
Abstract
Sexual minority men (SMM) are disproportionately affected by HIV. Although pre-exposure prophylaxis (PrEP) is an effective way of reducing HIV incidence, PrEP use has remained relatively low. Social support may be one effective factor in increasing PrEP use among SMM, but the association between social support and PrEP use/adherence is not well understood. The objective of this paper was to summarize the current literature on the association of social support and PrEP use among SMM in the United States. A systematic search was conducted using six different databases MEDLINE / PubMed, PsycINFO, Cochrane CENTRAL, Google Scholar, Embase, and Web of Science using terms established from keywords and medical subject headings (MeSH) terms before being adapted to each database. Data were extracted for key study factors (e.g., study population, geographic location, study design) and main findings. This search produced eleven articles: ten manuscripts and one conference abstract. Of these, two were randomized control trials, two were interventions, three were qualitative, and four were cross-sectional. The studies were widespread across the country, but most were in major metropolitan areas. From the articles included in this review, findings were inconsistent in the association between social support; some studies showed null findings, others that only certain sources of social support were significant, and others that there was a significant association between social support and PrEP use. This review highlights the complexity of the relationship between social support and PrEP use among SMM, indicating the need for further research to identify specific types and sources of support that effectively enhance PrEP uptake and adherence. Targeted interventions based on these insights could significantly reduce HIV incidence in the population.
Resumen
Los hombres pertenecientes a minorías sexuales (HSH) se ven afectados de forma desproporcionada por el VIH. Aunque la profilaxis preexposición (PrEP) es una forma eficaz de reducir la incidencia del VIH, el uso de la PrEP se ha mantenido relativamente bajo. El apoyo social puede ser un factor eficaz para aumentar el uso de la PrEP entre los SMM, pero la asociación entre el apoyo social y el uso/adherencia a la PrEP no se conoce bien. El objetivo de este documento fue resumir la literatura actual sobre la asociación entre el apoyo social y el uso de la PrEP entre los HSH en los Estados Unidos. Se realizó una búsqueda sistemática en seis bases de datos diferentes MEDLINE / PubMed, PsycINFO, Cochrane CENTRAL, Google Scholar, Embase y Web of Science utilizando términos basados en palabras clave y términos de encabezamientos de materias médicas (MeSH) antes de adaptarlos a cada base de datos. Se extrajeron datos para los factores clave del estudio (p. ej., población del estudio, ubicación geográfica, diseño del estudio) y los hallazgos principales. Esta búsqueda produjo once artículos: diez manuscritos y un resumen de conferencia. De ellos, dos eran estudios controlados aleatorizados, dos eran intervenciones, tres eran estudios cualitativos y cuatro eran estudios transversales. Los estudios estaban repartidos por todo el país, pero la mayoría se realizaban en las principales áreas metropolitanas. De los artículos incluidos en esta revisión, los hallazgos fueron inconsistentes en la asociación entre el apoyo social; algunos estudios mostraron hallazgos nulos, otros que sólo ciertas fuentes de apoyo social eran significativas y otros que existía una asociación significativa entre el apoyo social y el uso de la PrEP. Esta revisión pone de manifiesto la complejidad de la relación entre el apoyo social y el uso de la PrEP entre los HSH, lo que indica la necesidad de realizar más investigaciones para identificar los tipos y las fuentes de apoyo específicos que mejoran de forma efectiva la aceptación y el cumplimiento de la PrEP. Las intervenciones específicas basadas en estos conocimientos podrían reducir significativamente la incidencia del VIH en la población.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
An estimated 1.2 million individuals are living with human immunodeficiency virus (HIV) in the United States [1]. Sexual minority men (SMM) make up a disproportionately high rate of HIV incidence, accounting for 48% of all new HIV cases in 2019 [2]. In 2012, the landscape of the HIV epidemic changed due to the approval of pre-exposure prophylaxis (PrEP), the antiretroviral combination of emtricitabine and tenofovir disoproxil fumarate (Truvada ®; F/TDF), by the US Food and Drug Administration to prevent an individual from contracting HIV [3]. PrEP has since been found to be highly effective in preventing HIV infection among those who take it as prescribed [4,5,6,7,8,9]. Despite this, PrEP uptake has been slow; over 1.1 million individuals are estimated to have indications for PrEP, but only an estimated 224,000 individuals (around 20%) have a prescription [10, 11].
Although the awareness and usage of PrEP have increased since the time PrEP was approved in the US [12], there remain myriad barriers to accessing and remaining on PrEP for many SMM. Structural-level barriers to PrEP include limited access to healthcare services, a lack of health insurance, the inability to pay for a PrEP prescription, and a lack of providers with PrEP knowledge [13,14,15,16,17,18,19]. Moreover, previous studies have shown that culturally insensitive healthcare experiences concerning HIV stigma, racism, and homophobia increase medical mistrust and reduce the likelihood of engaging in PrEP or other preventative HIV behaviors among SMM [20]. Individual-level psychosocial barriers include a lack of knowledge about PrEP and concern for PrEP side effects. Further, there is a societal stigma associated with taking PrEP, wherein PrEP has been associated with promiscuity, infidelity, and homosexuality [21,22,23,24,25,26].
Fortunately, social support may be a factor that can mitigate some of these barriers to increase PrEP use and adherence among SMM. Social support is defined as any communication from providers to a recipient that decreases uncertainty and increases the recipient’s personal control in a situation [27]. Social support may arise from different people in one’s social network and can express itself in different ways. Social support theory posits that there are three main forms of social support that can impact health behavior: emotional support (esteem, concern) instrumental support (tangible resources such as money, aid, time), or informational support (education) [28]. Social support may also come from formal sources, such as professional health providers (e.g., counselors or therapists) [29, 30]. Among the lesbian, gay, bisexual, transgender, queer, and more (LGBTQ+) community, a “chosen family” or “gay family”, groups comprised of other members of the LGBTQ + community, may provide social support in the face of parental rejection for identifying as SMM [31, 32]. Older members of a chosen family may act as mentors toward younger members, and all members may provide social support to one another [33]. There are also identity-specific subgroups within the LGBTQ + community that may provide additional social support to SMM who identify with that subgroup (e.g., house and ball community, drag, bear, leather, etc.) [33].
Previous studies have shown that increased social support has been associated with increased PrEP use in other populations [34]. The mechanism through which social support increases PrEP use and adherence may be through reducing stigma and increasing mutual learning in a social network [35,36,37]. However, methodological limitations have constrained the state of knowledge regarding the role of social support in fostering PrEP use among SMM. Further, inconsistent measurement of social support has limited our understanding of the underlying mechanisms or causal factors that serve to increase PrEP use. Varying assessments of social support among SMM have also limited our understanding of the impact that distinct types and sources of support received, as well as the perceived quality of that support, has on PrEP use among SMM. This research is needed to identify modifiable social support intervention targets for increasing PrEP use among SMM.
Given that SMM are disproportionately affected by HIV, it is crucial to fully elucidate factors such as social support that have been shown to strengthen engagement in PrEP use. To date, a scoping review has not been conducted to describe the various pathways and overall impact that social support has on PrEP use behaviors among SMM in the United States. The objective of this scoping review is to summarize the current literature base investigating the association between social support and PrEP use among SMM in the United States. Scoping reviews are appropriate for locating and summarizing literature on emerging topics and identifying gaps, such as how social support is associated with PrEP use [38,39,40].
Methods
Search Strategy
Following Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [41] guidelines, a systematic search was performed for studies investigating the association between constructs of the Social Support Theory and PrEP use and adherence among SMM in the US. The search for peer-reviewed articles was conducted on October 27, 2022, using six different databases: MEDLINE / PubMed, PsycINFO, Cochrane CENTRAL, Google Scholar, Embase, and Web of Science. The search was conducted using terms established by using keywords and medical subject headings (MeSH) terms before being adapted to each database (Table 1). Terms were established for SMM, PrEP, and social support terms. Within each category, the Boolean operator OR was used to expand the search, and then combined using the AND term for the three categories.
Inclusion Criteria and Selection Process
There were two phases of applying the selection criteria. Studies first had to meet the inclusion criteria during the title and abstract screening. The article must (1) not have a definitely irrelevant title, (2) be in English, (3) take place in the United States, (4) include sexual minority, cisgender, adult, HIV-negative men, (5) include PrEP use/adherence terms, and (6) include social support terms. Studies that progressed to the full-text screening criteria phase were included in the final analysis if they met the additional inclusion criteria that the full article must (1) be in English, (2) take place in the United States, (3) include sexual minority, cisgender, adult, HIV-negative men, (4) be a study (e.g., not a commentary, editorial, etc.), (5) measure PrEP use/adherence as an outcome, (6) assess social support as an exposure, and (7) assess the association between social support and PrEP use/adherence. There were no exclusions based on the date of publication. Three researchers (CN, HR, OJ) independently performed each extraction step before meeting and compared what studies they deemed appropriate to include. Any discrepancies were discussed and decided between the three researchers. Approval by the university’s Institutional Review Board (IRB) was not required.
Results
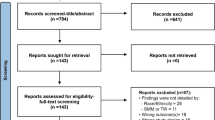
Our search yielded 419 articles (Fig. 1). After removing a total of 113 duplicates, 307 articles progressed to the first step of title and abstract screening. This first phase excluded 212 articles based on the title/abstract screening criteria, and one article was excluded as it was embargoed, leaving 94 articles to undergo full-text screening. Of these, 11 studies were included for data extraction in this scoping review [42,43,44,45,46,47,48,49,50,51,52].

PRISMA diagram [65] for systematic search
Description of Studies
Eleven articles were included in the data analysis: ten manuscripts and one conference abstract (Table 2). The study designs were diverse, with three qualitative interview studies [48, 50, 52], four cross-sectional studies [42,43,44, 47], two interventions [46, 49], and two randomized control trials [45, 51]. The studies took place in varied geographic locations across the US. Four took place in the mid-Atlantic region [42, 44, 47, 51]: one in Washington, DC [51] and three from the same study in the metropolitan areas of Philadelphia, PA, Baltimore, MD, and Washington, DC [42, 44, 47]. These three studies used different inclusion/exclusion criteria and thus had different datasets [42, 44, 47]. Three other studies took place in the Midwest [46, 48, 52]: two in Milwaukee, WI [46, 52], and one in both Milwaukee, WI and Cleveland, OH [48]. Additionally, two studies took place in Los Angeles, CA [45, 49], one took place in Jackson, MS [43], and one spanned several cities across different regions of the US, including Providence, RI, Jackson, MS, and St. Louis, MO [50]. Notably, all studies were centered in major metropolitan areas. Six articles included only Black or African-American men in their study [43, 45, 48] or had a high proportion of Black or African-American participants [46, 49, 51]. While the majority of studies included both SMM who were using PrEP and those who were not, two studies included only those who were actively taking PrEP [50, 52], and one intervention included only SMM who were not actively using PrEP [45]. A summary of all article measurements and findings is below (Table 3).
Qualitative Findings
Three qualitative interview studies in this review produced similar overarching thematic categories encompassing social factors that influence PrEP use. These include the perceived stigma that PrEP use equates to promiscuity, supportive and unsupportive healthcare providers, support from the LGBTQ + community or chosen families, and support from romantic relationships. These underscored the importance of both social support and social networks and their potential positive influence on PrEP knowledge, uptake, and adherence [48, 50, 52]. Specifically, discussions of PrEP within a social network positively contributed to the normalization of PrEP, thereby increasing self-efficacy to initiate PrEP use [48, 50]. Participants further highlighted that being an active member of their LGBTQ + community led to a reduction in PrEP-related stigma. Overall, discussing PrEP with other LGBTQ + men provided companionship, educational/informational support, and validation and therefore normalized PrEP use, leading participants to perceive the medication as a resource [48, 50, 52].
Inversely, participants in two studies who belonged to multiple marginalized groups (e.g., racial/ethnic minority and sexual minority) noted that discussing PrEP use within their social networks increased the level of stigma experienced around the use of PrEP and its perceived association with promiscuity, contributing to gossip and rumors that increased experiences of stigma and served as barriers to PrEP use [48, 52]. Some partnered participants also reported that initiating PrEP in the context of monogamous relationships may be seen as a sign of being unfaithful or unethically non-monogamous, both of which have the potential to elicit anger or judgment from their partner or the wider community [52]. A reported solution to this may be an increase in partnered peer mentors with experience taking PrEP [48].
Notably, a universally present theme for PrEP interventions focused on engaging a sexually affirming social network of healthcare providers [48, 50, 52]. Some participants were also of the belief that, if healthcare providers and personnel were better equipped to educate patients on the benefits and process of taking PrEP, the community would become less reliant on their social networks for the same information [52].
Observational Findings
Among the cross-sectional studies, there were inconsistent findings regarding the relationship between social support and PrEP use. Most of the studies found null or non-statistically significant results. One study investigated the association between social identity support and PrEP engagement among young SMM in Philadelphia, Baltimore, and Washington, DC through an online survey. The investigators measured social identity support by creating a latent variable from three constructs: gay community attachment, sexual orientation disclosure, and emotional support. Using structural equation modeling to assess the relationships between social identity support, PrEP norms, and economic instability, the investigators did not find a statistically significant direct association between social support and PrEP norms (β = 0.10, 95% CI: -0.12–0.32). However, there was a significant indirect association between social identity support and PrEP engagement mediated by descriptive PrEP norms (β = 0.18, 95% CI: 0.09–0.28) [42].
In another study, investigators assessed whether participants’ family social support and comfort with parent-sex communication were associated with PrEP uptake among young SMM. Family social support was from one question asking participants the extent to which they received social/emotional support from their family (0 not at all, 1 a little, 2 somewhat, 3 a lot). To measure comfort with parent-sex communication, participants rated the extent to which they felt comfortable about their sexual behaviors, sexual identity/attraction, sexual health, and taking PrEP with each of their parents respectively (0 not at all, 1 a little, 2 somewhat, 3 very). Although family social support was not significantly associated with current PrEP use, after adjusting for family dynamics and demographics, there was a significant association between comfort levels with communication about sex with parents and current PrEP use (aOR 1.87; 95% CI: 1.18–2.98; p = 0.008) [44].
A third analysis conducted in the same mid-Atlantic corridor among young men who have sex with men (YMSM) used structural equation modeling to test pathways between PrEP stereotypes, stigma, lifetime PrEP use, and gay community attachment. Gay community attachment was comprised of four questions about their area’s LGBTQ + community (e.g., “Participant in my area’s LGBTQ + community is a positive thing for me”). Higher gay community attachment was significantly and directly associated with lifetime PrEP use (β = 0.25, 95% CI: 0.11–0.40, p = 0.001). Gay community attachment was a measure developed by the authors comprised of variables related to feeling like part of the area’s LGBTQ + community, feeling like participating in said community was a positive experience, feeling a bond with the community, and feeling proud of the community [47].
Finally, the fourth and final cross-sectional study investigated factors associated with PrEP use among Black / African American SMM in Jackson, MS, including social support. This analysis was conducted at the individual level and the zip code level. Social support was measured using the four-item Emotional Support Scale [53]. After adjusting for covariates, the authors found that there were no statistically significant associations between social support and PrEP use at the individual level, (aOR 0.93, 95% CI: 0.81–1.07, p = 0.31). Similarly, there was no significant association between social support measured in a cluster mean at the zip code level (aOR 0.78, 95% CI 0.6–1.01, p = 0.06) [43].
Experimental Findings
The first intervention study investigated a social network intervention that enrolled five participants (i.e., seeds) who were Black, HIV-negative, men who had sex with men [46]. The seeds, in turn, recruited their network members (average: 8, range: 4–12). The social network intervention included five weekly group sessions and two biweekly booster sessions focused on inspiring or energizing network leaders to help their friends avoid HIV infection by learning about PrEP, practicing conversations about PrEP, normalizing PrEP, and developing plans to help their friends adopt PrEP. After the intervention was completed at three months, three of the 27 individuals in the intervention initiated PrEP use, increasing the prevalence of PrEP use from one (3%) to four total participants (12%) [49].
The second intervention study was a peer navigation study [49]. It was adapted from the CDC’s Antiretroviral Treatment Access Study (ARTAS) [54], which successfully linked HIV-positive participants to HIV care. The five-session intervention provided PrEP knowledge, assessing the participant for PrEP adherence, removing any barriers to adherence, and text messages aimed to increase adherence using Social Support Theory, Health Belief Model, and Social Cognitive Theory. 91.5% of SMM were successfully linked to PrEP care in a median number of nine (IQR 4–15) days. Of all participants, 69.6% reported that they were still taking PrEP. 83.3% of SMM reported that they did not miss one PrEP dose in the previous four days, and 48.7% reported that they did not miss one PrEP dose in the previous 30 days. About 20% of participants (MSM: 19.2%) reported that they did not take a PrEP dose on four or more consecutive days in the previous 30 days. Nearly half (46.5%) of MSM elected to receive the adherence support text messages; these MSM were more likely to report that they still took PrEP medication than participants who did not receive the text messages (85.7% vs. 61.4%; χ2(1) = 12.0, p < 0.001). The association between text message support and PrEP adherence was significant for MSM (81.1% vs. 59.3%; FET, p = 0.014) [49].
Finally, two randomized controlled trials met the inclusion criteria in this review. The first compared financial incentives against a social media support group and a control group among young SMM of color in Washington, DC [51]. Participants were randomized 1:1:1 to standard-of-care PrEP (control group), standard-of-care PrEP plus an invitation to a bidirectional Facebook support group supervised by two clinicians (social media group), or standard-of-care PrEP plus a $50 gift card at each of two follow-up visits (financial incentive group). Participant adherence to PrEP was measured using dried blood spot (DBS) tenofovir diphosphate levels. After six months, protective PrEP adherence (≥ 4 doses/week) was measured in 46% of the financial incentive group and 57% of the social media support group compared to 67% of the control group (p = 0.38). Both the financial and social media arms had no statistical impact on PrEP adherence compared to the control arm [51].
The second randomized controlled trial assessed the Passport to Wellness intervention, which was comprised of a customized wellness plan, financial incentives, social/educational group outings, and a peer mentor pairing who provided support, encouragement, and navigation [45]. Participants were randomized 1:1 into the Passport to Wellness intervention or to a version that did not include the peer mentor aspect. The peer mentor intervention arm had PrEP awareness and use increase from 0 to 22% compared to the control arm whose use increased from 0 to 9%. However, the results of the generalized linear mixed model were not statistically significant at α = 0.05; the odds of current usage of PrEP was 1.48 (95% CI: 0.31–7.00) as likely among peer-supported group compared to non-peer-supported group (p = 0.625) [45].
Discussion
The systematic search conducted in this scoping review resulted in 11 studies, demonstrating the scarcity of research on the association between social support and PrEP use among SMM. All studies were conducted in major metropolitan areas, with few taking place in the US Southeast region where rates of HIV are among the highest [2]. The findings were mixed on the association between social support and PrEP use and varied from null to positive associations; several studies had null findings [43, 45, 51], some showed that social support, in general, was directly [46, 48,49,50, 52] or indirectly [42] associated with increased PrEP use or adherence, and others showed that social support from specific members was associated with increased PrEP use [44, 47]. This inconsistency of findings suggests the need for more research on how the different forms and sources of social support may impact PrEP use among SMM.
The qualitative studies in this analysis suggested the substantial importance of social support for use, normalization, and destigmatization of PrEP. This aligns with previous studies that have shown that resistance to HIV-related care is rooted in HIV stigma and a fear of negative consequences from peers [55]. Normalizing HIV-treatment and -prevention services may help an individual feel more comfortable seeking or discussing HIV-related medications such as PrEP. Empowering those who are taking PrEP to disclose their use of PrEP, when safe to do so, and share their experiences with other members of their social networks could be one way of reducing stigma and increasing the acceptability of PrEP [34, 48, 56]. Previous studies have shown normalizing HIV care may act as a protective factor against the internalization of sex-negative attitudes and improve an individual’s health outcomes and self-care practices [57, 58].
The source providing social support to SMM may also make a difference; two studies described the importance of the gay community [47] and parent-child social support [44]. Receiving social support from another individual in one’s gay community may help to normalize PrEP if that individual has favorable views of PrEP or is taking PrEP themselves, which has been associated with higher PrEP adherence [9, 59]. A key strategy to normalize PrEP is to also do so in clinical settings through LGBTQ-affirming healthcare providers and using standardized approaches to PrEP provision and education [60]. Leveraging a peer-driven approach may be another strategy, as previous studies have shown that having a mentor or role model within one’s identifying community has been beneficial to PrEP use and adherence [61]. In general, further investigation into the specific sources of social support, whether it be from the gay community, parents, or healthcare providers, is warranted.
The experimental studies in this analysis provided social support in a variety of ways: a customized wellness plan intervention informed by Social Support Theory, a social network intervention, a peer navigator intervention, and a bidirectional Facebook group. While the experimental studies did not find any statistically significant associations, one important result that stood out was that individuals who received theory-based text message support were more likely to report taking PrEP medication than participants who did not receive the text messages [49]. Behavioral change interventions benefit greatly from theory, as theoretically informed interventions often lead to better outcomes than those that do not consult theory [62]. Further, this suggests that, given that the social support in this study was provided through text, an anonymous source of social support may be an important strategy to investigate to avoid stigma or judgment from individuals in someone’s social network.
The observational studies in this analysis suggest that the association between social support and PrEP use needs further investigation. While some studies showed a direct association [46, 48,49,50, 52], Bonett et al. showed an indirect association between social identity support and PrEP engagement through PrEP norms [42]. This suggests that social network members who show support for sexual minorities are likely to influence overall peer norms around PrEP and that positive attitudes about PrEP in networks impact SMM’s decisions to take PrEP. In some models, social support has been shown to serve as a moderator; the stress-buffering theory posits that supportive social interactions may provide resources promoting adaptive behavioral responses when faced with stress [63]. One study that aligns with this hypothesis found that more friend-based social support acted as a buffer to above-average minority-identity stress and resulted in little negative effect [64]. The mechanisms behind the relationship between social support and PrEP use warrant further study. Future interventions may benefit from taking a social network approach to further investigate the function and structure of specific individuals on PrEP use and adherence among SMM. Further, these results indicate that quantitative measures may not be adequately capturing the nuanced ways that social support may bolster PrEP use for some SMM. Studies in this review measure social support, which may not necessarily equate to social support for PrEP use, given the associated stigma. The development of a PrEP-specific support measurement may be warranted.
These studies explore whether support from one’s social network members is associated with active participation in the HIV-prevention continuum through PrEP use and adherence, a critical effort to strengthen prevention efforts among SMM. These findings suggest a need to further investigate the specific ways that supportive members of social networks can influence SMM towards or away from using PrEP. Members of networks may be viewed as highly supportive in some ways (e.g., instrumental support), but less supportive or even stigmatizing about sexuality and/or the use of PrEP. Further study is warranted to identify the best forms and sources of PrEP-specific support to inform future interventions. For example, future interventions may benefit from social support aimed at reducing the stigma associated with PrEP and HIV. Social support and related factors work together to impact PrEP use. Once the mechanism of social support is better understood, researchers can develop meaningful interpersonal / community-based interventions that leverage those mechanisms of social support that help increase PrEP use and adherence in efforts to increase HIV prevention.
Limitations
There were several limitations to this review. The scope of this review was limited to the US and cisgender sexual minority men, limiting its application to other populations. Given the high variance in social determinants of health for different geographic areas and transgender populations, different reviews should be done for these populations, as their experiences are very different from this population. The studies included in this review were all conducted in major metropolitan areas and primarily in the northern half of the country, which is a major gap. However, many studies did prioritize Black and African American participants, which is a disproportionately affected group that should be emphasized. Further, only one of the studies in this analysis measured PrEP using dried blood spot scores, while the rest were self-reported measures. More studies are needed where PrEP use and adherence are confirmed via biomarkers.
Conclusion
The findings of this review highlight the complexity of the relationship between social support and PrEP use among SMM. While some studies have demonstrated a significant positive impact of social support on PrEP uptake and adherence, others showed null results. This inconsistency underscores the need for further research to elucidate the specific types and sources of PrEP-specific social support that most effectively promote PrEP use. Understanding these nuances can inform targeted interventions aimed at increasing PrEP utilization among SMM, ultimately contributing to the reduction of HIV incidence in this population.
Mixed results suggest social support may be highly nuanced and subjective for SMM and that a one-size-fits-all approach is likely not an effective way for social support or social network-based interventions to increase PrEP use. Further study is needed to assess the forms, functions, and quality ratings of social support for PrEP use among SMM. Additional study of the pathways and mechanisms by which social support bolsters or hinders PrEP use is also needed. Some members of SMM’s social networks may have less favorable views or stigmatizing attitudes towards PrEP, which may influence SMM’s comfort on discussing PrEP with their network members. Inversely, some studies demonstrated that SMM may have network members that are taking PrEP or have favorable views toward PrEP, which may increase the likelihood of discussing the medication. Previous studies have shown that having even one social network member increases one’s willingness to take PrEP themselves [56]. Social support-based interventions that seek to reduce PrEP stigma and increase social norms around PrEP use may be particularly important to investigate. Further, couples-based interventions that seek to normalize and reframe narratives around the use of PrEP as one potential method of loving and protecting one another in the context of supportive relationships are another potential avenue to pursue.
The current review suggests there may be paradoxical findings around how social network members can both help and hinder PrEP use and that these nuances need to be studied further. Moreover, social support and social network-based interventions focused on increasing PrEP uptake among SMM are likely to be most efficacious if interventionists can help participants identify the specific form of social support that would be helpful, offered by whom deemed most appropriate, and under what circumstances.
References
(CDC). Centers for Disease Control and Prevention. Estimated HIV incidence and prevalence in the United States 2014–2018. Atlanta, GA, US; 2019.
(CDC) Centers for Disease Control and Prevention. HIV Surveillance Report. Atlanta, GA, US. 2019 May 2021.
Announcement. of FDA Approval for the use of Truvada for pre-exposure prophylaxis [press release]. New York State Department of Health2012.
Baeten Jared M, Donnell Deborah N, Patrick M, Nelly R, Campbell James D, Wangisi, Jonathan, et al. Antiretroviral prophylaxis for HIV prevention in heterosexual men and women. N Engl J Med. 2012;367(5):399–410.
Grant Robert M, Lama Javier R, Anderson Peter L, McMahan Vanessa, Liu Albert Y, Lorena V, et al. Preexposure Chemoprophylaxis for HIV prevention in men who have sex with men. N Engl J Med. 2010;363(27):2587–99.
Grant RM, Anderson PL, McMahan V, Liu A, Amico KR, Mehrotra M, et al. Uptake of pre-exposure prophylaxis, sexual practices, and HIV incidence in men and transgender women who have sex with men: a cohort study. Lancet Infect Dis. 2014;14(9):820–9.
McCormack S, Dunn David, editor. Pragmatic open-label randomised trial of preexposure prophylaxis: the PROUD study. Conference on retroviruses and opportunistic infections (CROI); 2015.
Catherine MJ-MC, Bruno S, Gilles P, Laurent C, Isabelle C, et al. On-demand preexposure prophylaxis in men at high risk for HIV-1 infection. N Engl J Med. 2015;373(23):2237–46.
Volk Jonathan E, Marcus Julia L, Phengrasamy Tony B, Derek ND, Phuong F, Stephen, Hare C, Bradley. No new HIV infections with increasing use of HIV preexposure prophylaxis in a clinical practice setting. Clin Infect Dis. 2015;61(10):1601–3.
Sullivan Patrick S, Mera GR, Farah M, Pembleton Elizabeth S, Guest Jodie L, Jones, Jeb, et al. Trends in the use of oral emtricitabine/tenofovir disoproxil fumarate for pre-exposure prophylaxis against HIV infection, United States, 2012–2017. Ann Epidemiol. 2018;28(12):833–40.
Smith Dawn K, Van Michelle H, Jeremy G. Estimates of adults with indications for HIV pre-exposure prophylaxis by jurisdiction, transmission risk group, and race/ethnicity, United States, 2015. Ann Epidemiol. 2018;28(12):850–7. e9.
Sullivan PS, Sanchez TH, Zlotorzynska M, Chandler CJ, Sineath RC, Kahle E, Tregear S. National trends in HIV pre-exposure prophylaxis awareness, willingness and use among United States men who have sex with men recruited online, 2013 through 2017. J Int AIDS Soc. 2020;23(3).
Eaton Lisa A, Driffin Daniel D, Bauermeister Jose S, Harlan, Conway-Washington Christopher. Minimal awareness and stalled uptake of pre-exposure prophylaxis (PrEP) among at risk, HIV-negative, black men who have sex with men. AIDS Patient Care STDs. 2015;29(8):423–9.
Khanna Aditya S, Michaels Stuart S, Britt M, Ethan G, Keith Y, Lindsay, et al. Preexposure prophylaxis awareness and use in a population-based sample of young black men who have sex with men. JAMA Intern Med. 2016;176(1):136–8.
Baeten Jared M, Haberer Jessica E, Liu Albert Y, Sista Nirupama. Preexposure prophylaxis for HIV prevention: where have we been and where are we going? JAIDS J Acquir Immune Defic Syndr. 2013;63:S122–9.
Tellalian David M, Khalid BU, Fritz, Hardy W, David. Pre-exposure prophylaxis (PrEP) for HIV infection: results of a survey of HIV healthcare providers evaluating their knowledge, attitudes, and prescribing practices. AIDS Patient Care STDs. 2013;27(10):553–9.
Krakower Douglas W, Norma M, Jennifer A, Maloney Kevin, Mayer Kenneth H. HIV providers’ perceived barriers and facilitators to implementing pre-exposure prophylaxis in care settings: a qualitative study. AIDS Behav. 2014;18:1712–21.
Krakower Douglas M, Kenneth H. Engaging healthcare providers to implement HIV pre-exposure prophylaxis. Curr Opin HIV AIDS. 2012;7(6):593–9.
Blumenthal Jill J, Sonia K, Douglas S, Xiaoying Y, Jason M, Kenneth, et al. Knowledge is power! Increased provider knowledge scores regarding pre-exposure prophylaxis (PrEP) are associated with higher rates of PrEP prescription and future intent to prescribe PrEP. AIDS Behav. 2015;19:802–10.
Lutete Priscila MDW, Sabounchi Nasim S, Paige Mark Q, Lounsbury David W, Noah R, et al. Intersectional stigma and Prevention among Gay, Bisexual, and same gender–loving men in New York City, 2020: System Dynamics models. Am J Public Health. 2022;112(S4):S444–51.
Calabrese Sarah K, Underhill K. How stigma surrounding the use of HIV preexposure prophylaxis undermines prevention and pleasure: a call to destigmatize truvada whores. Am J Public Health. 2015;105(10):1960–4.
Haire Bridget G. Preexposure prophylaxis-related stigma: strategies to improve uptake and adherence–a narrative review. HIV/AIDS-Research Palliat Care. 2015:241–9.
Rod K, Will S, Anna C. Complex and conflicting social norms: implications for implementation of future HIV pre-exposure prophylaxis (PrEP) interventions in Vancouver, Canada. PLoS ONE. 2016;11(1):e0146513.
Grace Daniel J, Jody MP, Paul S, Matthew JP, Tan Darrell HS. The pre-exposure prophylaxis-stigma paradox: learning from Canada’s first wave of PrEP users. AIDS Patient Care STDs. 2018;32(1):24–30.
Calabrese Sarah K. Understanding, contextualizing, and addressing PrEP stigma to enhance PrEP implementation. Curr HIV/AIDS Rep. 2020;17:579–88.
Dubov Alex G Jr, Phillip A, Frederick L, Fraenkel Liana. Stigma and shame experiences by MSM who take PrEP for HIV prevention: a qualitative study. Am J Men’s Health. 2018;12(6):1843–54.
Albrecht Terrance L, Adelman Mara B. Communicating social support: Sage Publications, Inc; 1987.
Cohen S, Wills TA. Stress, social support, and the buffering hypothesis. Psychol Bull. 1985;98(2):310–57.
Rice Eric W, Hailey. Wollin Heather. Social Support. In: Loue S, editor. Mental Health Practitioner’s guide to HIV/AIDS. New York, NY, US: Springer New York; 2013. pp. 385–8.
Waddell E, Needham, Messeri Peter A. Social Support, Disclosure, and Use of Antiretroviral Therapy. AIDS Behav. 2006;10(3):263–72.
Schneider David M. The power of culture: notes on some aspects of gay and lesbian kinship in America today. Cult Anthropol. 1997;12(2):270–4.
Weston Kath. Families we choose: lesbians, gays, kinship. New York, NY, US: Columbia University; 1997.
Zarwell M, Ransome Y, Barak N, Gruber D, Robinson WT. PrEP indicators, social capital and social group memberships among gay, bisexual and other men who have sex with men. Cult Health Sex. 2019;21(12):1349–66.
Felsher M, Dutra K, Monseur B, Roth AM, Latkin C, Falade-Nwulia O. The influence of PrEP-Related Stigma and Social Support on PrEP-Use Disclosure among women who inject drugs and Social Network members. AIDS Behav. 2021;25(12):3922–32.
Beals Kristin P, Anne PL, Gable Shelly L. Stigma management and well-being: the role of perceived social support, emotional processing, and suppression. Pers Soc Psychol Bull. 2009;35(7):867–79.
Kalichman Seth C, DiMarco M, James A, Webster L. DiFonzo Kari. Stress, social support, and HIV-status disclosure to family and friends among HIV-positive men and women. J Behav Med. 2003;26:315–32.
Garcia Jonathan, Colson Paul W, Parker Caroline, Hirsch Jennifer S. Passing the baton: community-based ethnography to design a randomized clinical trial on the effectiveness of oral pre-exposure prophylaxis for HIV prevention among black men who have sex with men. Contemp Clin Trials. 2015;45:244–51.
Armstrong Rebecca H, Belinda J, Doyle, Jodie. Waters Elizabeth. ‘Scoping the scope’of a cochrane review. J Public Health. 2011;33(1):147–50.
Munn Zachary P, Micah DJ, Cindy S, Catalin T. McArthur Alexa, Aromataris Edoardo. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med Res Methodol. 2018;18:1–7.
Arksey, Hilary. O’Malley Lisa. Scoping studies: towards a methodological framework. Int J Soc Res. 2005;8(1):19–32.
Moher David L, Alessandro T, Jennifer, Altman Douglas G, The Prisma Group. Preferred reporting items for systematic reviews and Meta-analyses: the PRISMA Statement. PLOS Med. 2009;6(7):e1000097.
Bonett S, Bauermeister J, Meanley S. Social identity support, descriptive norms, and economic instability in PrEP engagement for emerging adult MSM in the United States. AIDS Care.
Burns PA, Hall CDX, Poteat T, Mena LA, Wong FY. Living while Black, Gay, and poor: the Association of Race, Neighborhood Structural disadvantage, and PrEP utilization among a sample of Black men who have sex with men in the Deep South. AIDS Educ Prev. 2021;33(5):395–410.
Flores DD, Meanley SP, Wood SM, Bauermeister JA. Family characteristics in Sex Communication and Social Support: implications for emerging adult men who have sex with men’s PrEP Engagement. Arch Sex Behav. 2020;49(6):2145–53.
Harawa NT, Schrode KM, McWells C, Weiss RE, Hilliard CL, Bluthenthal RN. Small randomized controlled trial of the New Passport to Wellness HIV Prevention Intervention for Black Men Who have sex with men (BMSM). AIDS Educ Prev. 2020;32(4):311–24.
Kelly JA, Amirkhanian YA, Walsh JL, Brown KD, Quinn KG, Petroll AE, et al. Social network intervention to increase pre-exposure prophylaxis (PrEP) awareness, interest, and use among African American men who have sex with men. AIDS Care. 2020;32(sup2):40–6.
Meanley S, Connochie D, Choi SK, Bonett S, Flores DD, Bauermeister JA. Assessing the role of Gay Community attachment, Stigma, and PrEP stereotypes on Young men who have sex with men’s PrEP uptake. AIDS Behav. 2021;25(6):1761–76.
Quinn KG, Christenson E, Spector A, Amirkhanian Y, Kelly JA. The influence of peers on PrEP perceptions and use among Young Black Gay, Bisexual, and other men who have sex with men: a qualitative examination. Arch Sex Behav. 2020;49(6):2129–43.
Reback CJ, Clark KA, Rünger D, Fehrenbacher AE. A Promising PrEP Navigation intervention for Transgender women and men who have sex with men experiencing multiple Syndemic Health disparities. J Community Health. 2019;44(6):1193–203.
Rogers BG, Sosnowy C, Zanowick-Marr A, Chan PA, Mena LA, Patel RR et al. Facilitators for retaining men who have sex with men in pre-exposure prophylaxis care in real world clinic settings within the United States. BMC Infect Dis. 2022;22(1).
Ware C, Sparks A, Levy M, Wolf H, Siegel M. Null effect of financial incentives or social media support on PrEP adherence in a randomized controlled trial of young men who have sex with men of colour. J Int AIDS Soc. 2021;24(SUPPL 1):131.
Zapata JP, Petroll A, de St Aubin E, Quinn K. Perspectives on Social Support and Stigma in PrEP-related care among gay and bisexual men: a qualitative investigation. J Homosex. 2022;69(2):254–76.
Krause Neal. Negative interaction and satisfaction with social support among older adults. Journals Gerontology: Ser B: Psychol Sci Social Sci. 1995;50(2):P59–73.
Gardner Lytt I, Metsch Lisa R, Anderson-Mahoney Pamela, Loughlin Anita M, Del Carlos R, Steffanie S, et al. Efficacy of a brief case management intervention to link recently diagnosed HIV-infected persons to care. Aids. 2005;19(4):423–31.
Turan B, Crockett KB, Buyukcan-Tetik A, Kempf MC, Konkle-Parker D, Wilson TE, et al. Buffering internalization of HIV Stigma: implications for treatment adherence and depression. J Acquir Immune Defic Syndr. 2019;80(3):284–91.
Storholm ED, Klein DJ, Pedersen ER, D’Amico EJ, Rodriguez A, Garvey R, Tucker JS. Sociodemographic and behavioral risk correlates of PrEP interest and use among young adults experiencing homelessness in Los Angeles. AIDS Behav. 2024;28(4):1216–26.
Martin H, Toby L, Brandon B, Dale H, Jeanne E, Dean M, et al. Trends in attitudes to and the Use of HIV Pre-exposure Prophylaxis by Australian Gay and Bisexual men, 2011–2017: implications for further implementation from a diffusion of innovations Perspective. AIDS Behav. 2019;23(7):1939–50.
Lin F, Deng-Min C. Al-Raes Maria. Social support, mental health needs, and HIV risk behaviors: a gender-specific, correlation study. BMC Public Health. 2019;19(1):651.
Flash C, Landovitz R, Giler RM, Ng L, Magnuson D, Wooley SB, Rawlings K. Two years of Truvada for pre-exposure prophylaxis utilization in the US. J Int AIDS Soc. 2014;17(4 Suppl 3):19730.
Calabrese SK, Earnshaw VA, Underhill K, Hansen NB, Dovidio JF. The impact of patient race on clinical decisions related to prescribing HIV pre-exposure prophylaxis (PrEP): assumptions about sexual risk compensation and implications for access. AIDS Behav. 2014;18(2):226–40.
Kaufman MR, Casella A, Wiginton JM, Xu W, DuBois DL, Arrington-Sanders R, et al. Mentoring Young African American men and Transgender women who have sex with men on sexual health: Formative Research for an HIV Mobile Health intervention for mentors. JMIR Form Res. 2020;4(12):e17317.
Susan M. Prestwich Andrew. Are interventions theory-based? Development of a theory coding scheme. Health Psychology: Official J Div Health Psychol Am Psychol Association. 2010;29(1):1.
Brian L, Sheldon C. Social support theory and measurement. Social support measurement and intervention: a guide for health and social scientists. New York, NY, US: Oxford University Press; 2000. pp. 29–52.
Fingerhut AW. The role of Social Support and Gay Identity in the stress processes of a sample of caucasian gay men. Psychol Sex Orientat Gend Divers. 2018;5(3):294–302.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71.
Acknowledgements
Ms. Nacht, Mr. Jessup, Ms. Reynolds, and Ms. Amato are employed through funding by grant #R01MH126762 (PI: Storholm) from the National Institute of Mental Health. Ms. Nacht is also funded through a T32 hosted at University of California – San Diego, funded by the National Institute on Drug Abuse #T32DA023356 (co-PIs: Steffanie A. Strathdee, Natasha K. Martin). The authors have no further acknowledgements to disclose.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Authorship Contribution
Carrie L. Nacht, MPH: conceptualization, methodology, validation, formal analysis, investigation, writing – original draft, visualization, project administration, Owen Jessup: Formal analysis, investigation, writing – original draft, writing – review & editing. Hannah E. Reynolds: Formal analysis, investigation, writing – original draft, writing – review & editing. Marianna Amato, MS: Writing – original draft, writing – review & editing. Erik D. Storholm, PhD: supervision, funding acquisition.
Disclaimer
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Conflict of interest
The authors have no conflicts of interest to disclose.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Nacht, C.L., Reynolds, H.E., Jessup, O. et al. The Association between Social Support and Pre-Exposure Prophylaxis use among Sexual Minority Men in the United States: A Scoping Literature Review. AIDS Behav (2024). https://doi.org/10.1007/s10461-024-04446-4
Accepted:
Published:
DOI: https://doi.org/10.1007/s10461-024-04446-4