
Abstract
Aims
Type 1 and 2 diabetes mellitus (T1DM and T2DM) can lead to emotional distress and cognitive impairments, often caused by psychological factors such as low mood or anxiety; yet, few studies have explored the theoretical mechanisms underlying these relationships and within one study. This study explored the relationships between psychological states (anxiety/worry, fatigue) and diabetes outcomes (diabetes distress, cognitive dysfunction), and whether resilience mediated the association between these in T1DM and T2DM.
Methods
A sample of 307 UK adults with a clinical diagnosis of diabetes (T1DM = 129; T2DM = 178) completed a cross-sectional online survey, composed of six questionnaires. Associations between variables were investigated using Pearson’s correlations and Structural Equation Modelling (SEM).
Results
Psychological states were significantly correlated with diabetes outcomes, and resilience was significantly related to both psychological states and diabetes outcomes. The SEM model achieved an acceptable model fit with a significant mediating effect of resilience between psychological states (anxiety/worry, fatigue) and diabetes outcomes (diabetes distress, cognitive dysfunction), with no significant differences between diabetes type.
Conclusions
We propose a new theoretical model of T1DM and T2DM that could be used to provide guidance for those designing interventions. These findings help to understand the complex nature of diabetes management, suggesting resilience could be a key factor in managing psychological states and diabetes outcomes.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
The two main classifications of diabetes are T1DM and T2DM, and whilst they share clinically similar symptoms, the aetiology of the disorder types differs significantly [1]. Both have a strong genetic component [1], and inadequate long-term self-management is associated with greater risk of serious acute complications (e.g., coma) and chronic (e.g., cardiopathy, sexual dysfunction, retinopathy, nephropathy, limb loss) [2]. Approximately one third of people with T2DM and two thirds of people with T1DM do not achieve the target glycated haemoglobin (HbA1c) levels [2]. The constant demands of living with diabetes can also take a significant psychological toll, with many individuals experiencing distress, depressed mood, anxiety, fatigue and reduced quality of life [3, 4]. The rising burden of diabetes globally is a major health priority, placing increased demands on patients, carers, health systems and society [5]. Identifying and understanding the key psychological factors that contribute to diabetes management and outcomes is therefore a key priority.
Existing literature shows both T1 and T2 diabetes suffer from high levels of anxiety and fatigue, with diabetes distress and executive functioning (EF) issues [8, 9]. Diabetes distress and EF issues are positively associated with each other, and with anxiety and fatigue [8,9,10,11,12,13,14,15,16,17,18,19]. Resilience is an increasingly important factor in diabetes self-management because resilience can be taught through intervention [27, 45]. Resilience is defined as the capacity to adapt and maintain psychological and physical ‘wellbeing’ in the face of adversity [6] and has been found to correlate negatively with anxiety, fatigue, diabetes distress and cognitive dysfunction [6, 7, 20,21,22,23,24,25,26,27,28]. These patterns of associations suggest that resilience may act as a mediator [29] but not a moderator; research suggests a causal relationship between anxiety/fatigue and resilience, and resilience and diabetes distress/cognition, therefore, resilience cannot theoretically be a moderator variable [29]. Studies have yet to explore the role of resilience in conjunction with anxiety, fatigue, diabetes distress and executive dysfunction simultaneously, within one model; this is the focus of the present research and is depicted in Fig. 1.
Existing literature suggests direct associations between anxiety (predictor) and diabetes distress and cognition (outcomes), and between fatigue and cognition. There is still little research to suggest a direct link between fatigue and diabetes distress [8]. Park et al. [30] found the relationship between fatigue and diabetes distress was mediated by diabetes symptoms, suggesting the relationship may be an indirect one, and is reflected as such in the proposed model (see Fig. 1).
Winkley et al. [31] suggest future research should focus on underlying theories, rather than replicating existing psychological models that usually deliver small effect sizes. Since theory-based interventions are more likely to produce longer-lasting and larger effects than those without [32], this supports the need to focus more on the underlying theoretical mechanisms, with a focus on the psychosocial effects of living with and managing diabetes [3].
Therefore, the overall aim was to formulate and test an original theoretical model, based on a critical review of existing literatures, that could be used to provide guidance for those designing interventions for T1DM and T2DM groups. More specifically, the study aims were to: 1) to explore whether resilience mediated the association between psychological states and diabetes outcomes, and 2) to assess whether T1DM and T2DM diabetics differ in relation to covariances amongst the afore-mentioned variables.
Based on the above literature, the hypotheses for the proposed structural model are as follows:
Direct relationships will be:
-
H1: Anxiety/worry will be positively related to diabetes distress [14,15,16]
-
H2: Anxiety/worry will be negatively related to cognition [17,18,19, 22]
-
H3: Fatigue will be negatively related to cognition [9, 12, 13, 15]
The mediating relationships will be:
Method
Design
A correlation design was used to investigate the strength and direction of associations between the following variables in people with T1DM and T2DM: anxiety, fatigue, diabetes distress, cognition and resilience (as a potential mediator).
Participants
Adults in the Northwest UK with T1DM (n = 129) and T2DM (n = 178) were recruited via diabetes support groups, local newspaper advertisements and social media advertisements. Participants completed an e-survey, created using the platform Qualtrics. Exclusion criteria included people below the age of 18 years, those with diabetes that is not T1DM/T2DM, and those who failed to state diabetes type.
Both T1DM and T2DM groups were mostly female (77.5 and 79.2%, respectively), with mean ages of 432.41 (SD = 178.99) and 663.99 (SD = 129.65), and were white British (80.6% and 72.5%, respectively). T1DM durations ranged from 5—960 months (80 years), whereas T2DM ranged from 1 to 444 months (37 years). Average diabetes durations were 235.71 (T1DM), 97.08 (T2DM), and average HbA1c levels were 62.11 mmol/mol (T1DM) and 62.271 mmol/mol (T2DM).
Sample size requirements for structural equation modelling
Guidance taken from Boateng [34] and Wolf et al. [35] was used to inform sample size; sample sizes of 100–200 are recommended, or at least 5 cases per model parameter. See also [35, 36] for SEM discussion with smaller sample sizes.
Materials and procedure
Participants were provided a link to an anonymous survey, first directing them to the study participation information sheet. Consent was confirmed through completing and submitting the questionnaires. Any participants who did not submit at the end of the survey were deemed to have withdrawn and their data was not used.
Anxiety/worry (psychological state latent variable)
Anxiety/worry was assessed using the Penn State Worry Questionnaire (PSWQ) [48], a 16-item single factor scale that is considered the ‘gold standard’ for measuring unspecific worry. Scores range between 16 and 80, with a higher score indicating higher anxiety. Internal consistency (Cronbach’s alpha) for this sample was 0.97 and 0.98 for T1DM and T2DM groups, respectively.
Fatigue (psychological state latent variable)
Fatigue was measured using Flinder’s Fatigue Scale (FFS) [49], a 7-item single factor scale measuring daytime fatigue (e.g., frequency, severity), often associated with insomnia. Six items use a 5-point Likert scale, and item 5 uses a multiple item checklist. Scores range between 0–31, with higher scores indicating greater fatigue. Internal consistency for this sample was 0.92 and 0.90 for T1DM and T2DM groups, respectively.
Diabetes distress (diabetes outcome latent variable)
Diabetes-specific distress was assessed using the Diabetes Distress Scale (DDS) [50], a 17-item, 4-factor measure consisting of emotional, physician, regimen and interpersonal distress subscales. (Overall and subscale scores were used in correlational analyses, but only subscales were used in the SEM.) Scores range between 17 and 102, where higher scores indicate greater distress. Items relating to their respective factor are averaged, where a mean score of 3 or higher indicates moderate distress, worthy of clinical attention. Internal consistency for this sample was 0.94 and 0.95 for T1DM and T2DM groups, respectively.
Cognition (diabetes outcome latent variable)
Cognition/EF was assessed using the Dysexecutive Questionnaire (DEX) [51], a 20-item, three-factor measure consisting of volition, inhibition and social regulation subscales. Scores range between 0 and 80, with higher scores indicating greater problems with EF. Internal consistency for this sample was 0.88 for T1DM and T2DM groups.
Resilience (mediator variable)
Resilience was measured using the Connor-Davidson Resilience Scale (CD-RISC) [52], a 25-item single factor scale, where resilience is defined as the capacity to adapt and maintain psychological and physical wellbeing in the face of stress, adversity or trauma [6]. Scores range between 0–100, where higher scores indicate greater resilience. Internal consistency for this sample was 0.95 for T1DM and T2DM groups.
Data analytic strategy (SEM)
Structural equation modelling was chosen for analysis as it is a flexible method that can be used to explore relationships between latent variables [34], using AMOS (version 27). Two psychological state latent variables (anxiety and fatigue) were categorised as predictor variables. A third latent variable was resilience (mediator variable). Two diabetes outcome latent variables (diabetes distress and cognition) were categorised as outcome variables. Figure 1 shows the operationalisation of exogenous, endogenous and mediator variables. As recommended in SEM literature [34], an alternative model was also tested, whereby diabetes distress was incorporated as an exogenous variable rather than endogenous, based on existing literature findings [30].
The maximum likelihood chi-square statistic was used to evaluate the measurement and structural models, but as this is sensitive to sample size, the normed chi-square (χ2 /df) was also used alongside several other indices to assess model fit, including: comparative fit index (CFI), Tucker-Lewis index (TLI), incremental fit index (IFI), root mean square error of approximation (RMSEA) and standardised root mean square residual (SRMR). Hu & Bentler [37] suggested acceptable cut-off criteria indicative of good model fit are > 0.95 (CFI, TLI, IFI). However, given the exploratory nature of this study, it was decided best to use more conservative criteria, indicative of moderate fit. Therefore, the following cut-offs for acceptable model fit were used: χ2/df 1–5; CFI, TLI and IFI > 0.90; RMSEA ≤ 0.06—0.08; and SRMR ≤ 0.08 [37, 38]. Standardised regression weights were used to interpret direct effects, and bias-corrected bootstrap confidence intervals technique was used to assess the significance of standardised indirect effects.
Results
Preliminary analyses
Data were examined for missing values, outliers and normal distribution. Missing value analysis for validated measures were < 5%, missing variables at random (Little’s MCAR test: Chi-Square = 42,895.414, df = 42,606.00, p = 0.161). Missing values were replaced using person mean substitution by scale/subscale. Outlier detection revealed seven univariate outliers that were dealt with using winzorising, and five multivariate outliers were removed. Given the large sample size (n > 300), distribution shape/skewness and kurtosis were used to determine normality. Mean and SD values were calculated for all variables recorded, separately for T1 and T2 groups, and independent samples t tests, Pearson’s correlations and SEM analyses were then run separately for each diabetes group.
Correlational analyses
Pearson’s correlations were conducted to examine a) the relationship between psychological states (anxiety, fatigue) and diabetes outcome measures (diabetes distress, cognition), b) multicollinearity i.e., high correlations between indicators of psychological state latents and indicators of the outcome measures with each other and c) the potential for a mediating relationship of resilience between psychological states and diabetes outcomes. These correlations were undertaken for T1DM (n = 129) and T2DM (n = 178) diabetes groups separately. Effect sizes (r values) were deemed to be small, medium or large if they were, 0.10, 0.30 or 0.50, respectively [39].
T1DM Correlations: All psychological state and diabetes outcome variables were significantly positively correlated, except from the cognition (social regulation only) values. Correlations between components of diabetes distress, anxiety, fatigue and cognition were significant and typically moderate in strength. All psychological state and diabetes outcome variables were significantly negatively associated with resilience values, and typically moderate to strong in strength.
T2DM Correlations: All psychological state and diabetes outcome variables were significantly positively correlated, except from the cognition (social regulation only) values, as in T1DM. Correlations between components of diabetes distress, anxiety, fatigue and cognition were significant and typically moderate in strength. All psychological state and diabetes outcome variables were significantly negatively correlated with resilience values, and typically moderate to strong in strength.
Measurement models: confirmatory factor analysis (CFA)
Factor loading, and reliability and validity
Using a factor loading of at least 0.40 [34], 6 items were deleted (see Appendix 3). To assess the reliability and validity of scales used, Composite Reliability (CR) and Average Variance Extracted (AVE) values were calculated, and all scales met acceptable cut-off values for Cronbach’s alpha (> 0.70) and CR (> 0.60), demonstrating adequate reliability [40].
Multigroup CFA: model fit statistics, T1DM and T2DM groups
Pearson’s correlations were conducted between the latent variables in both diabetes groups; all correlations between psychological states, resilience and diabetes outcomes were significant, with no evidence of multicollinearity (r ≤ 0.90).
Fit indices are presented in Table 1; all indicators loaded onto their respective factors (> 0.40), and each scale achieved acceptable values in ≥ 3 fit indices (see Table 1). This suggests the data are suitable for SEM analysis.
Structural models
A diagrammatic representation of the structural model (for T1DM and T2DM) is presented in Figs. 2 and 3. This shows the standardised path coefficients, significance levels and R2 values, which indicate the amount of variance explained by the independent variables. The values of fit statistics for the structural model were all found to be within acceptable limits: χ2 (Chi-Square) = 139.905, df = 58, and χ2/df ratio = 2.41, CFI = 0.94, IFI = 0.94, TLI = 0.90, RMSEA = 0.07, and SRMR = 0.07.
The results of the initial hypotheses tests for each path in the structural model are summarised in Table 2.
SEM: T1DM
Findings were similar for both T1DM and T2DM. As shown in Table 2, hypotheses 1, 2 and 3 were non-significant and therefore unsupported. However, hypotheses 4, 5, 6 and 7, which are part of the indirect effect were all supported: anxiety and fatigue had a significant negative influence on resilience, and resilience had a significant negative influence on diabetes distress and cognition.
To identify the presence of mediation, bootstrapping was used to calculate direct and indirect effects in T1DM. Results confirmed a mediating effect of resilience on the relationships between psychological states (anxiety, fatigue) and diabetes outcomes (diabetes distress, cognition) in T1DM.
SEM: T2DM
For T2DM, hypotheses 1, 2 and 3 were non-significant and therefore unsupported. However, hypotheses 4, 5, 6 and 7 were all supported: anxiety and fatigue were found to have a significant negative influence on resilience, and resilience has a significant negative influence on diabetes distress and cognition.
To confirm the presence of mediation, bootstrapping was used to calculate direct and indirect effects in T2DM. Results confirmed a mediating effect of resilience on the relationships between psychological states (anxiety, fatigue) and diabetes outcomes (diabetes distress, cognition) in T2DM.
Model comparisons
The above SEM model was used as a baseline comparison, and non-significant pathways were consecutively constrained to zero to confirm whether eliminating non-significant pathways results in a more parsimonious final model [34]. The paths of H1-3 were consecutively constrained in models 1, 2 and 3, after which a full mediation model was tested in model 4; all direct paths from psychological states to diabetes outcomes were constrained to zero, leaving only indirect paths (see Appendix 6 for comparison table).
Model 4 is the most parsimonious solution; the non-significant pathways have been eliminated without negatively impacting the model fit statistics, and therefore, model 4 was used as the final structural model (see Fig. 4). Multigroup analysis of Model 4 revealed no significant differences between T1DM and T2DM groups (χ2= 8.68, p = 0.730), suggesting the model is appropriate to both groups.
In summary, structural equation modelling identified a significant mediational effect of resilience on psychological states (anxiety, fatigue) and diabetes outcomes (diabetes distress, cognition), in both T1DM and T2DM.
Alternative model testing
An alternative model was tested, whereby diabetes distress was incorporated as an exogenous variable rather than endogenous. This model was rejected due to poor fit.
Fit indices yielded a poorer model fit compared to the initial model: χ2 (Chi-Square) = 172.606, df = 60, and χ2/df ratio = 2.877. Comparative Fit Index (CFI) = 0.913, Incremental Fit Index (IFI) = 0.915, Tucker-Lewis Index (TLI) = 0.87, Root Mean Square Error of Approximation (RMSEA) = 0.08, and Standardised Root Mean Square Residual (SRMR) = 0.091.
For the T1DM group, hypotheses 1, 2, 3, 4, 5 and 7 were non-significant and therefore unsupported. Hypothesis 6, which is part of the indirect effect was supported (β = -0.414, t = -1.96, p = 0.050), suggesting fatigue had a significant negative effect on resilience. Mediation analysis revealed no significant effects.
For the T2DM group, hypotheses 1, 2, 3, 4 and 7 were non-significant and therefore unsupported. Hypotheses 5 and 6, which are part of the indirect effect were supported (β = -0.059, t = -2.54, p = 0.011; β = -0.218, t = -3.09, p = 0.002, respectively), suggesting a significant effect of anxiety and fatigue on resilience. Mediation analysis revealed significant indirect effects of anxiety (-0.156, p = 0.001) and fatigue (-0.578, p = 0.001), suggesting resilience mediated the relationship between both anxiety and fatigue, and cognition.
Multigroup analysis revealed no significant differences between T1DM and T2DM groups (χ2 = 2.33, p = 0.507), suggesting the model is appropriate to both groups.
Discussion
This study was the first to test a theoretical model whereby psychological states (anxiety/worry, fatigue) and diabetes outcomes (diabetes distress, cognition) are mediated by resilience, in both T1DM and T2DM groups. Preliminary correlations between predictor and outcome variables were as expected, based on past evidence [8, 12], in both T1DM and T2DM. All psychological state and diabetes outcome variables were significantly negatively associated with resilience, laying the groundwork for SEM. The proposed structural model achieved an acceptable model fit with no significant differences between diabetes type, suggesting the model was appropriate for both T1DM and T2DM groups.
For both T1DM and T2DM groups, direct relationships within the model were not significant and therefore not supported. However, indirect paths demonstrating the mediating effect were all significant. Bootstrapping confirmed a significant mediating effect of resilience between psychological states (anxiety, fatigue) and diabetes outcomes (diabetes distress, cognition) in both T1DM and T2DM. Additionally, the model supports an indirect relationship between diabetes distress and fatigue, which is similar to the findings of Park et al. [30], although this study looked at resilience as a mediator variable rather than diabetes symptoms. Interestingly, Lasselin et al., [41] also found data supporting higher rates of fatigue in T2DM compared to T1DM, however the SEM revealed no significant multigroup differences in fatigue.
Mediation research is necessary for advancement of psychological theory and clinical therapies [44]. These findings confirm a novel theoretical model that has the potential to optimise intervention treatments and subsequently improve diabetes self-management (i.e., improving disease prognosis and health outcomes). Resilience has also been found to play a protective role in the psychological states of other diseases, for example, protecting against: depression in adults managing cardiac disease [45]; psychological distress in cancer patients [46]; and diabetes-specific distress in diabetes patients [7]; where each study found improved health outcomes with greater resilience. Despite this, the mechanisms by which resilience acts as a protective factor are not well known [7, 45], which this study aimed to address. The mediating effect of resilience (in the context of anxiety/fatigue) can be utilised in early education interventions (e.g., conversion maps) to improve knowledge and management of diabetes outcomes [47], which can prevent serious diabetes complications (e.g., limb loss) [4]. Resilience training would provide a protective measure against negative psychological states/disorders and help improve health outcomes; this would be widely applicable to other areas of life and managing other chronic diseases.
This study has several strengths. Structural Equation Modelling allows for investigation of complex relationships simultaneously and is able to measure unobserved variables using observed variables (accounting for error measurement, rather than treating them separately) [34]. Another benefit is that SEM performs well with a range of sample sizes, including ones smaller than that of this study [e.g., 35, 36]. Yet, it is important for future studies to confirm this model using a larger diverse sample. Although this study is cross-sectional rather than longitudinal, SEM allows one to test theoretically plausible ideas about the order of variables, and thus, this study identified anxiety and fatigue as psychological risk factors that can be mediated by resilience.
This study has several areas for further investigation. Comparisons of individual difference variables such as males and females and ethnicity were not investigated, which is important for this theoretical model because findings have suggested gender and racial differences in diabetes management [42]. For example, males report more problem-focused coping methods whereas females report more negative and emotion-focused coping styles. It is important also to note total samples for T1DM and T2DM groups were mostly female (77.5% and 79.2%, respectively), which is not representative in the current diabetes literature [43]. This could suggest that females are more likely to reach out to others regarding their diabetes, which has significant implications in both healthcare and research settings. It is important to confirm these results in a more representative population regarding gender split, to ensure reliability of findings.
Conclusions
This study showed resilience mediates the relationship between anxious and fatigued psychological states and diabetes distress and cognition in adults with T1DM and T2DM. It is recommended those devising interventions for people with T1DM and T2DM target resilience as a potential psychological mechanism; specifically, to offset problems with diabetes distress and cognition, as a consequence of anxiety/worry and fatigue. This could help improve health outcomes and quality of life in people with this lifelong condition, which in turn can positively impact mental health and wellbeing.
Appendices
Appendix 1: Means (and standard deviations) for participant classification information and demographics
Type 1 (N = 129) | Type 2 (N = 178) | Total (N = 307) | |||
|---|---|---|---|---|---|
Male (27) | Female (100) | Male (36) | Female (141) | ||
Age* | 432.41 (178.99) | 663.99 (129.65) | 566.89 (190.34) | ||
Diabetes Duration* | 235.71(179.14) | 97.08 (85.51) | 155.16 (149.52) | ||
HbA1c** | 62.11/ 7.8 (17.01) | 62.271/ 7.8 (18.68) | 62.204/ 7.8 (17.93) | ||
Ethnicity | |||||
British/English | 104 | 129 | 233 | ||
Welsh | 1 | 0 | 1 | ||
Irish | 3 | 1 | 4 | ||
British Asian | 1 | 3 | 4 | ||
White Non-Hispanic | 1 | 0 | 1 | ||
Greek | 1 | 1 | 2 | ||
German | 0 | 2 | 2 | ||
Mixed Caribbean | 0 | 1 | 1 | ||
American | 0 | 1 | 1 | ||
Greek | 0 | 1 | 1 | ||
White European | 0 | 6 | 6 | ||
White | 16 | 32 | 48 | ||
Mixed | 0 | 1 | 1 | ||
Appendix 2: Correlations (Pearson’s r) between psychological states, resilience and diabetes outcomes in Type 1 and 2 groups
PSWQ | FFS | DDS_TOT | DDS_EB | DDS_PRD | DDS_RRD | DDS_ID | DEX_TOT | DEX_VOL | DEX_INH | DEX_SR | CDRISC | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
PSWQ | - | 0.41** | 0.57** | 0.59** | 0.32** | 0.54** | 0.38** | 0.44** | 0.55** | 0.34** | -0.03 | -0.52** |
FFS | 0.46** | - | 0.49** | 0.49** | 0.37** | 0.33** | 0.43** | 0.30** | 0.41** | 0.18* | 0.07 | -0.34** |
DDS_TOT | 0.49 ** | 0.50 ** | - | 0.88** | 0.74** | 0.86** | 0.81** | 0.41** | 0.48** | 0.31** | 0.15 | -0.51** |
DDS_EB | 0.53 ** | 0.50 ** | 0.89 ** | - | 0.48** | 0.70** | 0.64** | 0.43** | 0.48** | 0.35** | 0.09 | -0.50** |
DDS_PRD | 0.24 ** | 0.32 ** | 0.80 ** | 0.60 ** | - | 0.47** | 0.53** | 0.29** | 0.29** | 0.22* | 0.14 | -0.30** |
DDS_RRD | 0.42 ** | 0.48 ** | 0.87 ** | 0.71 ** | 0.53 ** | - | 0.59** | 0.35** | 0.43** | 0.30** | 0.12 | -0.50** |
DDS_ID | 0.47 ** | 0.39 ** | 0.84 ** | 0.71 ** | 0.59 ** | 0.65 ** | - | 0.25** | 0.32** | 0.09 | 0.15 | -0.34** |
DEX_TOT | 0.45 ** | 0.46 ** | 0.42 ** | 0.43 ** | 0.19 * | 0.44 ** | 0.35 ** | - | 0.85** | 0.83** | 0.61** | -0.50** |
DEX_VOL | 0.48 ** | 0.59 ** | 0.51 ** | 0.53 ** | 0.27 ** | 0.50 ** | 0.42 ** | 0.82 ** | - | 0.58** | 0.37** | -0.58** |
DEX_INH | 0.32 ** | 0.31 ** | 0.23 ** | 0.25 ** | 0.07 | 0.29 ** | 0.16 * | 0.82 ** | 0.51 ** | - | 0.46** | -0.28** |
DEX_SR | 0.13 | 0.14 | 0.18 * | 0.20 ** | 0.10 | 0.17 * | 0.15 * | 0.61 ** | 0.34 ** | 0.44 ** | - | -0.18* |
CDRISC | -0.47 ** | -0.44 ** | -0.47 ** | -0.46 ** | -0.27 ** | -0.45 ** | -0.39 ** | -0.41 ** | -0.53 ** | -0.16 * | -0.23 ** | - |
Appendix 3: Full CFA Results for Measurement Model 1, Type 1 and 2 Diabetes Groups ( T2 = bold)
Conceptual variable (and subscales) | Item | Factor loading | t value (C.R.) | R2 value | CR (composite reliability) | AVE (Average variance extracted) | Cronbach’s alpha (α) |
|---|---|---|---|---|---|---|---|
DDS | Q1 | 0.79** 0.80** | Fixed Fixed | 0.621 0.637 | 0.968 0.977 | 0.644 0.716 | 0.935 0.951 |
Emotional burden | Q14 | 0.93** 0.89** | 12.436 13.839 | 0.873 0.792 | |||
(EB) | Q8 | 0.87** 0.85** | 11.331 13.011 | 0.760 0.725 | |||
Q3 | 0.87** 0.85** | 11.308 13.028 | 0.758 0.726 | ||||
Q11 | 0.70** 0.74** | 8.578 10.868 | 0.495 0.554 | ||||
Physician related | Q4 | 0.81** 0.91** | Fixed Fixed | 0.653 0.823 | |||
Distress (PRD) | Q2 | 0.76** 0.87** | 9.114 17.405 | 0.576 0.764 | |||
Q9 | 0.84** 0.88** | 10.319 17.555 | 0.714 0.770 | ||||
Q15 | 0.77** 0.91** | 9.269 18.951 | 0.592 0.821 | ||||
Regimen related | Q6 | 0.86** 0.91** | Fixed Fixed | 0.731 0.828 | |||
Distress (RRD) | Q12 | 0.68** 0.85** | 8.432 16.568 | 0.456 0.731 | |||
Q16 | 0.86** 0.78** | 11.888 13.902 | 0.739 0.615 | ||||
Q5 | 0.66** 0.60** | 8.157 9.001 | 0.434 0.355 | ||||
Q10 | 0.69** 0.90** | 8.699 18.841 | 0.477 0.817 | ||||
Interpersonal | Q17 | 0.87** 0.88** | Fixed Fixed | 0.754 0.768 | |||
Distress (IP) | Q7 | 0.77** 0.87** | 10.197 14.972 | 0.600 0.749 | |||
Q13 | 0.85** 0.84** | 11.595 14.348 | 0.724 0.711 | ||||
PSWQ | Q5 | 0.898** 0.911** | Fixed Fixed | 0.807 0.831 | 0.971 0.980 | 0.699 0.769 | 0.971 0.980 |
(Q8 removed) | Q7 | 0.869** 0.929** | 14.875 21.816 | 0.756 0.862 | |||
Q4 | 0.893** 0.909** | 15.860 20.461 | 0.797 0.827 | ||||
Q15 | 0.897** 0.909** | 16.073 20.459 | 0.805 0.827 | ||||
Q14 | 0.882** 0.911** | 15.400 20.589 | 0.778 0.830 | ||||
Q3 | 0.849** 0.906** | 14.077 20.246 | 0.720 0.821 | ||||
Q13 | 0.877** 0.897** | 15.162 19.691 | 0.768 0.805 | ||||
Q10 | 0.859** 0.891** | 14.457 19.320 | 0.737 0.793 | ||||
Q11 | 0.835** 0.896** | 13.590 19.659 | 0.697 0.804 | ||||
Q2 | 0.846** 0.883** | 13.976 18.879 | 0.715 0.780 | ||||
Q6 | 0.829** 0.873** | 13.398 18.337 | 0.688 0.762 | ||||
Q16 | 0.771** 0.856** | 11.630 17.465 | 0.594 0.733 | ||||
Q9 | 0.765** 0.789** | 11.459 14.628 | 0.585 0.622 | ||||
Q12 | 0.727** 0.802** | 10.509 15.133 | 0.529 0.644 | ||||
Q1 | 0.715** 0.772** | 10.205 14.020 | 0.511 0.596 | ||||
FFS | Q1 | 0.902** 0.908** | Fixed Fixed | 0.814 0.825 | 0.925 0.909 | 0.673 0.632 | 0.916 0.899 |
(Q7 removed) | Q2 | 0.883** 0.911** | 14.786 18.916 | 0.779 0.829 | |||
Q6 | 0.792** 0.838** | 11.877 15.742 | 0.628 0.702 | ||||
Q4 | 0.828** 0.764** | 12.925 13.188 | 0.685 0.584 | ||||
Q3 | 0.836** 0.762** | 13.175 13.103 | 0.699 0.580 | ||||
Q5 | 0.659** 0.521** | 8.773 7.527 | 0.434 0.271 | ||||
DEX (3 factors) | Q8 | 0.706** 0.722** | Fixed Fixed | 0.498 0.521 | 0.915 0.919 | 0.477 0.489 | 0.881 0.882 |
DEX: Volition | Q19 | 0.756** 0.746** | 7.641 9.285 | 0.571 0.557 | |||
Q10 | 0.627** 0.778** | 6.437 9.669 | 0.393 0.606 | ||||
Q4 | 0.704** 0.713** | 7.174 8.888 | 0.496 0.509 | ||||
Q18 | 0.748** 0.776** | 7.578 9.646 | 0.560 0.603 | ||||
DEX: Inhibition | Q9 | 0.666** 0.687** | Fixed Fixed | 0.444 0.471 | |||
Q2 | 0.691** 0.544** | 6.654 6.477 | 0.477 0.296 | ||||
Q17 | 0.707** 0.813** | 6.779 9.146 | 0.499 0.661 | ||||
Q16 | 0.735** 0.632** | 6.997 7.431 | 0.541 0.400 | ||||
Q15 | 0.610** 0.615** | 5.989 7.247 | 0.372 0.378 | ||||
DEX: Social | Q20 | 0.763** 0.682** | Fixed Fixed | 0.582 0.465 | |||
Regulation | Q13 | 0.535** 0.639** | 3.892 5.112 | 0.286 0.408 | |||
CD-RISC: | Q5 | 0.808** 0.756** | Fixed Fixed | 0.652 0.572 | 0.955 0.950 | 0.504 0.477 | 0.954 0.949 |
Q9,18,20,3 removed | Q17 | 0.805** 0.744** | 10.644 10.380 | 0.648 0.554 | |||
Q4 | 0.788** 0.761** | 10.329 10.659 | 0.621 0.580 | ||||
Q11 | 0.809** 0.734** | 10.723 10.214 | 0.654 0.538 | ||||
Q23 | 0.704** 0.787** | 8.877 11.076 | 0.495 0.619 | ||||
Q22 | 0.821** 0.696** | 10.957 9.619 | 0.674 0.485 | ||||
Q7 | 0.770** 0.723** | 10.009 10.049 | 0.593 0.523 | ||||
Q21 | 0.756** 0.719** | 9.770 9.985 | 0.572 0.518 | ||||
Q24 | 0.730** 0.741** | 9.310 10.322 | 0.533 0.548 | ||||
Q14 | 0.710** 0.737** | 8.977 10.266 | 0.504 0.543 | ||||
Q8 | 0.710** 0.699** | 8.973 9.668 | 0.503 0.489 | ||||
Q12 | 0.666** 0.728** | 8.274 10.122 | 0.443 0.530 | ||||
Q25 | 0.682** 0.706** | 8.528 9.772 | 0.465 0.498 | ||||
Q16 | 0.711** 0.641** | 8.995 8.763 | 0.505 0.410 | ||||
Q19 | 0.751** 0.613** | 9.679 8.353 | 0.564 0.376 | ||||
Q15 | 0.707** 0.634** | 8.927 8.669 | 0.499 0.402 | ||||
Q6 | 0.613** 0.636** | 7.472 8.694 | 0.376 0.405 | ||||
Q1 | 0.654** 0.607** | 8.086 8.256 | 0.427 0.368 | ||||
Q13 | 0.549** 0.628** | 6.553 8.574 | 0.301 0.395 | ||||
Q10 | 0.530** 0.613** | 6.295 8.350 | 0.281 0.376 | ||||
Q2 | 0.527** 0.551** | 6.251 7.429 | 0.277 0.303 |
Appendix 4: Bootstrapping Mediation Analysis in Type 1 Diabetes Group
To confirm the presence of mediation, bootstrapping was used to calculate direct and indirect effects in type 1 diabetes (see below).
Mediation analysis in type 1 diabetes | |||
|---|---|---|---|
Hypothesis | Direct Effect | Indirect Effect | Result |
Anxiety → Res → D.Distress | − 0.018 (ns) | 0.086** | Sig Mediation |
Anxiety → Res → Cognition | − 0.007 (ns) | 0.069** | Sig Mediation |
Fatigue → Res → D.Distress | n/a | 0.299** | Sig Mediation |
Fatigue → Res → Cognition | 0.023 (ns) | 0.240** | Sig Mediation |
Appendix 5: Bootstrapping mediation analysis in Type 2 diabetes group
To confirm the presence of mediation, bootstrapping was used to calculate direct and indirect effects in type 2 diabetes (see below).
Mediation analysis in type 2 diabetes | |||
|---|---|---|---|
Hypothesis | Direct Effect | Indirect Effect | Result |
Anxiety → Res → D.Distress | − 0.001 (ns) | 0.059** | Sig Mediation |
Anxiety → Res → Cognition | 0.008 (ns) | 0.061** | Sig Mediation |
Fatigue → Res → D.Distress | n/a | 0.201** | Sig Mediation |
Fatigue → Res → Cognition | 0.026 (ns) | 0.209** | Sig Mediation |
Appendix 6: Fit Statistics of alternative model comparisons for Type 1 and 2 diabetes
Model | χ2 | df | ∆ χ2 | ∆df | χ2/df | CFI | RMSEA | SRMR |
|---|---|---|---|---|---|---|---|---|
Base model (see Fig. 1) | 139.905 | 58 | – | – | 2.41 | 0.94 | 0.07 | 0.07 |
Model 1 | 142.843 | 60 | 2.938** | 2 | 2.38 | 0.94 | 0.07 | 0.07 |
Model 2 | 141.464 | 60 | 1.559** | 2 | 2.34 | 0.94 | 0.07 | 0.07 |
Model 3 | 141.580 | 60 | 1.675** | 2 | 2.36 | 0.94 | 0.07 | 0.07 |
Model 4 | 146.908 | 64 | 7.003** | 6 | 2.30 | 0.94 | 0.07 | 0.07 |
**p<0.001; *p.<0.05
Model 1: The path of Hypothesis 1 (H1 Anxiety/Worry → Diabetes Distress) was constrained to zero.
Model 2: The path of Hypothesis 3 (H2 Anxiety/Worry → Cognition) was constrained to zero.
Model 3: The path of Hypothesis 4 (H3 Fatigue → Cognition) was constrained to zero.
Model 4: The paths of hypotheses 1,2 & 3 were constrained to zero.

Proposed Structural Model: Psychological States (Anxiety/Worry, Fatigue), and Diabetes Outcomes (Diabetes Distress, Cognition), with Resilience as Mediator. Key: PSWQ (Penn State Worry Questionnaire); FFS (Flinder’s Fatigue Scale); CD−RISC (Connor-Davidson Resilience Scale), DDS (Diabetes Distress Scale, using four subscales: Emotional Burden, Physician Related Distress, Regimen Related Distress, Interpersonal Distress); DEX (Dysexecutive Questionnaire, using three subscales: Volition, Inhibition and Social Regulation). The proposed structural model shows association pathways between predictor variables (anxiety, fatigue) and diabetes outcome variables (diabetes distress, cognition), mediated by resilience. The boxes indicate the measures used to assess their respective variable

Structural Model for T1DM. The structural model shows pathway coefficients between predictor variables, resilience and diabetes outcome variables in the T1DM group. All indirect pathways (i.e. involving the mediator) were significant, and direct pathways were non-significant) *** p = < 0.001, ** p = < 0.05

Structural Model for T2DM. The structural model shows pathway coefficients between predictor variables, resilience and diabetes outcome variables in the T2DM group. All indirect pathways (i.e. involving the mediator) were significant, and direct pathways were non-significant) *** p = < 0.001, ** p = < 0.05

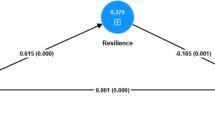
Final Structural Model for T1DM and T2DM. This shows the most parsimonious model, with all non-significant paths removed. All indirect pathways (i.e., involving the mediator) were significant at the p < 0.001 level. Standardised beta coefficients are provided for each pathway, indicating effect strength and direction of each predictor variable on outcome variable, and R2 values indicate the amount of variance explained by the independent variables (T2DM values are formatted in bold, underlined)
Dataset availability
The datasets generated and analysed during the current study are available from the corresponding author on reasonable request.
References
Zaccardi F, Webb DR, Yates T, Davies MJ (2016) Pathophysiology of type 1 and type 2 diabetes mellitus: a 90-year perspective. Postgrad Med J 92(1084):63–69. https://doi.org/10.1136/postgradmedj-2015-133281
National Health Service, NHS (2021) National Diabetes Audit, 2019–20. Care Processes and Treatment Targets: England and Wales
Wylie TAF, Shah C, Connor R, Farmer AJ, Ismail K, Millar B, Morris A, Reynolds RM, Robertson E, Swindell R, Warren E, Holt RIG (2019) Diabetes UK Position Statements. Transforming mental wellbeing for people with diabetes: research recommendations from Diabetes UK’s 2019 Diabetes and Mental Well-Being Workshop. Diabetes Med 36(12):1532–38. https://doi.org/10.1111/dme.14048
Robinson DJ, Coons M, Haensel H, Vallis M, Yale JF (2018) Diabetes and mental health. Can J Diabetes 42(1):S130–S141
Forouhi NG, Wareham NJ (2019) Epidemiology of diabetes. Medicine 47(1):22–27. https://doi.org/10.1016/j.mpmed.2018.10.004
Terte I, Stephens C, Huddleston L (2014) The development of a three-part model of psychological resilience. Stress Health 30(5):416–424
Yi-Frazier JP, Yaptangco M, Semana S, Buscaino E, Thompson V, Cochrane K, Tabile M, Alving E, Rosenberg AR (2015) The association of personal resilience with stress, coping, and diabetes outcomes in adolescents with type 1 diabetes: variable- and person-focused approaches. J Health Psychol 20(9):1196–1206. https://doi.org/10.1177/1359105313509846
Fritschi C, Quinn L (2010) Fatigue in patients with diabetes: a review. J Psychosom Res 69(1):33–41. https://doi.org/10.1016/j.jpsychores.2010.01.021
Goendorp MM, Tack CJ, Steggink E, Bloot L, Bazelmans E, Knoop H (2014) Chronic fatigue in type 1 diabetes: highly prevalent but not explained by hyperglycaemia or glucose variability. Diabetes Care 37(1):73–80
Ba J, Chen Y, Liu D (2021) Fatigue in adults with type 2 diabetes: a systematic review and meta-analysis. West J Nurs Res 43(2):172–181
Fritschi C, Quinn L, Hacker ED, Penckofer SM, Wang E, Foreman M, Ferrans CE (2012) Fatigue in women with type 2 diabetes. Diabetes Education 38(5):662–672
Griggs S, Morris NS (2018) Fatigue among adults with type 1 diabetes mellitus and implications for self-management: an integrative review. Diabetes Educ 44(4):325–339. https://doi.org/10.1016/S1262-3636(08)73394-9
Hidayat BF, Sukartini T, Kusumaningrum T (2020) A systematic review of fatigue in type 2 diabetes. Journal Ners, Special Issues 15(2):513–517
Hill S, Gingras J, Gucciardi E (2013) The lived experience of Canadian university students with type 1 diabetes mellitus. Can J Diabetes 37(4):237–242
Menting J, Nikolaus S, van der Veld. (2016) Severe fatigue in type 1 diabetes: exploring its course, predictors and relationship with HbA1c in a prospective study. Diabetes Res Clin Pract 121:127–134
Nguyen LA, Pouwer F, Winterdijk P et al (2020) Prevalence and course of mood and anxiety disorders, and correlates of symptom severity in adolescents with type 1 diabetes: results from diabetes LEAP. Pediatr Diabetes 22:638–648. https://doi.org/10.1111/pedi.13174
Pietrzak RH, Maruff P, Woodward M, Fredrickson J, Fredrickson A, Krystal JH, Darby D (2012) Mild worry symptoms predict decline in learning and memory in healthy older adults: a 2-year prospective cohort study. Am J Geriatr Psychiatry 20(3):266–275. https://doi.org/10.1097/JGP.0b013e3182107e24
Raffield LM, Brenes GA, Cox AJ, Freedman BI, Hugenschmidt CE, Hsu F, Xu J, Wagner BC, Williamson JD, Maldjian JA, Bowden DW (2016) Associations between anxiety and depression symptoms and cognitive testing and neuroimaging in type 2 diabetes. J Diabetes Complications 30(1):143–149
Shaban C, Fosbury JA, Cavan DA, Kerr D, Skinner TC (2009) The relationship between generic and diabetes specific psychological factors and glycaemic control in adults with type 1 diabetes. Diabetes Res Clin Pract 85(5):e26–e29
Frazao MCLO, Pimenta CJL, Silva CRR, Vicente MC, Costa TF, Costa KNFM (2018) Resilience and functional capacity of elderly people with diabetes mellitus. Rev Rene 19:3323
Hood KK, Iturralde E, Rausch J., Weissberg-Benchell J (2018). Preventing diabetes distress in adolescents with type 1 diabetes: results 1 year after participation in the STePS Program. Diabetes Care 1 August 41(8):1623–1630. https://doi.org/10.2337/dc17-2556
Murdock KW, LeRoy AS, Lacourt TE, Duke DC, Heijnen CJ, Fagundes C (2016) Executive functioning and diabetes: the role of anxious arousal and inflammation. Psychoendocrinology 71:102–109
Ruiz-Aranda D, Mateo-Rodriguez C, Olmedo IS, Garcia CG, Enriquez AJ, Martinez-Brocca MA (2020) relationship between resilience and quality of life in patients with fear of hypoglycaemia: the mediating effects of anxiety and depression. Sustainability 12(20):8512. https://doi.org/10.3390/su12208512
Santos FRM, Bernardo V, Gabbay MAL et al (2013) The impact of knowledge about diabetes, resilience and depression on glycaemic control: a cross-sectional study among adolescents and young adults with type 1 diabetes. Diabetol. Metab. Syndr 5(55). https://doi.org/10.1186/1758-5996-5-55
Scott SR, Ellisor BM, O’Donnell MB, O’Daffer A, Manczak EM, Malik F, Yi-Frazer J (2020). Both sides of the coin matter: Resilience and Distress one Year postdiagnosis are associated with long-term A1C outcomes in adolescents with Type I Diabetes Melitus. Am Diabetes Assoc 69(1)
Wang XG, Wen YQ, Kuang HB, Lin LX, Cui H (2021) The impacts of resilience on the association between illness uncertainty and sleep quality among patients with type 2 diabetes mellitus. Journal of Integrated Nursing 3:12–18
Wang R-H, Hsu H-C, Kao C-C, Yang Y-M, Lee Y-J, Shin S-J (2017) Associations of changes in psychosocial factors and their interactions with diabetes distress in patients with type 2 diabetes: a longitudinal study. J Adv Nurs 73(5):1137–1146. https://doi.org/10.1111/jan.13201
Vemuri P, Lesnick TG, Knopman DS, Przybelski SA, Reid RI, Mielke MM, Graff-Radford J, Lowe VJ, Machulda MM, Petersen RC, Jack CR (2019) Amyloid, vascular, and resilience pathways associated with cognitive aging. Ann Neurol 86(6):866–877. https://doi.org/10.1002/ana.25600
Hayes AF (2022). Introduction to mediation, moderation, and conditional process analysis: a regression based approach. Third edition, Guilford Press. ISBN 9781462549030.
Park H, Park C, Quinn L, Fritschi C (2015) Glucose control and fatigue in type 2 diabetes: the mediating roles of diabetes symptoms and distress. J Adv Nurs 71(7):1650–1660. https://doi.org/10.1111/jan.12632
Winkley K, Upsher R, Stahl D et al. (2020). Psychological interventions to improve glycemic control in adults with type 2 diabetes: a systematic review and meta-analysis. BMJ Open Diabetes Research and Care, 8:e001150. https://doi.org/10.1136/bmjdrc-2019-001150
Zhao F-F, Suhonen R, Koskinen S, Leino-Kilpi H (2017) Theory-based self-management educational interventions on patients with type 2 diabetes: a systematic review and meta-analysis of randomized controlled trials. J Adv Nurs 73(4):812–833. https://doi.org/10.1111/jan.13163
Amiri S, Behnezhad S (2019) Diabetes and anxiety symptoms: A systematic review and meta-analysis. Int J Psychiatry Med, 91217419837407. Advance online publication. https://doi.org/10.1177/0091217419837407
Boateng SL (2018) Structural equation modelling made easy: for business and social science research using SPSS and AMOS. Washington: independently published.
Wolf EJ, Harrington KM, Clark SL, Miller MW (2013) Sample size requirements for structural equation models: an evaluation of power, bias, and solution propriety. Educ Psychol Measur 76(6):913–934. https://doi.org/10.1177/0013164413495237
Sideridis G, Simos P, Papanicolaou A, Fletcher J (2014) Using structural equation modeling to assess functional connectivity in the brain power and sample size considerations. Educ Psychol Measur. https://doi.org/10.1177/0013164414525397
Hu L, Bentler PM (1999) Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct Equ Modeling 6(1):1–55. https://doi.org/10.1080/10705519909540118
Schrieber JB (2008) Core reporting practices in structural equation modelling. Res Social Adm Pharm 4(2):83–97
Cohen J (1988) Statistical power analysis for the behavioral sciences, 2nd edn. Lawrence Erlbaum Associates, Publishers, Hillsdale, NJ
Hair JF, Black WC, Babin BJ, Anderson RE (2010) Multivariate data analysis, 7th edn. Prentice Hall, Upper Saddle River, NJ
Lasselin J, Layé S, Barreau JB, Rivet A, Dulucq MJ, Gin H, Capuron L (2012) Fatigue and cognitive symptoms in patients with diabetes: relationship with disease phenotype and insulin treatment. Psychoneuroendocrinology 37(9):1468–1478
McCoy MA, Theeke LA (2019) A systematic review of the relationships among psychosocial factors and coping in adults with type 2 diabetes mellitus. Int J Nursing Sci 6(4):468–477. https://doi.org/10.1016/j.ijnss.2019.09.003
Sattar N (2013) Gender aspects in type 2 diabetes mellitus and cardiometabolic risk. Clin Endocrinol Metabolism 27:501–507
Windgassen S, Goldsmith K, Moss-Morris R, Chalder T (2016) Establishing how psychological therapies work: the importance of mediation analysis. J Ment Health 25(2):93–99. https://doi.org/10.3109/09638237.2015.1124400
Ketcham A, Matus A, Riegel B (2020) Resilience and depressive symptoms in adults with cardiac disease: a systematic review. J Cardiovasc Nurs 37(4):312–323
Macia G, S., Barranco, M., Alonso, E. & Iraurgi, I, (2022) Role of resilience and emotion control in relation to people with cancer. J Health Psychol 27(1):211–222
Defeudis G, Khazrai YM, Di Rosa C et al (2018) Conversation Maps™, an effective tool for the management of males and females with type 2 diabetes and mildly impaired glycemic control. Hormones 17:113–117. https://doi.org/10.1007/s42000-018-0005-9
Meyer TJ, Miller ML, Metzger RL, Borkovec TD (1990) Development and validation of the penn state worry questionnaire. Behav Res Ther 28(6):487–495
Gradisar M, Lack L, Richards H, Harris J, Gallasch J, Boundy M, Johnston A (2007) The Flinders Fatigue Scale: preliminary psychometric properties and clinical sensitivity of a new scale for measuring daytime fatigue associated with insomnia. J Clin Sleep Med 3(7):722–728
Polonsky WH, Fisher L, Earles J (2005) Assessing psychological distress in diabetes: development of the diabetes distress scale. Diabetes Care 28(3):626–631
Wilson BA, Alderman N, Burgess PW, Emslie H, Evans JJ (1996) Behavioural assessment of the dysexecutive syndrome: test manual. Thames Valley Test Company, England
Connor KM, Davidson JR (2003) Development of a new resilience scale: the Connor‐Davidson resilience scale (CD‐RISC). Depress Anxiety 18(2):76–82
Funding
This study was funded by the University of Central Lancashire, as part of a studentship PhD.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Consent
Study-specific approval was obtained from the University Ethics Committee, and informed consent was obtained from all individual participants included in the study; this includes consent for data to be published in a relevant journal.
Competing interests
All authors certify that they have no affiliations with or involvement in any organisation or entity with any financial interest in the subject matter or materials discussed in this manuscript.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article belongs to the topical collection Health Education and Psycho-Social Aspects, managed by Massimo Porta and Marina Trento.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Pate, R., Caswell, N., Gardner, K.J. et al. A structural equation model in adults with type 1 and 2 diabetes: exploring the interplay of psychological states and diabetes outcomes, and the mediating effect of resilience. Acta Diabetol 59, 1575–1587 (2022). https://doi.org/10.1007/s00592-022-01955-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00592-022-01955-3