
Abstract
Ambulatory care sensitive hospitalizations are widely considered as important measures of access to as well as quality and performance of primary care. In our study, we investigate the impact of spending, process quality and continuity of care in the ambulatory care sector on ambulatory care sensitive hospitalizations in patients with type 2 diabetes. We used observational data from Germany’s major association of insurance companies from 2012 to 2014 with 55,924 patients, as well as data from additional sources. We conducted negative binomial regression analyses with random effects at the district level. To control for potential endogeneity of spending and physician density in the ambulatory care sector, we used an instrumental variable approach. We controlled for a wide range of covariates, such as age, sex, and comorbidities. The results of our analysis suggest that spending in the ambulatory care sector has weak negative effects on ambulatory care sensitive hospitalizations. We also found that continuity of care was negatively associated with hospital admissions. Patients with type 2 diabetes are at increased risk of hospitalization resulting from ambulatory care sensitive conditions. Our study provides some evidence that increased spending and improved continuity of care while controlling for process quality in the ambulatory care sector may be effective ways to reduce the rate of potentially avoidable hospitalizations among patients with type 2 diabetes.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
A large proportion of today’s hospital admissions are thought to be avoidable through effective management and timely treatment in the ambulatory care sector. So-called ambulatory care sensitive conditions (ACSC) have become a measure to assess access, quality and performance of care, as an indicator of quality in ambulatory care [1, 2] and are sometimes used as a rough estimate of the proportion of potentially avoidable hospitalizations in health care systems. These hospital admissions are not only undesirable for patients but also disruptive and costly for payers and purchasers of care, such as statutory or private health insurers, or clinical commissioning groups.
Ways to reduce these potentially avoidable hospitalizations include controlling acute episodes of an illness, managing a chronic condition effectively, or preventing a disease in the first place [3]. Most of these approaches involve an increase in the use of ambulatory care resources. In general, it has been assumed that increasing the volume of health services provided, for example through more ambulatory care spending, will lead to improvements in the health status of a population [4]. This raises the question of whether an increase in ambulatory care spending can reduce hospitalizations for ACSC.
Considering the budget constraints in most health care systems, several empirical studies have explored the relationship between health care resourcing and patient outcomes with the aim of estimating the extent to which an increase in the volume of health care services yields benefits for patients [5].
A number of studies have examined the relationship between the use of ambulatory care resource and hospitalizations while specifically focusing on ACSC. Many of these have reported a negative relationship between physician density and ambulatory care sensitive hospitalizations (ACSH) [6,7,8,9,10]. A systematic review of studies examining the effects of primary health care resourcing on diabetes-related hospitalizations concluded that access to ambulatory care was negatively associated with hospitalizations, whereas evidence of an association between the use of ambulatory care and hospitalizations was inconclusive [11]. The authors recommended that future studies adjust adequately for patients’ health status and disease severity. Sundmacher and Kopetsch [12], in turn, used aggregate-level data to investigate the impact of the volume of office-based care on hospitalizations for ACSC in Germany. They found that increasing the volume of medical services reduced the rate of hospitalizations, albeit with diminishing marginal returns.
This study focuses on patients with type 2 diabetes. The chronic disease is an ACSC and one of the top ten causes of death worldwide. Its prevalence has quadrupled within the past 36 years and is likely to increase further [13]. Diabetes is also a major cause of morbidity and is associated with more and longer hospital stays and an increased number of surgical complications [14,15,16]. In addition, diabetes complicates the diagnosis and treatment of other medical disorders [17]. Ambulatory care plays a key role in the management of patients with diabetes [18]. This includes monitoring the disease, taking preventive measures, administering medical treatment, and giving lifestyle advice [19]. Good continuity of care and the adherence to clinical practice guidelines are well-documented to be associated with fewer hospitalizations among patients with diabetes [20, 21]. Coordination and continuity of care have the potential to reduce the duplication of services and overall health care costs, and to improve health outcomes [22, 23]. The results of earlier studies suggest that improved continuity of care can result in better control of chronic diseases, higher patient satisfaction, and fewer emergency department visits and hospitalizations [24,25,26,27]. Especially in systems of statutory health insurance, such as that in Germany, where no gatekeeping is in place, care coordination becomes even more relevant [28]. Measures to improve the quality of care may be complicated or hampered by fragmentation of the ambulatory sector. Moreover, incentives to contain costs can be located within individual physicians.
Specifically in the German health care system, ambulatory care is characterized by professional autonomy and a large proportion of office-based physicians in solo practices [29]. In the statutory health system, no gatekeeping is in place, and patients can seek ambulatory care at any GP or specialist office-based physician at any point in time. Coordination of care for chronically ill, multimorbid patients is a major challenge in the health care system [30]. Problems in coordination of care can lead to increased ambulatory care costs and negative consequences for patients, such as redundant, diverging procedures and deterioration in health states [31, 32].
Earlier studies have investigated the effects of ambulatory care resourcing on ambulatory care sensitive hospitalizations using aggregated data or have analyzed the effects on health outcomes, of processes of care for specific diseases. Our study contributes to the literature by investigating the effect of ambulatory care spending on hospitalizations among patients with type 2 diabetes using measures of care continuity and process indicators at the level of individual patients. In doing so, we adjust for a number of known risk factors for hospitalizations among this patient group.
Methods
Study setting and data sources
This is an observational study based on insurance claims data from 2012 through 2014 provided by the scientific research institute of the regional statutory health insurers (AOKen) in Germany, which cover approximately 36% of the population insured within the country’s system of statutory health insurance [33]. The data used contain information about inpatient and outpatient visits and spending, prescriptions, and diagnoses among a sample of patients older than 18 years and with at least two confirmed diabetes diagnoses in two different quarters. This sample was drawn from a larger sample of 3.08 million patients with a diabetes diagnosis. Our sample was smaller, because data protection regulations did not allow the statutory insurers to provide us with the full data set. In addition, to ensure a complete history of patients’ health care, we excluded patients who had died during or were not insured throughout the entire period 2012–2014.
We excluded patients who were living with HIV, had a diagnosis of metastatic cancer, were on dialysis, were dependent on opioids, or were receiving intensive nursing or palliative care because of the specifics of these treatments/diseases and the high likelihood of hospitalization independent of the ambulatory care treatment as well as different treatment goals. In addition, patients with diseases whose treatment is considered to be very expensive were excluded from further analyses (i.e., high-risk patients). In identifying high-risk patients, we concentrated on the diagnoses of the high-risk patient pool in former versions of the morbidity-based risk adjustment scheme in Germany [34, 35]. We report results including the patients with HIV, metastatic cancer, dependent on opioids, and high-risk patients in sensitivity analyses later in the appendix. We assumed that a hospitalization would be most likely for these patients and that presumably timely and effective ambulatory care was not able to prevent these hospital cases.
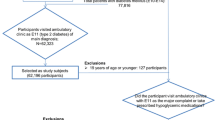
We expected that treatments received over the course of 2 years would impact upon health outcomes in the following year. Therefore, we defined an observation period (2012–2013) and a period for potential hospitalizations (2014). To compute valid continuity scores and due to plausibility considerations, we excluded patients who had made less than three ambulatory care visits to GPs during the observation period of 2 years. Owing to plausibility considerations, we also excluded patients for whom the statutory health insurers spent less than 25 Euro on ambulatory care per year during the observation period, because three visits to ambulatory care would already exceed that value. Figure 1 illustrates the process of selecting data for the analysis.

Data selection for the analysis
In addition, we used district-level data from the Federal Institute for Research on Building, Urban Affairs and Spatial Development [36] (physician density, unemployment rate and hospital density) and the Science Council [37] (medical students in a region) in our analyses to inform on structural variables, such as the physician density.
Dependent variable
Our dependent variable was the number of hospitalizations due to ACSC. Patients with type 2 diabetes are at high risk of developing complications and comorbidities as the disease progresses [38], and several studies have shown that type 2 diabetes patients suffer from both a greatly increased all-cause hospitalization rate and diabetes-related hospitalization rate [39,40,41]. Complications and hospitalizations of individuals with diabetes can potentially be avoided and delayed through ambulatory care [38], which includes the prevention of diseases, controlling acute episodes of illnesses, and managing chronic conditions effectively.
To account for the fact that patients with type 2 diabetes experience a higher risk of vascular complications and morbidity related to increased need for ambulatory care [42], we used a list of hospitalizations following ACSC as dependent variable in our analysis. The range of hospitalizations is thought to capture all potentially avoidable hospitalizations that might result from a deterioration in health caused by a health state that could potentially have been avoided with ambulatory care. This list comprised 22 conditions specific to the German health care sector (see Table 2), resulting from potentially inadequate ambulatory care treatment [44].
We defined a hospitalization as a hospital admission that lasted at least 1 night. A hospitalization was defined as ambulatory care sensitive if the main diagnosis for the hospital admission in 2014 was coded as one of the included diagnosis groups (see Table 1). In addition, diabetes had to be at least a secondary diagnosis for the hospital admission so that we could be certain that patients were also treated because of diabetes.
Ambulatory care spending, continuity of care and process indicators
Our primary explanatory variable was total ambulatory care spending per patient. We decided to include all ambulatory spending for a patient for two reasons: First, we assumed that diabetes would affect any treatment in ambulatory care. Therefore, the inclusion of all ambulatory care spending was a way to ensure a patient-oriented approach to our analysis. Second, ambulatory care spending is billed to statutory health insurers primarily in the form of quarterly capitation-type lump sums in Germany [28, 45], meaning that the incremental spending on the treatment of one disease cannot be measured without making crude assumptions. Spending was defined as cost to the statutory health insurer, which can be seen as an indicator for sector-specific resource use for the ambulatory care treatment of diabetes patients from the payer perspective. Patient co-payments, prescriptions, and private payments are, therefore, not included in our analyses. Out-of-pocket spending, however, is comparably low in Germany [46]. We hypothesized that, in case the care received was effective, hospitalizations would decrease as ambulatory care spending increases.
We aimed to depict continuity of care in our analyses, because measures to reduce ACSH at the systems level include interventions to improve the continuity of care [21, 47]. We assumed based on prior empirical literature that continuous care would decrease the risk of a hospitalization [25,26,27].
In our study, we operationalized continuity of care using the continuity of care index of Bice and Boxerman 1977. It measures the dispersion of visits and quantifies the percentage of visits to distinct providers. The index is commonly used [49, 50] and reflects both the total number of visits and the number of health care providers the patients sees [48]. It was used, because we hypnotized that continuity of care with the relevant providers would have positive effects on the treatment of patients in a system without gatekeeping and a lack of coordination. The index is calculated by dividing the sum of the squared number of visits per provider minus the total number of visits to all providers during the observation period by the number of all visits minus the number of all visits minus one.
Continuity of Care Index (COCI) =\(\frac{{\mathop \sum \nolimits_{j = 1}^{k} n^{2} - N}}{{N\left( {N - 1} \right)}}\).
(k = number of providers, n = number of visits to provider; N = total number of visits to all providers).
The index ranges from 0 to 1 and increases when more visits are made to a smaller number of providers. In this study, we considered only those visits in 2012/2013 that were made to diabetes-relevant physicians within primary care (i.e., GPs and internal medicine physicians/internists). Alternative measures of continuity of care (COCI with GPs only, COCI with a wider set of physicians and the modified continuity index) are applied in the supplementary material. In addition, we controlled for the number of visits to these physicians based on the number of days for which physicians billed a service.
We also operationalized indicators reflecting processes of care within the observation period. Individuals with diabetes require systematic and interdisciplinary regular care [18]. We selected a composite process indicator for ambulatory care treatment based on recommendations from clinical practice guidelines, measurable using the routine data, and relevant to all diabetes patients. We indicated whether a patient received a yearly blood glucose test, a yearly microalbuminuria test, and at least one funduscopy examination within the observation period. These indicators are suggested for quality measurement in health care systems as they are reliably measureable and highly relevant for health outcomes of patients [51]. The gold standard for measuring control of blood sugar in diabetes is measuring glycated hemoglobin (hbA1c) [13]. A yearly hbA1c test and a test for microalbuminuria are recommended in medical guidelines and is seen as effective care for patients with diabetes [52,53,54]. The presence of microalbuminuria has been shown to predict progression to diabetic nephropathy, which is associated with fairly high mortality rates [54]. Earlier empirical studies that have examined the effect of processes of care on hospitalizations have, in particular, identified a negative association between these and regular hbA1c and microalbumin tests [18]. Furthermore, at least biennial eye screening is recommended for individuals with type 2 diabetes [53]. It allows for early detection and timely treatment of visual impairments [55]. To address aspects of disease prevention, we indicated whether patients received an influenza vaccination in each year of the observation period. Influenza vaccinations have been shown to reduce the risk of hospitalizations in type 2 diabetes patients by about 80% [56]. A yearly influenza vaccination in type 2 diabetes patients is recommended by the German permanent vaccination commission [57]. We hypothesized that patients who were treated according to medical guidelines and recommendations in the two observation years would have fewer hospitalizations. The composite measure was dichotomized and indicated when patients received all four recommended processes of ambulatory care. In sum, these process indicators represent a proxy for interdisciplinary, preventive, and comprehensive ambulatory care treatment following medical guidelines and recommendations.
Control variables
Our study was informed by earlier research that identified adjustment for a number of known risk factors for hospitalizations among patients with type 2 diabetes [18, 58, 59].
We controlled for the age and gender of patients, as well as for disease severity and disease-specific risk factors. We determined whether patients were receiving insulin with at least one prescription each year during the observation period to control for disease severity and calculated a diabetes severity index based on an adapted Diabetes Complication Severity Index (DSI) [42, 58]. The DSI aims to systematically quantify diabetes complications and includes seven complications of diabetes [retinopathy, nephropathy, neuropathy, cerebrovascular, cardiovascular, peripheral vascular disease (PVD), metabolic disease]. Furthermore, we added risk factors according to the United Kingdom Prospective Diabetes Study and the US Centers for Disease Control and Prevention/RTI diabetes model to our regression analysis [58, 59]. These were operationalized using dummy variables for the relevant comorbidities for which a diagnosis was coded in the years 2012/2013. For a complication to be included in the DSI and a risk factor to be considered at least one confirmed outpatient or inpatient ICD diagnosis, OPS code, or reimbursement code to be documented in the observation period. Furthermore, we indicated via the M3 multimorbidity index whether patients had multiple diseases [60]. In addition, we used the number of prescribed medications (operationalized as ATC agents) to control for the overall morbidity of patients. In case hospitalizations occurred in 2012/2013, we also included a variable to control for the health status of patients following prior hospitalizations.
Causes of ACSH can be related to the health care system, to physicians, to patients’ personal or social circumstances, or some combination of these [61]. We, therefore, also controlled for the unemployment rate (2012), the number of hospital beds (2012), and the density of internists and GPs in the district in which the patient lived (2015). Germany divides into 401 administrative districts incorporating different levels of population density and structure. In line with previous results, we hypothesized that unemployment would increase the risk of hospitalization [62]. Informed by prior empirical evidence, we assumed that physician density (i.e., internists and GPs in the case of diabetes) in a region would be negatively associated with ACSH [6, 11]. Furthermore, based on prior research we expected hospital bed availability to be positively associated with ACSH [63].
Analytical approach
We explored how spending, continuity and process quality in the ambulatory care sector affects ACSH using a negative binomial model with random effects at the district level. As the dependent variable “hospitalizations due to ACSC” showed a right-skewed distribution with a variance exceeding the mean value, we performed the Vuong closeness test to rule out the possibility that a zero-inflated negative binomial model would have been the better choice. Most variables were available at the individual level. However, the unemployment rate and the variables related to health system access (i.e., internist and GP density, hospital density) were aggregated at the level of districts, giving the model two levels of analysis (i.e., individual and district). We controlled for this by means of random effects.
We undertook multiple regression analyses to assess the association between ambulatory care characteristics and health outcomes in an iterative manner. We first analyzed the effect of ambulatory care spending on health outcomes. To address the effects of coordinated care, we also added a continuity of care index and the number of visits to general practitioners and internists to our second regression analysis. Finally, to capture the additional effect of effective care on hospitalizations, we added the variable indicating whether the recommended processes had been conducted to our third regression.
Instrumental variable approach
An unbiased estimation of the coefficients of the regression equation requires that the error term does not correlate with the explanatory variables. However, we do not consider this assumption to be valid in our case. The level of ambulatory care spending and the number of hospitalizations for ACSC may be influenced by unobserved third variables (omitted variables). This could be the case with unrecorded morbidity, which was not measurable in our data and may have influenced the level of ambulatory spending and hospitalizations. Also, the distribution of physicians across Germany was not strictly regulated until the early 1990s [28]. Based on the different regional distribution of morbidity, incentives may have existed for physicians to move to areas with high or low morbidity. In this case, the causality between physician density and hospitalizations may be reversed in the regression (i.e., endogeneity).
An instrumental variable approach was used to control for potential endogeneity of the two variables ambulatory care spending and physician supply with ACSH. The main challenge of the instrumental variable approach was to find an instrument which (a) we could use to control for potential endogeneity of ambulatory care spending and physician density with ACSH but (b) after controlling for exogenous covariates, clearly correlated with the explanatory variable but not with the error term [64]. We chose the approximated average ambulatory care spending per person in a district as this instrument for the individual ambulatory spending. Associations of statutory health insurance physicians negotiate a regional budget for the ambulatory sector with the statutory health insurers. Once physicians exceed the regional budget, they continue to be reimbursed for their services but at progressively lower prices. We thus expected regional average ambulatory care spending to correlate with ambulatory care spending per patient and not with the individual hospitalizations and, therefore, used the former as an instrument for the latter. With regard to physician density in a region, the assumption seems to be met for the number of medical students in a region (2013). We assumed that physicians cluster in proximity to the university at which they are trained [65] and used the number of medical students in a region as an instrument for the physician density in a region.
We undertook a Shorrocks–Shapley decomposition to investigate the relative contribution of groups of regressors to the pseudo R2 [66]. Here, we aimed to show the total impact of the ambulatory care characteristics under investigation, compared with patients’ morbidity and health care provision variables.
We conducted all analyses using Stata 14.
Results
Descriptive statistics
A total of 55,924 patients with type 2 diabetes were included in our analysis (summary statistics are provided in Table 1). The mean age of the patients was 66 years and 50.95% were men. Statutory health insurers spent an average of €820 on ambulatory care per patient each year. In total, 4.80% of the patients received all recommended processes during the observation period. Highest rates are achieved by yearly hbA1c tests (average 87%). Lowest rates are observed with the yearly microalbumin test (average 21%). Patients had a mean continuity of care index of 0.71 and made a mean number of 15 visits to ambulatory care physicians per year.
Overall, 9.82% of the included patients were hospitalized at least once due to an ACSC in 2014. Of these hospitalizations, 14.44% were coded with diabetes as the main diagnosis. Table 2 shows the distribution of hospital cases among the 22 ACSC per 1000 type 2 diabetes patients. Among these conditions, ischemic heart disease was the ACSC with most ACSH followed by diabetes and heart failure. The hospitalization rates are 2.1 times higher than in the general German population with highest differences in ischemic heart diseases, diabetes and heart failure.
Regression results
The results of the negative binomial regressions are shown in Table 3. Results of the regressions with instrumental variables are preferred over regular regressions. In the first stage, both instruments exceed the critical value of F > 10 established by Staiger and Stock [67] and are thus regarded as valid. The Hausman specification tests also indicate potential endogeneity in all regressions. The following interpretations refer to the results of the instrumental variable regressions.
The first two columns show the results for the effect of ambulatory care spending only. The columns in the middle give the results of the regression models that incorporated the continuity of care index and the number of physician visits. The last two columns show the results of the models that included the measure of effective ambulatory care. All coefficients are reported as incidence rate ratios (IRR) and indicate the factor change in ACSH when an explanatory factor increases by 1 unit, holding all other variables constant. An incidence ratio of 1, for example, suggests that the explanatory variable is a neutral factor in the distribution of hospitalizations between patients. An incidence ratio of 1.5 suggests that an increase in the explanatory variable of 1 unit is associated with a 50% increase in the number of ACSH for the patient.
In all three models, we found a weak negative association between ambulatory care spending and health outcomes, indicating that an increase in ambulatory care spending is associated with fewer ACSH even when controlling for continuous and effective care.
A negative association also existed for continuity of care and hospitalizations. We found that an increase in the continuity of care index from 0 to 1 was associated with a 17% reduction in the number of hospitalizations. The negative association also holds for the alternative measures of continuity of care with GPs only and the wider set of physicians involved in the treatment of diabetes patients and the modified continuity index (see supplementary material). A higher number of physician visits was associated with a higher number of hospitalizations. The variable for effective care was associated with an 23% increase in the number of hospitalizations.
Moreover, when looking at our control variables for morbidity and prior health care use, there was a positive association with the number of hospitalizations resulting from ACSC. Patients with prior hospitalizations are expected to experience 76–77% more hospitalizations. In addition, as expected, hypertension, depression, obesity, and sleeping disorders were positively associated with hospitalizations. A higher number of ATC agents was associated with a higher number of hospitalizations. Women had 5% fewer hospitalizations than men.
Health sector variables showed the expected associations with the number of hospitalizations. Hospital bed density and the number of hospitalizations were positively associated. Physician density was associated with fewer hospitalizations.
The results of the Shapley decomposition analysis for the three groups of variables indicate the following: ambulatory care characteristics (including spending, continuity of care, and the variable for effective care) account for 9.8% of the pseudo R2, morbidity of patients (including gender and age groups) for about 85.5%, and system-related factors of health provision for 4.7%.
Discussion
Many unplanned hospital admissions are undesirable for patients and disruptive and costly for health care systems [24]. Those that are caused by ACSC account for a particularly large amount of health spending [68]. A substantial proportion of these hospitalizations can probably be avoided, however, if patients have good access to effective ambulatory care [24,25,26]. We, therefore, investigated the effect of ambulatory care spending on avoidable hospitalizations in a sample of 55,924 patients with type 2 diabetes.
The risk of hospitalization following ACSC in this group is very high. Compared with the general public in Germany [43], patients in our sample had rates of hospitalization that were four times higher for ischemic heart diseases, three times higher for heart failure, and eight times higher for diabetes. Overall, hospitalization rates resulting from ACSC were 2.1 times higher in our sample than in the general population in Germany, which is similar to differences in rates seen in comparable settings [44].
We find evidence that ambulatory care plays an important role in the management of patients with diabetes, including the prevention of avoidable hospitalizations. In our analysis, which was based on individual-level data from type 2 diabetes patients, we found high variation in costs among patients and a weak negative association between ambulatory care spending and potentially avoidable hospitalizations. After controlling for coordinated and effective care, the relationship between ambulatory care resourcing and hospitalizations remained unchanged. Ambulatory care spending was negatively associated with the number of hospitalizations. While previous literature focused on studying the relationship of resources, such as the physician density, physician visits or operating hours and ACSH [11], our study adds to the previous literature with important information on the effect of health care spending on ACSH.
We find in line with the results of earlier studies that continuity of care has a positive effect on ACSH [26, 69]. Having regular contact with a physician may decrease the likelihood of hospitalization [70]. Continuity of care may facilitate an effective and trusting relationship between patients and physicians and lead to patients understanding their disease better and, therefore, also to greater adherence to treatment or preventive measures [24]. The fragmentation between the ambulatory care and hospital sectors in Germany is a well-known barrier to well-coordinated and continuous care [71].
Furthermore, we did not find that effective care was associated with a lower number of hospitalizations. The coefficient was not significant. Also in earlier studies, the association of diabetes processes of care and hospitalizations in patients with type 2 diabetes was unclear [18]. In absolute terms, we observed that only ~ 5% of our sample received the recommended care indicating regular blood glucose, eye, and microalbumin examination as well as an influenza vaccination. Initiatives to promote adherence to these, where appropriate, may help to reduce hospitalizations and also have other positive effects [19].
In our decomposition analysis, approximately one tenth of the pseudo R2 could be explained by variables related to access to ambulatory care. An even greater part could be accounted for by variables related to morbidity. In the regression analysis, we found that especially the variables for the number of medications and prior hospitalizations had an impact on the number of hospitalizations. Patients with a higher number of medications resulting from a larger number of comorbidities and prior hospitalizations are those who are most sensitive to discontinuities in care [44, 72]. Policy makers designing initiatives to promote effective and continuous care may want to target these risk groups if a broader population-based approach is not desired or possible.
Our study has several important limitations. First, our sample was drawn from routine data from one major group of statutory health insurers in Germany, which insures approximately one third of all individuals with statutory health insurance in Germany. Our results may not be generalizable to the overall population [73]. Second, our data did not allow us to capture fully the health status of patients. We strove to include a homogeneous patient population by excluding certain conditions, and by controlling for disease severity, risk factors, and comorbidity. However, we cannot rule out that patients’ disease progression was not adequately depicted. Third, we could not include patient preferences or socioeconomic variables at a patient level in our analyses even though these have been shown to be highly relevant to the utilization of health care [61, 62]. We did, however, include socioeconomic status at a regional level based on the assumption that this would approximate patient-level differences.
Furthermore, ambulatory care spending does not always correlate with the number of visits to physicians, because ambulatory care spending is driven mainly by quarterly capitation-type lump sum payments and only specific services are billed additionally. The number of visits to physicians and continuity of care are thus subject to these limitations in routine data.
Last, we attempted to describe quality of care using a composite process indicator. No indicator, however, perfectly describes the quality of care, and individual medical conditions and patient preferences may justify deviations from the recommendations made in clinical practice guidelines [74]. We cannot rule out that our process indicator captured decisions driven by patient preferences and behavior. We aimed to include indicators with low medical uncertainty to depict the effects of effective care rather than the results of preferences for care. However, there remains some uncertainty on the effectiveness of procedures for individual patients. Finally, the results of effective ambulatory care may require more than 2 years to become apparent.
In summary, we provide weak evidence that increased spending and improved continuity of care in the ambulatory care sector may reduce hospitalizations and should be considered when promoting ambulatory care initiatives for people living with chronic illnesses.
Data availability
Data provided by the insurance fund cannot be provided due to data protection regulations.
Code availability
Upon request.
References
Weissman, J.S., Gatsonis, C., Epstein, A.M.: Rates of avoidable hospitalization by insurance status in Massachusetts and Maryland. JAMA 268, 2388–2394 (1992)
Purdy, S., Griffin, T., Salisbury, C., Sharp, D.: Ambulatory care sensitive conditions: terminology and disease coding need to be more specific to aid policy makers and clinicians. Public Health 123, 169–173 (2009). https://doi.org/10.1016/j.puhe.2008.11.001
Billings, J., Zeitel, L., Lukomnik, J., Carey, T.S., Blank, A.E., Newman, L.: Impact of socioeconomic status on hospital use in New York City. Health Aff 12, 162–173 (1993). https://doi.org/10.1377/hlthaff.12.1.162
Kim, K., Moody, P.M.: More resources better health? A cross-national perspective. Soc Sci Med 34, 837–842 (1992). https://doi.org/10.1016/0277-9536(92)90253-M
Gallet, C.A., Doucouliagos, H.: The impact of healthcare spending on health outcomes: a meta-regression analysis. Soc Sci Med 179, 9–17 (2017). https://doi.org/10.1016/j.socscimed.2017.02.024
Ansari, Z., Laditka, J.N., Laditka, S.B.: Access to health care and hospitalization for ambulatory care sensitive conditions. Med Care Res Rev 63, 719–741 (2006). https://doi.org/10.1177/1077558706293637
Laditka, J.N., Laditka, S.B., Probst, J.C.: More may be better: evidence of a negative relationship between physician supply and hospitalization for ambulatory care sensitive conditions. Health Serv Res 40, 1148–1166 (2005). https://doi.org/10.1111/j.1475-6773.2005.00403.x
Berlin, C., Busato, A., Rosemann, T., Djalali, S., Maessen, M.: Avoidable hospitalizations in Switzerland: a small area analysis on regional variation, density of physicians, hospital supply and rurality. BMC Health Serv Res 14, 289–310 (2014). https://doi.org/10.1186/1472-6963-14-289
Daly, M.R., Mellor, J.M., Millones, M.: Do avoidable hospitalization rates among older adults differ by geographic access to primary care physicians? Health Serv Res (2017). https://doi.org/10.1111/1475-6773.12736
Rosano, A., Loha, C.A., Falvo, R., van der Zee, J., Ricciardi, W., Guasticchi, G., et al.: The relationship between avoidable hospitalization and accessibility to primary care: a systematic review. Eur J Public Health 23, 356–360 (2013). https://doi.org/10.1093/eurpub/cks053
Gibson, O.R., Segal, L., McDermott, R.A.: A systematic review of evidence on the association between hospitalisation for chronic disease related ambulatory care sensitive conditions and primary health care resourcing. BMC Health Serv Res 13, 336 (2013). https://doi.org/10.1186/1472-6963-13-336
Sundmacher, L., Kopetsch, T.: The impact of office-based care on hospitalizations for ambulatory care sensitive conditions. Eur J Heal Econ 16, 365–375 (2014). https://doi.org/10.1007/s10198-014-0578-4
World Health Organization (WHO): Global Report on Diabetes (2016). https://www.who.int/diabetes/global-report/en/. Accessed 15 Jan 2020
Caminal, J., Starfield, B., Sánchez, E., Casanova, C., Morales, M.: The role of primary care in preventing ambulatory care sensitive conditions. Eur J Public Health 14, 246–251 (2004). https://doi.org/10.1093/eurpub/14.3.246
Rasekaba, T.M., Lim, W.K., Hutchinson, A.F.: Effect of a chronic disease management service for patients with diabetes on hospitalisation and acute care costs. Aust Health Rev 36, 205 (2012). https://doi.org/10.1071/AH10992
Wang, J., Imai, K., Engelgau, M.M., Geiss, L.S., Wen, C., Zhang, P.: Secular trends in diabetes-related preventable hospitalizations in the United States, 1998–2006. Diabetes Care 32, 1213–1217 (2009). https://doi.org/10.2337/dc08-2211
Redelmeier, D.A., Tan, S.H., Booth, G.L.: The treatment of unrelated disorders in patients with chronic medical diseases. N Engl J Med 338, 1516–1520 (1998). https://doi.org/10.1056/NEJM199805213382106
Comino, E.J., Islam, M.F., Tran, D.T., Jorm, L., Flack, J., Jalaludin, B., et al.: Association of processes of primary care and hospitalisation for people with diabetes: a record linkage study. Diabetes Res Clin Pract 108, 296–305 (2015). https://doi.org/10.1016/j.diabres.2015.02.003
Dusheiko, M., Gravelle, H., Martin, S., Rice, N., Smith, P.C.: Does better disease management in primary care reduce hospital costs? Evidence from English primary care. J Health Econ 30, 919–932 (2011). https://doi.org/10.1016/j.jhealeco.2011.08.001
Campbell, D.J., Lacny, S.L., Weaver, R.G., Manns, B.J., Tonelli, M., Barnabe, C., et al.: Age modification of diabetes-related hospitalization among First Nations adults in Alberta, Canada. Diabetol Metab Syndr 6, 108 (2014). https://doi.org/10.1186/1758-5996-6-108
Christakis, D.A., Mell, L., Koepsell, T.D., Zimmerman, F.J., Connell, F.A.: Association of lower continuity of care with greater risk of emergency department use and hospitalization in children. Pediatrics 107, 524–529 (2001)
Shin, D.W., Cho, J., Yang, H.K., Park, J.H., Lee, H., Kim, H., et al.: Impact of continuity of care on mortality and health care costs: a nationwide cohort study in Korea. Ann Fam Med 12, 534–541 (2014). https://doi.org/10.1370/afm.1685
Weinstein, M.C., Skinner, J.A.: Comparative effectiveness and health care spending—implications for reform. N Engl J Med 362, 460–465 (2010). https://doi.org/10.1056/NEJMsb0911104
Barker, I., Steventon, A., Deeny, S.R.: Association between continuity of care in general practice and hospital admissions for ambulatory care sensitive conditions: cross sectional study of routinely collected, person level data. BMJ 356, j84 (2017). https://doi.org/10.1136/BMJ.J84
Busby, J., Purdy, S., Hollingworth, W.: How do population, general practice and hospital factors influence ambulatory care sensitive admissions: a cross sectional study. BMC Fam Pract 18, 67 (2017). https://doi.org/10.1186/s12875-017-0638-9
Hong, J.-S., Kang, H.-C.: Continuity of ambulatory care and health outcomes in adult patients with type 2 diabetes in Korea. Health Policy (New York) 109, 158–165 (2013)
Tsai, H.-Y., Chou, Y.-J., Pu, C.: Continuity of care trajectories and emergency room use among patients with diabetes. Int J Public Health 60, 505–513 (2015). https://doi.org/10.1007/s00038-015-0671-1
Busse, R., Blümel, M.: Germany: health system review. Health Syst Transit 16, 1–296 (2014)
World Health Organization (WHO): Ambulatory care sensitive conditions in Germany. Copenhagen WHO Reg Off Eur (2015). http://www.euro.who.int/__data/assets/pdf_file/0004/295573/ASCS-Germany-2015-rev1.pdf?ua=1. Accessed 15 Jan 2020
Sachverständigenrat zur Begutachtung der Entwicklung im Gesundheitswesen (SVR). Bedarfsgerechte Steuerung der Gesundheitsversorgung (2018). https://doi.org/10.5771/1611-5821-2018-6-37
Schneider, A., Donnachie, E., Tauscher, M., Gerlach, R., Maier, W., Mielck, A., et al.: Costs of coordinated versus uncoordinated care in Germany: results of a routine data analysis in Bavaria. BMJ Open 6, e011621 (2016). https://doi.org/10.1136/BMJOPEN-2016-011621
Hofmarcher, M.M., Oxley, H., Rusticelli, E.: Improved health system performance through better care coordination. OECD Health Working Papers No. 30, OECD Publishing. https://doi.org/10.1787/246446201766
Bundesministerium für Gesundheit (BMG). Gesetzliche Krankenversicherung-Mitglieder, mitversicherte Angehörige und Krankenstand, Jahresdurchschnitt 2018 (2019). https://www.bundesgesundheitsministerium.de/fileadmin/Dateien/3_Downloads/Statistiken/GKV/Mitglieder_Versicherte/KM1_JD_2018.pdf. Accessed 15 Jan 2020
Bundesversicherungsamt (BVA). Festlegungen zum Riskikostrukturausgleich (2019). https://www.bundesversicherungsamt.de/risikostrukturausgleich/festlegungen.html. Accessed 15 Jan 2020
Drösler, S., Garbe, E., Hasford, J., Schubert, I., Ulrich, V., van den Ven, W., et al.: Sondergutachten zu den Wirkungen des morbiditätsorientierten Risikostrukturausgleiches-Antwort der Bundesregierung, 1 (2017). https://www.bundesgesundheitsministerium.de/fileadmin/Dateien/5_Publikationen/Gesundheit/Berichte/Sondergutachten_Wirkung_RSA_2017.pdf. Accessed 15 Jan 2020
Federal Institute for Research on Building UA and SD. INKAR online n.d. https://www.inkar.de/. Accessed 23 Dec 2021
Wissenschaftsrat: Hintergrundinformation zur Medizinierausbildung in Deutschland (Modellstudiengänge) (14 Jul 2014) (2019). https://www.wissenschaftsrat.de/download/archiv/hginfo_2114.pdf. Accessed 15 Jan 2020
World Health Organization (WHO): Diabetes-Fact sheet (2019). https://www.who.int/health-topics/diabetes#tab=tab_1. Accessed 15 Jan 2020
Srinivasan, B.T., Jarvis, J., Khunti, K., Davies, M.J.: Recent advances in the management of type 2 diabetes mellitus: a review. Postgrad Med J 84, 524–531 (2008). https://doi.org/10.1136/pgmj.2008.067918
Dawson, K.G., Gomes, D., Gerstein, H., Blanchard, J.F., Kahler, K.H.: The economic cost of diabetes in Canada, 1998. Diabetes Care 25, 1303–1307 (2002). https://doi.org/10.2337/diacare.25.8.1303
Simpson, S.H., Corabian, P., Jacobs, P., Johnson, J.A.: The cost of major comorbidity in people with diabetes mellitus. CMAJ 168, 1661–1667 (2003)
von Ferber, L., Köster, I., Hauner, H.: Medical costs of diabetic complications total costs and excess costs by age and type of treatment results of the German CoDiM study. Exp Clin Endocrinol Diabetes 115, 97–104 (2007). https://doi.org/10.1055/s-2007-949152
Sundmacher, L., Fischbach, D., Schüttig, W., Naumann, C., Augustin, U., Faisst, C.: Which hospitalisations are ambulatory care-sensitive, to what degree, and how could the rates be reduced? Results of a group consensus study with German providers. Health Policy 119, 1415–1423 (2015). https://doi.org/10.1016/j.healthpol.2015.08.007
Niefeld, M.R., Braunstein, J.B., Wu, A.W., Saudek, C.D., Weller, W.E., Anderson, G.F.: Preventable hospitalization among elderly Medicare beneficiaries with type 2 diabetes. Diabetes Care 26, 1344–1349 (2003). https://doi.org/10.2337/DIACARE.26.5.1344
Kifmann, M.: Competition policy for health care provision in Germany. Health Policy (New York) 121, 119–125 (2017). https://doi.org/10.1016/J.HEALTHPOL.2016.11.014
OECD/European Observatory on Health Systems and Policies (2017) Germany: Country Health Profile 2017, State of Health in the EU, OECD Publishing, Paris/European Observatory on Health Systems and Policies, Brussels. https://doi.org/10.1787/9789264283398-en
Menec, V.H., Sirski, M., Attawar, D., Katz, A.: Does continuity of care with a family physician reduce hospitalizations among older adults? J Health Serv Res Policy 11, 196–201 (2006)
Bice, T.W., Boxerman, S.B.: A quantitative measure of continuity of care. Med Care 15, 347–349 (1977)
Cho, K.H., Lee, S.G., Jun, B., Jung, B.-Y., Kim, J.-H., Park, E.-C.: Effects of continuity of care on hospital admission in patients with type 2 diabetes: analysis of nationwide insurance data. BMC Health Serv Res 15, 107 (2015). https://doi.org/10.1186/s12913-015-0745-z
Chan, C.-L., You, H.-J., Huang, H.-T., Ting, H.-W.: Using an integrated COC index and multilevel measurements to verify the care outcome of patients with multiple chronic conditions. BMC Health Serv Res 12, 405 (2012). https://doi.org/10.1186/1472-6963-12-405
Nicolucci, A., Greenfield, S., Mattke, S.: Selecting indicators for the quality of diabetes care at the health systems level in OECD countries. Int J Qual Health Care 18, 26–30 (2006). https://doi.org/10.1093/intqhc/mzl023
Baicker, K., Chandra, A.: Medicare spending, the physician workforce, and beneficiaries’ quality of care. Health Aff 23, W4-184-W4-197 (2004). https://doi.org/10.1377/hlthaff.W4.184
Landgraf, R., Kellerer, M., Aberle, J., Fach, E.-M., Gallwitz, B., Hamann, A., et al.: Therapie des typ-2-diabetes. Diabetol Stoffwechsel 13, S144–S165 (2018)
Shekelle, P.G., Vijan, S.: Quality indicators for the management of diabetes mellitus for vulnerable older persons- RAND CORP SANTA MONICA CA Working paper WR-187 (2004)
Hwang, J.: Decomposing socioeconomic inequalities in the use of preventive eye screening services among individuals with diabetes in Korea. Int J Public Health 61, 613–620 (2016). https://doi.org/10.1007/s00038-016-0804-1
Colquhoun, A.J., Nicholson, K.G., Botha, J.L., Raymond, N.T.: Effectiveness of influenza vaccine in reducing hospital admissions in people with diabetes. Epidemiol Infect 119, 335–341 (1997). https://doi.org/10.1017/S095026889700825X
Robert Koch Institut: Empfehlungen der Ständigen Impfkommission beim Robert Koch-Institut–2019/2020. Epidemiol Bull, 314–64 (2019). https://doi.org/10.25646/6233.7
Kähm, K., Laxy, M., Schneider, U., Rogowski, W.H., Lhachimi, S.K., Holle, R.: Health care costs associated with incident complications in patients with type 2 diabetes in Germany. Diabetes Care 41, 971–978 (2018). https://doi.org/10.2337/dc17-1763
Alva, M.L., Gray, A., Mihaylova, B., Leal, J., Holman, R.R.: The impact of diabetes-related complications on healthcare costs: new results from the UKPDS (UKPDS 84). Diabet Med 32, 459–466 (2015). https://doi.org/10.1111/dme.12647
Gurney, J.K., Stanley, J., Sarfati, D.: The M3 multimorbidity index outperformed both Charlson and Elixhauser indices when predicting adverse outcomes in people with diabetes. J Clin Epidemiol 99, 144–152 (2018). https://doi.org/10.1016/j.jclinepi.2018.04.002
Freund, T., Campbell, S.M., Geissler, S., Kunz, C.U., Mahler, C., Peters-Klimm, F., et al.: Strategies for reducing potentially avoidable hospitalizations for ambulatory care-sensitive conditions. Ann Fam Med 11, 363–370 (2013). https://doi.org/10.1370/afm.1498
Gonçalves, M.R., Hauser, L., Prestes, I.V., Schmidt, M.I., Duncan, B.B., Harzheim, E.: Primary health care quality and hospitalizations for ambulatory care sensitive conditions in the public health system in Porto Alegre, Brazil. Fam Pract 33, 238–242 (2016). https://doi.org/10.1093/fampra/cmv051
Kim, A.M., Park, J.H., Yoon, T.H., Kim, Y.: Hospitalizations for ambulatory care sensitive conditions as an indicator of access to primary care and excess of bed supply. BMC Health Serv Res 19, 1–7 (2019). https://doi.org/10.1186/s12913-019-4098-x
Cameron, A.C., Trivedi, P.K.: Microeconometrics: methods and applications. Cambridge University Press, Cambridge (2005)
Fagan, E.B., Gibbons, C., Finnegan, S.C., Petterson, S., Peterson, L.E., Phillips, R.L., et al.: Family medicine graduate proximity to their site of training: policy options for improving the distribution of primary care access. Fam Med 47, 124–130 (2015)
Shorrocks, A.F.: Decomposition procedures for distributional analysis: a unified framework based on the Shapley value. J Econ Inequal 11, 99–126 (2013). https://doi.org/10.1007/s10888-011-9214-z
Staiger, D.O., Stock, J.H.: Instrumental variables regression with weak instruments. Econometrica 65, 557–586 (1997)
Galarraga, J.E., Mutter, R., Pines, J.M.: Costs associated with ambulatory care sensitive conditions across hospital-based settings. Acad Emerg Med 22, 172–181 (2015). https://doi.org/10.1111/acem.12579
Bazemore, A., Petterson, S., Peterson, L.E., Phillips, R.L.: More comprehensive care among family physicians is associated with lower costs and fewer hospitalizations. Ann Fam Med 13, 206–213 (2015). https://doi.org/10.1370/afm.1787
Wolters, R.J., Braspenning, J.C.C., Wensing, M.: Impact of primary care on hospital admission rates for diabetes patients: a systematic review. Diabetes Res Clin Pract 129, 182–196 (2017). https://doi.org/10.1016/J.DIABRES.2017.05.001
Röttger, J., Blümel, M., Busse, R.: Selective enrollment in disease management programs for coronary heart disease in Germany—an analysis based on cross-sectional survey and administrative claims data. BMC Health Serv Res 17, 246 (2017). https://doi.org/10.1186/s12913-017-2162-y
Saver, B.G., Wang, C.-Y., Dobie, S.A., Green, P.K., Baldwin, L.-M.: The central role of comorbidity in predicting ambulatory care sensitive hospitalizations. Eur J Public Health 24, 66–72 (2014). https://doi.org/10.1093/eurpub/ckt019
Hoffmann, F., Icks, A.: Diabetes prevalence based on health insurance claims: large differences between companies. Diabet Med 28, 919–923 (2011). https://doi.org/10.1111/j.1464-5491.2011.03305.x
Rahman, F., Guan, J., Glazier, R.H., Brown, A., Bierman, A.S., Croxford, R., et al.: Association between quality domains and health care spending across physician networks. PLoS ONE 13, e0195222 (2018). https://doi.org/10.1371/journal.pone.0195222
Funding
Open Access funding enabled and organized by Projekt DEAL. Research work was not funded by third party funding.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Schuettig, W., Sundmacher, L. The impact of ambulatory care spending, continuity and processes of care on ambulatory care sensitive hospitalizations. Eur J Health Econ 23, 1329–1340 (2022). https://doi.org/10.1007/s10198-022-01428-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10198-022-01428-y