
Abstract
Objectives
8-Hydroxideoxyguanosine (8-OHdG) is a marker of oxidative stress, and Forkhead Box-O1 (FOXO1) is a transcription factor and signaling integrator in cell and tissue homeostasis. This study aims to determine FOXO1 and 8-OHdG levels in serum and saliva samples of periodontitis patients and to evaluate their relationship with clinical periodontal parameters.
Materials and Methods
Twenty healthy individuals, twenty generalized Stage III Grade B periodontitis patients, and nineteen generalized Stage III Grade C periodontitis patients were included in the study. Clinical periodontal parameters (plaque index (PI), probing depth (PD), bleeding on probing (BOP), and clinical attachment level (CAL)) were recorded. Salivary and serum 8-OHdG and FOX-O1 levels were analyzed by enzyme-linked immunosorbent assay (ELISA).
Results
Clinical periodontal parameters showed a statistically significant increase in periodontitis groups compared to the control group (p < 0.05). 8-OHdG salivary levels were significantly higher in both periodontitis groups compared to the control group. The salivary FOXO1 levels were significantly lower in both periodontitis groups compared to the control group. Salivary FOXO1 level had a low-grade negative correlation with BOP and salivary 8-OHdG level.
Conclusions
While reactive oxygen species increase in periodontal inflammation, low expression of FOXO1, an important transcription factor for antioxidant enzymes, supports that this molecule plays a vital role in tissue destruction, and FOXO1 can be seen as a potential immune modulator.
Clinical relevance
The role of FOXO1 in supporting antioxidant defense may suggest that FOXO1 is a candidate target for periodontitis treatment.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
All organisms have various enzymatic and nonenzymatic antioxidant defense systems to protect themselves from the harmful effects of oxidative stress (OS). Under normal physiological conditions, there is a dynamic balance between reactive oxygen species (ROS) and antioxidant system (AO). When the balance disappears in favor of ROS, OS occurs with a decrease in antioxidant defense and/or an increase in ROS activity and causes varying degrees of damage to tissues [1, 2], such as depolymerization of extracellular matrix components, lipid peroxidation, oxidation of enzymes such as antiproteases, induction of proinflammatory cytokines and DNA damage [3, 4].
8-hydroxydeoxyguanosine (8-OHdG) is an oxidized nucleoside released by DNA damage. Studies have shown that 8-OHdG in body fluids acts as an oxidative stress marker and is used to evaluate oxidative damage in disorders, including chronic inflammatory diseases [5,6,7,8].
FOXOs are members of the O (other) class of the Forkhead superfamily called FKHR (forkhead rhabdomyosarcoma) [9]. Four members of this class are known as FOXO1, FOXO3, FOXO4, and FOXO6. While FOXO1, FOXO3, and FOXO4 play a role in apoptosis signaling [10, 11], FOXO1 and FOXO6 antagonize oxidative stress through the transcription of manganese superoxide dismutase, which catalyzes the conversion of O2− to H2O2 [12, 13]. It helps cells maintain and counteract the effect of ROS by stimulating cell cycle inhibition [11, 14]. It has been observed that FOXO1 overexpression protects periodontal ligament cells against oxidative damage and increases their osteogenic capacity in the inflammatory setting [15].
As a result of studies examining the role of FOXO1 in antioxidant defense, it has been revealed that it is associated with some systemic inflammatory diseases such as cardiovascular diseases [16], brain diseases [17], and skeletal muscle diseases [18], but there is not enough data on its relationship with periodontitis. In this study, we tested the hypothesis that the FOXO1 may regulate antioxidant mechanisms in periodontal inflammation and aimed to evaluate the salivary and serum FOXO1 and 8-OHdG levels in advanced periodontitis patients.
Materials and Methods
Study Population
This cross-sectional study conducted at the Department of Periodontology, School of Dentistry, Ankara University, included a total of 39 systematically healthy non-smoker patients with generalized Stage III periodontitis (20 participants for the Grade B group and 19 participants for the Grade C group), and 20 systematically and periodontally healthy non-smoker individuals.
The study received ethical approval from the Human Subject's Ethics Board of Ankara University (Approval No: 03/10, dated 03.02.2021) and was conducted in compliance with the principles outlined in the Helsinki Declaration. Written consent was obtained from all participants before their involvement in the study.
The diagnosis was based on the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions [19]. Periodontally healthy individuals were defined as having a probing depth (PD) ≤ 3 mm and no signs of inflammation. The diagnosis of Stage III periodontitis was made in patients exhibiting interdental radiographic bone loss of ≥ 2 mm in nonadjacent, distinct teeth, or buccal or oral radiographic bone loss up to 15% with a PD of > 3 mm for ≥ 2 teeth. The additional condition for Grade B was % bone loss/age 0.25–1, and for Grade C was % bone loss/age > 1 [19].
We excluded individuals from the study who had taken antibiotics, anti-inflammatory or immunosuppressive drugs, or contraceptives within the three months leading up to the research. Patients were excluded if they met any one of the following conditions: systemic disease (diabetes mellitus, rheumatoid arthritis, hypertension, metabolic syndrome, obesity), pregnancy, antibiotics, or anti-inflammatory medication for the last three months, active periodontal treatment in the previous six months, periodontal surgery in the last year, medications affecting the gingiva (e.g., calcium channel blocker, phenytoin, or cyclosporine). All participants were non-smokers, i.e., never smokers or had reportedly quit for a minimum period of 2 years before enrollment [20].
Periodontal Clinical Parameters
All study participants were evaluated clinically on their first visit to the Departments of Periodontology by one trained and calibrated examiner (ESG). Full mouth periodontal examination included clinical measurements of probing depth (PD), clinical attachment level (CAL), and plaque index (PI) [21], recorded to the nearest mm, and bleeding on probing (BOP) (%) [22]. Clinical parameters were recorded at six tooth sites (mesio-buccal, mid-buccal, disto-buccal, mesio-lingual, mid-lingual, and disto-lingual).
Saliva and Serum Sampling
Each patient was instructed on the collection protocol, and unstimulated saliva samples were obtained from them in the early hours of the day (between 9:00 am and 11:00 am). The participants were instructed to rinse their mouths with distilled water and sit comfortably while spitting into plastic tubes for 5 min. Subsequently, the saliva samples were centrifuged at 2800 × g for 10 min, and the resulting supernatant was transferred to Eppendorf tubes [7].
Standard venipuncture was performed for venous blood sample collection, and the samples were allowed to clot at room temperature for 30 min. Following clotting, the blood samples were centrifuged at 3000 × g for 10 min to separate the serum. All samples were stored at -80 °C until the day of analysis [7].
8-OHdG and FOX-O1 Analysis
The levels of 8-OHdG and FOX-O1 in serum and saliva samples were measured using commercially available ELISA kits.Footnote 1 The assays were conducted following the instructions provided by the manufacturers, and colorimetric assessment was carried out using a microplate reader set at a wavelength of 450 nm2. The intra- and inter-assay accuracy for FOXO1 and 8-OHdG was 10% and 12%, respectively. The minimum detection ranges for the assays were as follows: FOXO1, 0.312-20 ng/mL; 8-OHdG, 74.07–6,000 pg/mL. Each sample was analyzed twice, and the average of the results was used for subsequent calculations.
Statistical Analyses
Sample size analysis was performed a priori using specific software.Footnote 2 Considering a large effect size (1) for the analysis involving three groups, an α-error of 0.05, and a power of 80%, the total sample size was 51 participants. However, considering the possibility of confounders and incomplete data, the study was designed to include 59 patients.
All analyses were performed using commercially available statistical software.Footnote 3 Shapiro Wilk test was used to evaluate whether data were normally distributed. Chi-square test was applied for categorical variables. The t-test was used between the two independent groups.
The Bonferroni test was used as a "one-way ANOVA test" multiple comparison test to compare variables among the three groups. The Kruskal–Wallis test was used for data that were not normally distributed. Correlations between biochemical and periodontal clinical parameters were performed using Spearman correlation analysis. A value of p < 0.05 was considered significant.
Results
Study Population and Periodontal Clinical Parameters
Systemically healthy, twenty patients with Stage III Grade B periodontitis (SIIIGB, nine females, 11 males; 27–61 years old, mean 38.9 ± 10.17) and nineteen patients with generalized Stage III Grade C periodontitis (SIIIGC, 11 females, eight males; 19–41 years old, mean 27.53 ± 5.46), and twenty periodontally healthy subjects (C, 11 females and nine males; 23–49 years old, mean 30.75 ± 8.6) were included in the study.
Demographic and periodontal clinical parameters are presented in Table 1. Periodontitis group had significantly higher clinical periodontal parameters than the control group (p < 0.05). The mean age of the SIIIGB group was statistically significantly higher than the other two groups (p < 0.05), but there was no significant difference between the groups in terms of gender, body mass index, and saliva flow rate (p > 0.05).
Biochemical Parameters
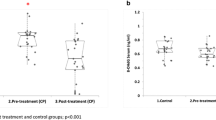
Salivary and serum 8-OHdG and FOXO1 levels are presented in Fig. 1. Salivary 8-OHdG levels were statistically significantly increased in the periodontitis groups compared to the control group (p < 0.05). Salivary FOXO1 levels were statistically significantly decreased in the periodontitis groups compared to the control group. However, no significant difference was found between the periodontitis groups in terms of 8-OHdG and FOXO1 levels (p > 0.05). Serum 8-OHdG and FOXO1 levels were similar in periodontitis and control groups (p > 0.05).

Salivary and serum levels of 8-OHdG and FOXO1
Correlations Between Periodontal and Biochemical Parameters
The correlation between periodontal and biochemical parameters is shown in Table 2. Salivary 8-OHdG level was positively correlated with all clinical periodontal parameters (p and rho values are 0.570/0.001 for PD; 0.573/ < 0.001 for BOP; 0.470/0.00; 0.600/ < 0.001 for CAL) and negatively correlated with serum 8-OHdG level (-0.259/0.048). Salivary FOXO1 level was negatively correlated with BOP (-0.336/0.010) and salivary 8-OHdG level (0.395/0.002).
Discussion
This study aimed to evaluate the salivary and serum FOXO1 and 8-OHdG levels in Stage III periodontitis patients. Based on the hypothesis that FOXO1 may regulate antioxidant mechanisms in periodontal inflammation, we evaluated and compared saliva and serum samples obtained from SIIIGB and SIIIGC with non-periodontitis healthy controls. While salivary 8-OHdG level was statistically significantly higher in periodontitis groups, salivary FOXO-1 level was significantly lower.
Recent studies have shown a significant relationship between periodontal disease and oxidative stress [23,24,25,26,27,28,29], and 8-OHdG is accepted as a sensitive indicator of DNA damage and a marker that defines oxidative stress [30, 31]. As a result of this study, salivary 8-OHdG levels were significantly higher in periodontitis groups than in the control group, consistent with the literature [32,33,34]. On the other hand, salivary 8-OHdG levels did not show significant difference between the periodontitis groups. Considering the literature data, 8-0HdG levels are accepted as a marker of periodontal inflammation [35, 36]. According to the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions [19], Stage III periodontitis is graded according to bone loss/age, and subclassification in our periodontitis group is made accordingly. It was evaluated whether there was a difference between these grades regarding oxidative stress and FOXO. As a result of this evaluation, no difference was found between Grade B and Grade C.
Although there is a difference in salivary 8-OHdG levels between the periodontitis and control groups, serum 8-OHdG levels were similar in periodontitis and control groups. Similarly, Konopka et al. observed no difference in serum 8-OHDg levels between periodontitis and control groups [37]. The researchers concluded that the oxidative burst observed in periodontitis is extensive enough to cause significant DNA damage at the local level. The level of 8-OHdG can be higher than the plasma concentration in the microcirculation and effectively change the redox status locally.
FOXO1, a transcription factor, plays a crucial role in regulating various cellular processes such as cell survival, differentiation, the reduction of ROS, and apoptosis [38, 39]. In the current study, salivary FOXO1 levels were statistically significantly lower in periodontitis groups than in the control group. Antioxidant systems are expected to be activated to prevent or reduce tissue damage caused by oxidative stress in periodontal disease. Accordingly, FOXO1 levels, whose antioxidant effect is known, could be expected to be higher in periodontitis groups. However, it can be thought that the high level of oxidative stress (8-OHdG) may prevent the functioning of antioxidant systems [40]. However, it is also known that ROS regulates the localization and activation of FOXO1. In case of an increase in OS, it causes FOXO1 to be inactivated by its acetylation by being transported out of the nucleus and reduces target gene expression [41]. On the other hand, it may be another interpretation to assume that the destruction is severe due to the insufficient functioning of the antioxidant mechanism in the periodontal destruction process. On the contrary, when activated, FOXO1 functions as a vital signal integrator, contributing to maintaining homeostasis and adapting to environmental shifts [42], which are crucial for periodontal health. Consequently, Ren et al. highlighted that disturbances in the normal signaling of FOXO1 could have implications for periodontal dysbiosis [43]. From this point of view, we can also consider that FOXO1 levels were lower than the control group in our study as the deterioration of physiological FOXO1 signal in periodontal inflammation. Interestingly, despite growing evidence indicating that periodontal pathogens can induce FOXO1 activity [43, 44] to maintain its intracellular existence by inhibiting apoptosis [44], the specific roles of FOXO1 in periodontal homeostasis and disease are not extensively documented.
FOXO1 plays a crucial role in regulating different aspects of mucosal immunity by influencing the migration and activation of dendritic cells, macrophages, and neutrophils. It also impacts the development and function of T-helper cells and B-lymphocytes [45,46,47]. Moreover, FOXO1 controls cytokine production, protects hematopoietic stem cells from oxidative stress, and regulates vital functions of keratinocytes, potentially contributing to the maintenance or restoration of the epithelial barrier [48, 49]. However, the effects and role of FOXO1 can vary depending on the specific conditions, such as diabetes [50, 51]. Consequently, predicting the impact of FOXO1 on various diseases can be challenging. In subsequent studies, examining the behavior of FOXO1 in different stages of periodontitis will highlight the intricate nature of FOXO. These findings indicate that epigenetic factors like high glucose levels or elevated oxidative stress highly regulate it.
The cross-sectional nature of this study is its main limitation; due to the study design, randomization in the selection of patients was not possible.
Our results showed a negative correlation between salivary 8-OHdG and FOXO1 levels. It is known that oxidative stress is one of the most critical factors in the tissue destruction mechanism in periodontal breakdown. In contrast, a deficiency in all antioxidant systems in the disease process is mentioned [52]. Considering all these, the negative correlation of FOXO1 saliva level with 8-OHdG may also be related to the nature of the disease.
Gaining a deeper understanding of the mechanisms involved in protection against oxidative stress, which is an essential factor in the development of periodontal disease, will be valuable for a more comprehensive understanding of the pathology of periodontitis. Literature data indicate that FOXO-1 may be a new therapeutic agent in some inflammatory diseases such as diabetes [53], obesity [54], and hypertension [55]. However, no study confirms FOXO1 as a therapeutic agent in periodontal disease. More in vitro and in vivo studies are needed to ensure the role of FOXO1 in promoting tissue regeneration in periodontitis, the immune system, and osteogenesis.
Conclusions
According to our results, the oxidative stress (8-OHdG)/antioxidant (FOXO1) ratio in patients with periodontitis varies in favor of oxidative stress compared to the healthy group. FOXO1 is an essential parameter of the antioxidant system that plays a role in the pathogenesis of periodontal disease, and this role should be elucidated in further studies.
Notes
ELISA Cloud Immunoassay, Cloud-Clone Corp, Houston, USA.
SPSS for Windows R4.
References
Abou Sulaiman AE, Shehadeh RM (2010) Assessment of total antioxidant capacity and the use of vitamin C in the treatment of non-smokers with chronic periodontitis. J Periodontol 81(11):1547–1554. https://doi.org/10.1902/jop.2010.100173
Bardaweel SK, Gul M, Alzweiri M, Ishaqat A, Salamat HAAL, Bashatwah RM (2018) Reactive Oxygen Species: the Dual Role in Physiological and Pathological Conditions of the Human Body. Eurasian J Med 50(3):193–201. https://doi.org/10.5152/eurasianjmed.2018.17397
Canakçi CF, Ciçek Y, Canakçi V (2005) Reactive oxygen species and human inflammatory periodontal diseases. Biochemistry (Mosc) 70(6):619–628. https://doi.org/10.1007/s10541-005-0161-9
Sies H (1997) Oxidative stress: oxidants and antioxidants. Exp Physiol 82(2):291–295. https://doi.org/10.1113/expphysiol.1997.sp004024
Chapple IL (2000) Matthews JB (2007) The role of reactive oxygen and antioxidant species in periodontal tissue destruction. Periodontol 43:160–232. https://doi.org/10.1111/j.1600-0757.2006.00178.x
Wu LL, Chiou CC, Chang PY, Wu JT (2004) Urinary 8-OHdG: a marker of oxidative stress to DNA and a risk factor for cancer, atherosclerosis and diabetics. Clin Chim Acta 339(1–2):1–9. https://doi.org/10.1016/j.cccn.2003.09.010
Önder C, Kurgan Ş, Altıngöz SM, Bağış N, Uyanık M, Serdar MA, Kantarcı A, Günhan M (2017) Impact of non-surgical periodontal therapy on saliva and serum levels of markers of oxidative stress. Clin Oral Investig 21(6):1961–1969. https://doi.org/10.1007/s00784-016-1984-z
Graille M, Wild P, Sauvain JJ, Hemmendinger M, Guseva Canu I, Hopf NB (2020) Urinary 8-OHdG as a Biomarker for Oxidative Stress: A Systematic Literature Review and Meta-Analysis. Int J Mol Sci 21(11):3743. https://doi.org/10.3390/ijms21113743
Barthel A, Schmoll D, Unterman TG (2005) FoxO proteins in insulin action and metabolism. Trends Endocrinol Metab 16(4):183–189. https://doi.org/10.1016/j.tem.2005.03.010
Dijkers PF, Medema RH, Lammers JW, Koenderman L, Coffer PJ (2000) Expression of the pro-apoptotic Bcl-2 family member Bim is regulated by the forkhead transcription factor FKHR-L1. Curr Biol 10(19):1201–1204. https://doi.org/10.1016/s0960-9822(00)00728-4
Nakamura T, Sakamoto K (2008) Forkhead transcription factor FOXO subfamily is essential for reactive oxygen species-induced apoptosis. Mol Cell Endocrinol 281(1–2):47–55. https://doi.org/10.1016/j.mce.2007.10.007
Klotz LO, Sánchez-Ramos C, Prieto-Arroyo I, Urbánek P, Steinbrenner H, Monsalve M (2015) Redox regulation of FoxO transcription factors. Redox Biol 6:51–72. https://doi.org/10.1016/j.redox.2015.06.019
Kim S, Koh H (2017) Role of FOXO transcription factors in crosstalk between mitochondria and the nucleus. J Bioenerg Biomembr 49(4):335–341. https://doi.org/10.1007/s10863-017-9705-0
Tothova Z, Kollipara R, Huntly BJ, Lee BH, Castrillon DH, Cullen DE, McDowell EP, Lazo-Kallanian S, Williams IR, Sears C, Armstrong SA, Passegué E, DePinho RA, Gilliland DG (2007) FoxOs are critical mediators of hematopoietic stem cell resistance to physiologic oxidative stress. Cell 128(2):325–339. https://doi.org/10.1016/j.cell.2007.01.003
Huang X, Chen H, Xie Y, Cao Z, Lin X, Wang Y (2019) FoxO1 Overexpression Ameliorates TNF-α-Induced Oxidative Damage and Promotes Osteogenesis of Human Periodontal Ligament Stem Cells via Antioxidant Defense Activation. Stem Cells Int 2019:2120453. https://doi.org/10.1155/2019/2120453
Kyriazis ID, Hoffman M, Gaignebet L, Lucchese AM, Markopoulou E, Palioura D, Wang C, Bannister TD, Christofidou-Solomidou M, Oka SI, Sadoshima J, Koch WJ, Goldberg IJ, Yang VW, Bialkowska AB, Kararigas G, Drosatos K (2021) KLF5 Is Induced by FOXO1 and Causes Oxidative Stress and Diabetic Cardiomyopathy. Circ Res 128(3):335–357. https://doi.org/10.1161/CIRCRESAHA.120.316738
Li W, Zhu Q, Xu X, Hu X (2021) MiR-27a-3p suppresses cerebral ischemia-reperfusion injury by targeting FOXO1. Aging (Albany NY) 13(8):11727–11737. https://doi.org/10.18632/aging.202866
Kosmas K, Michael Z, Papathanasiou AE, Spyropoulos F, Adib E, Jasuja R, Christou H (2022) Skeletal Muscle Dysfunction in Experimental Pulmonary Hypertension. Int J Mol Sci 23(18):10912. https://doi.org/10.3390/ijms231810912
Tonetti MS, Greenwell H, Kornman KS (2018) Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J Periodontol 89(1):S159–S172. https://doi.org/10.1002/JPER.18-0006
Buduneli N, Kardesler L, Isik H et al (2006) Effects of smoking and gingival inflammation on salivary antioxidant capacity. J Clin Periodontol 33:159–164
Silness J, Loe H (1964) Periodontal disease in pregnancy II. Correlation between oral hygiene and periodontal condition. Acta Odontol Scand 22:121–135
Ainamo J, Bay I (1975) Problems and proposals for recording gingivitis and plaque. Int Dent J 25(4):229–235
Emekli-Alturfan E, Yarat A, Çalışkan-Ak E, Pisiriciler R, Kuru B, Noyan Ü (2013) Determination of storage time of saliva samples obtained from patients with and without chronic periodontitis for the comparison of some biochemical and cytological parameters. J Clin Lab Anal 27(4):261–266. https://doi.org/10.1002/jcla.21592
Sundar NM, Krishnan V, Krishnaraj S, Hemalatha VT, Alam MN (2013) Comparison of the salivary and the serum nitric oxide levels in chronic and aggressive periodontitis: a biochemical study. J Clin Diagn Res 7(6):1223–1227. https://doi.org/10.7860/JCDR/2013/5386.3068
Nguyen TT, Ngo LQ, Promsudthi A, Surarit R (2016) Salivary Lipid Peroxidation in Patients With Generalized Chronic Periodontitis and Acute Coronary Syndrome. J Periodontol 87(2):134–141. https://doi.org/10.1902/jop.2015.150353
Akalin FA, Baltacioğlu E, Alver A, Karabulut E (2009) Total antioxidant capacity and superoxide dismutase activity levels in serum and gingival crevicular fluid in pregnant women with chronic periodontitis. J Periodontol 80(3):457–467. https://doi.org/10.1902/jop.2009.080218
Baltacıoğlu E, Kehribar MA, Yuva P, Alver A, Atagün OS, Karabulut E, Akalın FA (2014) Total oxidant status and bone resorption biomarkers in serum and gingival crevicular fluid of patients with periodontitis. J Periodontol 85(2):317–326. https://doi.org/10.1902/jop.2013.130012
Wei D, Zhang XL, Wang YZ, Yang CX, Chen G (2010) Lipid peroxidation levels, total oxidant status and superoxide dismutase in serum, saliva and gingival crevicular fluid in chronic periodontitis patients before and after periodontal therapy. Aust Dent J 55(1):70–78. https://doi.org/10.1111/j.1834-7819.2009.01123.x
Toczewska J, Maciejczyk M, Konopka T, Zalewska A (2020) Total Oxidant and Antioxidant Capacity of Gingival Crevicular Fluid and Saliva in Patients with Periodontitis: Review and Clinical Study. Antioxidants (Basel) 9(5):450. https://doi.org/10.3390/antiox9050450
Dizdaroglu M (1998) Facts about the artifacts in the measurement of oxidative DNA base damage by gas chromatography-mass spectrometry. Free Radic Res 29(6):551–563. https://doi.org/10.1080/10715769800300591
Valavanidis A, Vlachogianni T, Fiotakis C (2009) 8-hydroxy-2’ -deoxyguanosine (8-OHdG): A critical biomarker of oxidative stress and carcinogenesis. J Environ Sci Health C Environ Carcinog Ecotoxicol Rev 27(2):120–139. https://doi.org/10.1080/10590500902885684
Sawamoto Y, Sugano N, Tanaka H, Ito K (2005) Detection of periodontopathic bacteria and an oxidative stress marker in saliva from periodontitis patients. Oral Microbiol Immunol 20(4):216–220. https://doi.org/10.1111/j.1399-302X.2005.00215.x
Takane M, Sugano N, Iwasaki H, Iwano Y, Shimizu N, Ito K (2002) New biomarker evidence of oxidative DNA damage in whole saliva from clinically healthy and periodontally diseased individuals. J Periodontol 73(5):551–554. https://doi.org/10.1902/jop.2002.73.5.551
Takane M, Sugano N, Ezawa T, Uchiyama T, Ito K (2005) A marker of oxidative stress in saliva: association with periodontally-involved teeth of a hopeless prognosis. J Oral Sci 47(1):53–57. https://doi.org/10.2334/josnusd.47.53
Muthuraj M, Janakiram S, Chithresan K (2021) Is 8-OHdG a reliable marker in Periodontitis – the sixth complication of Diabetes mellitus? Clin Dent 15(6):12–17
Paredes-Sánchez E, Montiel-Company JM, Iranzo-Cortés JE, Almerich-Torres T, Bellot-Arcís C, Almerich-Silla JM (2018) Meta-analysis of the use of 8-OhDG in saliva as a marker of periodontal disease. Dis Markers 7916578. https://doi.org/10.1155/2018/7916578.
Konopka T, Król K, Kopeć W, Gerber H (2007) Total antioxidant status and 8-hydroxy-2’-deoxyguanosine levels in gingival and peripheral blood of periodontitis patients. Arch Immunol Ther Exp (Warsz) 55(6):417–422. https://doi.org/10.1007/s00005-007-0047-1
Deng Y, Wang F, Hughes T, Yu J (2018) FOXOs in cancer immunity: Knowns and unknowns. Semin Cancer Biol 50:53–64. https://doi.org/10.1016/j.semcancer.2018.01.005
Liang X, Su Y, Huo Y (2020) Forkhead box protein O1 (FoxO1) /SERPINB1 ameliorates ROS production in diabetic nephropathy. Food Sci Nutr 9(1):44–51. https://doi.org/10.1002/fsn3.1859
Zuo L, Zhou T, Pannell BK, Ziegler AC, Best TM (2015) Biological and physiological role of reactive oxygen species–the good, the bad and the ugly. Acta Physiol (Oxf) 214(3):329–348. https://doi.org/10.1111/apha.12515
Brunet A, Sweeney LB, Sturgill JF, Chua KF, Greer PL, Lin Y, Tran H, Ross SE, Mostoslavsky R, Cohen HY, Hu LS, Cheng HL, Jedrychowski MP, Gygi SP, Sinclair DA, Alt FW, Greenberg ME (2004) Stress-dependent regulation of FOXO transcription factors by the SIRT1 deacetylase. Science 303(5666):2011–2015. https://doi.org/10.1126/science.1094637
Tsuchiya K, Ogawa Y (2017) Forkhead box class O family member proteins: The biology and pathophysiological roles in diabetes. J Diabetes Investig 8(6):726–734. https://doi.org/10.1111/jdi.12651
Ren L, Yang J, Wang J, Zhou X (2021) Liu C (2021) The Roles of FOXO1 in Periodontal Homeostasis and Disease. J Immunol Res 2021:5557095. https://doi.org/10.1155/2021/5557095
Li S, Dong G, Moschidis A, Ortiz J, Benakanakere MR, Kinane DF, Graves DT (2013) P gingivalis modulates keratinocytes through FOXO transcription factors. PLoS One 8(11):e78541. https://doi.org/10.1371/journal.pone.0078541
Chung S, Ranjan R, Lee YG, Park GY, Karpurapu M, Deng J, Xiao L, Kim JY, Unterman TG, Christman JW (2015) Distinct role of FoxO1 in M-CSF- and GM-CSF-differentiated macrophages contributes LPS-mediated IL-10: implication in hyperglycemia. J Leukoc Biol 97(2):327–339. https://doi.org/10.1189/jlb.3A0514-251R
Dong G, Wang Y, Xiao W, Pacios Pujado S, Xu F, Tian C, Xiao E, Choi Y, Graves DT (2015) FOXO1 regulates dendritic cell activity through ICAM-1 and CCR7. J Immunol 194(8):3745–3755. https://doi.org/10.4049/jimmunol.1401754
Yusuf I, Zhu X, Kharas MG, Chen J, Fruman DA (2004) Optimal B-cell proliferation requires phosphoinositide 3-kinase-dependent inactivation of FOXO transcription factors. Blood 104(3):784–787. https://doi.org/10.1182/blood-2003-09-3071
Ponugoti B, Dong G, Graves DT (2012) Role of forkhead transcription factors in diabetes-induced oxidative stress. Exp Diabetes Res 2012:939751. https://doi.org/10.1155/2012/939751
Behl Y, Siqueira M, Ortiz J, Li J, Desta T, Faibish D, Graves DT (2008) Activation of the acquired immune response reduces coupled bone formation in response to a periodontal pathogen. J Immunol 181(12):8711–8718. https://doi.org/10.4049/jimmunol.181.12.8711
Xiao E, Graves DT (2015) Impact of Diabetes on the Protective Role of FOXO1 in Wound Healing. J Dent Res 94(8):1025–1026. https://doi.org/10.1177/0022034515586353
Eijkelenboom A, Burgering BM (2013) FOXOs: signalling integrators for homeostasis maintenance. Nat Rev Mol Cell Biol 14(2):83–97. https://doi.org/10.1038/nrm3507
Chen E, Wang T, Tu Y, Sun Z, Ding Y, Gu Z, Xiao S (2023) ROS-scavenging biomaterials for periodontitis. J Mater Chem B 11(3):482–499. https://doi.org/10.1039/d2tb02319a
Benchoula K, Arya A, Parhar IS, Hwa WE (2021) FoxO1 signaling as a therapeutic target for type 2 diabetes and obesity. Eur J Pharmacol 891:173758. https://doi.org/10.1016/j.ejphar.2020.173758
Dansen TB, Kalkhoven E (2015) Targeting FOXO1 as an option to treat obesity? Cell Cycle 14(16):2558. https://doi.org/10.1080/15384101.2015.1060779
Savai R, Al-Tamari HM, Sedding D, Kojonazarov B, Muecke C, Teske R, Capecchi MR, Weissmann N, Grimminger F, Seeger W, Schermuly RT, Pullamsetti SS (2014) Pro-proliferative and inflammatory signaling converge on FoxO1 transcription factor in pulmonary hypertension. Nat Med 20(11):1289–1300. https://doi.org/10.1038/nm.3695
Acknowledgements
The authors report no conflicts of interest related to this study.
Funding
Open access funding provided by the Scientific and Technological Research Council of Türkiye (TÜBİTAK). No funding was obtained for this study.
Author information
Authors and Affiliations
Contributions
ESG contributed to the study design, collected samples, recorded clinical data, helped interpret the results, and wrote the manuscript with input from other authors. ZG and SK contributed to the study design, helped collect samples, helped interpret the results, and wrote the manuscript with input from other authors. NB helped with sample collection. MAS contributed to biochemical analysis and study design, performed the statistical analysis, and helped interpret the results. MG contributed to the study design, overseeing the implementation of the study and helping with the interpretation of results and manuscript revision. All authors reviewed and approved the submitted final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
This study received ethical approval from the Human Subject's Ethics Board of Ankara University (Approval No: 03/10, dated 03.02.2021) to ensure the appropriate use and access of human subjects in research. The study was conducted in accordance with the principles outlined in the Helsinki Declaration.
Informed consent
Prior to the study, written consent was obtained from all participants.
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Gurbuz, E.S., Guney, Z., Kurgan, S. et al. Oxidative Stress and FOXO-1 Relationship in Stage III Periodontitis. Clin Oral Invest 28, 270 (2024). https://doi.org/10.1007/s00784-024-05670-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00784-024-05670-x