
Abstract
Purpose
Near-infrared spectroscopy (NIRS) sensors measure muscle oxygen saturation (SmO2) as a performance factor in endurance athletes. The objective of this study is to delimit metabolic thresholds relative to maximal metabolic steady state (MMSS) using SmO2 in cyclists.
Methods
Forty-eight cyclists performed a graded incremental test (GTX) (100 W-warm-up followed by 30 W min) until exhaustion. SmO2 was measured with a portable NIRS placed on the vastus lateralis. Subjects were classified by VO2max levels with a scale from 2 to 5: L2 = 45–54.9, L3 = 55–64.9, L4 = 65–71, L5 = > 71, which represent recreationally trained, trained, well-trained, and professional, respectively. Then, metabolic thresholds were determined: Fatmax zone, functional threshold power (FTP), respiratory compensation point (RCP), and maximal aerobic power (MAP). In addition, power output%, heart rate%, VO2%, carbohydrate and fat consumption to cutoff SmO2 point relative to MMSS were obtained.
Results
A greater SmO2 decrease was found in cyclists with > 55 VO2max (L3, L4 and L5) vs. cyclists (L2) in the MMSS. Likewise, after passing FTP and RCP, performance is dependent on better muscle oxygen extraction. Furthermore, the MMSS was defined at 27% SmO2, where a non-steady state begins during exercise in trained cyclists.
Conclusion
A new indicator has been provided for trained cyclists, < 27% SmO2 as a cut-off to define the MMSS Zone. This is the intensity for which the athlete can sustain 1 h of exercise under quasi-steady state conditions without fatiguing.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Currently, sports scientists and coaches use various parameters to classify performance in endurance athletes such as cycling and triathlon; among these, we find VO2max, power and heart rate at different exercise intensities [1, 2]. During a graded exercise test (GXT) it is possible to obtain points and/or metabolic thresholds such as the fatmax zone, ventilatory thresholds, maximum aerobic power (MAP) and the functional threshold power (FTP) [3, 4], which can be used in well-trained cyclists as a practical and non-invasive alternative to estimate the maximum lactate steady state (MLSS) [5]. Also, a key parameter is the respiratory compensation point (RCP), which allows distinguishing between fatigued and non-fatigued work, this occurs due to the worsening of metabolic acidosis produced by respiratory compensation and is identified by an increase in minute ventilation (VEQ) in relation to CO2 production (VCO2); this generally occurs at approximately 80% VO2max [6, 7]. The FTP and RCP show a similar physiological mechanism due to work under fatigue conditions [8, 9], which is related to the “maximum metabolic steady state” (MMSS), representing the highest metabolic rate at which exercise can be maintained almost exclusively by oxidative metabolism, representing the upper limit of sustainable exercise [10]. Therefore, MMSS is a valuable component when prescribing personalised exercise. Measuring metabolic thresholds is routine in cyclists and triathletes because they can accurately track the subtle improvements in endurance performance that elite athletes attain during a season.
Heart rate and power output are often used as indicators of workload. These parameters are of interest because of their relationship with oxygen consumption during training, as wearable watches and sensors are based on these parameters to calculate the energy expenditure [11, 12]. However, there are some problems in considering HR as an indicator of internal workload, because it shows variability in unstable conditions, for example in the transition from fatigue-recovery states and psychological disorders such as stress [13]. Interestingly, in recent years portable sensors have been invented that measure muscle oxygen saturation (SmO2), which is a variable that can be used to monitor training on a scale of 0–100% and is validated by brands such as portable MOXY [14], as used in cyclists and triathletes. From a scientific point of view, decreased SmO2 is an indicator of better performance during cycling [15]. It also has a correlation with VO2, ventilatory thresholds and MLSS [16,17,18]. However, although there are studies that use SmO2 during GXT to estimate ventilatory threshold points [17, 18] and training zones (moderate, heavy and severe intensity) [19], there are scientific gaps regarding the physiological behaviour during SmO2 transitions in fatmax zone, FTP, RCP and MAP. SmO2 during fatmax, FTP and CPR relative to MMSS could differentiate the performance level of athletes, since, as a general rule, performance is a mediator of daily training planning [20]. As such, there has been no response with a solid scientific basis, so it is important to reach an agreement and suggest a new proposal for the SmO2 interpretation and its applicability as an internal load.
Therefore, the objective of this study was to delimit the MMSS by VO2max levels using SmO2 in trained cyclists; the following hypotheses are considered: (i) the use of SmO2 during exercise can identify the performance level and metabolic thresholds of the cyclists, and (ii) SmO2 can be used to determine the approximate MMSS from the FTP and RCP breakpoints. The objective of this study was to delimit the MMSS by VO2max levels using SmO2 in trained cyclists.
Methods
Participants
The sample included was 48 trained cyclists and triathletes (Experience in endurance training 10.9 ± 4.9 years and Skinfold of the vastus laterialis (ATT) 10.7 ± 5.9 mm), performance was classified by performance levels using the VO2max (ml/kg/min) with a scale from 1 to 5: level 1: < 45; level 2: 45–54.9; level 3: 55–64.9 level 4: 65–71; level 5: > 71, representing untrained, recreationally trained, trained, well-trained, and professional subject groups, respectively [2]. For this study, level 1 is ruled out because the participants are athletes and no value < 45 of VO2max was found. The descriptive values based on the physiological parameters of the subjects are shown in the Table 1. No physical limitations or musculoskeletal injuries that could affect training were reported. This study was conducted during the agonistic season. The study was carried out in accordance with the Helsinki Declaration and approved by the Bio-Ethical Committee of the University of Extremadura with N° registration code: 131/2018. A signed consent was obtained from each subject prior to their participation.
Experimental design
The trial design was cross-sectional. Participants carried out the test under similar environmental conditions (21–24 °C and 45–55% relative humidity) and were asked to abstain from performing intense exercise 48 h prior to the test. Before the GXT, body mass and Skinfold of Vastus laterialis values were ascertained. Then, a GXT was performed to obtain the physiological together with the SmO2.
Performance assessments
Maximal graded exercise test (GXT)
First, a standardized warm-up of 10 min at 100 W was performed, the set up consisted in increments 30 W·min-3 until exhaustion [21]. The end of the test was considered when the participant was unable to maintain the power output of each final completed stage. During GXT participants were monitored through a gas exchange measurement system/device with breath-by-breath technology and calibrated before each test (Metalyzer 3b, CORTEX Biophysik GmbH, Leipzig, Germany). Each participant used their own bike mounted on a smart training device (Bkool, model Bkool one; Madrid, Spain). The protocol was completed with a PowerTap P1 (PP1), which produced reliable output power readings of 100–500 W, in a seated position (rho ≥ 0.987), and an absolute reliability index (150–500 W; COV = 2.3%; SEM < 1.0 W) [22]. The PowerTap during cardiopulmonary tests are more ecologically valid, allowing cyclists to use their own bicycles [22]. HR was collected via a HR monitor (HRM-Tri; Garmin Ltd., Olathe, KS, USA). The smart trainer assessed power with internal sensors that were paired to a smartwatch for future analysis (Forerunner 735xt, Garmin,Olathe, KS, USA). Finally, when GXT was finished, a drop of capillary blood was drawn for lactate measurement (Lactate Pro 2, Arkray Factory, Inc., Amstelveen, The Netherlands), after 3 min of passive recovery [23].
Muscle oxygen saturation assessment
Local muscle oxygen saturation (SmO2) was assessed with a near-infrared spectroscopy (NIRS) device (MOXY, Fortiori Design LLC, Minneapolis, Minnesota, USA). Which is valid for measuring SmO2 (ICC: r = 0.773–0.992) [24]. It was attached firmly to the belly of the right vastus lateralis muscle (midway between lateral epicondyle and greater trochanter of femur) using a dark elastic strap to avoid light contamination and movement artifacts. The vastus lateralis was selected based on previous evidence and considering the role of this muscle in cycling [25]. The skinfold thickness at the NIRS measurement site (VL) was measured using a skinfold caliper (Harpenden Ltd.) to ensure that the skinfold thickness was < 1/2 of the distance between the emitter and the detector. (25 mm). The raw muscle O2 saturation (SmO2) signal was treated with a soft spline filter to reduce noise created by movement [26] using a Minitab 19 (Minitab, Inc, State College, PA; www.minitab.com, USA).
For the data analysis the following guidelines were followed:
-
(1)
The average value of the last minute of the 3-min step was used.
-
(2)
Data was excluded when changes in SmO2 > 10% were observed, compared to the previous SmO2 value, this was considered as measurement error.
-
(3)
Data that gave 0% of reading were excluded due to the apparent lost signal. The data was viewable in real time to the NIRS technology expert researchers and muscle oxygenation measurement, using ANT + technology software (Golden Cheetah version 3.4, USA) and joint data processing software (Excel 2016, Microsoft Office 365, USA).
Gas exchange analysis to determine metabolic thresholds
Fatmax Zone: The Fat oxidation (FAT), carbohydrate oxidation (CHO) were calculated using appropriate stoichiometric equations [27] and energy equivalence, based on the measured values achieved
Data analysis to determine Fatmax involved the measured values approach in the stage with the highest recorded fat oxidation value and the corresponding ̇VO2 [21].
Maximum Metabolic Steady State (MMSS): MMSS is considered to be the highest oxidative metabolic rate that can be sustained during continuous exercise. However, there are several indices that are often used to identify the MMSS [28]
-
1.
Functional Thresholds Power (FTP): The FTP was calculated with the maximum incremental cycle test methodology until exhaustion to find the resulting maximum power, from which the FTP is obtained by the following equation [29]:
$$\mathrm{FTP}=\mathrm{Output power} \left(W\right) \times 0.865-56.484.$$ -
2.
Respiratory Compensation Point (RCP): The RCP is defined as the anabrupt and positive ‘‘acceleration’’ in VE/VO2 versus VO2 and VE/VCO2 versus VO2 data [30], and was confirmed by a simultaneous reduction of the end-expiratory pressure of CO2 [20] This was determined by 2 independent exercise physiologists by visual inspection. We also provide the VEQ values as a reference for each performance group. V-slope load was identified in that intensity of exercise which, in a plot of the minute production of CO2 over the minute utilization of oxygen (VO2), shows an increase in the slope above 1.0 [31]. The VO2max was defined as the highest plateau (two successive maximal within 150 mL·min−1, averaging the data every 5 s) reached [32].
-
3.
SmO2 Transition to metabolic threshold: The transition point of muscle oxygenation was identified as the difference in the SmO2 values from FTP to RCP/VT2.
Statistic analysis
A descriptive analysis of the data extracted from the incremental test was applied and the Shapiro Wilk normality test was applied for each variable. When normality was reached, the two-way repeated measures analyses of variance ANOVA test was performed to identify the effects of the two categories: VO2max levels and metabolic thresholds relative to MMSS. Then a bonferroni post hoc was applied to identify the internal differences between the groups. In addition, the receiver operating characteristic (ROC) curves was used to establish a cutoff for SmO2 at the MMSS value, and the area under curve (AUC) was used to evaluate the performance of a classifier, where the threshold cut-off values were defined by the points representing the highest concomitant sensitivity and specificity, the AUC was interpreted according to with the following guidelines: not informative (AUC = 0.5), less accurate (0.5–0.7), moderately accurate (0.7–0.9), high precision (0.9–1) and perfect discriminatory test (AUC = 1.0) [33]. Also, a differential analysis of the performance variables was performed using the SmO2 cut-off established in relation to MMSS. The level of significance was established at p < 0.05 with 95% confidence intervals. The results were expressed as mean ± standard deviation. All analyzes were performed with SPSS software (version 22).
Results
Table 1 shows the mean values of the general physiological parameters during a GET, differences were found in level 2 vs level 3,4 and 5, in the variables weight, VO2max (p ≤ 0.001), HRmax (p ≤ 0.001), Resting HR (p ≤ 0.001), Lactate (p ≤ 0.001), Power W (p ≤ 0.001), Fat% (p = 0.000) and SmO2 (p ≤ 0.005), observing a worse performance at level 2.
Table 2 shows the SmO2 values comparing by performance levels in the metabolic thresholds: Fatmax, transition between FTP and RCP and MAP. Differences were found in level 2 vs level 5 (FO Δ = 17 p ≤ 0.005; FTP ∆ = 14 p ≤ 0.001; RCP Δ = 17 p ≤ 0.001; MAP Δ = 12 p ≤ 0.001). Likewise, differences were found between level 2 vs level 3 and 4 in SmO2 at the FTP and RCP (SmO2 difference of levels 2 vs levels 3 and 4 Δ = 18; Δ = 21; Δ = 22; p ≤ 0.001 and Δ = 13; Δ = 16, respectively).
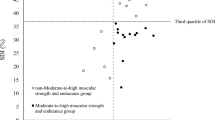
Figure 1 represents the ROC curve to assess the cut-off of SmO2 and maximum metabolic steady state in relation to FTP and CPR, established from VO2max level 3 (> 55 ml/kg/min). We found an 63% (AUC) with a SE = 0.039; p = 0.001 and lower and upper limits = (0.55–0.70%), which indicates a value of 26.80 for SmO2, Sensitivity = 0.595 and Specificity = 0.558, hence we propose 27% SmO2 as an approximation to MMSS and < 27 SmO2 as a reference for the fatigue thresholds.

An analysis of the receptor operating characteristics (ROC) curve to evaluate the cut-off for muscle oxygen saturation and maximum metabolic steady state
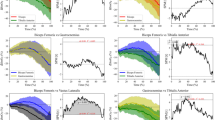
Figure 2 shows differences by VO2max levels with the SmO2 kinetics during GET. First, we observed better MSSS and better SmO2 performance at levels 4 and 5 (W:289 ± 51; SmO2: 26 ± 8 and L5 = W: 301 ± 25; SmO2: 24 ± 4) vs 2 and 3 (L2 = W: 214 ± 35; SmO2: 40 ± 14 and L3 = W: 252 ± 41; SmO2: 29 ± 8 p ≤ 0.001). It was also observed that levels 3, 4 and 5 use less SmO2 than level 2 after passing MMSS (L:3 9 ± 6; L4:10 ± 7 and L5: 7 ± 8 vs 15 ± 8 p ≤ 0.001).

Reference of muscle oxygen saturation at the maximal metabolic steady state: comparison by VO2max levels
Likewise, we highlight that before exceeding the MMSS, the use of oxygen is similar in all the performance groups where no difference was observed (L2: 26 ± 15; L3: 28 ± 17; L4: 27 ± 19 and L5: 22 ± 18, respectively). Finally, it can be seen that in levels 3, 4 and 5 the SmO2 vs the output power is reached close to 27%, in level 2 a delay is observed and SmO2 at the MMSS is greater than 27% (possibly between 40 and 45%).
Table 3 shows the differences by VO2max levels, using the reference point of 27% SmO2, considering it as a fatigue threshold, once the MMSS is exceeded. Also, shows physiological parameters. Differences were found between level 2 y 3 with the level 5 in time (L5 vs. L2: Δ = 4.0 p ≤ 0.005; L3: Δ = 2.0 p ≤ 0.001) and W/kg (level 5 vs level 2:Δ = 0.71 p ≤ 0.005; level 3: Δ = 0.44 p ≤ 0.005), also is observed that the level 5 group consumed more fat when reaching the 30% SmO2 point (L5 vs. L2: Δ = 2.1 p ≤ 0.001; L3: Δ = 1.9 p ≤ 0.001 Δ = 1.7 p ≤ 0.001).
Discussion
This study used SmO2 to check performance differences by VO2max levels through the measurement of metabolic thresholds associated with MMSS such as FTP and RCP. The main finding is that subjects trained from a VO2max > 55 can take into consideration SmO2 values of < 27% as the internal training load nears FTP and RCP. Also, it is assumed that below 27% SmO2 the maximum metabolic steady state occurs and is observable by critical oxygenation, as recently discovered by Feldmann and Erlacher [34].
According to the findings, athletes with a greater training status (higher VO2max levels) achieved a better performance in reducing SmO2 values [15]. A greater SmO2 decrease is related to power output increase [24, 34]. Likewise, our study determined that SmO2 in the fatmax zone only showed a difference with athletes of Level 5 “ > 71 VO2max” vs. Level 2 “ < 55 VO2max”; however, in the MAP zone there is only a difference between the greater capacity “ > 65 VO2max”. This explains that the differences between athletes in energy expenditure during high-intensity exercise and the use of muscle oxygen to generate ATP as metabolic fuel [35]. Figure 2 also shows a greater SmO2 decrease in athletes with higher VO2max after passing the FTP and CPR breakpoint. Therefore, fatigue resistance depends on the ability to maintain critical oxygenation (CO) over time with lower SmO2 values [19]. OC is the ability of the muscle to maintain adequate oxygen supply to match oxygen demand as the basis for steady-state exercise theory [34, 36]
In our study, athletes > 65VO2max achieved greater desaturation levels than less highly trained athletes; this is supported by Fontana et al. [37], who found that the oxygen used after passing the RCP is lower and depends on the capacity for ATP production that comes from non-oxidative metabolic pathway. To explain the physiological mechanisms of the progressive decrease in SmO2 and increase in VO2 from a systemic perspective, it is the result of a linear increase in cardiac output (i.e., systemic blood flow) and a hyperbolic increase in the arterio-venous O2 difference (that is, systemic O2 extraction) until depletion [38]. Portable NIRS-derived local O2 extraction (SmO2) within active tissues does not show the same hyperbolic profile as systemic measurements, indicating that the central and peripheral profiles of O2 extraction and blood flow are different [39]. However, these studies did not discuss the changes in metabolic pathways within the muscle, which, once the MMSS-related with fatigue thresholds are exceeded, are less dependent on oxygen to generate power [40,41,42]. As a results, there is a muscle O2 extraction reserve that can only be used at the GTX end, that is, at high intensities (> 85% VO2max), which is observable in a greater SmO2 decrease and greater oxygen extraction capacity by the muscle [43]. This was seen in our study, as higher VO2max can desaturate more oxygen, so SmO2 can be considered as a performance factor in high intensity exercise.
Likewise, a better interaction between the supply and extraction of O2 by the muscle depends on the recruitment of motor units covered by the muscle fibres; in this sense, the type II fibres are activated to a higher level after the FTP and RCP breakpoints, and, therefore, there is a metabolic pathway change; being an ‘oxygen independent’ energy system [44], a lower extraction of muscle oxygen was observed since type II fibres have less oxidative capacity and need less oxygen to function, but they achieve better performance in the high-intensity zones due to their glycolytic capacity to maintain a greater force and power production [42, 43]. This, has also been demonstrated in the greater progressive recruitment of fast-contracting motor units (type II fibres) in the vastus lateralis muscle with EMG at the end of the exercise (> 80%) where there is less extraction of tissue oxygen [45].
On the other hand, among the factors that explain the SmO2 decrease after FTP and RCP are an increase in the oxygen partial pressure and hydrogen (H), a decrease in pH and the CO2 partial pressure within the active muscles [46], which cause a vasodilator response when the high intensity exercise cannot be sustained [47]. The demand of oxygen extraction then follows in a hyperbolic and non-linear way, due to the muscles’ attempts to restore PCr/ATP by the non-oxidative pathway, which is why small increases in muscle oxygen occur during the heavy and severe intensity domains (VO2 phase II and III) [43]. Likewise, previous studies determined that the VO2 slowing at the exercise end causes an increase in the respiratory muscle work, and this attenuates the increase in blood flow and O2 transport in the legs [48]. This also supports the proposal to use < 27% SmO2 in trained subjects, not as a breakpoint but rather as a fatigue threshold. Therefore, it is necessary to understand that critical oxygenation occurs after this threshold < 27% SmO2.
Finally, we highlight that there is already a breakpoint in oxygenated HBO within the muscle; that is, in a similar way to SmO2, the signal from this breakpoint is a reliable biomarker of exercise intensity which is closely associated with VO2 at the RCP [49, 50], since it occurs at the same metabolic rate [37]. The RCP is close to 27% SmO2 (between 26 and 30%) observed in AUC (Fig. 1), which indicates that the MMSS may be before or after 27% SmO2, depending specifically on the degree of training. In this sense, Table 3 shows that when comparing all of the performance variables at the established point from 27% of each subject, no differences were found. This means that a gold-standard point within the SmO2 scale (0–100%) demarcates the intensity domain; because it will always be the same value. For example, with improvements in the VO2max% level, the fatigue zone would be delayed and better tolerated. Therefore, we suggest that the SmO2 value relative to MMSS represents the same metabolic rate for all groups. Our study found differences only in fat consumption (kcal/min) and with the greater capacity to produce power per weight (W/kg) in Level 5 vs Level 2 because the oxidative capacity resulting from the greater use of oxygen by type II fibres is inversely correlated with exercise economy and a lower capacity to produce power output [51]. It was observed that those at Level 5 maintained more power with the use of lower VO2max% (Table 3). This approach should be tested with different training programs and GXT protocols.
Limitations and recommendations
A limitation of our study was the non-measurement of critical power (CP), which denotes the transition from the intensity of heavy-severe exercise with relatively little error (SE, 11%), while the MMSS tend to underestimate by 11%. Also, RCP and VT2 overestimate CP by 6 and 21%, respectively [52]; therefore, 27% SmO2 is not an exact point and may overestimate some untrained athletes and non-cyclists. Also, during training, the cadence must be taken into account, since the use of muscle oxygenation is affected by acceleration [53]. Although there were small differences in the use of CH, HR%, power% and VO2max% in our study (Table 3), they were not statistically significant. This does not mean that it is not possible to train for targets over fatigue threshold or set point of < 27% SmO2, but this must be tested with seasonal training effects.
Conclusion
To summarise, trained cyclists and triathletes with a > 55 VO2max (ml/kg/min) could use values lower than 27% SmO2 as high-intensity zones and breakpoints relative to FTP and RCP, which is the intensity at which the athlete can sustain 1 h of exercise in quasi-steady-state conditions without fatiguing. Also, a greater SmO2 decrease is better in more highly trained athletes, this can be used to measure peripheral adaptations to training.
References
Capostagno B, Lambert MI, Lamberts RP (2016) A systematic review of submaximal cycle tests to predict, monitor, and optimize cycling performance. Int J Sports Physiol Perform 11(6):707-714
De Pauw K, Roelands B, Cheung SS, et al (2013) Guidelines to classify subject groups in sport-science research. Int J Sports Physio. Perform 8(2):111–122. https://doi.org/10.1123/ijspp.8.2.111
Nikolovski Z, Barbaresi S, Cable T, Peric R (2020) Evaluating the influence of differences in methodological approach on metabolic thresholds and fat oxidation points relationship. Eur J Sports Sci 21:61–68. https://doi.org/10.1080/17461391.2020.1717640
Borszcz FK, Tramontin AF, Bossi AH, et al (2018) Functional threshold power in cyclists: validity of the concept and physiological responses. Int J Sports Med 39(10):737–742. https://doi.org/10.1055/s-0044-101546
Borszcz FK, Tramontin AF, Costa VP (2019) Is the functional threshold power interchangeable with the maximal lactate steady state in trained cyclists? Int J Sports Physiol Perform. https://doi.org/10.1123/ijspp.2018-0572
Bergstrom HC, Housh TJ, Zuniga JM et al (2012) Estimated times to exhaustion and power outputs at the gas exchange threshold, physical working capacity at the rating of perceived exertion threshold, and respiratory compensation point. Appl Physiol Nutr Metab. https://doi.org/10.1139/H2012-057
Broxterman RM, Craig JC, Smith JR et al (2015) Influence of blood flow occlusion on the development of peripheral and central fatigue during small muscle mass handgrip exercise. J Physiol. https://doi.org/10.1113/JP270424
Keir DA, Fontana FY, Robertson TC et al (2015) Exercise intensity thresholds: identifying the boundaries of sustainable performance. Med Sci Sports Exerc. https://doi.org/10.1249/MSS.0000000000000613
Barranco-Gil D, Gil-Cabrera J, Valenzuela PL et al (2020) Functional threshold power: relationship with respiratory compensation point and effects of various warm-up protocols. Int J Sports Physiol Perform. https://doi.org/10.1123/ijspp.2019-0402
Iannetta D, Inglis EC, Pogliaghi S et al (2020) A “step-Ramp-Step” protocol to identify the maximal metabolic steady state. Med Sci Sports Exerc. https://doi.org/10.1249/MSS.0000000000002343
O’Toole ML, Douglas PS, Hiller WDB (1989) Lactate, oxygen uptake, and cycling performance in triathletes. Int J Sports Med. https://doi.org/10.1055/s-2007-1024935
Boudreaux BD, Hebert EP, Hollander DB et al (2018) Validity of Wearable Activity Monitors during Cycling and Resistance Exercise. Med Sci Sports Exerc. https://doi.org/10.1249/MSS.0000000000001471
Born DP, Stöggl T, Swarén MBG (2016) Running in Hilly Terrain: NIRS is more accurate to monitor intensity than heart rate. Int J Sports Physiol Perform. https://doi.org/10.1123/IJSPP.2013-0455
Feldmann A, Schmitz RW, Erlacher D (2019) Near-infrared spectroscopy-derived muscle oxygen saturation on a 0% to 100% scale: reliability and validity of the Moxy Monitor. J Biomed Opt 24:115001
Olcina G, Perez-Sousa M, Escobar-Alvarez J, Timón R (2019) Effects of cycling on subsequent running performance, stride length, and muscle oxygen saturation in triathletes. Sports. https://doi.org/10.3390/sports7050115
McMorries RM, Joubert DP, Jones EJ, Faries MD (2019) A Validation Study of a Noninvasive Lactate Threshold Device. Int J Exerc Sci 12(2):221. https://digitalcommons.wku.edu/ijes/vol12/iss2/7
Rodrigo-Carranza V, González-Mohíno F, Turner AP et al (2021) Using a portable near-infrared spectroscopy device to estimate the second ventilatory threshold. Int J Sports Med 42:905–910. https://doi.org/10.1055/A-1343-2127/ID/R8503-0019
Snyder AC, Parmenter MA (2009) Using near-infrared spectroscopy to determine maximal steady state exercise intensity. J Strength Cond Res 23:1833–1840. https://doi.org/10.1519/JSC.0B013E3181AD3362
Kirby BS, Clark DA, Bradley EM, Wilkins BW (2021) The balance of muscle oxygen supply and demand reveals critical metabolic rate and predicts time to exhaustion. J Appl Physiol 130:1915–1927. https://doi.org/10.1152/JAPPLPHYSIOL.00058.2021
Lucía A, Pardo J, Durántez A et al (1998) Physiological differences between professional and elite road cyclists. Int J Sports Med. https://doi.org/10.1055/s-2007-971928
Achten J, Jeukendrup AE (2003) Maximal fat oxidation during exercise in trained men. Int J Sports Med. https://doi.org/10.1055/s-2003-43265
Pallarés JG, Lillo-Bevia JR (2018) Validity and reliability of the powertap P1 pedals power meter. J Sport Sci Med 17:305–311
Gupta S, Goswami A, Sadhukhan AK, Mathur DN (1996) Comparative study of lactate removal in short term massage of extremities, active recovery and a passive recovery period after supramaximal exercise sessions. Int J Sports Med 17:106–110. https://doi.org/10.1055/S-2007-972816/BIB
Crum EM, O’Connor WJ, Van Loo L et al (2017) Validity and reliability of the Moxy oxygen monitor during incremental cycling exercise. Eur J Sport Sci 17:1037–1043. https://doi.org/10.1080/17461391.2017.1330899
Shibuya K, Tanaka J (2003) Skeletal muscle oxygenation during incremental exercise. Arch Physiol Biochem 111:475–478. https://doi.org/10.3109/13813450312331342355
Rodriguez RF, Townsend NE, Aughey RJ, Billaut F (2018) Influence of averaging method on muscle deoxygenation interpretation during repeated-sprint exercise. Scand J Med Sci Sport. https://doi.org/10.1111/sms.13238
Jeukendrup AE, Wallis GA (2005) Measurement of substrate oxidation during exercise by means of gas exchange measurements. Int J Sport Med Suppl 26(S1):S28–S37. https://doi.org/10.1055/s-2004-830512
Jones AM, Burnley M, Black MI et al (2019) The maximal metabolic steady state: redefining the ‘gold standard.’ Physiol Rep 7:e14098. https://doi.org/10.14818/PHY2.14098
Denham J, Scott-Hamilton J, Hagstrom AD, Gray AJ (2020) Cycling power outputs predict functional threshold power and maximum oxygen uptake. J strength Cond Res. https://doi.org/10.1519/JSC.0000000000002253
Wasserman K, Hansen JE, Sue DY, et al (2011) Principles of exercise testing and interpretation: including pathophysiology and clinical applications: fifth edition
Se G, Bc R, Aj W et al (2001) Validity and reliability of combining three methods to determine ventilatory threshold. Med Sci Sports Exerc 33:1841–1848. https://doi.org/10.1097/00005768-200111000-00007
Lacour JR, Padilla-Magunacelaya S, Chatard JC et al (1991) Assessment of running velocity at maximal oxygen uptake. Eur J Appl Physiol Occup Physiol 622(62):77–82. https://doi.org/10.1007/BF00626760
Swets JA (1988) Measuring the accuracy of diagnostic systems. Sci Sci. https://doi.org/10.1126/science.3287615
Feldmann A, Erlacher D (2021) Critical oxygenation: Can muscle oxygenation inform us about critical power? Med Hypotheses 150:110575. https://doi.org/10.1016/J.MEHY.2021.110575
Lacour JR (2011) Activité musculaire et dépense d’énergie. Rev Mal Respir 28(10):1278–1292. https://doi.org/10.1016/j.rmr.2011.06.014
Jones AM, Vanhatalo A, Burnley M et al (2010) Critical power: implications for determination of VO2max and exercise tolerance. Med Sci Sports Exerc 42:1876–1890. https://doi.org/10.1249/MSS.0B013E3181D9CF7F
Fontana FY, Keir DA, Bellotti C et al (2015) Determination of respiratory point compensation in healthy adults: Can non-invasive near-infrared spectroscopy help? J Sci Med Sport. https://doi.org/10.1016/j.jsams.2014.07.016
Calbet JAL, Gonzalez-Alonso J, Helge JW et al (2007) Cardiac output and leg and arm blood flow during incremental exercise to exhaustion on the cycle ergometer. J Appl Physiol. https://doi.org/10.1152/japplphysiol.01281.2006
Murias JM, Spencer MD, Keir DA, Paterson DH (2013) Systemic and vastus lateralis muscle blood flow and O2 extraction during ramp incremental cycle exercise. Am J Physiol - Regul Integr Comp Physiol. https://doi.org/10.1152/ajpregu.00016.2013
Poole DC, Schaffartzik W, Knight DR et al (1991) Contribution of exercising legs to the slow component of oxygen uptake kinetics in humans. J Appl Physiol. https://doi.org/10.1152/jappl.1991.71.4.1245
Di Prampero PE, Ferretti G (1999) The energetics of anaerobic muscle metabolism: A reappraisal of older and recent concepts. Respir Physiol. https://doi.org/10.1016/S0034-5687(99)00083-3
Colosio AL, Caen K, Bourgois JG, Boone J, Pogliaghi S (2020) Bioenergetics of the VO2 slow component between exercise intensity domains. Eur J Physiol 427:1447–1456
Calaine Inglis E, Iannetta D, Murias JM (2017) The plateau in the NIRS-derived [HHb] signal near the end of a ramp incremental test does not indicate the upper limit of O2 extraction in the vastus lateralis. Am J Physiol - Regul Integr Comp Physiol. https://doi.org/10.1152/ajpregu.00261.2017
Chamari K, Padulo J (2015) ‘Aerobic’ and ‘Anaerobic’ terms used in exercise physiology: a critical terminology reflection. Sport Med - Open. https://doi.org/10.1186/s40798-015-0012-1
Iannetta D, Qahtani A, Mattioni Maturana F, Murias JM (2017) The near-infrared spectroscopy-derived deoxygenated haemoglobin breaking-point is a repeatable measure that demarcates exercise intensity domains. J Sci Med Sport. https://doi.org/10.1016/j.jsams.2017.01.237
Casey DP, Joyner MJ (2012) Compensatory vasodilatation during hypoxic exercise: Mechanisms responsible for matching oxygen supply to demand. J Physiol 590:6321–6326
Boone J, Bouckaert J, Barstow TJ et al (2012) Influence of priming exercise on muscle deoxy[Hb + Mb] during ramp cycle exercise. Eur J Appl Physiol. https://doi.org/10.1007/s00421-011-2068-z
Harms CA, Babcock MA, McClaran SR et al (1997) Respiratory muscle work compromises leg blood flow during maximal exercise. J Appl Physiol. https://doi.org/10.1152/jappl.1997.82.5.1573
Keir DA, Pogliaghi S, Murias JM (2018) The Respiratory Compensation Point and the Deoxygenation Break Point Are Valid Surrogates for Critical Power and Maximum Lactate Steady State. Med Sci Sports Exerc 50(11):2375–2378. https://doi.org/10.1249/mss.0000000000001698
Inglis EC, Iannetta D, Keir DA, Murias JM (2020) Training-induced changes in the respiratory compensation point, deoxyhemoglobin break point, and maximal lactate steady state: Evidence of equivalence. Int J Sports Physiol Perform. https://doi.org/10.1123/ijspp.2019-0046
Hunter GR, Bamman MM, Larson-Meyer DE et al (2005) Inverse relationship between exercise economy and oxidative capacity in muscle. Eur J Appl Physiol. https://doi.org/10.1007/s00421-005-1370-z
Galán-Rioja MÁ, González-Mohíno F, Poole DC, González-Ravé JM (2020) Relative proximity of critical power and metabolic/ventilatory thresholds: systematic review and meta-analysis. Sport Med 50(10):1771–1783. https://doi.org/10.1007/s40279-020-01314-8
Skovereng K, Ettema G, Van Beekvelt M (2017) The effect of cadence on shank muscle oxygen consumption and deoxygenation in relation to joint specific power and cycling kinematics. PLoS ONE. https://doi.org/10.1371/journal.pone.0169573
Funding
Open Access funding provided thanks to the CRUE-CSIC agreement with Springer Nature. This study has been supported by the Government of Extremadura with funding from the European Regional Development Fund undergrant (Ref: GR21189).
Author information
Authors and Affiliations
Contributions
GO and AG contributed to the conception of the study. AV, RT and GO designed and reviewed the protocol of the study. AG performed the data collection. AV and AG organised the database. AV and AG performed the statistical analysis. AV and RT wrote the first draft of the manuscript. AV, RT and GO wrote sections of the manuscript. RT and GO supervised the project. All authors contributed to manuscript revision, read, and approved the submitted version.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Ethical approval
The study was carried out in accordance with the Helsinki Declaration and approved by the Bio-Ethical Committee of the University of Extremadura with N° registration code: 131/2018.
Informed consent
A signed consent was obtained from each subject prior to their participation.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Vasquez-Bonilla, A.A., González-Custodio, A., Timón, R. et al. A proposal to identify the maximal metabolic steady state by muscle oxygenation and VO2max levels in trained cyclists. Sport Sci Health 19, 919–927 (2023). https://doi.org/10.1007/s11332-022-00985-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11332-022-00985-2