
Abstract
Aims
The role of liver steatosis and increased liver enzymes (ALT) in increasing incident type 2 diabetes mellitus (T2DM) is debated, because of their differential effects on different ethnicities and populations. The aim of this study was to evaluate the role of elevated ALT in the development of T2DM in non-diabetic obese subjects receiving routine medical treatment.
Methods
A total of 1005 subjects [296 men and 709 women, aged 45.7 ± 13.12 years, body mass index (BMI) 39.5 ± 4.86 kg/m2] were followed for a mean period of 14.3 ± 4.44 years. Subjects were evaluated for several metabolic variables, including the triglyceride-glucose index and the presence of metabolic syndrome (IDF 2005 definition), and were subdivided into ALT quartiles.
Results
T2DM developed in 136 subjects, and the difference was significant between the first and the fourth ALT quartile (p = 0.048). Both at univariate analysis and at stepwise regression, ALT quartiles were associated with incident T2DM. Traditional risk factors for T2DM coexisted, with a somehow greater predictive value, such as triglyceride-glucose index, age, arterial hypertension, LDL-cholesterol, and metabolic syndrome.
Conclusions
These data suggest an association between elevated ALT levels and the risk of incident T2DM in obesity.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Several cross-sectional and prospective studies have shown that deterioration of glucose tolerance and incidence of type 2 diabetes mellitus (T2DM) in the general population are associated with elevated liver enzymes, even though with some discrepancies among different ethnic groups [1,2,3,4,5,6,7]; ALT was the main enzyme involved in the majority of studies, while in others the enzyme was γGT (γ-glutamil transferase) [2,3,4,5,6,7]. Obesity is often accompanied by elevated liver enzymes [5, 6, 8], and bariatric surgery (BS) is associated with decreases of body weight, ALT and AST levels, and with a reduced incidence of T2DM [8]. However, in obese subjects only cross-sectional studies have evaluated the association of T2DM with elevated liver enzymes [5, 6]. To better understand the possible role of liver enzymes in incident diabetes, in this study we retrospectively analyzed two cohorts of obese subjects that had been already evaluated for co-morbidities and mortality after routine medical treatment or BS [8, 9].
Materials and methods
This study is a second analysis of two studies aimed at evaluation of prevention of co-morbidities and of mortality in subjects undergoing BS versus control subjects receiving routine medical treatment, and details of the studies have already been published [8, 9]. It is important to remember that the National Health System (NHS) covers more than 95% of all hospital admissions, medical and surgical procedures and medical expenses of citizens [10] (Italian Survey 2012). The Regional Lumbardy Administrative Database contains since 1988 all pertinent data of all citizens, and in particular, the Lumbardy database collects several information, including (1) an archive of residents who receive NHS assistance, reporting demographic and administrative data; (2) a database on diagnosis at discharge from public or private hospitals of the region; (3) a database on outpatient drug prescriptions reimbursable by the NHS; and (4) a database on outpatient visits, including visits in specialist ambulatory care and diagnostic laboratories accredited by the NHS. For each patient, these databases are linked through a single identification code. The Italian National Health System keeps record of all acute and chronic diseases (diabetes mellitus, liver and cardiovascular diseases, selected thyroid, renal, and lung diseases, among others). This system yields the right to exemption from medical charges (exemptions), that means life-long free prescriptions and examinations for any disease. Therefore, together with hospital admissions, exemptions were considered a proxy of development of chronic diseases. This procedure has previously been employed and validated [8, 11, 12].
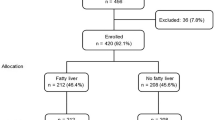
For this study, we considered only obese subjects without diabetes at baseline receiving routine medical treatment; subjects undergoing BS were excluded from the study, because BS can prevent incidence of T2DM [8]. Therefore, we analyzed a total of 1005 subjects (296 men and 709 women, aged 45.7 ± 13.12 years) which were followed for a mean period of 14.3 ± 4.44 years. Clinical, and laboratory characteristics of subjects under study are shown in Table 1, where subjects have been subdivided according to ALT quartiles. Diagnosis of incident diabetes was based on exemption together with date of exemption, and therefore only clinical diabetes was considered. The presence of the triglyceride-glucose index (TYG) was included [13], and metabolic syndrome was estimated according to the 2005 IDF definition [14].
Statistical analysis
Data of subjects in study were analyzed first as being part of ALT quartiles. One way analysis of variance (ANOVA) was employed to assess significant differences between data of subjects in the different ALT quartiles. Chi-square analysis was employed to assess distribution of subjects within each ALT quartile developing diabetes. Then, a univariate regression analysis was performed to assess association between each independent variable (all variables listed in Table 1) and incidence of diabetes. Finally, a stepwise regression was used to assess the risk of diabetes connected with independent variables statistically significant at univariate analysis. Various models of stepwise regression were used, with incident diabetes as the dependent variable (Table 2); age, sex, blood glucose, TYG index, glucose tolerance, arterial hypertension, LDL-cholesterol, ALT quartile, AST quartile, and metabolic syndrome were alternatively introduced as independent variables; triglycerides were generally omitted from models because of collinearity with age, TYG index, AST, ALT, and metabolic syndrome. p levels < 0.05 were considered statistically significant. All statistical analyses were performed through Stata, version 17.0, for MacIntosh.
Results
Table 1 shows that with increase of ALT quartiles, waist circumference also increased, as well as blood glucose and the triglyceride-glucose index, LDL-cholesterol, triglycerides, ALT, and AST, ALT, and frequency of metabolic syndrome. In contrast, age and sex ratio were different in the different ALT quartiles, and HDL-cholesterol decreased; mean values of blood glucose were within the normal range of values. At chi-square analysis, incidence of diabetes progressively increased with greater ALT quartiles (27/265, 30/261, 39/230, and 40/249, respectively, p = 0.068), although not significantly; when only 1st and 3rd ALT or 1st and 4th quartiles were compared, the difference was statistically significant (p = 0.0272 and p = 0.048, respectively, Table 2). The low statistical significance is likely due to the small sample size; in fact, when the whole sample was doubled in a simulation analysis, the overall analysis yielded a p value = 0.0026. At univariate regression analysis, age, waist circumference, blood glucose, TYG index and glucose tolerance, arterial hypertension, systolic BP, diastolic BP, LDL-cholesterol, triglycerides, metabolic syndrome, ALT and ALT quartile, but not AST or γGT, were all positively correlated with incident diabetes, while female sex, HDL-cholesterol and EGFR were negatively correlated with incident diabetes. At stepwise regression (Table 3), in Model 1, risk factors for incident diabetes were age, TYG index, LDL-cholesterol, ALT quartiles; when ALT quartiles are substituted by AST quartiles, only age (p = 0.043), TYG index (p = 0.001), and LDL cholesterol (p = 0.040) were statistically significant risk factors; # when TYG index was substituted by Blood Glucose, only Blood Glucose (p = 0.001) and LDL cholesterol (p = 0.016) were statistically significant risk factors. In Model 2, risk factors for incident diabetes were TYG index, LDL-cholesterol, and ALT quartile; when ALT quartiles are substituted by AST quartiles, only age (p = 0.009), TYG index (p = 0.001), and LDL cholesterol (p = 0.036) were statistically significant risk factors. In Model 3, age, ALT quartile, and metabolic syndrome were risk factors for incident diabetes; when ALT quartiles are substituted by AST quartiles, only age (p = 0.002), and Metabolic Syndrome (p = 0.001) were statistically significant risk factors. In Model 4, glucose tolerance, L-cholesterol, and ALT quartiles were risk factors for incident diabetes; when ALT quartiles are substituted by AST quartiles, only glucose tolerance (p = 0.001), and LDL cholesterol (p = 0.022) were statistically significant risk.
Discussion
In this study, markers of glucose metabolism (fasting blood glucose, TYG index, glucose intolerance and metabolic syndrome) and liver enzymes, mainly ALT, were predictors of incident diabetes in non-diabetic obese subjects receiving routine medical treatment over a mean follow-up of about 14 years. Raised liver enzymes, ALT and AST could be signs of MAFLD (NAFLD) [15] [16,17,18,19], and liver steatosis is a component of metabolic syndrome X/insulin resistance syndrome [18,19,20,21,22]. Therefore, it is not surprising that increased ALT levels were associated with incident diabetes in obese subjects receiving routine medical treatment. This association holds even at stepwise regression, albeit other traditional risk factors for diabetes coexist, with a somehow greater predictive value, such as TYG index, glucose tolerance, age, arterial hypertension, LDL-cholesterol, and metabolic syndrome, while blood glucose abolished the predictive role of ALT; of note, the fact that blood glucose levels were within the normal range of values, and that TYG index and glucose tolerance had a very strong predictive role. Of interest the fact that AST had no significant role, as already reported in other studies [3]; in contrast, cross-sectional studies in obese subjects [5, 6] reported a different role of ALT and γGT, probably linked to the different size of the studies and to the different ethnic groups considered. These data suggest an association between glucose metabolism and elevated ALT levels and the risk of T2DM in obesity in obese non-diabetic subjects receiving routine medical treatment. We should also recall that decrease of liver enzymes after bariatric surgery is not universal, and that subjects not showing decrease of liver enzymes after BS are affected by a more severe insulin resistance than other subjects [23], and therefore are likely to be at risk of future incidence of T2DM. Our data add to cross-sectional [5, 6] and prospective [1,2,3,4, 7] studies showing a predictive role of liver enzymes in incident diabetes; however, these data probably represent a particular aspect of morbid obesity, and cannot be generalized; for instance, sex distribution of our study is different from studies in the general population, as it is for the cross-sectional study mentioned above [6]. It is likely that in different populations [1, 5, 6], and in different subjects, like gestational diabetes [24], other factors are of greater importance than liver enzymes.
Abbreviations
- ALT:
-
Alanine transaminase
- T2DM:
-
Type 2 diabetes mellitus
- BMI:
-
Body mass index
- AST:
-
Aspartate transaminase
- BS:
-
Bariatric surgery
- TYG:
-
Triglyceride-glucose index
- LDL:
-
Low-density lipoprotein
- EGFR:
-
Estimated glomerular filtration rate
- HDL:
-
High-density lipoprotein
- BP:
-
Blood pressure
- MAFLD:
-
Metabolic dysfunction-associated fatty liver disease
References
Morinaga A, Iwanaga K, Maki K et al (2023) Association between serum ALT levels and incidence of new-onset diabetes in general population of japanese: a longitudinal observational study (ISSA-CKD). BMJ Open 13:e074007
Sattar N, Scherbakova O, Ford I et al (2004) West of Scotland coronary prevention study. Elevated alanine aminotransferase predicts new-onset type 2 diabetes independently of classical risk factors, metabolic syndrome, and C-reactive protein in the west of Scotland coronary prevention study. Diabetes 53(11):2855–60
Hanley AJ, Williams K, Festa A, Wagenknecht LE, D’Agostino RB Jr, Haffner SM (2005) Liver markers and development of the metabolic syndrome: the insulin resistance atherosclerosis study. Diabetes 54(11):3140–3147
Wannamethee SG, Shaper AG, Lennon L, Whincup PH (2005) Hepatic enzymes, the metabolic syndrome, and the risk of type 2 diabetes in older men. Diabetes Care 28(12):2913–2918
Rodríguez-Hernández H, Simental-Mendía LE, Bermúdez-Peña C, Zambrano-Galván G, Rodríguez-Morán M, Guerrero-Romero F (2012) Elevated alanine aminotransferase levels are associated with impaired fasting glucose and type 2 diabetes in obese women. Ann Hepatol 11(6):966
Zheng D, Zhang X, You L et al (2022) The association of liver enzymes with diabetes mellitus risk in different obesity subgroups: a population-based study. Front Endocrinol (Lausanne) 13(13):961762
Ben-Assayag H, Brzezinski RY, Berliner S et al (2023) Transitioning from having no metabolic abnormality nor obesity to metabolic impairment in a cohort of apparently healthy adults. Cardiovasc Diabetol 22(1):226
Pontiroli AE, Zakaria AS, Fanchini M et al (2018) A 23-year study of mortality and development of co-morbidities in patients with obesity undergoing bariatric surgery (Laparoscopic gastric banding) in comparison with medical treatment of obesity. Cardiovasc Diabetol 17:161. https://doi.org/10.1186/s12933-018-0801-1
Pontiroli AE, Ceriani V, Tagliabue E et al (2020) Bariatric surgery, compared to medical treatment, reduces morbidity at all ages but does not reduce mortality in patients aged < 43 years, especially if diabetes mellitus is present: a post hoc analysis of two retrospective cohort studies. Acta Diabetol 57:323–333. https://doi.org/10.1007/s00592-019-01433-3
www.agenziafarmaco.it, www.epicentro.iss.it/farmaci. Rapporto OSMED 2011, first published 2012. Accessed 22. 06. 2018
Corrao G, Ibrahim B, Nicotra F et al (2014) Statins and the risk of diabetes: evidence from a large population-based cohort study. Diabetes Care 37:2225–2232
Loreggian L, Giorgini F, Zakaria AS et al (2022) Baseline conditions and nutritional state upon hospitalization are the greatest risks for mortality for cardiovascular diseases and for several classes of diseases: a retrospective study. Sci Rep 12:10819
Alizargar J, Bai C-H, Hsieh N-C, Wu S-FV (2020) Use of the triglyceride-glucose index (TyG) in cardiovascular disease patients. Cardiovasc Diabetol 19:8. https://doi.org/10.1186/s12933-019-0982-2
Athyros VG, Ganotakis ES, Elisaf M, Mikhailidis DP (2005) The prevalence of the metabolic syndrome using the national cholesterol educational program and international diabetes federation definitions. Curr Med Res Opin 21:1157–1159. https://doi.org/10.1185/030079905x53333
Eslam M, Newsome PN, Sarin SK et al (2020) A new definition for metabolic dysfunction-associated fatty liver disease: an international expert consensus statement. J Hepatol 73(1):202–209. https://doi.org/10.1016/j.jhep.2020.03.039. (Epub 2020 Apr 8 PMID: 32278004)
Folini L, Veronelli A, Benetti A et al (2014) Liver steatosis (LS) evaluated through chemical-shift magnetic resonance imaging liver enzymes in morbid obesity; effect of weight loss obtained with intragastric balloon gastric banding. Acta Diabetol 51:361–368. https://doi.org/10.1007/s00592-013-0516-4
Frige’ F, Laneri M, Veronelli A et al (2009) Bariatric surgery in obesity: changes of glucose and lipid metabolism correlate with changes of fat mass. Nutr Metab Cardiovasc Dis NMCD 19:198–204. https://doi.org/10.1016/j.numecd.2008.04.005
Lombardi R, Colavolpe L, Alletto F et al (2023) Comparison of the severity of metabolic, liver and cardiovascular damage in NAFLD patients attending the hepatology clinic over the last three decades. Dig Liver Dis Off J Ital Soc Gastroenterol Ital Assoc Study Liver. https://doi.org/10.1016/j.dld.2023.07.009
Rinella ME, Lazarus JV, Ratziu V et al (2023) A multi-society delphi consensus statement on new fatty liver disease nomenclature. J Hepatol. https://doi.org/10.1016/j.jhep.2023.06.003
Reaven GM (1988) Banting lecture 1988. Role of insulin resistance in human disease. Diabetes 1988(37):1595–1607. https://doi.org/10.2337/diab.37.12.1595
Velloso LA, Folli F, Sun XJ, White MF, Saad MJ, Kahn CR (1996) Cross-talk between the insulin and angiotensin signaling systems. Proc Natl Acad Sci USA 93:12490–12495. https://doi.org/10.1073/pnas.93.22.12490
Folli F, Kahn CR, Hansen H, Bouchie JL, Feener EP (1997) Angiotensin II inhibits insulin signaling in aortic smooth muscle cells at multiple levels. A potential role for serine phosphorylation in Insulin/Angiotensin II crosstalk. J Clin Invest 100:2158–2169. https://doi.org/10.1172/JCI119752
Gastaldelli A, Perego L, Paganelli M et al (2009) Elevated concentrations of liver enzymes and ferritin identify a new phenotype of insulin resistance: effect of weight loss after gastric banding. Obes Surg 19:80–86
Tseng S-T, Lee M-C, Tsai Y-T et al (2023) Risks after gestational diabetes mellitus in taiwanese women: a nationwide retrospective cohort study. Biomedicines 11:2120
Acknowledgements
This study was in part funded by the Ministry Health (Ricerca Corrente), Italy to IRCCS MultiMedica, Milan (Italy), Fondazione Romeo and Enrica Invernizzi, Milan (Italy), and Università degli Studi di Milano, Milan, Italy.
Funding
Open access funding provided by Università degli Studi di Milano within the CRUI-CARE Agreement. This study was in part funded by the Ministry Health (Ricerca Corrente), Italy to IRCCS MultiMedica, Milan (Italy), Fondazione Romeo and Enrica Invernizzi, Milan (Italy), and Università degli Studi di Milano, Milan, Italy.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflict of interest.
Ethical Standard Statement
The Ethics Committee of IRCCS Multimedica notified the Authors that, because of the nature of the study (non-interventional retrospective analysis of anonymized data), it could be approved without further analysis by the Ethics Committee.
Additional information
Managed By Massimo Porta.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Folli, F., Pontiroli, A.E., Zakaria, A.S. et al. Alanine transferase levels (ALT) and triglyceride-glucose index are risk factors for type 2 diabetes mellitus in obese patients. Acta Diabetol 61, 435–440 (2024). https://doi.org/10.1007/s00592-023-02209-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00592-023-02209-6