms in supporting the delivery of the RENEW exercise referral programme.
Funding
This RENEW programme and evaluation was funded by Trekstock. Trekstock received financial support from LetterOne and the Big Lottery Fund to deliver the RENEW programme. GP is support by an RM Partners Pan-London Cancer Vanguard Fellowship.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
SE is the Chief Executive Officer of Trekstock; JR is employed by Trekstock as Health Programmes Manager; GP has received remuneration for providing independent consultancy to Trekstock. No competing financial interests exist for AF or NB.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of Queen Mary University Research Ethics Committee (reference: QMREC2018/48/006) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Statement of welfare of animals
This article does not contain any studies with animals performed by any of the authors.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Pugh, G., Below, N., Fisher, A. et al. Trekstock RENEW: evaluation of a 12-week exercise referral programme for young adult cancer survivors delivered by a cancer charity. Support Care Cancer 28, 5803–5812 (2020). https://doi.org/10.1007/s00520-020-05373-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00520-020-05373-5