
Abstract
Purpose
The one-compartment model with first order absorption (ka1C) has been extensively used to fit oral data. But when the disposition parameters of the drug are not available, the bias in the parameter estimates remains unclear. In this paper, the effect of potential misspecification of the area under the curve (AUC) and the mean absorption time (MAT) was evaluated for three relatively slowly absorbed drugs/formulations.
Methods
Assuming a three-compartment disposition model with an input (absorption) rate described as a sum of two inverse Gaussian functions (2IG3C) as the true model, the deviations of AUC and MAT estimated with simpler models were analyzed. Simpler models, as the ka1C model (Bateman function), the one-compartment model with IG input function (IG1C) and the gamma density function were fitted to the oral data alone, and compared to the fits obtained with the 2IG3C model which also uses the 3C disposition parameters of the drug. Data from pharmacokinetic studies of trospium, propiverine and ketamine in healthy volunteers were analyzed using a population approach.
Results
The Bateman function (ka1C) allowed a robust estimation of the population mean AUC, but the individual estimates were highly biased. It failed in evaluating MAT. The simple alternative models did not improve the situation.
Conclusions
The Bateman function appears to be useful for estimating the population mean value of AUC after oral administration. The results reemphasize the fact that insight into the absorption process can be only gained when also intravenous reference data are available.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Just 100 years ago Murray Lyon published a paper entitled “The absorption of adrenalin” [1] where he derived the biexponential function for the first time in pharmacology. Dost was probably not aware of this work when he applied this model (later known as Bateman function) to oral absorption [2]. Now it is the most popular model in pharmacokinetics and has been used in more than 3000 population pharmacokinetic studies. The reason lies in the apparent simplicity of this model. It implies, however, two unrealistic assumptions:1) that the maximum of the absorption rate is reached immediately and 2) that the drug distributes instantaneously throughout the body (one - compartment model). Furthermore, it was argued that this would lead to unphysiologically long absorption times [3]. Nevertheless it may be a useful approximation for fitting oral concentration-time data when no information on distribution kinetics is available (i.e., no iv reference data). But according to the motto “Seek simplicity and distrust it.” [4], one should be aware of the approximations made and the potential effect of model misspecification.
Thus, the purpose of this communication is to examine the questions 1) of whether useful information on the absorption process can be extracted solely from data after oral (po) administration and 2) whether the Bateman function can serve as an empirical model to fit oral data. To this end, results obtained by using the Bateman function (monoexponential absorption rate) are compared with those obtained when fitting po data to a more complex model based on a flexible time course of absorption rate together with iv disposition parameters. Since this model not only provided an optimal fit (in contrast to the Bateman function) but also uses realistic assumptions, the parameter estimates were taken as the “true” parameter values. In the same way, we analyzed the performance of improvements of the one-compartment model, replacing the first order input function (absorption rate constant ka) by a flexible input function, i.e. a time- dependent fractional absorption rate ka(t) [5, 6]. Finally, the usefulness of the empirical alternative model, the unimodal gamma function [7] was investigated.
The model independent parameters area under the curve (AUC) and mean absorption time (MAT) resulting from the different alternative approaches were compared with the “true” values showing the differences in both population means and individual subject parameters. One specific question was whether reasonable estimates of MAT can be obtained from oral data alone. Note that we use the term MAT originally proposed by Cutler [8] as a measure of rate of bioavailability; it denotes the average time it takes for molecules to enter the systemic circulation following oral administration.
The study is based on bioavailability data of three drugs that were previously analyzed by the absorption model mentioned above. Data from a trospium study [9] and those obtained for the lowest and highest doses in the studies of propiverine [10] and R-ketamine [11] were analyzed. Propiverine and ketamine were administered as extended release and trospium as an immediated release formulation. Propiverine, ketamine are rapidly absorbed while trospium is only slowly absorbed. The low bioavailability of ketamine is due to a substantial hepatic first-pass extraction.
Methods
Model Based on Oral and Intravenous Reference Data (True Model)
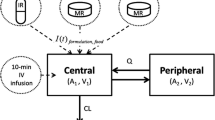
The data analysis has been described in detail in the original publications cited above. In short, the data obtained after iv injection were first fitted using a 3-compartment model; then, holding the six disposition parameters fixed, the parameters of the input function, i.e. the time course of the absorption rate (rate of drug input into the central compartment), I(t), were estimated by fitting the oral data. I(t) was described as a sum of two sum of inverse Gaussian (IG) functions (2IG3C model).
where D is dose, F is bioavailability, fi(t) denotes the IG function below and p is a nonnegative quantity that defines the relative contribution of each IG to the input function I(t).
where MTi and \({RD}_i^2\) are the scale and shape parameters, respectively, of the ith IG function. The mean absorption time is then given by
and \(AUC=FD/CL\).
where CL denotes clearance.
In the literature, one can find many examples where this model was successfully applied [12,13,14,15,16]. Since ka is not anymore a constant as for first-order absorption, but rather a function of time, we introduce the time-dependent absorption rate coefficient or fractional absorption rate ka(t) [5].
where Agi denotes the unabsorbed drug amount (note that dAgi/dt = I(t), Eq. 1).
Models Based Solely on Oral Data
Assuming that no iv reference data are available, the following models were used to fit oral plasma concentration-time data to:
-
1.
One-compartment model with first order absorption (ka1C)
The result is the Bateman function with absorption and elimination rate constants, ka and ke,
Where MAT = 1/ka and
-
2.
One-compartment model with IG input function (IG1C)
Instead of assuming a monoexponential absorption rate, i.e., a constant fractional absorption rate ka, the time course of absorption rate is described by a single IG function.
with f(t) given by Eq. 2. Then ka becomes a time-dependent function ka(t), and
\({\displaystyle \begin{array}{c} MAT= MT\\ {} AUC= FD/ CL\end{array}}\) .
-
3.
Unimodal gamma curve [7]
where Γ is the gamma function. Note that here no estimate of MAT is available.
Parameter Estimation
Parameter estimation was performed by population analysis (nonlinear mixed-effects modeling) using the ADAPT (Version 5) software [17]. ADAPT 5 provides estimates of the population mean and inter-subject variability as well as of the individual subject parameters (conditional means). We assumed log-normally distributed model parameters and that the measurement error has a standard deviation that is a linear function of the measured quantity. ‘Goodness of ft’ was assessed using the Akaike information criterion (AIC) and by plotting the predicted versus the measured responses. In all cases “rich” po data were fitted: Trospium 12 subjects with 24 measurements per subject, propiverine 10 subjects with 16 measurements per subject and ketamine 15 subjects with 14 measurements per subject. The mean plasma concentration time curves can be found in the Supplementary Material.
Results
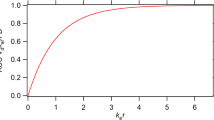
That the essential difference between the approaches lays in the models of the absorption process is shown in Fig. 1, where the time courses of absorption rates and of time-dependent absorption rate coefficients, ka(t), are shown for trospium as an example. It is clear a priori that the absorption rate increases from 0 to a maximum, and cannot be maximal at time 0 as for the ka1C model. The IG1C model reaches its (higher) maximum too early. The corresponding fractional absorption rates vary with time, except for ka1C model where ka = const. The ka(t)-function of the IG1C model reaches this value asymptotically.

Dose normalized time profiles of absorption rates resulting from fitting po data to the Bateman function (ka1C), to the IG input and one-compartment disposition model (IG1C) (both without iv data), and to the 2IG3C model with iv data (true model) (True) (left), and the corresponding time-dependent absorption rate coefficients (right). The curves were simulated using the population mean parameter estimates of the input function.
In no case an individual C(t) curve could be adequately fitted to a Bateman function (ka1C). This is also due to the fact that no concentration-time curve was log-concave, i.e., the logarithm of C(t) was not a concave function of time [5, 15]. A comparison of the goodness of fit plots is shown for trospium in Fig. 2. The AIC values for the models are summarized in Table I. The fractional deviations of the population mean values of AUC and MAT from those of the reference model (true values) are depicted in Table II. For AUC the relative low biases of the population means are in contrast to the large biases in the individual estimates (Fig. 2). The deviations of the MAT mean values estimated with the ka1C and IG1C model are unacceptable high for all drugs (except for trospium) (Table II).

Examples of fits of trospium data for a subject to the 2IG3C model with iv data (true model) (A) and to the ka1C model (Bateman function) (C). The corresponding goodness-of-fit plots (observed concentration versus the individual model-predicted values for all 12 subjects) are shown on the right site (B and D).
Discussion
An important and unexpected result is that the Bateman function allowed a robust estimation of the population mean value of AUC with biases less than 3% in 5 cases and 11% in one case (Table II). This may speak for its use as an empirical curve model in population kinetics. In contrast, the individual estimates are highly biased, but the positive and negative deviations cancel each other out (Fig. 3). However, the model fails in the estimation of MAT, with an underestimation between 25% and 70% in 5 cases and 6% in one case (Table II). That the replacement of first order absorption by the more realistic IG input model (IG1C) does not improve this situation, shows that the reason lies in the one-compartment approximation with its unrealistic assumption of instantaneous drug distribution throughout the body after iv injection. This suggests that the knowledge of distribution parameters together with clearance is a sine qua non for an estimation of reasonable MAT values. In other words, the iv data from bioavailability studies must be fitted separately in order to fix the disposition parameters when fitting the oral data. Note that the bias of the IG1C model with respect to the AUC population means is hardly lower than that for the Bateman function. Since the biases of AUC for the gamma model are in all cases higher than those of the Bateman function, it is not a useful alternative model.

The relative biases in AUC estimation derived from individual fits using the ka1C model (left) and IG1C model (right) for trospium (above) and ketamine 80 mg (below).
Although the assessment of alternative models was based on the accuracy of parameter estimation rather than the goodness of fit, Table I shows that the true model (2IG3C) has the lowest AIC, followed by the IG1C model in 4 of the 6 cases, while the gamma model provided the worst fit.
More complex input and disposition models as the 2IG input model and the two-compartment disposition model proved not suitable for fitting of po data (without iv data); on the one hand because of overparameterization and on the other hand due to the fact that information about the distribution process gets lost (vanishing of exponential terms). Thus, if MAT is long compared to the mean disposition residence time (MDRT = Vss/CL), log-concave curves are generated (apparent one-compartment distribution) [5]. While the Batman function is an appropriate empirical model for log-concave functions, it is not useful as a mechanistic model. Note that the MAT values for these drugs/formulations lay between 8 h and 13 h, with MAT/MDRT ratios of about 0.6 for trospium and R-ketamine, and 1 for propiverine. Since MAT > MDRT does not hold in these cases, it is not surprising that individual curves could not be adequately fitted to a Bateman function (Fig. 2).
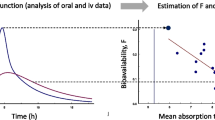
The results reveal the problems in estimating MAT from po data alone. Thus, as the absolute bioavailability F can be only estimated when iv data are available, the same holds also for MAT. Yet one may argue that this conclusion was based on only three pharmacokinetic studies. However, it is clear a priori that the oral C(t)-curve is the result of the input and disposition process: Using C(t)-data after po administration we can estimate the mean body residence time (MBRT) from the first moment of the curve
(e.g., MBRT = 1/ka + 1/ke for the ka1C model and MBRT = a/b for the gamma model), and
MAT is determined by.
Since MDRT can be estimated only from iv data, it is impossible to estimate MAT when no iv reference data are available. This problem remains also when a more complex input function improves the fit. This fact has not been recognized in some recently proposed models of drug absorption that are based on a one-compartment disposition model, e.g. [18,19,20]. Interestingly, the shortcomings of using the one-compartment approach to analyze drug absorption kinetics have been pointed out already 55 years ago [21]. Note also that recently the finite absorption time concept was proposed as an alternative to the one-compartment model [22].
In contrast to MAT, the area under the curve (AUC) after po administration can be estimated with any empirical model that fits the data. While the biases of AUC estimates (Table II and Fig. 3) are only characteristic for these drugs/formulations, analogous results may be obtained for other slowly absorbed drugs or extended release formulations. While the results obtained from such case studies cannot be simplistically generalized, at least the assumption that the Bateman function may be useful for fitting oral C(t)-data could not be disproved.
Conclusions
When no iv data are available, the Bateman function appears to be useful for estimating the population mean value of AUC after po administration. The low bias in the mean values is in contrast to the highly biased individual estimates of AUC. The results of this study reemphasize the fact that insight into the absorption process can be only gained when also iv reference data are available. Whereas this is well accepted for bioavailability, there is less agreement regarding the estimation of parameters of absorption kinetics (e.g. MAT). It is clear from theory and our results that the one- compartment approximation is not useful for this purpose.
References
Lyon DM. The Absorption of Adrenalin. J Exp Med. 1923;38(6):655–65. https://doi.org/10.1084/jem.38.6.655.
Dost FH. Kann man dem Clearance-Begriff einen solchen der “Entrance” gegenüberstellen? Arch Pharmakol Exp Pathol. 1951;213(5):435–52. PMID: 14934137
Macheras P. On an Unphysical Hypothesis of Bateman Equation and its Implications for Pharmacokinetics. Pharm Res. 2019;36(7):94. https://doi.org/10.1007/s11095-019-2633-4.
Whitehead AN. The concept of nature. Cambridge: Cambridge University Press; 1919.
Weiss M. Generalizations in linear pharmacokinetics using properties of certain classes of residence time distributions. II. Log-concave concentration-time curves following oral administration. J Pharmacokinet Biopharm. 1987;15(1):57–74.
Macheras P, Argyrakis P. Gastrointestinal drug absorption: is it time to consider heterogeneity as well as homogeneity? Pharm Res. 1997;14(7):842–7. https://doi.org/10.1023/a:1012183313218.
Weiss M. Use of gamma distributed residence times in pharmacokinetics. Eur J Clin Pharmacol. 1983;25(5):695–702. https://doi.org/10.1007/BF00542361. PMID: 6662168
Cutler DJ. Theory of the mean absorption time, an adjunct to conventional bioavailability studies. J Pharm Pharmacol. 1978;30(8):476–8. https://doi.org/10.1111/j.2042-7158.1978.tb13296.x.
Abebe BT, Weiss M, Modess C, Roustom T, Tadken T, Wegner D, et al. Effects of theP-Glycoprotein Inhibitor Clarithromycin on the Pharmacokinetics of Intravenous and Oral Trospium Chloride: A 4-Way Crossover Drug-Drug Interaction Study in Healthy Subjects. J Clin Pharmacol 2019. https://doi.org/10.1002/jcph.1421.
Weiss M, Sermsappasuk P, Siegmund W. Modeling the heterogeneous intestinal absorption of propiverine extended-release. Eur J Pharm Sci. 2015;76:133–7. https://doi.org/10.1016/j.ejps.2015.05.010.
Weiss M, Siegmund W. Pharmacokinetic Modeling of Ketamine Enantiomers and Their Metabolites After Administration of Prolonged-Release Ketamine With Emphasis on 2,6-Hydroxynorketamines. Clin Pharmacol Drug Dev. 2021; https://doi.org/10.1002/cpdd.993.
Csajka C, Drover D, Verotta D. The use of a sum of inverse Gaussian functions to describe the absorption profile of drugs exhibiting complex absorption. Pharm Res. 2005;22(8):1227–35. https://doi.org/10.1007/s11095-005-5266-8.
Wendling T, Ogungbenro K, Pigeolet E, Dumitras S, Woessner R, Aarons L. Model-based evaluation of the impact of formulation and food intake on the complex oral absorption of mavoglurant in healthy subjects. Pharm Res. 2015;32(5):1764–78. https://doi.org/10.1007/s11095-014-1574-1.
Tadken T, Weiss M, Modess C, Wegner D, Roustom T, Neumeister C, et al. Trospium chloride is absorbed from two intestinal "absorption windows" with different permeability in healthy subjects. Int J Pharm. 2016;515(1–2):367–73. https://doi.org/10.1016/j.ijpharm.2016.10.030.
Weiss M. Empirical models for fitting of oral concentration time curves with and without an intravenous reference. J Pharmacokinet Pharmacodyn. 2017;44(3):193–201. https://doi.org/10.1007/s10928-017-9507-3
Weiss M, D'Argenio DZ, Siegmund W. Analysis of Complex Absorption After Multiple Dosing: Application to the Interaction Between the P-glycoprotein Substrate Talinolol and Rifampicin. Pharm Res. 2022;39(12):3293–300. https://doi.org/10.1007/s11095-022-03397-6. 5.16
D’Argenio D, Schumitzky A, Wang X. User’s guide: Pharmacokinetic/pharmacodynamic systems analysis software. Los Angeles, CA: Biomedical Simulations Resource; 2009.
Savic RM, Jonker DM, Kerbusch T, Karlsson MO. Implementation of a transit compartment model for describing drug absorption in pharmacokinetic studies. J Pharmacokinet Pharmacodyn. 2007;34(5):711–26. https://doi.org/10.1007/s10928-007-9066-0.
Zahr N, Amoura Z, Debord J, Hulot JS, Saint-Marcoux F, Marquet P, et al. Pharmacokinetic study of mycophenolate mofetil in patients with systemic lupus erythematosus and design of Bayesian estimator using limited sampling strategies. Clin Pharmacokinet. 2008;47(4):277–84. https://doi.org/10.2165/00003088-200847040-00005.
Gomeni R, Komolova M, Incledon B, Faraone SV. Model-based approach for establishing the predicted clinical response of a delayed-release and extended-release methylphenidate for the treatment of attention-deficit/hyperactivity disorder. J Clin Psychopharmacol. 2020;40(4):350–8. https://doi.org/10.1097/JCP.0000000000001222.
Riegelman S, Loo JC, Rowland M. Shortcomings in pharmacokinetic analysis by conceiving the body to exhibit properties of a single compartment. J Pharm Sci. 1968;57(1):117–23. https://doi.org/10.1002/jps.2600570123.
Chryssafidis P, Tsekouras AA, Macheras P. Re-writing Oral Pharmacokinetics Using Physiologically Based Finite Time Pharmacokinetic (PBFTPK) Models. Pharm Res. 2022;39(4):691–701. https://doi.org/10.1007/s11095-022-03230-0.
Acknowledgements
The author is grateful to Dr. Werner Siegmund for providing the data used in this application.
Funding
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
ESM 1
(DOCX 108 kb)
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Weiss, M. Is the One-Compartment Model with First Order Absorption a Useful Approximation?. Pharm Res 40, 2147–2153 (2023). https://doi.org/10.1007/s11095-023-03582-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11095-023-03582-1