
Abstract
Introduction In the past few decades, mental health problems have increasingly contributed to sickness absence and long-term disability. However, little is known about prognostic factors of return to work (RTW) and disability of persons already on sick leave due to mental health problems. Understanding these factors may help to develop effective prevention and intervention strategies to shorten the duration of disability and facilitate RTW. Method We reviewed systematically current scientific evidence about prognostic factors for mental health related long term disability, RTW and symptom recovery. Searching PubMed, PsycINFO, Embase, Cinahl and Business Source Premier, we selected articles with a publication date from January 1990 to March 2009, describing longitudinal cohort studies with a follow-up period of at least 1 year. Participants were persons on sick leave or receiving disability benefit at baseline. We assessed the methodological quality of included studies using an established criteria list. Consistent findings in at least two high quality studies were defined as strong evidence and positive findings in one high quality study were defined as limited evidence. Results Out of 796 studies, we included seven articles, all of high methodological quality describing a range of prognostic factors, according to the ICF-model categorized as health-related, personal and external factors. We found strong evidence that older age (>50 years) is associated with continuing disability and longer time to RTW. There is limited evidence for the association of other personal factors (gender, education, history of previous sickness absence, negative recovery expectation, socio-economic status), health related (stress-related and shoulder/back pain, depression/anxiety disorder) and external i.e., job-related factors (unemployment, quality and continuity of occupational care, supervisor behavior) with disability and RTW. We found limited evidence for the association of personal/external factors (education, sole breadwinner, partial/full RTW, changing work tasks) with symptom recovery. Conclusion This systematic review identifies a number of prognostic factors, some more or less consistent with findings in related literature (mental health factors, age, history of previous sickness absence, negative recovery expectation, socio-economic status, unemployment, quality and continuity of occupational care), while other prognostic factors (gender, level of education, sole breadwinner, supervisor support) conflict with existing evidence. There is still great need for research on modifiable prognostic factors of continuing disability and RTW among benefit claimants with mental health problems. Recommendations are made as to directions and methodological quality of further research, i.e., prognostic cohort studies.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Results from psychiatric epidemiologic surveys in Europe and in the USA have shown that mood, anxiety and substance use disorders are highly prevalent in the general population, in primary care settings and among workers [1–3]. In the population of industrialized western countries, lifetime prevalence of any mental disorder range from 37.5 to 48.6, and 12-month prevalence from 19.9 to 29.1 [4].
In the past few decades, mental health problems have increasingly contributed to sickness absence and long-term disability [5, 6]. The Organization for Economic Co-operation and Development (OECD) reports in a recent paper that mental health problems now account for one-third of all new disability benefit claims on average, rising to as high as 40–50% in some member states [7]. In that paper the OECD shows that in the past 10–15 years, the inflow into disability benefits due to mental health conditions has almost doubled in some countries. In the Netherlands in the late 1960s, mental disorders accounted for 11% of all sickness absence with a duration longer than 1 year. From then on up to the present, this percentage has risen to 30% [8, 9].
Besides huge economic costs at population level [7, 10], long term disability in general and due to mental health conditions in particular, is associated at the individual level with lower socio-economic status, reduced quality of life and higher morbidity/mortality rates [11]. It is therefore of great importance to prevent the transition of short term sickness absence into long term or permanent disability and to rehabilitate those persons already on long term disability benefit by facilitating return to work (RTW).
It is widely recognized that causes of sickness absence and disability are multifactorial and not associated with medical conditions alone [12, 13]. Systematic reviews on this topic primarily focused on musculoskeletal and pain-related health conditions [14, 15].
However, research on prognosis of long term disability due to mental disorders is scarce. Blank et al. [16] conducted a systematic review in 2008 of all papers relating to RTW or risk of job loss resulting from long term absence due to mental illness. They found 14 articles of varying methodological quality identifying a range of factors restricting RTW, related to work, family history, health risk behaviours, social status and medical condition. In that review, all study types were included and studies dealing with absences for more than 6 months were excluded.
In the Dutch social security system, disability benefit assessment takes place after a period of 2 years of sickness absence [17]. At that moment mental disorders account for 30% of all disability claims [9]. Factors associated with sustained disability and RTW of Dutch benefit claimants after this 2 year period are not known. Evidence based knowledge about prognostic factors of long term disability and RTW of persons already on sick leave lasting longer than 6 months due to poor mental health is missing. Understanding these factors, and in particular those which are amenable to change through any intervention program, may help to develop effective prevention and interventions to facilitate RTW for long-term disabled persons. To our knowledge, the literature on long term disability and RTW due to poor mental health has not yet been reviewed systematically, including longitudinal study types only and irrespective of the duration of preceding sickness absence.
Objectives
The aim of this review is to investigate systematically current scientific evidence about the prognostic factors for long term disability and RTW of persons sick listed due to mental health problems, and factors for recovery of mental health symptoms.
Methods
The first (LRC) and second reviewer (SB) discussed search strategy, criteria for selecting studies, quality assessment and data extraction to reach consensus. In case of disagreement the third reviewer (JvdK) made the final decision.
Search Strategy
The first author and an experienced medical librarian performed an extensive search in biomedical, psychological and economic databases (PubMed, PsycINFO, Embase, Cinahl, Business Source Premier) to find relevant articles, using MeSH terms, subheadings and free text words, see Table 1. The search was limited to articles with a publication date from January 1990 to March 2009. Additionally, we searched for other relevant articles using the name of the first author and the reference lists of included articles.
Titles and abstracts were screened independently by two reviewers (LRC, SB). Full papers were retrieved if the abstract provided insufficient data to enable selection. Only papers written in English, German, French and Dutch were considered for inclusion in this review.
Criteria for Selecting Studies
To reach overall agreement (LRC, SB) on in- and exclusion criteria, we pilot-tested preliminary criteria in 20 full text articles randomly selected from the initial search. To also include retrospective cohort studies as type of study, we omitted from the preliminary list the term prognostic. We added the term symptom recovery as type of outcome measure. The final in- and exclusion criteria are presented in Box 1.
Assessment of Methodological Quality
We based the quality assessment of the selected studies on an established criteria list for assessing validity of prognostic studies, as recommended by Altman [18]. This list consists of 16 items, each having yes/no/don’t know answer options. Scholten-Peeters et al. [19] operationalized this criteria list for use in a systematic review on prognostic factors of whiplash. With permission of the author, we pilot tested this operationalization on agreement in an assessment of three studies on prognostic factors of whiplash and modified the list for use in the present review. This modified criteria list is presented in Appendix Table 8.
The quality of all included articles was scored independently by two reviewers (LRC, SB). If sufficient information was available, the item was rated one point. When information was not given or the information given was unclear, the item was rated zero point. For the total quality score we added all points for each study (maximum score 16 points).
Studies with a minimum score of 11 points (≥70%) were arbitrarily considered to be of high quality and those with a score lower then 11 points (<70%) of low quality. We calculated initial interobserver agreement on methodological quality using kappa statistics for dichotomous values.
Data Extraction
Using a standardized form, the first reviewer (LRC) extracted data on study design, source population, inclusion and exclusion criteria, numbers of participants, length of follow-up, loss to follow-up, outcome, prognostic factors and statistical analysis.
Levels of Evidence
Based on Sackett et al. [20] and similar to the approach used by other systematic reviews [21], we defined four levels of evidence to determine the strength of association of prognostic factors with outcome: strong, moderate, limited and inconclusive evidence, see Table 2. Non-significant effects cannot contribute to consistency. Findings of one high quality study opposing consistent findings in one or more low quality studies would result in a situation of inconclusive evidence.
Results
Selection of Studies
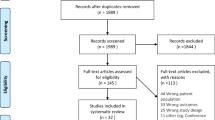
The initial search yielded 796 articles (search date: March 9th 2009). After selecting 36 references for full text reading, both reviewers (LRC, SB) agreed to include four articles for the present review. Searching the reference lists of those included articles, we found and included one additional article. Based on the name of the first author of the four included articles, we found two other relevant articles. In total we included seven articles for the present review [22–28]. Table 3 shows a flow chart of study selection.
Methodological Quality Scores
The final overall agreement between the two reviewers (LRC, SB) on quality score was κ = 0.84, which is considered to be very high. Disagreement originated mainly from reading errors and misinterpretation of the criteria list and was readily resolved in a consensus meeting. The methodological quality of all included studies is summarized in Table 4.
All studies were of high quality with sum scores ranging from 13 to 16 points. Across studies, the maximum score of each item was 7 points. The following items had <7 points: no inception cohort (item A, 5 points), no information of completers versus loss to follow-up (item F, 5 points), no (or insufficient) description of treatment used in the study population (item H, 3 points) and clinically relevant outcome measures (item L, 6 points).
Study Characteristics
The characteristics of each study as to quality score, design, recruitment, source population, case definition, response, numbers enrolled, measurements, follow-up, and loss to follow-up are presented in Table 5. Registry data were used in four studies [23, 24, 26, 28]. Only two studies linked registry data to data collected separately by other measurements, e.g., interview or questionnaire [24, 26]. Duration of sickness absence at baseline varied from 2 to 35 days (24) to ≥90 days [28].
Table 6 summarizes the study characteristics as to outcomes, prognostic factors and results. Only significant associations and prognostic factors are mentioned. The included studies used two types of outcome measures as dependent variables: disability (including RTW) and symptom recovery. Over 60 different types of prognostic factors were investigated (e.g., gender, age, socio-economic status, diagnosis, beliefs, occupational care, job- and employer-related factors). Statistical pooling of data in a meta-analysis was not possible due to the heterogeneity of study population, type of prognostic factors, outcome measures and study quality.
Evidence Synthesis
In Table 7 we present a qualitative summary of the evidence for all prognostic factors and their associations with disability duration and symptom recovery as outcome variables. In accordance with the International Classification of Functioning, Disability and Health (ICF-model), the prognostic factors are categorized as health-related factors, personal factors and external factors [29]. Only factors that are significantly associated with an increase or decrease of outcomes are mentioned. Table 7 also includes the modifiability of separate factors.
We found strong evidence that older age (>50 years) is associated with continuing disability and longer time to RTW for persons who are sick listed at baseline due to mental health problems. There is limited evidence for the association of health related factors (stress-related and shoulder/back pain, depression/anxiety disorder) with a longer duration of disability. We also found limited evidence that personal factors other than age (male gender, education, previous sickness absence, own expectation of duration of the absence >3 months, low socio-economic status) are related to continuing disability. We found limited evidence that full or partial RTW and changing work tasks is associated with symptom recovery. Furthermore, we found limited evidence for the association of external factors (unemployment, poor quality of interventions by the occupational physician aimed at the organization, poor continuity of occupational care, supervisor consulting with professional) with an increase of disability. There is limited evidence for the association of supervisor communication with the employee with a decrease of disability. There is limited evidence for the association of lower education and the position of sole breadwinner with an increase of poor mental health on a symptom level.
Discussion
In this systematic review we identified a total of 17 significant factors: 13 factors associated with disability/RTW, and 4 factors associated with symptom recovery, see Table 7. Of the 13 factors related to disability/RTW, only two factors were directly related to mental health, while the other 11 factors were of a personal or external nature in terms of the ICF-model. This seems to confirm the hypothesis that long term disability is for a large part related to non-medical conditions.
Health Factors
We found limited evidence for the association of stress-related and shoulder/back pain, and depression/anxiety disorder with a longer duration of disability. There is also limited evidence among non-depressed workers that better communication between supervisor and employee shortened time to full RTW. Disability and RTW outcomes may be influenced by a specific health factor, i.e., the prevalence of depressive symptoms. These findings are in line with the results of other research on disorder-related predictors of disability [30–33]. However, in general, in most studies addressing the relation between mental health and disability, mental health problems are poorly defined or use different diagnostic criteria and associations are not diagnosis-specific [6, 16]. Research data show an existing association between specific mental disorders and duration of disability, but nature and direction of this association remains to some extent unclear. It could be that multiple moderating or mediating factors are involved with effect-sizes depending on the severity of the disorder. It seems plausible that less severe mental disorders, such as dysthymia, adjustment disorder or simple phobia, are more susceptible to moderators than more severe disorders, such as major depressive disorder, bipolar disorder or psychotic disorders.
Personal Factors
We found strong evidence that older age (>50 years) is associated with continuing disability and longer time to RTW. This finding corresponds with the results of other systematic reviews [34]. In many western industrialized countries the age of the work force increases, due to demographic developments and government policies. As a result of this ageing process, occupational and insurance physicians and labor experts will encounter an increasing number of older workers unable or having increasing difficulties to perform their work tasks. Older workers and disability claimants are at a higher risk for continuing or even permanent disability and for a longer time to RTW. As age is not modifiable, the attention of professionals in occupational and insurance health care should be directed at other factors that are amenable to change, especially when dealing with older workers.
We found limited evidence for the association of gender with duration of disability and RTW. One included study found that in the third year of follow-up, men are 50–60% more likely to be in a healthy state than women, indicating a shorter duration of long term disability for men [23]. This finding is contrary to other research [35]. In four studies that we included in the present review, no significant effect of gender on disability and RTW outcome was found, whether analyzed as a potential confounder [24–26], or as an independent variable [28], and in one study the effect of gender on outcome was not investigated [27]. One included study found a non-significant effect of gender on the course of depressive symptoms [22]. These opposing results as to the effects of gender differences on duration of disability and time to RTW due to mental health problems are illustrative for the literature on this topic in general [6, 36].
One included study found, unexpectantly, that a high level of education predicted a longer time to RTW [27]. To our knowledge, there are no other studies to corroborate this. Another included study reported that a lower education increased the risk of depressive complaints, attributing to a longer time to RTW [22]. This is more in line with the literature on this subject [13, 16].
We found limited evidence that being the sole breadwinner increased the risk of prolonged depressive symptoms and contributed to a delayed RTW and disability [22]. However, in a Dutch study being the sole breadwinner significantly predicted RTW after long-term sick leave due to low back pain [37].
There is limited evidence that history of previous sickness absence is related to duration of disability and time to RTW. This is not surprising, since past sickness absence may be related to chronic health problems. This finding is in accordance with other research on this topic [38, 39].
There is limited evidence that absentees own expectation of disability duration >3 months is associated with longer time to RTW. This finding corresponds with the results of other studies [40]. In studies investigating the association of own expectation with health outcomes, Bandura’s concept of self-efficacy was most commonly accepted as underlying theoretical model [41].
We found limited evidence that low socioeconomic status predicted disability pension [28]. Indeed, many studies have documented the inverse relation between social class and morbidity, mortality, sickness absence and disability [42, 43].
External Factors
We found limited evidence that full or partial RTW and changing work tasks is associated with recovery of depressive symptoms. However, a Cochrane systematic review found little evidence that RTW i.e., supported employment improved symptoms, quality of life or social functioning [44].
One of the studies included in the present review found that the unemployed are less likely to be in a healthy state compared with the employed, indicating lower probabilities of RTW after long-term stress-related sickness absence [23]. This is in line with other studies [13, 16, 38]. However, due to few number of studies, little is known about underlying causes [45].
In the present review, we found limited evidence for the association of quality of occupational guideline-based care with disability and RTW. This is corroborated by results of other studies [46–48]. However, in a recent Cochrane review it was found impossible to investigate the effectiveness of workplace interventions among workers with mental health problems and other health conditions due to lack of studies [49].
We found limited evidence that continuity of occupational care shortens the duration of sickness absence of patients with adjustment disorder. Although the criteria for optimal performance in continuity of care differed as to frequency of contacts and number of different physicians, this finding is consistent with other studies on the relation of quality of care and outcome in patients with low back pain and in cancer survivors [50, 51]. To our knowledge, there are no other studies investigating this relation in sick listed workers with mental health problems.
We found limited evidence that frequent supervisory communication with workers with mental health problems decreased duration of disability. Sick listed workers may perceive good communication with their supervisor as social support. This finding corresponds with the insight that workplace support play an important role in disability management and enhances RTW [52, 53]. However, in one of the studies that we included for this review, it was found that this effect of support is beneficial in persons with low depression scores only [25]. Depressed workers may benefit less from communication with their supervisor. This is in line with the results of a recent study showing that more perceived social support is actually a barrier to RTW [54]. This is suggestive for a moderating effect of social support on the effects of mental health factors on RTW.
We found limited evidence that supervisor consulting with other professionals is more often associated with a longer duration of sickness absence. It is plausible that this relation is confounded by the severity of depressive symptoms: supervisors may consult occupational physicians more often if a problematic future RTW is foreseen in workers with more depressive symptoms, resulting in a later RTW.
Methodological Considerations
From a total of 796 articles, we only could find seven articles that fulfilled all our inclusion criteria. Moreover, four articles described results from the same cohort. Observational studies with non-significant results are less likely to be published [55]. Therefore, the few number of studies found for the present review could have resulted from publication bias. Also, the possibility that relevant articles remained undiscovered in databases that are difficult to locate cannot be excluded. Nevertheless, we believe that the small number of studies found was mainly the result of the strict definition of our inclusion criteria.
Our search strategy was to conduct a broad search using the search terms stated in Table 1, combined with specific criteria for in- and exclusion as to types of studies, participants and outcome measures, stated in Box 1. We did not include terms for minor mental health problems since we were interested in more severe mental disorders only and their association with long term disability. These major mental disorders, such as depressive disorder, anxiety disorder and adjustment disorder, are covered by the MeSH term Mental Disorders. We formulated strict in- and exclusion criteria: we selected studies among persons already receiving disability benefit at baseline only. Furthermore, in order to include all durations, we decided not to use the duration of sick leave or disability as an in- or exclusion criterion. By doing so, we prevented our search being biased by the fact that in research on disability the term long-term disability is not uniformly defined. We were interested in RTW as outcome. In general, studies on RTW focus on short term disability, while the interest of the present review lies primarily with long term disability. Therefore, we did not include RTW as a search term, but instead used it as an inclusion criterion.
To assess prognostic factors in a reliable way, prognostic studies need well defined inception cohorts of participants all at the same stage of their medical condition. Of the seven included studies, two studies did not use such an inception cohort, i.e., the duration of preceding sickness absence varied at baseline. This could have biased the assessment of prognostic factors. In four studies, treatment was not fully described or standardized. In these studies, unknown treatment could have confounded the assessment of prognostic factors. In two studies little or no information was presented of completers versus loss to follow-up. This also could have caused a biased assessment of prognostic factors. In the studies we included for this review, both the duration of disability at baseline and the time of follow-up varied. A relatively short follow-up time of 1 year was used in five studies. It cannot be excluded that effects of the prognostic factors found in these studies change over time, or that new factors arise, after the follow-up period ended.
To enhance the quality of future cohort studies on long term disability, we recommend (1) the use of an inception cohort at baseline; (2) to describe or standardize treatment or at least analyze the confounding effect on the prognostic factors studied; (3) a cohort large enough to allow diagnose-specific subgroup-analyses.
Conclusion
Factors that cannot be modified by any intervention program are useful in predicting disability/RTW outcome and identifying persons, groups or places at risk, but only modifiable factors can provide a sound basis for interventions. We identified four non-modifiable risk factors (older age, male gender, medium/higher education, history of previous sickness absence). We considered 13 factors to be amenable to change: two health related factors (stress-related and shoulder/back pain, depression/anxiety disorder), five personal factors (lower education, sole breadwinner, partial/full RTW, absentees own expectation of duration >3 months, socioeconomic status) and six external factors, all job-related (changing work tasks, unemployment, deviant occupational interventions aimed at organization, deviant continuity of occupational care, supervisor communication with employee, supervisor consulting with professional).
Some results of this systematic review are more or less consistent with findings in other studies, i.e., mental health factors [30–33], age [16, 34], history of previous sickness absence [38, 39], negative recovery expectation [40], socio-economic status [42, 43], unemployment [13, 16, 38], quality and continuity of occupational care [46–48, 50, 51], while other oppose existing evidence i.e., gender [6, 35, 36], level of education [13, 16], sole breadwinner [37], supervisor support [54].
Nature and severity of specific mental disorders remain strong predictors of disability and RTW due to poor mental health. Therefore, monitoring, assessing and contributing to optimize medical treatment is an important tool for occupational and insurance physicians to reduce duration of sickness absence and to prevent permanent disability.
There is consistent evidence that older age is significantly associated with the risk of continued disability. Confronted with an ageing work force, occupational health care should be targeted at prevention of long-term sickness absence among older workers at risk for continuing disability due to mental health problems. Interventions aimed at RTW of older absentees should be based on modifiable factors and effectuated without unnecessary delay. Such interventions should not a priori be omitted because of undue pessimism about chances based on age alone. Since older age is so clearly an important prognostic factor of continuing disability, policies at governmental and employer level should be directed at effective strategies to prevent sickness absences among older workers. To the benefit of workers already on sick leave, future research could be aimed at the development of age-specific interventions.
The finding that past sickness absence is related to duration of future disability and time to RTW is confirmed by related literature [38, 39]. Optimal managing of frequent short term sickness absence prevents long term disability.
Negative recovery expectations predict a longer time to RTW. Occupational care can help turning negative into positive expectancies by a cognitive-behavioral approach. The effectiveness of such interventions remain to be investigated.
In epidemiologic research, socio-economic status is often measured including level of education and unemployment. There is ample evidence in the literature that lower socio-economic status is a high risk factor of long term disability [28, 42, 43]. However, the role of education level in the disability process of persons suffering from poor mental health needs further clarifying.
The evidence found in the present review and related literature suggest that good quality and continuity of occupational guideline-based care is associated with a shorter duration of disability and time to RTW.
The gender-effect on disability and RTW remains unclear. More studies are needed to clarify mechanisms underlying the effect of gender on duration of long term disability and RTW. With the ICF-model as a guideline, future research can identify personal, job- and health-related factors that moderate and mediate the gender-effect.
It is hypothesized that being the sole breadwinner is a financial incentive to RTW, but whether or not employees with a bigger financial need return more often back to work, irrespective of their health, remains unclear.
Social support in the work place in general has a beneficial effect on RTW, but may be an unexpected barrier for persons in poor mental health. This warrants further research.
To conclude, there is still great need for high quality cohort studies to find relevant prognostic factors of long term disability among benefit claimants with mental health problems who are sick listed at baseline. Understanding these factors, and in particular those which are amenable to change through any intervention program, may help to develop effective prevention and intervention strategies to shorten the duration of disability and facilitate RTW.
References
Kessler RC, Chiu WT, Demler O, Merikangas KR, Walters EE. Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62(6):617–27.
Kessler RC. The global burden of anxiety and mood disorders: putting the European Study of the Epidemiology of Mental Disorders (ESEMeD) findings into perspective. J Clin Psychiatry. 2007;68(Suppl 2):10–9.
Bijl RV, Ravelli A, van ZG. Prevalence of psychiatric disorder in the general population: results of The Netherlands Mental Health Survey and Incidence Study (NEMESIS). Soc Psychiatry Psychiatr Epidemiol. 1998;33(12):587–95.
Cross-national comparisons of the prevalences and correlates of mental disorders. In: WHO International Consortium in Psychiatric Epidemiology. Bull World Health Organ. 2000;78(4):413–26.
Stansfeld S, Feeney A, Head J, Canner R, North F, Marmot M. Sickness absence for psychiatric illness: the Whitehall II Study. Soc Sci Med. 1995;40(2):189–97.
Hensing G, Wahlstrom R. Swedish Council on Technology Assessment in Health Care (SBU). Chapter 7. Sickness absence and psychiatric disorders. Scand J Public Health Suppl. 2004;63:152–80.
OECD. Sickness, disability and work: keeping on track in the economic downturn—background paper. 2009. http://www.oecd.org/dataoecd/42/15/42699911.pdf.
Klerk de JM, van der Zouwe N. Mental disorders and the WAO, 10 years later (in Dutch: Psychische stoornissen en de WAO, tien jaar later). Tijdschrift voor Bedrijfs en Verzekeringsgeneeskunde. 1993;5:162–7.
Knowledge Center UWV Quarterly Report 2007—III (in Dutch: Kenniscentrum UWV Kwartaalverkenning 2007—III). 2007. http://www.uwv.nl/Images/UKV%202007-III_tcm26-147000.pdf.
Smit F, Cuijpers P, Oostenbrink J, Batelaan N, de Beekman GRA. Costs of nine common mental disorders: implications for curative and preventive psychiatry. J Ment Health Policy Econ. 2006;9(4):193–200.
Alonso J, Angermeyer MC, Bernert S, Bruffaerts R, Brugha TS, Bryson H, et al. Disability and quality of life impact of mental disorders in Europe: results from the European Study of the Epidemiology of Mental Disorders (ESEMeD) project. Acta Psychiatr Scand Suppl. 2004;109(420):38–46.
Beemsterboer W, Stewart R, Groothoff J, Nijhuis F. A literature review on sick leave determinants (1984–2004). Int J Occup Med Environ Health. 2009;22(2):169–79.
Krause N, Frank JW, Dasinger LK, Sullivan TJ, Sinclair SJ. Determinants of duration of disability and return-to-work after work-related injury and illness: challenges for future research. Am J Ind Med. 2001;40(4):464–84.
Franche RL, Cullen K, Clarke J, Irvin E, Sinclair S, Frank J. Workplace-based return-to-work interventions: a systematic review of the quantitative literature. J Occup Rehabil. 2005;15(4):607–31.
MacEachen E, Clarke J, Franche RL, Irvin E. Systematic review of the qualitative literature on return to work after injury. Scand J Work Environ Health. 2006;32(4):257–69.
Blank L, Peters J, Pickvance S, Wilford J, Macdonald E. A systematic review of the factors which predict return to work for people suffering episodes of poor mental health. J Occup Rehabil. 2008;18(1):27–34.
de Boer WEL, Besseling JJM, Willems JHBM. Organisation of disability evaluation in 15 countries. Prat Organ Soins. 2007;38(3):205–17.
Altman DG. Systematic reviews of evaluations of prognostic variables. BMJ. 2001;323(7306):224–8.
Scholten-Peeters GG, Verhagen AP, Bekkering GE, van der Windt DA, Barnsley L, Oostendorp RA, et al. Prognostic factors of whiplash-associated disorders: a systematic review of prospective cohort studies. Pain. 2003;104(1–2):303–22.
Sackett DL, Straus SE, Richardson WS. Evidence-based medicine. How to practice and teach EBM. Guidelines. Edinburgh: Churchill Livingstone; 2000.
Willemse-van Son AH, Ribbers GM, Verhagen AP, Stam HJ. Prognostic factors of long-term functioning and productivity after traumatic brain injury: a systematic review of prospective cohort studies. Clin Rehabil. 2007;21(11):1024–37.
Brenninkmeijer V, Houtman I, Blonk R. Depressed and absent from work: predicting prolonged depressive symptomatology among employees. Occup Med (Lond). 2008;58(4):295–301.
Engström L, Janson S. Stress-related sickness absence and return to labour market in Sweden. Disabil Rehabil. 2007;29(5):411–6.
Nieuwenhuijsen K, Verbeek JH, Siemerink JC, Tummers-Nijsen D. Quality of rehabilitation among workers with adjustment disorders according to practice guidelines; a retrospective cohort study. Occup Environ Med. 2003;60(Suppl 1):i21–5.
Nieuwenhuijsen K, Verbeek JHA, de Boer AGE, Blonk RWB, van Dijk FJH. Supervisory behaviour as a predictor of return to work in employees absent from work due to mental health problems. Occup Environ Med. 2004;61(10):817–23.
Nieuwenhuijsen K, Verbeek JH, de Boer AG, Blonk RW, van Dijk FJ. Predicting the duration of sickness absence for patients with common mental disorders in occupational health care. Scand J Work Environ Health. 2006;32(1):67–74.
Nieuwenhuijsen K, Verbeek JHA, de Boer AGE, Blonk RWB, van Dijk FJH. Irrational beliefs in employees with an adjustment, a depressive, or an anxiety disorder: a Prospective Cohort Study. J Rat Emo Cogn Behav Ther. 2010;28(2):57–72.
Vaez M, Rylander G, Nygren A, Asberg M, Alexanderson K. Sickness absence and disability pension in a cohort of employees initially on long-term sick leave due to psychiatric disorders in Sweden. Soc Psychiatry Psychiatr Epidemiol. 2007;42(5):381–8.
Ustun TB, Chatterji S, Bickenbach J, Kostanjsek N, Schneider M. The International Classification of Functioning, Disability and Health: a new tool for understanding disability and health. Disabil Rehabil. 2003;25(11–12):565–71.
Hensing G, Spak F. Psychiatric disorders as a factor in sick-leave due to other diagnoses. A general population-based study. Br J Psychiatry. 1998;172:250–6.
Nystuen P, Hagen KB, Herrin J. Mental health problems as a cause of long-term sick leave in the Norwegian workforce. Scand J Public Health. 2001;29(3):175–82.
Sanderson K, Andrews G. Prevalence and severity of mental health-related disability and relationship to diagnosis. Psychiatr Serv. 2002;53(1):80–6.
Ormel J, Von KM, den Van BW, Katon W, Brilman E, Oldehinkel T. Depression, anxiety, and social disability show synchrony of change in primary care patients. Am J Public Health. 1993;83(3):385–90.
Dekkers-Sanchez PM, Hoving JL, Sluiter JK, Frings-Dresen MH. Factors associated with long-term sick leave in sick-listed employees: a systematic review. Occup Environ Med. 2008;65(3):153–7.
Hensing G, Brage S, Nygard JF, Sandanger I, Tellnes G. Sickness absence with psychiatric disorders—an increased risk for marginalisation among men? Soc Psychiatry Psychiatr Epidemiol. 2000;35(8):335–40.
De Rijk A, Janssen N, Alexanderson K, Nijhuis F. Gender differences in return to work patterns among sickness absentees and their associations with health: a prospective cohort study in The Netherlands. Int J Rehabil Res. 2008;31(4):327–36.
van der Giezen AM, Bouter LM, Nijhuis FJ. Prediction of return-to-work of low back pain patients sicklisted for 3–4 months. Pain. 2000;87(3):285–94.
Gjesdal S, Ringdal PR, Haug K, Maeland JG. Predictors of disability pension in long-term sickness absence: results from a population-based and prospective study in Norway 1994–1999. Eur J Public Health. 2004;14(4):398–405.
Koopmans PC, Roelen CA, Groothoff JW. Frequent and long-term absence as a risk factor for work disability and job termination among employees in the private sector. Occup Environ Med. 2008;65(7):494–9.
Mondloch MV, Cole DC, Frank JW. Does how you do depend on how you think you’ll do? A systematic review of the evidence for a relation between patients’ recovery expectations and health outcomes. CMAJ. 2001;165(2):174–9.
Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev. 1977;84(2):191–215.
North F, Syme SL, Feeney A, Head J, Shipley MJ, Marmot MG. Explaining socioeconomic differences in sickness absence: the Whitehall II Study. BMJ. 1993;306(6874):361–6.
Feeney A, North F, Head J, Canner R, Marmot M. Socioeconomic and sex differentials in reason for sickness absence from the Whitehall II Study. Occup Environ Med. 1998;55(2):91–8.
Crowther R, Marshall M, Bond G, Huxley P. Vocational rehabilitation for people with severe mental illness. Cochrane Database Syst Rev. 2001;(2), Article No CD003080.
Allebeck P, Mastekaasa A. Swedish Council on Technology Assessment in Health Care (SBU). Chapter 5. Risk factors for sick leave—general studies. Scand J Public Health Suppl. 2004;63:49–108.
Anema JR, Jettinghoff K, Houtman I, Schoemaker CG, Buijs PC, van den BR. Medical care of employees long-term sick listed due to mental health problems: a cohort study to describe and compare the care of the occupational physician and the general practitioner. J Occup Rehabil. 2006;16(1):41–52.
Rebergen DS, Bruinvels DJ, Bezemer PD, van der Beek AJ, van MW. Guideline-based care of common mental disorders by occupational physicians (CO-OP study): a randomized controlled trial. J Occup Environ Med. 2009;51(3):305–12.
van der Klink JJ, Blonk RW, Schene AH, van Dijk FJ. Reducing long term sickness absence by an activating intervention in adjustment disorders: a cluster randomised controlled design. Occup Environ Med. 2003;60(6):429–37.
van Oostrom SH, Driessen MT, de Vet HC, Franche RL, Schonstein E, Loisel P, et al. Workplace interventions for preventing work disability. Cochrane Database Syst Rev. 2009;(2), Article No CD006955.
van der Weide WE, Verbeek JH, van Dijk FJ. Relation between indicators for quality of occupational rehabilitation of employees with low back pain. Occup Environ Med. 1999;56(7):488–93.
Verbeek J, Spelten E, Kammeijer M, Sprangers M. Return to work of cancer survivors: a prospective cohort study into the quality of rehabilitation by occupational physicians. Occup Environ Med. 2003;60(5):352–7.
Lysaght RM, Larmour-Trode S. An exploration of social support as a factor in the return-to-work process. Work. 2008;30(3):255–66.
Brouwer S, Krol B, Reneman MF, Bultmann U, Franche RL, van der Klink JJ, et al. Behavioral determinants as predictors of return to work after long-term sickness absence: an application of the theory of planned behavior. J Occup Rehabil. 2009;19(2):166–74.
Brouwer S, Reneman MF, Bultmann U, van der Klink JJ, Groothoff JW. A prospective study of return to work across health conditions: perceived work attitude, self-efficacy and perceived social support. J Occup Rehabil. 2010;20(1):104–112.
Easterbrook PJ, Berlin JA, Gopalan R, Matthews DR. Publication bias in clinical research. Lancet. 1991;337(8746):867–72.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Appendix
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Cornelius, L.R., van der Klink, J.J.L., Groothoff, J.W. et al. Prognostic Factors of Long Term Disability Due to Mental Disorders: A Systematic Review. J Occup Rehabil 21, 259–274 (2011). https://doi.org/10.1007/s10926-010-9261-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10926-010-9261-5