
Abstract
Purpose
In 2003, a dedicated Dutch committee developed evidence-based guidelines for the treatment of inguinal hernia (IH) in children and adults. The aim of this study was to describe trends in hernia care before and after the publication of the guidelines on IH surgery in the Netherlands.
Methods
Originally, a retrospective baseline analysis of IH surgery in 90 Dutch hospitals was performed among patients treated for IH in 2001. The results of this baseline analysis were compared with a recently performed second analysis of patients treated for IH in 2005.
Results
In children <4 years of age, the study showed a significant decrease of contralateral explorations. In adults, the study showed that significantly more patients were treated with a mesh-based repair in 2005 (95.9 vs. 78.8%, P < 0.01). Moreover, there was an increase of patients with bilateral hernia treated with an endoscopic technique (41.5 vs. 22.3%, P < 0.01) and more patients were treated in day surgery (53.5 vs. 38.6%, P < 0.01). Lastly, a decline in operations performed for recurrent IH in adults was observed (10.9 vs. 13.3%, P < 0.01).
Conclusion
This study showed that most patients with IH in the Netherlands were treated according to the main recommendations of the Dutch evidence-based guidelines.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
In 2003, a Dutch committee developed evidence-based guidelines for the treatment of inguinal hernia (IH) in children and adults [1]. The guidelines for adults are mainly based on systematic reviews of randomised controlled trials (RCTs) with consistent results from individual (homogenous) studies, thus, creating level 1a evidence. In the guidelines for children, the level of evidence was 2b; RCTs of poorer quality or cohort or case–control studies. The main recommendations of these guidelines for children were first to perform a hernial sac resection with high ligation of the hernial sac, and second that contralateral exploration is not to be performed on a routine basis.
The main recommendations of the guidelines for adults were to use a mesh-based repair technique in adult patients (level 1a), preferably in day surgery (level 2b), and to consider local anaesthesia when performing open anterior repair (level 2c). For primary unilateral IH, the guidelines recommend a Lichtenstein repair technique (level 4). For recurrences after an anterior repair and bilateral hernia, an endoscopic repair technique is recommended, performed by a trained team (level 4). The guidelines, furthermore, consist of 20 chapters with recommendations on all aspects of IH treatment, from diagnosis to aftercare.
It was expected that the guidelines would improve the quality, efficiency and transparency of IH treatment [1]. To evaluate the implementation of these guidelines, published in 2002, a baseline analysis of IH surgery was performed among patients treated for IH in 2001 [2]. The results of this baseline analysis were compared with a second analysis of patients treated for IH in 2005, in order to describe trends in hernia care before and after the publication of the guidelines on IH surgery in the Netherlands. It was of primary interest to evaluate whether more patients with IH had been treated according to the main recommendations after the introduction of the guidelines. The secondary goal was to determine whether the recommendations had an effect on the percentage of operations performed for recurrences and other aspects, such as the frequency of ambulatory care surgery, type of anaesthesia, level of surgical expertise and complications.
Methods
To evaluate the implementation of the guidelines, a baseline study before their introduction had to be performed. A second study after the implementation could then serve as a comparison with the first study.
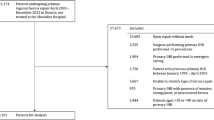
Consequently, a retrospective study was performed among patients treated for IH in the Netherlands in the period January–March 2001 [2]. The results of this study were used as the baseline values in comparison to the results of a second retrospective study of IH repairs performed over the period January–March 2005. The first retrospective data collection was performed in 2003 and the second data collection in 2007. Therefore, all patients had been operated upon at least a year prior to the data collection. In both studies, the exact same study design with original patient and operation charts was applied. For the first study, all Dutch hospitals (n = 130) were asked to participate. Of these 130 hospitals, 90 (69%) hospitals (52/72 teaching hospitals and 38/58 non teaching hospitals) participated. The 90 hospitals that had participated in the first analysis were all revisited. The following data were recorded: age, type of hospital (academic centre, teaching hospital or non-teaching hospital), admission or day surgery, operation for primary or recurrent hernia and previously used operation technique, unilateral or bilateral hernia, number of years after previous repair (in recurrent hernia), acute versus elective surgery, and the number and type of complications. The operation technique, the type of hernia and the type of anaesthesia were retrieved from the operation reports. Patients with bilateral hernia were evaluated as two separate hernias. Children (<18 years of age) and adults (≥18 years of age) were analysed separately.
Although the treatment of femoral hernias and IH can be similar, patients with femoral hernias were excluded from this study because of differences in pathology and incidence. In addition, the treatment of femoral hernias was not integrated in the guidelines.
Statistical analysis
Data were expressed as mean ± standard deviation (SD). Proportions were compared using Chi-square analysis with Yates’ correction. For all tests, a P-value <0.05 was considered to be significant.
Results
The study resulted in a total of 4,354 IH in 3,954 patients (children and adults) in 2001 and 5,374 IH in 4,846 patients in 2005.
Children
General findings
A total of 741 hernias in 691 children were operated in 2001, compared to 744 hernias in 696 children in 2005.
The patient, hernia and surgical characteristics are outlined in Table 1.
Operating techniques in children
Hernial sac resection in 2001 and 2005 was performed in 713 (96.2%) and 711 (95.6%) cases, respectively. In three cases (one patient with a bilateral hernia) in 2005, a hernial sac resection was performed using a laparoscopic technique. This was performed extraperitoneally in two patients and transabdominally in one patient. A hernioplasty (Bassini and Shouldice technique) was performed in 15 (2.1%) cases in 2001 and seven cases (0.9%) in 2005.
Mesh techniques were used in six (0.8%) cases in 2001 and 23 (3.1%) cases in 2005. In 2001 and 2005, the Lichtenstein technique was used in three (0.4%) and ten (1.3%) cases, respectively. The mean age of patients receiving a mesh repair was 15.4 years (range 12.0–17.8) in 2001 and 17.2 years (range 16.58–17.7) in 2005.
Acute or semi-acute surgery for strangulated or incarcerated hernia was performed in 44 (5.9%) patients in 2001 and 38 (5.1%) patients in 2005.
In children younger than 4 years of age, a contralateral exploration was performed in 45/404 (11.1%) children in 2001 and this decreased to 4/400 (1%) in 2005 (P < 0.01).
Complications
Complications were registered in 2001 and 2005 in 44 (5.9%) and 28 (3.8%) patients, respectively. In 13 (1.8%) patients in 2001 and ten (1.3%) patients in 2005, recurrences were reported within 12 months. All children in 2001 and nine in 2005 underwent a second operation.
Haematoma or seroma were reported in 12 (1.6%) cases in 2001 and seven (0.9%) cases in 2005. In 2001 one (0.1%) child and in 2005 four (0.5%) children suffered from postoperative bleeding, which resulted in reexploration in three cases.
There were 12 (1.8%) reports of pain in 2001; two of these patients suffered from chronic pain (one neuralgic, one somatic). In 2005, pain was reported in three (0.4%) patients, one of whom suffered from chronic pain (somatic). Both in 2001 and in 2005, two (0.3%) patients were reported to have developed wound infections.
Adults
General findings
A total of 3,613 hernia repairs in 3,263 patients were performed in 2001. In 2005, this was 4,630 and 4,150, respectively.
The patient, hernia and surgical characteristics are outlined in Table 2.
Operating techniques in adults
A mesh-based repair in 2001 and 2005 was performed in 2,847 (78.8%) and 4,442 (95.9%) IH operations, respectively.
The IH repair techniques used in both periods are shown in Table 3.
As shown in Table 3, a significant increase was found in the use of mesh techniques (P < 0.01). The Lichtenstein technique was the most often used technique both in 2001 and 2005, with a significant increase of 17.8% (from 40.2 to 58.0%) in 2005 (P < 0.01).
As for patients with bilateral hernia, endoscopic techniques were performed in 78 of 350 (22.3%) patients in 2001 and in 199 of 480 (41.5%) patients in 2005 (P < 0.01).
In both years, endoscopic techniques were performed more frequently in bilateral compared to unilateral hernias. In 2001, 13.4% (485 of 3,613) of all patients underwent an endoscopic technique compared to 22.3% (78 of 350) for bilateral hernias. In 2005, this was 18.5% (857 of 4,630) and 41.5% (199 of 480), respectively. In the case of recurrent IH, after an anterior repair, 90 (18.9%) and 116 (22.9%) patients in 2001 and 2005, respectively, were treated endoscopically (P = 0.126).
A total number of 71 (2.0%) and 82 (1.8%) patients underwent acute surgery for strangulated or incarcerated hernia in 2001 and 2005, respectively.
The average duration of hospitalisation in 2001 was 2.1 ± 2.0 days (range 1–40). In 2005, this was 1.8 ± 1.6 days (range 1–21).
Complications
One or more complications were registered in 499 (15.3%) patients in 2001 and 562 (13.5%) patients in 2005. The baseline analysis of the 2001 cohort reported (early) recurrences in 69 patients (1.9%). The recurrence rate of the second analysis was also 1.9% (88 patients).
Chronic pain (>3 months) was reported in 62 patients (1.7%) versus 95 patients (2.1%) in 2001 and 2005, respectively.
In both analyses, the majority of complications consisted of postoperative haematoma or seroma; 417 patients (11.5%) in 2001 and 375 patients (8.1%) in 2005.
Discussion
This study demonstrates that improvements have been made in the treatment of IH. Different factors can be responsible for changes in surgeons’ practice. Besides the introduction of the Dutch guidelines, attending scientific meetings, courses or reading literature, especially systematic reviews, can lead to changes in practice. The guidelines were well advertised and sent to each surgeon in hard copy. Various symposia were organised on this topic at the meeting of the Dutch Surgical Society. One drawback of this study is the retrospective character of the data, which may have caused bias in some aspects, which require further discussion.
Children
Few significant changes had occurred in IH surgery in children after the introduction of the guidelines. The majority of patients were being treated according to the guidelines; by hernial sac resection in day surgery under general anaesthesia. Laparoscopy in pediatric IH has been introduced in the Netherlands. Three patients were treated with an endoscopic procedure. Although the role of laparoscopic treatment of IH in children remains unclear, it may have its advantages in contralateral IH. The laparoscopic technique enables diagnosing a femoral hernia accompanied by an IH (preventing a pseudo recurrence). In addition, laparoscopic treatment results in a reduced operation time [3, 4].
A remarkable fact was the high incidence of patients treated for a recurrence within 1 year of follow-up in both analyses (2001 1.8%, 2005 1.3%). The relatively high percentages of early recurrences compared to the rate of 0.5–1% reported in the literature [5] should be considered as technical failures based on inadequate sac resection. There may have been recurrences in patients with insufficient internal rings, who should have undergone a hernioplasty.
The Dutch guidelines recommend that contralateral exploration should not be performed routinely, but can be considered in patients with a high risk of double-sided hernia, high risk of strangulation or a high risk of general anaesthesia (pre-matures) [1]. In 2005, the number of patients ≤4 years of age undergoing contralateral exploration had significantly decreased (11.1 vs. 1%, P < 0.01).
Adults
During the study period, the use of mesh-based operation techniques significantly increased by more than 17% to 95.9% in 2005.
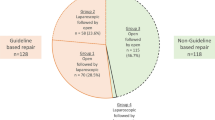
In addition, a significant increase in the use of endoscopic repairs for bilateral hernia was noted. In 2005, 41.5% of patients with bilateral hernias were treated according to the guidelines. Endoscopic techniques were performed more frequently in bilateral compared to unilateral hernia.
The upcoming of dedicated hernia centres and increased attention for IH surgery in the Netherlands during the past few years might have contributed to a higher volume of endoscopic repairs in the Netherlands.
The Dutch guidelines have stated that IH surgery in day surgery is as safe and effective as an inpatient setting, and is also more cost-effective [1]. Furthermore, IH surgery can be easily performed in day surgery, irrespective of the technique used [6, 7]. In accordance with these recommendations, a significant increase of patients treated in day surgery was found during the surveillance period (P < 0.01).
Open anterior IH techniques can be satisfactorily performed under local anaesthetic [8, 9]. The reduction of costs and a quicker return to normal activity in unilateral reducible IH are important factors [10]. The guidelines, therefore, recommend in the case of an open repair to consider local anaesthesia for all adult patients with a primary reducible unilateral IH [1]. Despite this recommendation, the study showed a significant decrease in the use of local anaesthetic (P < 0.01). This could be explained by unfamiliarity with the technique and insufficient training. Furthermore, improved safety and tolerability of general anaesthesia make local anaesthetic less appealing.
During the studied period (2001–2005), a significant decrease of operations performed for recurrences was shown (P < 0.01). Comparable results were found in a study concerning an Amsterdam teaching hospital [11]. This may possibly imply that the total number of recurrences is also decreasing. The increase of mesh-based techniques according to the Dutch evidence-based guidelines could provide an explanation. Furthermore, emphasis on IH surgery and training might have contributed to improved results [12, 13]. It has to be taken into account that the significant decrease only reflects operated recurrent hernias, as many patients with asymptomatic recurrences may not undergo repeated surgery. Although the recommendation of the guidelines was to consider the use of an endoscopic repair technique for recurrences after an anterior repair, only 22.9% of patients were treated accordingly.
Complications were not registered prospectively. The results should, therefore, be interpreted with caution. Early recurrence (<1 year) in 2005, as in 2001, was reported in 1.9% of patients. These are almost certainly caused by incorrect or inadequate operation technique, or a missed hernial sac, which, apparently, cannot be corrected with the use of mesh.
Currently, postoperative inguinal pain is a major endpoint. In this study, chronic pain was reported in 1.7% (2001) and 2.1% (2005) of patients. These percentages should be considered as underestimations due to the limitations of the retrospective study design since, in the literature overall, moderate to severe pain has been reported by 10–12% of patients [14, 15].
Conclusions
This study showed that most patients with inguinal hernia (IH) in the Netherlands were treated according to the main recommendations of the Dutch evidence-based guidelines. There was a significant increase in the use of mesh-based repairs, especially the Lichtenstein technique. Furthermore, a significant increase of patients treated in day surgery and an increase of patients with bilateral hernia treated with endoscopic techniques were shown.
Due to the character of the study, it is not possible to assess the exact effect of the introduction of the guidelines versus the ongoing developments in the literature and research on IH surgery.
Abbreviations
- IH:
-
Inguinal hernia
References
Simons MP, de Lange D, Beets GL, van Geldere D, Heij HA, Go PM (2003) De richtlijn behandeling liesbreuk voor de nederlandse vereniging voor heelkunde. Ned Tijdschr Geneeskd 147(43):2111–2117
de Lange DH, Aufenacker TJ, Roest M, Simmermacher RK, Gouma DJ, Simons MP (2005) Inguinal hernia surgery in The Netherlands: a baseline study before the introduction of the Dutch Guidelines. Hernia 9(2):172–177
Koivusalo AI, Korpela R, Wirtavuori K, Piiparinen S, Rintala RJ, Pakarinen MP (2009) A single-blinded, randomized comparison of laparoscopic versus open hernia repair in children. Pediatrics 123(1):332–337
Saranga Bharathi R, Arora M, Baskaran V (2008) Minimal access surgery of pediatric inguinal hernias: a review. Surg Endosc 22(8):1751–1762
Bonnard A, Aigrain Y (2003) Inguinal hernias in children. Rev Prat 53(15):1667–1670
Jarrett PE (2001) Day care surgery. Eur J Anaesthesiol Suppl 23:32–35
Prabhu A, Chung F (2001) Anaesthetic strategies towards developments in day care surgery. Eur J Anaesthesiol Suppl 23:36–42
O’Dwyer PJ, Serpell MG, Millar K, Paterson C, Young D, Hair A et al (2003) Local or general anesthesia for open hernia repair: a randomized trial. Ann Surg 237(4):574–579
van Veen RN, Mahabier C, Dawson I, Hop WC, Kok NF, Lange JF et al (2008) Spinal or local anesthesia in Lichtenstein hernia repair: a randomized controlled trial. Ann Surg 247(3):428–433
Song D, Greilich NB, White PF, Watcha MF, Tongier WK (2000) Recovery profiles and costs of anesthesia for outpatient unilateral inguinal herniorrhaphy. Anesth Analg 91(4):876–881
Aufenacker TJ, Schmits SP, Gouma DJ, Simons MP (2009) Do guidelines influence results in inguinal hernia treatment? A descriptive study of 2,535 hernia repairs in one teaching hospital from 1994 to 2004. Hernia 13(1):35–39
Wilkiemeyer M, Pappas TN, Giobbie-Hurder A, Itani KM, Jonasson O, Neumayer LA (2005) Does resident post graduate year influence the outcomes of inguinal hernia repair? Ann Surg 241(6):879–882
Aufenacker TJ, de Lange DH, Burg MD, Kuiken BW, Hensen EF, Schoots IG et al (2005) Hernia surgery changes in the Amsterdam region 1994–2001: decrease in operations for recurrent hernia. Hernia 9(1):46–50
Aasvang E, Kehlet H (2005) Chronic postoperative pain: the case of inguinal herniorrhaphy. Br J Anaesth 95(1):69–76
Poobalan AS, Bruce J, Smith WC, King PM, Krukowski ZH, Chambers WA (2003) A review of chronic pain after inguinal herniorrhaphy. Clin J Pain 19(1):48–54
Acknowledgments
The authors would like to thank all of the participating hospitals.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
de Lange, D.H., Kreeft, M., van Ramshorst, G.H. et al. Inguinal hernia surgery in the Netherlands: are patients treated according to the guidelines?. Hernia 14, 143–148 (2010). https://doi.org/10.1007/s10029-009-0578-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10029-009-0578-y