
Abstract
Purpose
Evaluate the outcomes of ACL (Anterior Cruciate Ligament) reconstruction techniques that use a hamstring graft with a preserved tibial insertion and compare them to standard techniques.
Methods
A systematic literature review and meta-analysis was done of the PubMed, MEDLINE, Cochrane and Ovid databases to identify published clinical studies on ACL reconstruction in which a non-detached hamstring tendon (NDHT) was used as a graft and to compare them to studies in which a detached hamstring tendon (DHT) or other techniques were used. The eligible studies were analyzed for the knee laxity, Lachman test, pivot shift test, joint range of motion, anterior drawer, pain, re-tear, revision surgery, Lysholm score, Tegner score, ACL-RSI scale, KOOS, IKDC, SNQ and Howell scale.
Results
Twelve articles in which NDHT was used for ACL reconstruction were analyzed. There was no significant difference between NDHT and DHT in the Lachman > 1 (p = .07), pivot shift test > 1 (p = .40), re-tears (p = .62), pain (p = .85) and the Tegner score (p = .95). However, the outcomes were somewhat better with the NDHT technique for the Lachman (RR = 0.30; 95% CI 0.08–1.12), pivot shift test (RR = 0.50; 95% CI 0.10–2.49) and re-tears (RR = 0.66; 95% CI 0.13–3.42). The other criteria were not included in the meta-analysis because of lack of data or because specific outcome scores were used in each article.
Conclusion
NDHT techniques provide similar results to DHT for ACL reconstruction and tend to produce better stability and a lower re-tear rate.
Similar content being viewed by others
Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Anterior cruciate ligament (ACL) tears are one of the most common knee injuries [1,2,3,4]. Several types of grafts have been used for reconstruction surgery to restore knee stability [5,6,7,8]. Among the available reconstruction techniques, those using the hamstring tendon are among the most common and produce very good results [4, 7,8,9]. Standard techniques use the gracilis (G) and semitendinosus (ST) which are harvested and detached from their tibial insertion [10,11,12,13] (detached hamstring graft, DHT).
Some surgeons have proposed using a graft in which the tibial insertion of the hamstring tendons is preserved [10, 12, 13] (non-detached hamstring graft, NDHT). They contend that preserving the tibial insertion helps to retain the graft’s innervation and vascularization. Zaffagnini et al. [14] showed that a well-defined vascular network and a wide swath of nerve fibers were present on the insertion of these tendons. Furthermore, the construct is more solid due to the double tibial fixation (original insertion + mechanical fixation) [15,16,17]. The goal of using this technique is to achieve better graft integration [18,19,20,21, 21,22,23] in order to attain better functional outcomes and a lower retear rate.
To date, the only literature review on this subject was published by Ruffili et al. [24] in 2015. They included six studies with a total of 363 patients but could not group them or compare their outcomes. Nevertheless, three of the studies found that the function outcome scores were better when the tibial insertion of the hamstring grafts was preserved. The three other studies did not find a statistically significant difference. Thus, it seems appropriate to carry out of an updated systematic literature review and meta-analysis of all the published results with these new techniques in which the tibial insertion of the hamstring tendons is preserved. The analysis soughs to answer the following question: In ACL reconstruction, does using a NDHT graft produce clinical, functional and imaging outcomes that are at least equal to using a DHT graft?
Methods
Study eligibility (inclusion and exclusion criteria)
Eligible studies were prospective clinical trials reporting the results of NDHT and those comparing NDHT with DHT. The ineligible criteria were: reviews and articles published in languages other than French or English, studies with less than 12-month follow-up, studies investigating the outcomes of multi-ligament surgery and retrospective studies. We chose to exclude retrospective studies because their scientific value is less than that of prospective studies.
Literature search
An exhaustive search of articles published in the PubMed, MEDLINE, Cochrane and Ovid databases was done by following PRISMA guidelines [25]. The following keywords were used in the search: “non-detached”, “preserved tibial insertion” in combination with the term “ACL reconstruction”. All articles published up to January 1, 2022 were included, including articles published online. The references of the primary and review articles and main orthopedic textbooks were cross-referenced to identify any additional articles meeting the inclusion criteria that had not been identified during the primary search.
Study selection and data abstraction
The articles identified in the searches were screened by two authors who extracted the data independently; any conflicts were resolved before the final analysis. In clinical and comparative studies, the endpoints were compiled. When the data needed for a statistical analysis were not presented, the study authors were contacted by email. The following data were extracted from each study: (1) knee stability, including the mean side-to-side difference and the percentage of side-to-side difference above 3 mm (using a KT-1000/2000 arthrometer or Rolimeter), Lachman test graded as normal (score 1) or abnormal (score 2 or 3), pivot shift test graded as normal (grade 0 or 1) or abnormal (grade 2 or 3), joint range of motion, anterior drawer, pain, retear and revision surgery; (2) functional outcome scores, including the Lysholm, Tegner, ACL-RSI, KOOS and IKDC; (3) MRI criteria such as the signal-to-noise quotient (SNQ), Howell score and scores specific to each study. Only studies that were selected by the two authors were included in this meta-analysis.
Data analysis
The primary outcome measures were the clinical, functional and MRI parameters listed above. Study results were tabulated as the number of events and total number of subjects in the experimental (NDHT) versus control (DHT) groups for Lachman = 2 or 3, pivot shift = 2 or 3, pain and re-tear. Study results were tabulated using the mean and standard deviation (SD) together with the total number of subjects in the experimental versus control groups for continuous endpoints (Tegner score). Missing mean and SD were assessed from the median, range, and the size of the sample [26]. Missing SD (without median and range) was assessed according to the sample size and means from reported P values [27].
To describe the experimental results (NDHT), the frequency of an event or the weighted mean (continuous endpoints) was calculated together with 95% confidence intervals (95%CI). The risk ratio of an event in the experimental versus control group was calculated according to the inverse variance approach with their 95% CI. When the number of events was equal to zero in each group, it was imputed to one to estimate the risk ratio. The mean differences between experimental and control group were estimated for continuous endpoints according to the inverse variance approach with their 95% CI.
Forest plots were used to assess heterogeneity across studies, as well as Cochran’s heterogeneity statistic and Higgins I2 coefficients [28]. A P value < 0.1 or I2 > 50% was considered suggestive of statistical heterogeneity, prompting random effects modeling. To assess the risk of bias, the level of evidence of each study included in this meta-analysis was determined and included in the summary table (online Appendix). Funnel plots were generated to assess small-study effects [29]. The Review Manager 5.2 analysis software (The Cochrane Collaboration, Copenhagen, Denmark) was used to perform these analyses.
Results
Literature search, study selection and characteristics
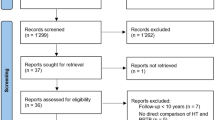
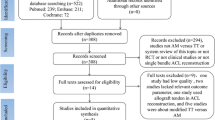
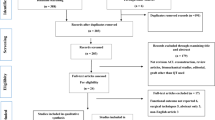
The literature search of the various databases identified 220 articles. After excluding duplicates, 187 articles remained. After screening the title and abstract of these articles, 25 articles were retained, and the full text read to evaluate their eligibility. In the end, 12 articles met the inclusion criteria: 3 studies reported the results of NDHT [30,31,32], 6 studies compared the results of NDHT and DHT [33,34,35,36,37,38], 3 studies compared the results of NDHT and other ACL reconstruction techniques (2 used the ST4 technique [37, 39] and 1 used a bone-patellar tendon-bone graft [40]). (Fig. 1) The main features of the selected studies are summarized in the online Appendix.

Flow chart summarizing the selection of articles according to PRISMA guidelines. NDHT non-detached hamstring tendon graft, DHT Detached hamstring tendon graft, ST4 four-bundle semitendinosus graft, BPTB: Bone patellar tendon bone graft
Analysis of NDHT outcomes
Primary endpoints
The meta-analysis of NDHT outcomes found stable knees with good clinical scores and few complications (Table 1).
Other endpoints
The meta-analysis could not be completed for the other endpoints: (1) 3 articles incorporated KT2000 Arthrometer measurements but did not disclose the SD (2) none of the articles evaluated the knee ROM and the Lysholm had no mean ± SD values; (3) none of the articles evaluated the ACL-RSI, KOOS and TTE; (4) the IKDC was evaluated in a single article; (5) 3 articles evaluated the SNQ but did not disclose the SD; (6) only one article measured the Howell grade and (7) the specific scores used in each study could not be combined.
Analysis of outcomes of NDHT versus DHT
Primary endpoints
There was no significant difference between NDHT and DHT in the Lachman > 1 (p = 0.07), pivot shift test > 1 (p = 0.40), re-tears (p = 0.62), pain (p = 0.85) and the Tegner score (p = 0.95) (Fig. 2). However, the outcomes were somewhat better with the NDHT technique for the Lachman (RR = 0.30; 95% CI 0.08–1.12), pivot shift test (RR = 0.50; 95% CI 0.10–2.49) and re-tears (RR = 0.66; 95% CI 0.13–3.42). There was considerable heterogeneity in the analysis of the Tegner score since studies go in the opposite direction.

Forest plots comparing the Lachman, pivot shift, retear rate, pain and Tegner score between the NDHT (non-detached hamstring tendon) and DHT (detached hamstring tendon) techniques for ACL reconstruction
Other endpoints
The meta-analysis could not be completed on the other endpoints: (1) some of the criteria were analyzed in one study only (KT2000 Arthrometer, ROM, anterior drawer, re-operation, other complications, IKDC, Howell) (2) two studies evaluated the Lysholm score but did not disclose the SD; (3) none of the articles evaluated the ACL-RSI, KOOS and TTE (Tibial Tunnel Enlargement); (4) 3 articles evaluated the KT1000 and SNQ but did not disclose the SD; (5) the specific scores used in each study could not be combined.
Funnel plots
No publication bias was identified by visual inspection of the funnel plots (online appendix).
Discussion
The most important findings of the present study were that techniques using NDHT grafts produce outcomes that are at least equivalent to techniques using DHT grafts for ACL reconstruction. The analysis of outcomes with NDHT found stable knees with good clinical scores and few complications. A comparison of the NDHT and DHT techniques found similar results in terms of stability, pain and function.
Our meta-analysis findings are consistent with the review of literature published by in 2015 by Ruffilli et al. [24] of 363 patients. Our analysis of studies using the NDHT techniques found very good clinical and functional outcomes, particularly for a positive pivot shift test (0.49%; 95% CI, 0.00–1.43%) and retear rate (0.00%; 95% CI, 0.00–0.00%). These findings are also consistent with retrospective studies that were not included in this meta-analysis. Buda et al. [16], in their retrospective study of 28 patients, found excellent results in the functional IKDC with a mean score of 93.8/100 and in the MRI results with 25/28 patients having a Yamato score of 1. Meynard et al. [41] did a retrospective study of long-term outcomes in patients who had undergone ACL reconstruction with NDHT and had a mean follow-up of 9.9 years. The mean KOOS was 86.3 ± 16.3, 94.4% had a negative pivot shift and 49/50 patients had a knee that was labelled as “normal” or “nearly normal” during the objective IKDC evaluation (Grade A or B).
In our meta-analysis, the results of the Lachman (RR = 0.30, 95% CI 0.08–1.12), pivot shift test (RR = 0.50, 95% CI 0.10–2.49) and retear rate (RR = 0.66, 95% CI 0.13–3.42) were not statistically significant but were better when using the NDHT technique. A lack of statistical power may have contributed to this lack of statistical significance since the meta-analysis was based on only two or three studies for each of these criteria.
The results of the pain assessment in our meta-analysis (RR = 1.14, 95% CI 0.30–4.40) were slightly better for the DHT group. We can't find an explanation for these results because the only difference between the two techniques is that the tibial insertion of the hamstring tendons is detached in one group (DHT) but not the other (NDHT).
The graft’s signal in MRI is now widely used to evaluate good graft incorporation and to validate certain surgical techniques [42, 43]. Grassi et al. [33] used MRI as the endpoint in their study. MRI was done at 4 and 18 months postoperative to compare a NDHT technique to a conventional DHT technique. The signal was lower in the group in which the tendon’s tibial insertion was preserved at 4 months (p = 0.008) and 18 months (p = 0.028), suggestive of better graft ligamentization.
In our systematic literature review, no retears occurred in the 174 patients who underwent ACL reconstruction with NDHT graft (0.00; 95% CI 0.00%–0.00%). The absence of retears can be explained by the relative short duration of the follow-up in the studies included. In fact, other than the studies by Marcacci et al.[31] with an 11-year follow-up and by Zaffagnini et al. [40] with an 8-year follow-up, the other studies had a mean follow-up of about 2 years. It would be interesting to evaluate the retear rate in the longer term, when patients have returned to their sports activity. This may confirm that the NDHT construct is indeed more solid.
Limitations
The current study has several limitations. First, not every article included featured a randomized controlled trial (online Appendix); this can bring about differences in the populations studied, which can alter the results obtained. Second, the criteria studied in this meta-analysis could only be compared directly in a limited number of studies, either because the criteria were not the same or because some data were missing. Nevertheless, this is the only meta-analysis so far to analyze a large cohort of patients who have undergone ACL reconstruction with NDHT graft. Third, while the surgical techniques use the same tendons (ST and G), there are differences between them, particularly in the fixation method used (screw, Endobutton, staple), which can introduce bias in the results.
Conclusions
NDHT techniques provide similar results to DHT for ACL reconstruction and tend to produce better stability and a lower re-tear rate.
References
Bram JT, Magee LC, Mehta NN et al (2021) Anterior cruciate ligament injury incidence in adolescent athletes: a systematic review and meta-analysis. Am J Sports Med 49:1962–1972. https://doi.org/10.1177/0363546520959619
Kaeding CC, Pedroza AD, Reinke EK et al (2015) Risk factors and predictors of subsequent ACL injury in either knee after ACL reconstruction: prospective analysis of 2488 primary ACL reconstructions from the MOON Cohort. Am J Sports Med 43:1583–1590. https://doi.org/10.1177/0363546515578836
Montalvo AM, Schneider DK, Yut L et al (2019) What’s my risk of sustaining an ACL injury while playing sports? a systematic review with meta-analysis. Br J Sports Med 53:1003–1012. https://doi.org/10.1136/bjsports-2016-096274
Sanders TL, Maradit Kremers H, Bryan AJ et al (2016) Incidence of anterior cruciate ligament tears and reconstruction: a 21-year population-based study. Am J Sports Med 44:1502–1507. https://doi.org/10.1177/0363546516629944
Cerulli G, Zamarra G, Vercillo F, Pelosi F (2011) ACL reconstruction with “the original all-inside technique.” Knee Surg Sports Traumatol Arthrosc 19:829–831. https://doi.org/10.1007/s00167-010-1371-2
Crawford C, Nyland J, Landes S et al (2007) Anatomic double bundle ACL reconstruction: a literature review. Knee Surg Sports Traumatol Arthrosc 15:946–964. https://doi.org/10.1007/s00167-007-0343-7
Mouarbes D, Menetrey J, Marot V et al (2019) anterior cruciate ligament reconstruction: a systematic review and meta-analysis of outcomes for quadriceps tendon autograft versus bone-patellar tendon–bone and hamstring-tendon autografts. Am J Sports Med 47:3531–3540. https://doi.org/10.1177/0363546518825340
Samuelsen BT, Webster KE, Johnson NR et al (2017) Hamstring autograft versus patellar tendon autograft for ACL reconstruction: is there a difference in graft failure rate? a meta-analysis of 47,613 patients. Clin Orthop 475:2459–2468. https://doi.org/10.1007/s11999-017-5278-9
Roger J, Bertani A, Vigouroux F et al (2020) ACL reconstruction using a quadruple semitendinosus graft with cortical fixations gives suitable isokinetic and clinical outcomes after 2 years. Knee Surg Sports Traumatol Arthrosc 28:2468–2477. https://doi.org/10.1007/s00167-020-06121-2
Kim S-J, Kim H-K, Lee Y-T (1997) Arthroscopic anterior cruciate ligament reconstruction using autogenous hamstring tendon graft without detachment of the tibial insertion. Arthrosc J Arthrosc Relat Surg 13:656–660. https://doi.org/10.1016/S0749-8063(97)90198-5
Marcacci M, Molgora AP, Zaffagnini S et al (2003) Anatomic double-bundle anterior cruciate ligament reconstruction with hamstrings. Arthrosc J Arthrosc Relat Surg 19:540–546. https://doi.org/10.1053/jars.2003.50129
Sonnery-Cottet B, Freychet B, Murphy CG et al (2014) Anterior cruciate ligament reconstruction and preservation: the single-anteromedial bundle biological augmentation (sambba) technique. Arthrosc Tech 3:e689–e693. https://doi.org/10.1016/j.eats.2014.08.007
Zaffagnini S, Marcheggiani Muccioli GM, Bonanzinga T et al (2013) Anatomic double-bundle anterior cruciate ligament reconstruction leaving hamstrings tibial insertion intact: technical note. Musculoskelet Surg 97:39–43. https://doi.org/10.1007/s12306-012-0230-3
Zaffagnini S, Golanò P, Farinas O et al (2003) Vascularity and neuroreceptors of the pes anserinus: Anatomic Study: Vascularity of Pes Anserinus. Clin Anat 16:19–24. https://doi.org/10.1002/ca.10073
Bahlau D, Clavert P, Favreau H et al (2019) Mechanical advantage of preserving the hamstring tibial insertion for anterior cruciate ligament reconstruction–A cadaver study. Orthop Traumatol Surg Res 105:89–93. https://doi.org/10.1016/j.otsr.2018.11.014
Buda R, Di Caprio F, Giuriati L et al (2008) Partial ACL tears augmented with distally inserted hamstring tendons and over-the-top fixation: an MRI evaluation. Knee 15:111–116. https://doi.org/10.1016/j.knee.2007.12.002
Liu S, Sun Y, Wan F et al (2018) Advantages of an attached semitendinosus tendon graft in anterior cruciate ligament reconstruction in a rabbit model. Am J Sports Med 46:3227–3236. https://doi.org/10.1177/0363546518799357
Claes S, Verdonk P, Forsyth R, Bellemans J (2011) The “Ligamentization” process in anterior cruciate ligament reconstruction: what happens to the human graft? a systematic review of the literature. Am J Sports Med 39:2476–2483. https://doi.org/10.1177/0363546511402662
Fules PJ, Madhav RT, Goddard RK et al (2003) Evaluation of tibial bone tunnel enlargement using MRI scan cross-sectional area measurement after autologous hamstring tendon ACL replacement. Knee 10:87–91. https://doi.org/10.1016/S0968-0160(02)00086-8
Ge Y, Li H, Tao H et al (2015) Comparison of tendon–bone healing between autografts and allografts after anterior cruciate ligament reconstruction using magnetic resonance imaging. Knee Surg Sports Traumatol Arthrosc 23:954–960. https://doi.org/10.1007/s00167-013-2755-x
Howell SM, Knox KE, Farley TE, Taylor MA (1995) Revascularization of a human anterior cruciate ligament graft during the first two years of implantation. Am J Sports Med 23:42–49. https://doi.org/10.1177/036354659502300107
Pauzenberger L, Syré S, Schurz M (2013) “Ligamentization” in hamstring tendon grafts after anterior cruciate ligament reconstruction: a systematic review of the literature and a glimpse into the future. Arthrosc J Arthrosc Relat Surg 29:1712–1721. https://doi.org/10.1016/j.arthro.2013.05.009
Weiler A, Peters G, Mäurer J et al (2001) Biomechanical properties and vascularity of an anterior cruciate ligament graft can be predicted by contrast-enhanced magnetic resonance imaging: a two-year study in sheep <sup/>. Am J Sports Med 29:751–761. https://doi.org/10.1177/03635465010290061401
Ruffilli A, Traina F, Evangelisti G et al (2015) Preservation of hamstring tibial insertion in anterior cruciate ligament reconstruction: a review of the current literature. Musculoskelet Surg 99:87–92. https://doi.org/10.1007/s12306-015-0346-3
Moher D, Liberati A, Tetzlaff J et al (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 6:e1000097. https://doi.org/10.1371/journal.pmed.1000097
Hozo SP, Djulbegovic B, Hozo I (2005) Estimating the mean and variance from the median, range, and the size of a sample. BMC Med Res Methodol 5:13. https://doi.org/10.1186/1471-2288-5-13
Follmann D, Elliott P, Suh I, Cutler J (1992) Variance imputation for overviews of clinical trials with continuous response. J Clin Epidemiol 45:769–773. https://doi.org/10.1016/0895-4356(92)90054-Q
Higgins JPT (2003) Measuring inconsistency in meta-analyses. BMJ 327:557–560. https://doi.org/10.1136/bmj.327.7414.557
Peters JL, Sutton AJ, Jones DR et al (2008) Contour-enhanced meta-analysis funnel plots help distinguish publication bias from other causes of asymmetry. J Clin Epidemiol 61:991–996. https://doi.org/10.1016/j.jclinepi.2007.11.010
Bahlau D, Favreau H, Eichler D et al (2019) Clinical, functional, and isokinetic study of a prospective series of anterior cruciate ligament ligamentoplasty with pedicular hamstrings. Int Orthop 43:2557–2562. https://doi.org/10.1007/s00264-019-04392-0
Marcacci M, Zaffagnini S, Giordano G et al (2009) Anterior cruciate ligament reconstruction associated with extra-articular tenodesis: a prospective clinical and radiographic evaluation with 10- to 13-year follow-up. Am J Sports Med 37:707–714. https://doi.org/10.1177/0363546508328114
Sinha S, Naik AK, Maheshwari M et al (2018) Anterior cruciate ligament reconstruction with tibial attachment preserving hamstring graft without implant on tibial side. Indian J Orthop 52:170–176. https://doi.org/10.4103/ortho.IJOrtho_85_17
Grassi A, Casali M, Macchiarola L et al (2021) Hamstring grafts for anterior cruciate ligament reconstruction show better magnetic resonance features when tibial insertion is preserved. Knee Surg Sports Traumatol Arthrosc 29:507–518. https://doi.org/10.1007/s00167-020-05948-z
Gupta R, Bahadur R, Malhotra A et al (2017) Outcome of hamstring autograft with preserved insertions compared with free hamstring autograft in anterior cruciate ligament surgery at 2-year follow-up. Arthrosc J Arthrosc Relat Surg 33:2208–2216. https://doi.org/10.1016/j.arthro.2017.06.040
Liu S, Li H, Tao H et al (2018) A randomized clinical trial to evaluate attached hamstring anterior cruciate ligament graft maturity with magnetic resonance imaging. Am J Sports Med 46:1143–1149. https://doi.org/10.1177/0363546517752918
Papachristou G, Sourlas J, Plessas S, Papachristou K (2008) Arthroscopic ACL reconstruction with Δ plasty: an innovative approach with hamstrings’ transfer and double tibial tunnel. Knee Surg Sports Traumatol Arthrosc 16:420–426. https://doi.org/10.1007/s00167-007-0426-5
Zaffagnini S, Marcacci M, Lo Presti M et al (2006) Prospective and randomized evaluation of ACL reconstruction with three techniques: a clinical and radiographic evaluation at 5 years follow-up. Knee Surg Sports Traumatol Arthrosc 14:1060–1069. https://doi.org/10.1007/s00167-006-0130-x
Zhang Y, Liu S, Chen Q et al (2020) Maturity progression of the entire anterior cruciate ligament graft of insertion-preserved hamstring tendons by 5 years: a prospective randomized controlled study based on magnetic resonance imaging evaluation. Am J Sports Med 48:2970–2977. https://doi.org/10.1177/0363546520951507
Ruffilli A, Pagliazzi G, Ferranti E et al (2016) Hamstring graft tibial insertion preservation versus detachment in anterior cruciate ligament reconstruction: a prospective randomized comparative study. Eur J Orthop Surg Traumatol 26:657–664. https://doi.org/10.1007/s00590-016-1812-9
Zaffagnini S, Bruni D, Marcheggiani Muccioli GM et al (2011) Single-bundle patellar tendon versus non-anatomical double-bundle hamstrings ACL reconstruction: a prospective randomized study at 8-year minimum follow-up. Knee Surg Sports Traumatol Arthrosc 19:390–397. https://doi.org/10.1007/s00167-010-1225-y
Meynard P, Pelet H, Angelliaume A et al (2020) ACL reconstruction with lateral extra-articular tenodesis using a continuous graft: 10-year outcomes of 50 cases. Orthop Traumatol Surg Res 106:929–935. https://doi.org/10.1016/j.otsr.2020.04.007
Cavaignac E, Marot V, Faruch M et al (2018) hamstring graft incorporation according to the length of the graft inside tunnels. Am J Sports Med 46:348–356. https://doi.org/10.1177/0363546517733472
Cavaignac E, Mesnier T, Marot V et al (2020) Effect of lateral extra-articular tenodesis on anterior cruciate ligament graft incorporation. Orthop J Sports Med 8:232596712096009. https://doi.org/10.1177/2325967120960097
Acknowledgements
Joanne Archambault, PhD for English language assistance
Funding
There was no funding for this work.
Author information
Authors and Affiliations
Contributions
NV drafted the manuscript and did literature research. EC reviewed the manuscript and did the literature research. VM and MC did the methodology. EB did the data analysis. All authors read and approved final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
Etienne Cavaignac is a paid consultant for Arthrex and Amplitude.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Vari, N., Cavaignac, E., Cavaignac, M. et al. Outcomes of hamstring graft with preserved tibial insertion for ACL reconstruction: systematic review and meta-analysis. Eur J Orthop Surg Traumatol 34, 67–73 (2024). https://doi.org/10.1007/s00590-023-03698-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00590-023-03698-5