
Abstract
Objectives
We perform a cost-effectiveness analysis (CEA) and budget impact analysis (BIA) of baloxavir marboxil compared to current care in the Netherlands for patients at risk of influenza-related complications, including patients with comorbidities and the elderly.
Methods
In the CEA, a decision tree model was developed to assess the cost-effectiveness of baloxavir marboxil for a cohort of 52-year-olds from a societal perspective. A lifetime horizon was taken by incorporating the quality-adjusted life expectancy. The BIA included different epidemiological scenarios, estimating different plausible epidemiological scenarios for seasonal influenza considering the whole Dutch population with an increased risk of influenza complications.
Results
The base-case ICER was estimated to be €8,300 per QALY. At the willingness-to-pay threshold of €20,000 per QALY, the probability of being cost effective was 58%. The base-case expected budget impact was €5.7 million on average per year, ranging from €1.5 million to €10.5 million based on the severity of the influenza epidemic and vaccine effectiveness.
Conclusion
In the Netherlands, baloxavir is a cost-effective treatment option for seasonal influenza, with a base-case ICER of €8,300 per QALY for the population aged 60 years and over and patients at high risk of influenza-related complications. For a large part, this ICER is driven by the reduction of the illness duration of influenza and productivity gains in the working population.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Influenza is an acute respiratory infection caused by various types of influenza A and B viruses in humans [1]. In many cases an infection with influenza will not lead to severe illness: these patients will not seek care and the infection will be self-limiting [2]. However, for a small percentage of patients an infection causes severe disease and these patients may need to be admitted to hospital [3]. A complicated illness course may be caused by a co-infection with bacteria, which can lead to a pneumonia, acute bronchitis or myocarditis [4]. Most cases of influenza will consistently be during the Winter season, but the intensity of epidemics vary considerably throughout the years [5]. The number of consults in Dutch primary care for influenza-like illness (ILI) differed considerably in the period between October 2013 and May 2019: ranging from 1200 consults during the influenza season to 2400 consults per 100,000 inhabitants [5]. The number of influenza-related hospitalizations also varies, ranging from 650 in 2014 to 9300 in 2018 (ICD J09–J11) [6]. The number of reported influenza-related deaths in this period ranged from 67 to 1207 [7], although this probably is an underestimation as not all influenza-related mortality will be primarily recorded as related to influenza. Excess deaths during severe epidemics can be as high as 9444, as was the case for the influenza season of 2017–2018 [8]. The majority of patients hospitalized and dying from influenza are over 65 years old [7]. Vaccinations have played an important role in preventing morbidity and mortality related to influenza, and have previously been estimated to reduce hospitalizations with 24% and deaths with 35% in the Netherlands [9].
In the Netherlands, elderly aged 60 years and older are invited for an annual influenza vaccination which can be administered by the general practitioner (GP) [10]. In addition, patients with certain comorbidities, such as dementia, obesity, and COPD/asthma, are also eligible for influenza vaccination [10]. Attaining a high coverage of influenza vaccinations will be important to be prepared for a potential influenza epidemic, especially in older adults. However, not everyone is willing to get the vaccine and efficacy is non-optimal as the strains against which the vaccine protects may not always match with the circulating influenza strains. In addition, on the national policy level, there is no target for the influenza vaccination coverage and for at-risk populations getting vaccinated remains highly facultative. Here, the Dutch government aims at good communication about the national vaccination programme for influenza, rather than implementing performance indicators such as vaccination coverage.
Antiviral treatment may be an important addition to the control of influenza infection and its complications to combat surges of influenza, especially in a world where the available hospital capacity may be under high pressure during the respiratory season due to COVID-19, influenza, and other (co-)infections. However, the use of antiviral treatment against influenza is yet uncommon in the Netherlands. One of the most common treatments is oseltamivir, but this is not reimbursed in the Netherlands [11] and the use of antivirals is currently not recommended by the Dutch society of General Practice (NHG) [12].
Recently, a new antiviral treatment was introduced: baloxavir marboxil (baloxavir further in text), also known under the brand name Xofluza®. In the CAPSTONE 1 and -2 trials, this antiviral was more effective at reducing the duration of symptoms and reduced influenza-related complications in otherwise-healthy adults and patients at high risk of complications compared to placebo [13, 14]. The effectiveness in alleviating influenza symptoms of baloxavir was similar to oseltamivir [13, 14], but baloxavir was more effective at reducing the viral load of influenza and the time to cessation of viral shedding [13], which may reduce transmission between patients [15]. Baloxavir needs to be taken within 48 h after the onset of symptoms and only needs to be administered once [14]. This treatment may be a good alternative not only for unvaccinated patients at risk of influenza-related complications, such as the older adults and patients with comorbidities but also for vaccinated patients during influenza seasons in which the vaccine is reported to be less effective by the Dutch public health institute due to a mismatch with circulating influenza strains. Recently, it was decided to not reimburse baloxavir in the Netherlands, however, the cost-effectiveness was not considered in this decision [16].
In this paper, we will perform a cost-effectiveness analysis (CEA) and budget impact (BI) analysis of baloxavir compared to current care in the Netherlands for patients at risk of influenza-related complications, including patients with comorbidities and the elderly. We will assess different scenarios regarding influenza incidence, vaccination effectiveness, and vaccination coverage, as these are highly uncertain after two years of strict infection prevention and control measures during the pandemic.
Methods
Intervention
With this analysis, we compared the current standard of care for seasonal influenza patients in the Dutch outpatient setting, to a scenario where baloxavir is considered for patients that have an indication for the annual influenza vaccination. The current standard of care can be described as symptomatic treatment, primarily with paracetamol, as the use of antivirals is not currently recommended in the Netherlands [12]. As the Netherlands has historically been conservative regarding the use of influenza treatments, we did not consider the introduction for the otherwise-healthy population under 60 years. In addition, since baloxavir was not approved in Europe for children under 12 years at the time of writing, we also did not consider this group.
Cost-effectiveness model
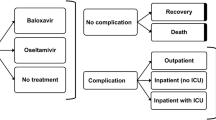
A probabilistic static closed cohort model with a typical short time frame was developed, as most influenza episodes will be short and without long-term complications. A lifetime horizon was taken by incorporating the quality-adjusted life years (QALYs) lost in the case of mortality, considering the cohort’s life expectancy. In line with Dutch guidelines, costs were discounted with 4% and health losses with 1.5% [17]. An overview of the model, visualized as a decision tree, is provided in Fig. 1.

Overview of cost-effectiveness and budget impact models—ILI influenza-like illness
For the base-case CEA, the target population was chosen to reflect the CAPSTONE-2 trial as closely as possible: a cohort of 1000 52-year-olds was considered, an even mix between males and females and all with underlying comorbidities [14]. Different age groups were considered in separate scenarios. The analysis was conducted from the societal perspective, according to the guidelines for conducting CEA in the Netherlands [17]. The model is available upon reasonable request. The Consolidated Health Economic Evaluation Reporting Standards checklist was included in the supplementary information [18].
BI model
A separate model, also displayed in Fig. 1, was developed to assess the BI of baloxavir over five influenza seasons starting in October 2022 and ending in May 2028. The BI was calculated for the whole eligible population in the Netherlands, which was estimated to be around 5.6 million individuals in the Netherlands in 2022, covering both vaccinated and unvaccinated people [19, 20]. The healthcare perspective was used for the BI analysis, e.g. no productivity losses were included.
For the BI model, the annual number of patients eligible for a baloxavir prescription needed to be estimated. ILI incidence as published by the World Health Organization for the Netherlands was used [5], using the five most recent influenza seasons before the COVID-19 pandemic. The influenza season was assumed to start every year in October and end in May. Baloxavir is only indicated for patients consulting their GP within 48 h after symptom onset, which was estimated to be the case for 67% of patients [21]. For the decision to prescribe baloxavir, we considered the patient’s vaccination status and the protection of the vaccine to the circulating strain of influenza. In the intervention group, all unvaccinated patients eligible for the annual influenza vaccine consulting for ILI would be prescribed baloxavir by the GP, while vaccinated patients would only be prescribed baloxavir if the vaccine was a mismatch with the circulating strains of influenza. To assess the proportion of patients adequately protected by an influenza vaccine, Dutch vaccine coverage data were used [20]. The key parameters for the BI analysis are included in the supplementary information.
Input parameters
Clinical inputs
The main clinical inputs considered were the duration of illness and mortality. 38% of patients consulting for ILI were considered to have an infection with influenza and baloxavir was assumed to only be effective for the “true influenza” group [22]. Since this varies highly between influenza seasons, this number was extensively varied in the probabilistic sensitivity analysis (PSA) [22]. Currently, influenza point-of-care (POC) diagnostics are not recommended in the Netherlands [4, 23]. To incorporate a potential scenario where POC diagnostics for influenza are widely implemented, a scenario was included where only patients with true influenza were treated with baloxavir. For patients with true influenza the duration of illness was modelled using data from the CAPSTONE-2 trial. The secondary clinical endpoint “time to return to pre-influenza health” was used, as this was expected to capture the full extent of the patients’ disease episode [14]. For the baloxavir group, this corresponded to an average duration of illness of 5.3 days, while this was 6.2 for the current standard of care group [14]. As a scenario, the primary efficacy endpoint was used: “time to improvement of symptoms” [14]. Various complications were included using the data reported in the CAPSTONE-2 trial: hospitalization, sinusitis, otitis media, bronchitis, and outpatient pneumonia [14]. Mortality was assumed to only occur in the hospital. Previously-reported in-hospital mortality stratified for age groups were used: 4% for 15–64 year olds (base case) and 43% for patients older than 65 years [24].
In case of an influenza infection resistant against baloxavir or ILI caused by other pathogens, simplified inputs were used as the outcomes were assumed to be the same for the baloxavir and current standard of care arms in the model. The disease duration for this group was 7.7 days in the base case [21] and the mortality rate 0.1% for patients aged 50–64 (base case) or 1.4% for patients aged 65 years and older [25]. Although baloxavir resistance was not considered in the base case, we did include it as a scenario. The main clinical inputs for the model are displayed in Table 1.
Utilities
For both true influenza and ILI caused by other pathogens, a disutility of 0.32 quality-adjusted life days was used per day of illness [26, 27]. Considering a full influenza episode, this resulted in a per-patient QALY loss of 0.0046 and 0.0055 QALYs in the baloxavir and current standard of care groups, respectively [14]. For both inpatient and outpatient complications, a disutility of 0.37 quality-adjusted life days was considered [25]. These disabilities were based on Belgian and British data, which was assumed to be comparable to the Dutch setting and varied in sensitivity analyses. For deceased patients, the QALYs lost were calculated using the age and sex-dependent life expectancy, which was 27.4 QALYs in the base case. Age and sex-dependent utilities were also applied [28] and future QALYs were discounted.
Table 1 clinical input parameters
Costs
The main costs are displayed in Table 2. The costs were based on Dutch reference prices whenever possible. Hospitalization costs for influenza-related complications were used as published previously [29], as well as costs associated with outpatient pneumonia [30]. For the other outpatient complications, the costs were assumed equal to one GP consult. Productivity losses were included in the model, based on an average number of hours worked per day of 4.4 [31], an unemployment rate of 14% [32], and hourly wages of €36.19 [33]. For unpaid work, people were assumed to spend an average of 4 h per week on this [34] and it was valued as informal care at €14.58 per hour [33]. In case of mortality, the production losses were estimated using the friction cost method, with a friction period of 126 days [17, 33, 35, 36]. Future non-related medical costs for all survivors were included in a scenario analysis using the PAID 3.0 tool [37, 38]. All costs were inflated to 2021 euros using the consumer price index [39].
Analysis
Cost-effectiveness analysis
The main health-economic outcome considered was the incremental cost-effectiveness ratio (ICER) expressed as the costs per QALY. A deterministic sensitivity analysis was performed to assess the effect of varying individual input parameters on the ICER, and this was visualized using a Tornado diagram. The inputs were varied with plus and minus 25%. A PSA was performed to assess the effect of varying all parameters simultaneously in a Monte Carlo simulation using 10,000 model replications, using the distributions and ranges of the input parameters as detailed in Table 1. A cost-effectiveness plane and cost-effectiveness acceptability curve (CEAC) were constructed to visualize the results. Various scenario analyses were performed:
-
outcome used is “Time to improvement of symptoms” from CAPSTONE-2;
-
only patients with true influenza are treated with baloxavir;
-
baloxavir resistance set to 10% (assumption);
-
cohort of age 65;
-
cohort of age 75;
-
inclusion of indirect medical costs in life years gained;
-
using a healthcare perspective;
-
using a healthcare perspective and equal discounting at 3.5%.
For these scenarios the deterministic ICER was calculated, as well as the probability of being cost-effective at both the €20,000 and the €50,000 willingness-to-pay thresholds, which are used in the Netherlands. All ICERs were rounded to the nearest hundreds of euros.
BI
The BI was expected to vary depending on the incidence of ILI and the effectiveness of the influenza vaccination campaign. In the base case, we estimated the average BI of baloxavir by using historical incidence data over several influenza seasons and averaging these. In addition, we included two sensitivity analyses: a best-case scenario with low incidence of ILI and a high vaccination coverage, taking the COVID-19 booster campaign as an example, and a worst-case scenario where a mismatch of the vaccine with the currently circulating virus was assumed and all patients consulting for ILI aged 60 years or within a risk group were treated with baloxavir.
Results
Cost effectiveness
The base-case ICER was estimated to be €8,300 per QALY, see also Table 3 for an overview. At the willingness-to-pay threshold of €20,000 per QALY, the probability of being cost effective was 58%, or 71% at 50,000 per QALY, see also Fig. 2 for the CEAC and the CE plane included in the supplementary information. Table 3 also includes various scenario analyses. The DSA is shown in Fig. 3; the main parameters influencing the model are the illness duration, costs of baloxavir, discounting, hourly wages, and the occurrence of complications, including hospitalizations.

Cost-effectiveness acceptability curve of baloxavir compared to care as usual

Tornado diagram of deterministic sensitivity analysis
BI
The base-case expected BI was €5.7 million on average per year. The best-case scenario, where ILI incidence was assumed to be at the lowest level since 2014–2015 with a good match between the vaccine and the circulating types of influenza, was €1.5 million. The worst-case, with a high incidence of ILI and a mismatch between the vaccine and circulating types of influenza, increased the BI to €10.5 million. A relevant outcome for the healthcare sector is the number of influenza-related hospitalizations, which is reduced annually by 263 in the base-case scenario and up to 501 in the worst-case scenario. A full overview is displayed in Table 4.
Discussion
With a base-case ICER of €8,300 per QALY, baloxavir is likely to be cost effective for the Dutch setting, although the probabilistic results show quite some uncertainty around this estimate. This uncertainty is mainly due to the small number of complications measures in the CAPSTONE 2 trial, and the resulting uncertainty. In around 20% of the simulations, baloxavir is associated with health losses, i.e. the ICER is in the upper-left quadrant. In those simulations, the probability of some of the complications, mainly the number of hospitalizations is higher in the baloxavir arm. Baloxavir is considered cost-saving in around 30% of the simulations: the productivity gains and prevented complications are sufficient to offset the costs of baloxavir. We have included several scenarios for older adult populations, and both the deterministic and probabilistic results are robust, i.e., baloxavir can be considered cost-effective. Productivity losses play a minor role in these older cohorts, but the cost effectiveness is mainly driven by prevented hospitalizations and mortality, as older generations have higher risks for these clinical events.
The BI of baloxavir is estimated at €5.7 million per year in the base-case scenario and mainly depends on the incidence of ILI, the vaccine effectiveness, and the vaccine coverage. Between the best-case and the worst-case scenarios, the BI ranged from €1.5 million to €10.5 million.
This is the first study assessing the cost-effectiveness and BI for baloxavir in a European country. Two economic analyses have been published for Japan [40, 41], one of which [40] assessed baloxavir for high-risk patients. Although the authors also used a decision tree, there are some important differences due to the setting for which the cost-effectiveness was assessed: in the Japanese study baloxavir was compared to laninamivir, the most-often prescribed antiviral for influenza in that market, and the model incorporated the use of a rapid diagnostic test for influenza [40]. No productivity losses were incorporated in the Japanese study [40]. However, since the QALY differences between the comparators are quite small, differences in drug costs and model assumptions can have a major impact on the ICER as can be seen in the deterministic sensitivity and scenario analyses. For other countries, other assumptions and costs inputs may need to be made. An example of a major difference could be that not in all countries, productivity losses are included, as is the case for the Netherlands [17]. The exclusion of productivity losses increases the ICER to €50,100 per QALY. Most countries use equal discounting rates for costs and effects, which means that our final scenario, in which an equal discounting rate was used and productivity losses were excluded may be the most generalizable result for other European countries. In this scenario the deterministic ICER was €59,900 per QALY. In most European countries, alternative influenza antiviral treatment is not often prescribed [42], but for the countries where this is the case, another comparator may be more appropriate.
In a previous study, we showed the potential value of improved diagnostics for respiratory-tract infections, including ILI, in Dutch primary care [43]. Although improved diagnostic strategies had the potential to reduce antimicrobial resistance, significant investments needed to be made in diagnostics [43]. The scenario included in the present study where the proportion of true influenza cases is increased from 38 to 100% shows that this makes baloxavir treatment highly likely to be cost saving. Improved influenza diagnostics could further personalize baloxavir prescriptions, as primarily patients likely to benefit from the treatment will receive it. This study shows that further targeted treatment could offset some of the additional costs of improved diagnostic strategies, provided adequately performing diagnostic tests are available.
The present study has some limitations. The modelled results are uncertain, due to the uncertainty associated with the main outcomes, such as most importantly the hospitalization rate. As influenza only causes serious complications in a small fraction of infected patients [14], a large number of patients would need to be included in a trial to show a significant difference in all the separately modelled complications. However, the aggregated occurrence of influenza-associated complications was significantly lower in the baloxavir group compared to placebo [14]. There were no adverse events included in the model, as the safety profile of baloxavir in adults is very similar to placebo [13, 14, 44]. We only included inpatient mortality, which we expect to underestimate the real mortality as patients may also decease in the outpatient setting. Although baloxavir has shown to reduce the viral load of influenza and the time to cessation of viral shedding, which may impact transmission [13, 15], this was not included in the CEA. We do not expect the targeted implementation of baloxavir, as proposed in this paper, would have a major impact on influenza transmission. Finally, we assessed a seasonal influenza situation, and although baloxavir may provide value to prepare for influenza pandemics as well, this was outside of the scope of the current research.
As we enter a situation where further measures to reduce COVID-19 transmission are hopefully not necessary, a surge of other respiratory infections is something that should be considered by policy makers. This includes a toolbox with adequate vaccination programmes, sufficient diagnostic capacity, and effective treatment against infections. For the Netherlands, baloxavir is a cost-effective influenza antiviral treatment that can be a part of a comprehensive strategy to manage the effects of respiratory infections in terms of healthcare capacity and the economic effects of absence from work. Therefore, in the likely situation of a seasonal influenza outbreak, not reimbursing baloxavir could be considered a loss of opportunity from health, broader societal and economic perspectives. Yet, the interdependency between seasonal risk, effectiveness of the seasonal vaccine and vaccine coverage clearly defines the complexity of assessing the added value and need for antivirals in the treatment of influenza. Although an effective influenza vaccination programme should remain a priority, antiviral treatment can be important from an equity perspective, as vaccine coverage in the Netherlands is lower in groups with a low socio-economic status [45] and certain religious subgroups [46].
Conclusion
In the Netherlands, baloxavir is a cost-effective treatment option for seasonal influenza, with a base-case ICER of €8,300 per QALY for the population aged 60 years and over and patients at high risk of influenza-related complications. For a large part, this ICER is driven by the illness duration of influenza and productivity gains in the working population.
Data availability
The data that support the findings of this study are available from the corresponding author, upon reasonable request.
References
Krammer, F., Smith, G.J.D., Fouchier, R.A.M., Peiris, M., Kedzierska, K., Doherty, P.C., Palese, P., Shaw, M.L., Treanor, J., Webster, R.G., García-Sastre, A.: Influenza. Nat. Rev. Dis. Primer. 4, 3 (2018). https://doi.org/10.1038/s41572-018-0002-y
Teirlinck, A.C., de Gier, B., Meijer, A., Donker, G., de Lange, M., Koppeschaar, C., van der Hoek, W., Kretzschmar, M.E., McDonald, S.A.: The incidence of symptomatic infection with influenza virus in the Netherlands 2011/2012 through 2016/2017, estimated using Bayesian evidence synthesis. Epidemiol. Infect. (2019). https://doi.org/10.1017/S095026881800273X
Gezondheidsraad: Vaccinatie risicogroepen op grond van leeftijd en medische indicatie. Den Haag (2021). https://www.gezondheidsraad.nl/binaries/gezondheidsraad/documenten/adviezen/2021/09/20/griepvaccinatie-herziening-van-de-indicatiestelling-2021/Achtergronddocument_risicogroepen.pdf
LCI richtlijnen. Influenza. https://lci.rivm.nl/richtlijnen/influenza. Accessed 17 Dec 2021
World Health Organization WHO FLUMART OUTPUTS. https://apps.who.int/flumart/Default?ReportNo=16
StatLine–Ziekenhuisopnamen en-patiënten; diagnose-indeling ICD-10 (3-teken niveau). https://opendata.cbs.nl/#/CBS/nl/dataset/84069NED/table?searchKeywords=Nederland%20in%20cijfers
Centraal Bureau voor de Statistiek: Overledenen; doodsoorzaak (uitgebreide lijst), leeftijd, geslacht. https://opendata.cbs.nl/statline/#/CBS/nl/dataset/7233/table?ts=1640005380130
Monitoring sterftecijfers Nederland|RIVM. https://www.rivm.nl/monitoring-sterftecijfers-nederland
Backer, J.A., Wallinga, J., Meijer, A., Donker, G.A., van der Hoek, W., van Boven, M.: The impact of influenza vaccination on infection, hospitalisation and mortality in the Netherlands between 2003 and 2015. Epidemics 26, 77–85 (2019). https://doi.org/10.1016/j.epidem.2018.10.001
Gezondheidsraad: Griepvaccinatie: herziening van de indicatiestelling 2021. Den Haag (2021). https://www.gezondheidsraad.nl/documenten/adviezen/2021/09/20/griepvaccinatie-herziening-van-de-indicatiestelling-2021
Zorginstituut Nederland: Medicijnkosten. https://www.medicijnkosten.nl/
Influenza|NHG-Richtlijnen. https://richtlijnen.nhg.org/behandelrichtlijnen/influenza
Hayden, F.G., Sugaya, N., Hirotsu, N., Lee, N., de Jong, M.D., Hurt, A.C., Ishida, T., Sekino, H., Yamada, K., Portsmouth, S., Kawaguchi, K., Shishido, T., Arai, M., Tsuchiya, K., Uehara, T., Watanabe, A.: Baloxavir marboxil for uncomplicated influenza in adults and adolescents. N. Engl. J. Med. 379, 913–923 (2018). https://doi.org/10.1056/NEJMoa1716197
Ison, M.G., Portsmouth, S., Yoshida, Y., Shishido, T., Mitchener, M., Tsuchiya, K., Uehara, T., Hayden, F.G.: Early treatment with baloxavir marboxil in high-risk adolescent and adult outpatients with uncomplicated influenza (CAPSTONE-2): a randomised, placebo-controlled, phase 3 trial. Lancet Infect. Dis. 20, 1204–1214 (2020). https://doi.org/10.1016/S1473-3099(20)30004-9
Hayden, F.G., Asher, J., Cowling, B.J., Hurt, A.C., Ikematsu, H., Kuhlbusch, K., Lemenuel-Diot, A., Du, Z., Meyers, L.A., Piedra, P.A., Takazono, T., Yen, H.-L., Monto, A.S.: Reducing influenza virus transmission: the potential value of antiviral treatment. Clin. Infect. Dis. 74, 532–540 (2022). https://doi.org/10.1093/cid/ciab625
Ministerie van Volksgezondheid Welzijn en Sport: GVS-advies baloxavir marboxil (Xofluza®) – Advies - Zorginstituut Nederland. https://www.zorginstituutnederland.nl/publicaties/adviezen/2022/11/24/gvs-advies-baloxavir-marboxil-xofluza
Zorginstituut Nederland: Guideline for economic evaluations in healthcare. Diemen (2016)
Husereau, D., Drummond, M., Augustovski, F., de Bekker-Grob, E., Briggs, A.H., Carswell, C., Caulley, L., Chaiyakunapruk, N., Greenberg, D., Loder, E., Mauskopf, J., Mullins, C.D., Petrou, S., Pwu, R.-F., Staniszewska, S.: Consolidated Health Economic Evaluation Reporting Standards 2022 (CHEERS 2022) statement: updated reporting guidance for health economic evaluations. Eur. J. Health Econ. 23, 1309–1317 (2022). https://doi.org/10.1007/s10198-021-01426-6
Statistics Netherlands: CBS StatLine - Bevolking; geslacht, leeftijd en burgerlijke staat, 1 januari. http://statline.cbs.nl/Statweb/publication/?DM=SLNL&PA=7461BEV&D1=0&D2=1-2&D3=1-100&D4=61&HDR=T,G3&STB=G1,G2&VW=T
Heins M Hooiveld, Mariëtte, Hooiveld M, Korevaar J. Monitor Vaccinatiegraad Nationaal Programma Grieppreventie 2019. NIVEL; 2020. ISBN: 978-94-6122-641-9
Butler, C.C., van der Velden, A.W., Bongard, E., Saville, B.R., Holmes, J., Coenen, S., Cook, J., Francis, N.A., Lewis, R.J., Godycki-Cwirko, M., Llor, C., Chlabicz, S., Lionis, C., Seifert, B., Sundvall, P.-D., Colliers, A., Aabenhus, R., Bjerrum, L., Jonassen Harbin, N., Lindbæk, M., Glinz, D., Bucher, H.C., Kovács, B., Radzeviciene Jurgute, R., Touboul Lundgren, P., Little, P., Murphy, A.W., De Sutter, A., Openshaw, P., de Jong, M.D., Connor, J.T., Matheeussen, V., Ieven, M., Goossens, H., Verheij, T.J.: Oseltamivir plus usual care versus usual care for influenza-like illness in primary care: an open-label, pragmatic, randomised controlled trial. The Lancet. 395, 42–52 (2020). https://doi.org/10.1016/S0140-6736(19)32982-4
Dolk, F.C.K., de Boer, P.T., Nagy, L., Donker, G.A., Meijer, A., Postma, M.J., Pitman, R.: Consultations for influenza-like illness in primary care in The Netherlands: a regression approach. Value Health. 24, 11–18 (2021). https://doi.org/10.1016/j.jval.2020.10.013
Nederlandse vereniging voor medische microbiologie. Behandeling Influenza (2021). https://richtlijnendatabase.nl/richtlijn/behandeling_influenza/startpagina_-_behandeling_influenza.html. Accessed 20 Dec 2021
Cromer, D., van Hoek, A.J., Jit, M., Edmunds, W.J., Fleming, D., Miller, E.: The burden of influenza in England by age and clinical risk group: a statistical analysis to inform vaccine policy. J. Infect. 68, 363–371 (2014). https://doi.org/10.1016/j.jinf.2013.11.013
Tappenden, P., Jackson, R., Cooper, K., Rees, A., Simpson, E., Read, R., Nicholson, K.: Amantadine, oseltamivir and zanamivir for the prophylaxis of influenza (including a review of existing guidance no. 67): a systematic review and economic evaluation. Health Technol. Assess. (2009). https://doi.org/10.3310/hta13110
Bilcke, J., Coenen, S., Beutels, P.: Influenza-like-illness and clinically diagnosed flu: disease burden, costs and quality of life for patients seeking ambulatory care or no professional care at all. PLoS ONE 9, e102634 (2014). https://doi.org/10.1371/journal.pone.0102634
Dolk, C., Eichner, M., Welte, R., Anastassopoulou, A., Van Bellinghen, L.-A., Poulsen Nautrup, B., Van Vlaenderen, I., Schmidt-Ott, R., Schwehm, M., Postma, M.: Cost-utility of quadrivalent versus trivalent influenza vaccine in germany, using an individual-based dynamic transmission model. Pharmacoeconomics 34, 1299–1308 (2016). https://doi.org/10.1007/s40273-016-0443-7
Szende, A., Janssen, B., Cabases, J. (eds.): Self-Reported Population Health: An International Perspective based on EQ-5D. Springer, Dordrecht (2014)
Marbus, S.D., Schweitzer, V.A., Groeneveld, G.H., Oosterheert, J.J., Schneeberger, P.M., van der Hoek, W., van Dissel, J.T., van Gageldonk-Lafeber, A.B., Mangen, M.-J.: Incidence and costs of hospitalized adult influenza patients in The Netherlands: a retrospective observational study. Eur. J. Health Econ. 21, 775–785 (2020). https://doi.org/10.1007/s10198-020-01172-1
Fens, T., van der Pol, S., Kocks, J.W.H., Postma, M.J., van Boven, J.F.M.: Economic impact of reducing inappropriate inhaled corticosteroids use in patients with chronic obstructive pulmonary disease: ISPOR’s guidance on budget impact in practice. Value Health. 22, 1092–1101 (2019). https://doi.org/10.1016/j.jval.2019.05.006
Centraal Bureau voor de Statistiek: Werkzame beroepsbevolking; arbeidsduur. https://www.cbs.nl/nl-nl/cijfers/detail/82647NED?dl=BB64
Centraal Bureau voor de Statistiek: StatLine–Arbeidsdeelname; kerncijfers. https://opendata.cbs.nl/statline/?dl=67DF4#/CBS/nl/dataset/82309NED/table
Hakkaart-van Roijen, L., Van der Linden, N., Bouwmans, C., Kanters, T., Tan, S: Kostenhandleiding: methodologie van kostenonderzoek en referentieprijzen voor economische evaluaties in de gezondheidszorg. Zorginstituut Nederland, Diemen (2015). https://www.zorginstituutnederland.nl/binaries/zinl/documenten/publicatie/2016/02/29/richtlijn-voor-het-uitvoeren-van-economische-evaluaties-in-de-gezondheidszorg/Richtlijn+voor+het+uitvoeren+van+economische+evaluaties+in+de+gezondheidszorg+(verdiepingsmodules).pdf
Statistiek, C.B. voor de: Vrijwilligerswerk 2020. https://www.cbs.nl/nl-nl/longread/rapportages/2021/vrijwilligerswerk-2020
Koopmanschap, M.A., Rutten, F.F.H., van Ineveld, B.M., van Roijen, L.: The friction cost method for measuring indirect costs of disease. J. Health Econ. 14, 171–189 (1995). https://doi.org/10.1016/0167-6296(94)00044-5
Centraal Bureau voor de Statistiek: Vacatures; stromen, seizoengecorrigeerd. https://opendata.cbs.nl/statline/portal.html?_la=nl&_catalog=CBS&tableId=84545NED&_theme=5
van Baal, P.H.M., Wong, A., Slobbe, L.C.J., Polder, J.J., Brouwer, W.B.F., de Wit, G.A.: Standardizing the inclusion of indirect medical costs in economic evaluations. Pharmacoeconomics 29, 175–187 (2011). https://doi.org/10.2165/11586130-000000000-00000
PAID 3.0. https://imta.shinyapps.io/PAID3code/
Centraal bureau voor de statistiek: Consumer price Index. https://opendata.cbs.nl/statline/#/CBS/nl/dataset/83131NED/table?ts=1627889467468
Dronova, M., Ikeoka, H., Itsumura, N., Hirotsu, N., Ansaripour, A., Aballéa, S., Onishi, Y., Hill, M., Igarashi, A.: Cost-effectiveness of baloxavir marboxil compared with laninamivir for the treatment of influenza in patients at high risk for complications in Japan. Curr. Med. Res. Opin. 37, 1135–1148 (2021). https://doi.org/10.1080/03007995.2021.1914942
Skrzeczek, A., Ikeoka, H., Hirotsu, N., Ansaripour, A., Aballéa, S., Onishi, Y., Hill, M., Igarashi, A.: Cost-effectiveness of baloxavir marboxil compared to laninamivir for the treatment of influenza in Japan. J. Infect. Chemother. Off. J. Jpn. Soc. Chemother. 27, 296–305 (2021). https://doi.org/10.1016/j.jiac.2020.10.018
van der Velden, A., van de Pol, A.C., Bongard, E., Cianci, D., Aabenhus, R., Balan, A., Böhmer, F., Lang, V.B., Bruno, P., Chlabicz, S., Coenen, S., Colliers, A., Garcia-Sangenis, A., Ghazaryan, H., Godycki-Cwirko, M., Jensen, S., Lionis, C., van der Linde, S.R., Malania, L., Pauer, J., Tomacinschii, A., Vellinga, A., Zastavnyy, I., Emmerich, S., Zerda, A., Verheij, T.J., Goossens, H., Butler, C.C.: Point of care testing, antibiotic prescribing and prescribing confidence for respiratory tract infections in primary care: prospective audit in 18 European countries. BJGP Open. (2021). https://doi.org/10.3399/BJGPO.2021.0212
van der Pol, S., Jansen, D.E.M.C., van der Velden, A.W., Butler, C.C., Verheij, T.J.M., Friedrich, A.W., Postma, M.J., van Asselt, A.D.I.: The opportunity of point-of-care diagnostics in general practice: modelling the effects on antimicrobial resistance. Pharmacoeconomics 40, 823–833 (2022). https://doi.org/10.1007/s40273-022-01165-3
Nakazawa, M., Hara, K., Komeda, T., Ogura, E.: Safety and effectiveness of baloxavir marboxil for the treatment of influenza in Japanese clinical practice: a postmarketing surveillance of more than 3000 patients. J. Infect. Chemother. Off. J. Jpn. Soc. Chemother. 26, 729–735 (2020). https://doi.org/10.1016/j.jiac.2020.04.014
Labuschagne, L.J.E., Smorenburg, N., van de Kassteele, J., Bom, B., de Weerdt, A.C., de Melker, H.E., Hahné, S.J.M.: Neighbourhood sociodemographic factors and COVID-19 vaccine uptake in the Netherlands: an ecological analysis. BMC Public Health 23, 1696 (2023). https://doi.org/10.1186/s12889-023-16600-z
Ruijs, W.L., Hautvast, J.L., van der Velden, K., de Vos, S., Knippenberg, H., Hulscher, M.E.: Religious subgroups influencing vaccination coverage in the Dutch Bible belt: an ecological study. BMC Public Health 11, 102 (2011). https://doi.org/10.1186/1471-2458-11-102
Teirlinck, A., van Asten, L., Brandsema, P., Dijkstra, F., Donker, G., Euser, S., van Gageldonk-Lafeber, A., Hooiveld, M., Lange, M. de, Meijer, A., Slump, E., van der Hoek, W.: Surveillance of influenza and other respiratory infections in the Netherlands: winter 2014/2015 (2015). (Rijksinstituut voor Volksgezondheid en Milieu RIVM). https://rivm.openrepository.com/handle/10029/579782
Teirlinck, A., van Asten, L., Brandsema, P., Dijkstra, F., Donker, G., van Gageldonk-Lafeber, A., Hooiveld, M., de Lange, M., Marbus, S., Meijer, A., van der Hoek, W.: Annual report. Surveillance of influenza and other respiratory infections in the Netherlands: winter 2015/2016 : Surveillance van influenza en andere luchtweginfecties: winter 2015/2016 (2016). (Rijksinstituut voor Volksgezondheid en Milieu RIVM). https://rivm.openrepository.com/handle/10029/620744
Teirlinck, A., van Asten, L., Brandsema, P., Dijkstra, F., Donker, G., van Gageldonk-Lafeber, A., Hooiveld, M., de Lange, M., Marbus, S., Meijer, A., van der Hoek, W.: Annual report Surveillance of influenza and other respiratory infections in the Netherlands: Winter 2016/2017 (2017). (Rijksinstituut voor Volksgezondheid en Milieu RIVM). https://rivm.openrepository.com/handle/10029/620919
Reukers, D., Asten, L. van, Brandsema, P., Dijkstra, F., Donker, G., Dam-Deisz, W., Hooiveld, M., Lange, M. de, Marbus, S., van den Broek, I., Meijer, A., Hoek, W. van der.: Annual report Surveillance of influenza and other respiratory infections: Winter 2017/2018 (2018). (Rijksinstituut voor Volksgezondheid en Milieu RIVM). https://rivm.openrepository.com/handle/10029/622145
Reukers, D.F.M., van Asten, L., Brandsema, P.S., Dijkstra, F., Donker, G.A., van Gageldonk-Lafeber, A.B., Hooiveld, M., de Lange, M.M.A., Marbus, S., Teirlinck, A.C., Meijer, A., van der Hoek, W.: Annual report Surveillance of influenza and other respiratory infections in the Netherlands: winter 2018/2019 (2019). (Rijksinstituut voor Volkgezondheid en Milieu RIVM). https://rivm.openrepository.com/handle/10029/623227
Acknowledgements
We would like to acknowledge the support from Roche Netherlands, especially Jeannette van der Ven and Luuk den Boer.
Funding
This study was sponsored by Roche Netherlands B.V.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Prof. Dr. Maarten J. Postma and Prof. Dr. Cornelis Boersma received grants and honoraria from various pharmaceutical companies, inclusive those developing, producing, and marketing influenza antivirals and vaccines. Dr. Simon van der Pol has no relevant financial or non-financial interests to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
van der Pol, S., Postma, M.J. & Boersma, C. Antivirals to prepare for surges in influenza cases: an economic evaluation of baloxavir marboxil for the Netherlands. Eur J Health Econ (2024). https://doi.org/10.1007/s10198-024-01683-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10198-024-01683-1