
Abstract
Corynebacterium coyleae is part of the commensal microflora of the skin, urethra, mucous membranes, and genital tract. Isolates from patients with urinary tract infection (UTI) were reported, but the pathogenic potential of this species has not been defined yet. The aim of the study is to determine whether C. coyleae could be the etiological agent of UTI and to analyze its antibiotic susceptibility. Urine samples were cultured quantitatively according to accepted laboratory procedures. The identification of bacterial isolates was carried out using the Vitek MS (bioMérieux) and antibiotic susceptibility was tested using disc diffusion according to EUCAST guidelines. Between 1 January 2017 and 30 October 2018, a total of 39 C. coyleae strains were isolated. This represented 0.32% of all urine samples cultured in the laboratory during the collection period. The strains were isolated from samples obtained from 35 women and 3 men (age median for all—64 years). One female patient presented with C. coyleae in her urine twice at an interval of 21 months. In six cases of UTI, C. coyleae was isolated in monoculture. The isolates had the same resistance pattern. A total of 11 strains were obtained from cases with a clinical diagnosis of UTI. In 13 cases, the strain was cultured in a monoculture and in 28 cases with accompanying species. All strains were susceptible to vancomycin. However, resistance to ciprofloxacin was observed for 58.4% of the strains. Urine isolates of C. coyleae must be considered as contamination or normal flora in most cases (28/39, 72%). In the remaining cases, it can be considered as potential etiologic agents, mostly in women and especially in the 6 UTI cases where C. coyleae was found as the single culture-positive species. Several of these isolates demonstrate resistance to antibiotics commonly used in empiric treatment of urinary tract infections.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Corynebacterium coyleae was isolated for the first time in 1997 by Funke et al. [1] from the blood cultures of six patients with episodes of fever of unknown origin; one patient was infected with the human immunodeficiency virus (HIV), whereas the other five patients had a previous surgical intervention as the underlying condition. Furthermore, C. coyleae has been recovered from a definite sepsis case, probable case of sepsis and soft tissue infection, and possible post-transfusion bacteremia, neonatal bacteremia [2], pancreatic abscesses mimicking malignant neoplasm [3], burn injuries [4], pleural fluid specimens [1, 5], abscesses [6], and ulcers [7]. Still, there is ongoing controversy on its official pathogen status.
Resistance to beta-lactam antibiotics has not commonly been described in C. coyleae isolates. All isolates tested by Fernandez et al. [2] were susceptible to β-lactams, gentamicin, rifampin, tetracycline, vancomycin, linezolid, and resistant to clindamycin. Isolates from hospitalized patients reported by Barberis et al. [5] demonstrated a significantly higher resistance rate to antibiotics than those from outpatients. The aim of the current study is to determine whether C. coyleae could be an etiological agent of urinary tract infections and to analyze its antibiotic susceptibility.
Material and methods
The retrospective analysis included urine cultures performed in 2017 (January 1st–December 31st) and in 2018 (January 1st–October 31st). The samples were taken from in- and outpatients. The patients were aged 21–90 (arithmetic mean—62 years, midrange—55 years, median—64 years). Urine samples were cultured quantitatively according to the laboratory’s procedures. Middle stream urine (MSU) samples from women after transplantation and catheterized samples (CS) were cultured with 10 μl loop on CPS medium (bioMerieux, France); samples from men were cultured with 1 μl loop; and 100 μl samples from percutaneous nephrostomy and samples taken directly from renal pelvis were cultured. CPS and McConkey were applied for MSU, and CS were additionally cultured on blood agar and Schoedler’s medium (bioMerieux, France). The samples were incubated in 37 °C for 18–24 h. The identification was initially based on the colony and cell morphology, and then carried out in the Vitek MS (bioMérieux, France). VITEK MS is an adequate tool for the identification of C. coyleae. Although the database only contains 37 spectra obtained for 9 strains, it is 97.3% accurate and does not provide incorrect identifications (no discordances). Due to the small size of C. coyleae colonies, circa 5–10 colonies were applied on the MALDI sample slide. The susceptibility was tested with the disc diffusion method according to EUCAST guidelines and standardized laboratory procedures.
Results
A total number of 39 strains were isolated, representing 0.32% of all urine cultures during this period. Thirty-six strains were from women and three from men. In case of one female (73 years), C. coyleae was isolated twice at an interval of 21 months. In 2017, seven strains were cultured from patients with UTI symptoms; in three cases as a monoculture (104 cfu/ml); in 3 cases together with Enterococcus faecalis (103 cfu/ml twice, 105 cfu/ml once); and in one case with E. coli (104 cfu/ml); 17 strains were cultured from non-UTI patients; in 9 cases as monoculture (twice 105 cfu/ml, fivefold 104 cfu/ml, once 103 cfu/ml and once 102 cfu/ml). In 2018, 4 strains were cultured from patients with UTI symptoms cases; in 3 cases as monoculture (once 104 cfu/ml, twice 103 cfu/ml) and in one case with E. coli (102 cfu/ml); 11 strains from non-UTI patients; 5 strains presented as monocultures (thrice 104 cfu/ml and twice 103 cfu/ml) and in 6 cases another species was found in addition (twice E. coli 103 cfu/ml, twice E. faecalis 104 cfu/ml, once S. agalactiae 104 cfu/ml and once S. hemolyticus 103 cfu/ml) (Tables 1 and 2).
In one case, two urine samples were taken on the same day in different ways: middle stream urine (MSU) and material directly from the nephrostomy. Both C. coyleae and E. coli were isolated from MSU and only E. coli from the renal pelvis. In the other case, the following organisms were cultured: C. coyleae, Proteus mirabilis, Prevotella spp., Peptococcus asaccharolyticus, Lactobacillus spp., and S. epidermidis from the material obtained by nephrostomy from a patient with pyonephrosis. Three days after antibiotic therapy was started, only P. mirabilis was cultured from the urine obtained from nephrostomy (Table 3).
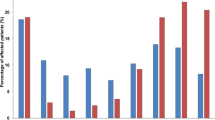
We analyzed the susceptibility of all strains to antibiotics applied in the treatment of UTI. Susceptibility rate to benzylpenicillin, ciprofloxacin, gentamycin, tetracycline, and vancomycin was 5.1%, 43.6%, 69.2%, 87.2%, 100%, respectively (Table 4).
Discussion
We present the biggest collection of clinical C. coyleae strains in current literature. The pathogenic role of this individual Corynebacterium species in human infections and their mechanisms of pathogenesis remain to be elucidated. There is a clear lack of distinction between colonization and infectious status, and there remains a need for additional clinical studies as well [6, 7]. The results of studies performed by other researchers show that Corynebacterium species, particularly those taxa found as part of the normal microflora, are prominent contaminants of clinical materials, although occasionally it is difficult to correctly decide if presence of such bacteria implies contamination or has clinical relevance. If Corynebacterium spp. are recovered from urine specimen as the only bacterial species encountered with a titer of > 104 cfu/ml or if it is the predominant organism recovered (> 105 cfu/ml), it is recommended to identify the isolate to the species level [6]. In Table 5, we present recovery of C. coyleae isolates from the genitourinary tract of women and men and their clinical significance as demonstrated by various authors. In addition, Fernández-Natal et al. [2] reported C. coyleae isolates from cases of sepsis, soft tissue infection, and post-transfusion bacteremia, which in vitro were susceptible to beta-lactams, gentamicin, rifampin, tetracycline, vancomycin, and linezolid, and resistant to clindamycin (Table 4). Resistance to erythromycin occurred in 83.3% of isolates, all of them presented phenotypic cMLS and harbored the gene ermX. Ortiz-Perez et al. [8] also detected ermX in 8/12 strains. The most concerning fact is that a large percentage of our strains is resistant to ciprofloxacin. We agree that the empirical use of quinolones should not be recommended, and clinically relevant Corynebacterium species always require antimicrobial susceptibility testing [5].
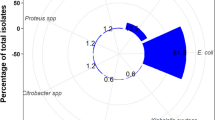
Contamination of a urine sample can contribute to under- or over-diagnosis of bacteriuria. In case that C. coyleae is a part of the normal microflora, it can potentially contribute to the implementation of unnecessary antimicrobial therapy [7]. In cases when the presence of C. coyleae in urine from a patient with UTI symptoms is accompanied by more commonly occurring pathogens (for example E. coli, Enterococcus spp., S. saprophyticus or Proteus spp.), it might be considered as contamination. However, if it comes to isolation of C. coyleae in quantities of 104 cfu/ml or 105 cfu/ml, the interpretation might be difficult, especially if the isolate is resistant to commonly prescribed antibiotics.
Based on the new findings presented here and the prior data published by others, C. coyleae is a rarely isolated species that should still be considered a pathogen that can be involved in complicated urinary tract infections, mostly in women. Isolation of C. coyleae may require confirmation by urinary tract punctuate to exclude contamination. Further studies on the role of C. coyleae in UTI are needed.
References
Funke G, Ramos CP, Collins MD (1997) Corynebacterium coyleae sp. nov., isolated from human clinical specimens. Int J Syst Bacteriol 47:92–96
Fernández-Natal MI, Sáez-Nieto JA, Fernández-Roblas R et al (2008) The isolation of Corynebacterium coyleae from clinical samples: clinical and microbiological data. Eur J Clin Microbiol Infect Dis 27(3):177–184
Taguchi M, Nishikawa S, Matsuoka H et al (2006) Pancreatic abscess caused by Corynebacterium coyleae mimicking malignant neoplasm. Pancreas 33:425–429
Duztas O, Erdem H, Pahsa A et al (2006) Epidemiology of corynebacterial urinary infections. IJID 10(3):264. https://doi.org/10.1016/j.ijid.2005.04.006
Barberis CM, Montalvo E, Imas S et al (2018) Total nephrectomy following Corynebacterium coyleae urinary tract infection. JMM Case Rep 5. https://doi.org/10.1099/jmmcr.0.005149
Bernard K An update on Corynebacterium species and their clinical significance. Clin Microbiol ASM Portal 2017 Hot Topic. https://clinmicro.asm.org/index.php/science-skills/training/82-about-asm/481-hot-topic-june-2017. Available 12 Feb 2019
Bernard K (2012) The genus Corynebacterium and other medically relevant. Coryneform-like bacteria. J Clin Microbiol 50(10):3152–3158
Ortiz-Perez A, Martın-de-Hijas NZ, Esteban J et al (2010) High frequency of macrolide resistance mechanisms in clinical isolates of Corynebacterium species. Microb Drug Resist 16(4). Inc). https://doi.org/10.1089/mdr.2010.0032
Verhelst R (2006) Characterization of the vaginal microflora. Dissertation submitted in fulfillment of the requirements for the degree of Doctor in Biomedical Sciences, Faculty of Medicine, University of Ghent
Turk S, Korrovits O, Punab M, Mandar R (2007) Coryneform bacteria in semen of chronic prostatitis patients. Int J Androl 30:123–128. https://doi.org/10.1111/j.1365-2605.2006.00722.x
Pearce MM, Hilt EE, Rosenfeld AB et al (2014) The female urinary microbiome: a comparison of women with and without urgency urinary incontinence. mBio 5(4):e01283–e01214. https://doi.org/10.1128/mBio.01283-14
Yang S (2015) The role of probiotic Lactobacillus in immune regulation and modulation of the vaginal microbiota during pregnancy. A thesis submitted in conformity with the requirements for the degree of Doctor of Philosophy Department of Physiology University of Toronto © Copyright by Siwen Yang
Brubaker L, Wolfe AJ (2016) The urinary microbiota: a paradigm shift for bladder disorders? Curr Opin Obstet Gynecol 28(5):407–412. https://doi.org/10.1097/GCO.0000000000000298
Schwaderer AL, Wolfe AJ (2017) The association between bacteria and urinary stones. Ann Transl Med 5(2):32. https://doi.org/10.21037/atm.2016.11.73
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Sokol-Leszczynska, B., Leszczynski, P., Lachowicz, D. et al. Corynebacterium coyleae as potential urinary tract pathogen. Eur J Clin Microbiol Infect Dis 38, 1339–1342 (2019). https://doi.org/10.1007/s10096-019-03565-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10096-019-03565-4