
Abstract
Purpose
To correlate in COVID-19 pneumonia CT-based semi-quantitative score of pulmonary involvement with high serum levels of KL-6, a biomarker of disease severity.
Methods
Between March 28 to May 21, 2020, 196 patients with strong suspicion of SARS-CoV-2 were evaluated with RT-PCR for SARS-CoV-2, chest CT scan and blood test, including KL-6 serum protein, in our Emergency Unit. The final population included only patients who underwent blood sampling for KL-6 within 5 days from CT scan (n = 63), including n = 37 COVID-19-positive patients and n = 26 with negative RT-PCR testing for SARS-CoV-2 (control group). A semi-quantitative CT score was calculated based on the extent of lobar involvement (0:0%; 1, < 5%; 2:5–25%; 3:26–50%; 4:51–75%; 5, > 75%; range 0–5; global score 0–25).
Results
CT score was significantly correlated with serum value of KL-6 (r = 27, p = 0.035). This correlation was also present in COVID-19 positive patients (r = 0.423, p = 0.009) and CT score median value was significantly higher in patients with high KL-6 value (> 400 U/mL; 12.00, IQR 5.00-18.00, p-value 0.027). In control group, no statistically significant correlation was found between CT score and KL-6 value and CT score was higher in patients with high KL-6, although this difference was not statistically significant (5.00, IQR:1.75–8.00 versus 3.50, IQR:2.00–6.50). "Crazy paving" at the right upper (n = 8; 61.5%) and middle lobe (n = 4; 30.8%) and "consolidation" at the middle lobe (n=5; 38.5%) were observed in COVID-19 group with a significant difference between patients with high KL-6 value.
Conclusion
CT score is highly correlated with KL-6 value in COVID-19 patients and might be beneficial to speed-up diagnostic workflow in symptomatic cases.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
New coronavirus pneumonia (COVID-19) has emerged since December 2019, and the World Health Organization declared a global health emergency on January 30, 2020 [1]. Nearly two years after the outbreak of the pandemic, there have been close to 430 million confirmed cases of COVID-19 worldwide, including more than 5.5 million deaths [2].
The most common clinical symptoms at presentation are fever and cough in addition to other nonspecific symptoms including dyspnea, headache, muscle aches and fatigue, as well as many non-pulmonary manifestations, such as diarrhea and muscle soreness and neurological impairment. Additionally, many patients have no clinical symptoms, this being one of the causes of the virus spreading [3,4,5,6].
Septic shock, acute respiratory distress syndrome, disseminated intravascular coagulation (DIC), and multi-organ failure are considered the most severe forms of this disease [7]. The case-fatality rate is higher among patients with preexisting disease, reaching about: 10.5% for cardiovascular disease, 7.3% for diabetes, 6.3% for chronic respiratory disease [8, 9].
Disease behavior is very heterogeneous and unpredictable, thus necessitating the identification of biomarkers that can assess the course of the disease. This purpose has been addressed in particular by laboratory biomarkers because of their relatively easy accessibility despite mainly obtaining nonspecific results. An increased D-dimer level is the most common laboratory finding in hospitalized patients with Sars-Cov2 infection [10]. Moreover, ferritin has been found to be drastically altered in COVID-19 patients with severe disease [11]. Several reports have also shown that vitamins D and K, which have so far been examined in neoplastic diseases, are dramatically altered in COVID-19 patients [12, 13].
What is emerging from recent literature is how the Krebs von den Lungen-6 (KL-6), a glycoprotein secreted by type II alveolar pneumocytes and bronchiolar epithelial, can be a useful biomarker for assessing disease severity of COVID-19 pneumonia [14]. Indeed, in COVID-19 critically ill patients requiring mechanical ventilation or intensive therapy, KL-6 serum level is increased. This biomarker has already been used to evaluate the prognosis of various interstitial lung diseases (ILDs), including idiopathic pulmonary fibrosis (IPF) [15,16,17]. Recently, it has been proposed as useful tool to evaluate acute respiratory distress syndrome (ARDS) and infective pneumonia, like severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) [14].
Computed tomography (CT) has a high sensitivity in SARS-CoV-2 patients; it is widely used to aid patient management being the reference diagnostic modality in pulmonary involvement assessment and in patient stratification [18].
Some authors, such as Pan et al. and Francone et al., have proposed a very useful CT score for a semiquantitative assessment of disease extension [19, 20].
Moreover, there are significant correlations between the degree of lung inflammation and the main clinical symptoms and laboratory findings [21].
However, to our knowledge, there are not many scientific evidences of correlation between CT score and KL-6 value during the course of COVID-19 disease.
The primary objective of this retrospective study in COVID-19 patients is to validate the possible role of KL-6 as a biomarker of disease severity, comparing KL-6 levels with CT images based on the semiquantitative score.
Methods
Patients selection criteria
Between March 28, 2020, and May 21, 2020, we retrospectively enrolled 196 consecutive patients with strong suspicion of COVID-19 interstitial pneumonia presenting to our Emergency Unit. This single-center study was approved by the Ethics Committees of our Institute (protocol number CE 109/2020), and written informed consent was waived due to the retrospective nature of the study.
Patients with highly suspected COVID-19 pneumonia were included, in accordance with internal guideline criteria.
All subjects underwent reverse transcriptase polymerase chain reaction (RT—PCR) detection test for SARS-CoV-2, chest CT scan and blood test including KL-6, antibodies COVID-19 (Ab COVID-19 BAU/mL, creatinine (n.v. 0.70–120 mg/dL), Interleukin-6 (IL-6; n.v. 1.5–7.0 pg/mL), D-dimer (n.v. 50–420 ng/mL) and platelets count (n.v. 150–450 × 109/l), prothrombin time (PT; n.v. 11–16 s) with derived measures as percent prothrombin activity (PT%; n.v. 70–120) and international normalized ratio (INR; n.v. 0.81–120).
After RT-PCR detection test for SARS-CoV-2, patients were divided into two groups: COVID-19-positive group (N = 162) and non-COVID-19 group (N = 34).
In subsequent analyses, to avoid changes in the inflammatory panel due to disease progression, we included only patients who underwent blood sampling for KL-6 within 5 days from CT scan.
The final population consisted of 63 patients, including 37 COVID-19-positive patients and 26 with negative RT-PCR testing for SARS-CoV-2.
The flowchart of the patient selection process is shown in Fig. 1.

Flowchart of the patient search and selection process
KL-6 and IL-6 detection
A blood sample was sent to the laboratory for the determination of KL-6 and IL-6 levels, at the first admission to the Emergency Department, before starting therapy.
KL-6 serum values were determined on a Lumipulse G1200 (Fujirebio-Europe, Gent, Belgium), using the LUMIPULSE G KL-6-II kit (Fujirebio, Tokyo, Japan). The principle of the method is agglutination of sialylated carbohydrate antigen in samples with KL-6 monoclonal antibody through antigen–antibody reaction. KL-6 detection range considered is between 50 and 10.000 U/mL, with intra-assay CV of < 4.4% and inter-assay CV of < 10%, and as a clinical cut-off we considered 400 U/mL. This value was established considering the mean value in a population of blood donors belonging to the transfusion center of our Institute, enrolled consecutively. We considered the value present at the 95th percentile on one hundred samples.
All standard biochemical analyses were performed by Elecysis Roche Instruments.
IL-6 detection range was between 1.5 and 5000 pg/mL; as a clinical cut-off, we considered 7.0 pg/mL.
CT protocol and imaging analysis
A multidetector CT scanner (Somatom Sensation 64; Siemens Healthineers) was used for examinations. All patients were instructed in breath-holding.
The following acquisition parameters have been used: 120 kV, 100 mAs, pitch 1.5 and collimation 0.6 mm; all images were reconstructed with a slice thickness of 1.00 mm, 512 × 512 mm, with both a sharp and soft kernel. Coronal and sagittal multiplanar reconstructions were also available in all cases.
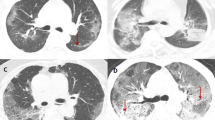
CT images were reviewed by two radiologists (L.M., P.R.) with at least 20-year experience in chest imaging, in consensus. For all patients, CT images were evaluated considering the presence of three thoracic CT patterns: (i) ground glass opacity, (ii) consolidation, (iii) crazy paving in agreement with the international standard nomenclature defined by the Fleischner Society glossary and previous literature on viral pneumonia [22,23,24][Fig. 2].

Chest CT findings of coronavirus disease 2019 (COVID-19): a ground glass opacity (GGO); b crazy-paving pattern (GGO and inter- and intralobular septal thickening); c consolidation
A semiquantitative evaluation of lung involvement was calculated for each of the 5 lobes according to Francone et al. [19] as follows: 0, no involvement; 1, < 5% involvement; 2, 5–25% involvement; 3, 26–50% involvement; 4, 51–75% involvement; and 5, > 75% involvement. The resulting global CT score was the sum of each individual lobar score (0 to 25) [Fig. 3].

Example of a semiquantitative CT score in a 38-year-old with SarS-CoV-2 pneumonia and a global CT score value of 21
Pleural effusion, fibrosis, single/multiple nodules with halo sign, lymphadenopathy, air bronchogram, bronchial thickening and bronchiectasis have also been reported.
Statistical analysis
Spearman’s rho coefficient was used to evaluate the linear relationship between the CT score and the KL-6 value. Data are expressed as median and interquartile range (IQR) for continuous variables and frequencies for categorical ones. Comparison between two groups was performed by Chi-square test or Mann–Whitney U test as appropriate. Spearman’s correlation index was used to assess the relationship between continuous measurements. A logistic regression model was used to determine the possible value of CT score in predicting the risk of critical illness in COVID-19 patients. All tests were two-tailed, and a value of P < 0.05 was considered as statistically significant. Analyses were performed using R version 4.0.1 (The R Project for Statistical Computing).
Results
Population
The final population included n = 37 COVID-19-positive patients (18 male, 19 female; median age 67) and n = 26 patients (10 male, 16 female; median age 74.50) with a negative RT-PCR test for SARS-CoV-2. Baseline characteristics are summarized in Table 1. In the COVID-19 group, 64% had KL-6 values > 400 U/mL (24/37 patients). As regards the other serum proteins, we found a significant association between D-Dimer and COVID-19 patients. The median value of D-dimer in the COVID-19-positive group was 4409 ng/mL, whereas in the non-COVID19 control group it was 1116,50 ng/mL, with a statistically significant difference between the two groups (p = 0.004).
CT score and KL-6 protein
CT score correlated with the KL-6 value in the whole population (rho = 27, p-value 0.035) (Fig. 4a). When considering only COVID-19-positive patients, this correlation was also present (rho = 0.423, p-value 0.009) (Fig. 4b). No statistically significant correlation was found between CT score and KL-6 value in the non-COVID-19 group alone (Fig. 4c).

Comparisons between CT scores and the KL-6 value in both groups of patients. Red dots in only COVID-19 patients and black dots in only non-COVID-19 patients
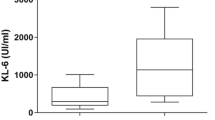
In COVID-19-positive group, CT score median value was significantly higher in patients with KL-6 > 400 U/mL than in patients KL-6 ≤ 400 U/mL (12.00, IQR 5.00–18.00 versus 4.50, IQR:3.75–7.25; p-value 0.027) (Fig. 5a). Also, in non-COVID-19 group CT score was higher in patients with KL-6 > 400 U/mL patients than in patients with KL-6 ≤ 400 U/mL patients, although this difference was not statistically significant (5.00, IQR:1.75–8.00 versus 3.50, IQR:2.00–6.50, p-value 0.716) (Fig. 5b).

Box plot of CT score stratified by KL-6 ≤ 400 and KL-6 > 400. a COVID-19-positive patients, and b non-Covid-19 group. Lines in the box represent the median (the thickest line), 25th, and 75th percentiles (the thinnest lines, below and above the median, respectively), and the whiskers (error bars) below and above the box indicate the 10th and 90th percentiles, respectively
Imaging features
Concerning CT findings, we observed a significant difference in radiological patterns between patients with KL-6 ≤ 400 U/mL and KL-6 > 400 U/mL in COVID-19-positive group. In particular, in COVID-19-positive patients with KL-6 > 400 U/mL the significant radiological patterns were "crazy paving" at the right upper (n = 8; 61.5%) and middle lobe (n = 4; 30.8%) and "consolidation" at the middle lobe (n = 5; 38.5%) (Table 2).
Discussion
Since the outbreak of the COVID-19 pandemic, several studies have been published on the role of inflammatory biomarkers to select different patient groups based on the impact of infection and prediction of outcome; however, these have often been nonspecific or in common with other diseases.
More recently, serum KL-6 has also been investigated and found to be a prognostic biomarker of COVID-19 disease, with increased values in more severely affected cases [17, 25].
Classifying the degree of disease considering not only clinical but also radiological or laboratory parameters is a crucial issue due to the lack of specific criteria. Several radiological studies highlight the primary role of CT in classifying disease severity, particularly in assessing the extent of parenchymal involvement by constructing CT scores, as suggested by some authors [19, 20].
In our study, we aimed to find a correlation between serum KL-6 protein and CT disease severity score by evaluating both a group of patients with Sars-Cov-2 and a control group with suggestive symptoms but negative RT-PCR test.
As a first result, we found a positive correlation between serum KL-6 values and CT score in the group of COVID-positive patients. Specifically, patients with higher values of the serum biomarker (> 400 U/ mL) were associated with a greater extent of parenchymal disease, with median CT score value of 12, whereas in patients with lower KL-6 values (< 400 U/mL) the median CT score value was 4.5 (p-value 0.027). Moreover, we also tested for a possible correlation between KL-6 values and CT score in the control group; however, we found no significant association in these patients (p-value 0.716).
A retrospective longitudinal analysis of 166 COVID-19 patients by Deng K. et al. showed significantly higher KL-6 values in severe/critical COVID-19 patients (n = 17) than in mild COVID-19 patients (n = 149) [26]. Moreover, in this study, the late value of serum KL-6 (+ 7 days; N = 80) was significantly associated with the presence of areas of lung injury on CT. In a subsequent paper, Varble N. al. sought to investigate and characterize the associations between clinical, laboratory, and imaging characteristics of asymptomatic and pre-symptomatic patients with SARS-CoV-2, finding that serum KL-6 value was one of the best parameters to distinguish asymptomatic patients with COVID-19-related CT infiltrates from asymptomatic patients without CT changes [27]. Finally, in more recent work by Arnold DT et al., the authors found that patients with abnormal CT scans at 12 weeks had significantly higher KL-6 levels during recovery than the group with negative CT [28].
In agreement with the above-mentioned works, we also found a significant association between KL-6 elevation and the presence of radiological alterations. However, differently from them, we also quantified the degree of CT lesion extension using a semiquantitative score, finding that increased KL-6 was associated not only with the presence but also with a greater extent of parenchymal lesions (CT score higher than 12).
As a second result, in our study we also found a significant difference in D-dimer values in the two populations, with higher values in the COVID-19 group (p = 0.004). This finding is well known in the literature, and our study is a further confirmation of the close relationship between COVID-19 infection, D-dimer value, and thus thrombotic risk, although the underlying mechanism needs further investigation [29, 30].
In our study, an interesting finding is a greater frequency of crazy paving pattern and consolidations involving the right upper and middle lobe in COVID-19-positive patients with KL-6 > 400 U/mL. According to some authors, these radiological findings may refer to a more severe and late state of disease [19]. The data confirm that a high KL-6 value can really correlate with a more severe state of the disease [31].
Our study has some limitations. First, it is a single-center study with a small cohort of patients. In fact, because patients referred to our unit were evaluated in emergency during a pandemic, not all clinical and laboratory data were always available.
Second, we did not make correlations between radiological and laboratory data with clinical outcomes; after initial admission to our emergency unit, the management of these patients was deferred to other departments or to the attending physician, so these data were not available for the entire cohort.
Conclusion
Our preliminary findings showed that the dynamic profile of KL-6 in COVID-19-positive patients correlates closely with CT lung severity, as determined by a semiquantitative score.
Further studies with larger populations and validation with clinical outcomes are needed to confirm our results, but serum KL-6 value at baseline may represent an early biomarker of lung disease extension in patients with Sars-Cov2 infection.
Data availability
The datasets analyzed during this study are available from the corresponding author upon reasonable request.
Code availability
Not applicable.
Abbreviations
- COVID-19:
-
Coronavirus disease 2019
- SARS-CoV-2:
-
Severe acute respiratory syndrome coronavirus 2
- DIC:
-
Disseminated intravascular coagulation
- KL-6:
-
Krebs von den Lungen-6
- ILDs:
-
Interstitial lung diseases
- IPF:
-
Idiopathic pulmonary fibrosis
- PT:
-
Prothrombin time
- INR:
-
International normalized ratio
- IL-6:
-
Interleukin-6
- CT:
-
Computer tomography
- CARDS:
-
COVID-19-related acute respiratory distress syndrome
- IQR:
-
Interquartile Range
- RT-PCR:
-
Retrotrascriptase polymerase chain reaction
References
Mahase E (2020) China coronavirus: WHO declares international emergency as death toll exceeds 200. BMJ m408. https://doi.org/10.1136/bmj.m408
World Health Organization WHO Coronavirus (COVID-19) Dashboard
Zhu Y, Li C, Chen L et al (2018) A novel human coronavirus OC43 genotype detected in mainland China. Emerg Microbes Infect 7:1–4. https://doi.org/10.1038/s41426-018-0171-5
Yang X-L, Hu B, Wang B et al (2016) Isolation and characterization of a novel bat coronavirus closely related to the direct progenitor of severe acute respiratory syndrome coronavirus. J Virol 90:3253–3256. https://doi.org/10.1128/JVI.02582-15
Zhu N, Zhang D, Wang W et al (2020) A novel coronavirus from patients with pneumonia in China, 2019. N Engl J Med 382:727–733. https://doi.org/10.1056/NEJMoa2001017
Wang C, Horby PW, Hayden FG, Gao GF (2020) A novel coronavirus outbreak of global health concern. The Lancet 395:470–473. https://doi.org/10.1016/S0140-6736(20)30185-9
Hui DS, Azhar I, E, Madani TA, et al (2020) The continuing 2019-nCoV epidemic threat of novel coronaviruses to global health: the latest 2019 novel coronavirus outbreak in Wuhan, China. Int J Infect Dis 91:264–266. https://doi.org/10.1016/j.ijid.2020.01.009
Malik YS, Sircar S, Bhat S et al (2020) Emerging novel coronavirus (2019-nCoV)—current scenario, evolutionary perspective based on genome analysis and recent developments. Vet Quart 40:68–76. https://doi.org/10.1080/01652176.2020.1727993
Wu Z, McGoogan JM (2020) Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the Chinese center for disease control and prevention. JAMA 323:1239. https://doi.org/10.1001/jama.2020.2648
Xue M, Zheng P, Bian X et al (2020) Exploration and correlation analysis of changes in Krebs von den Lungen-6 levels in COVID-19 patients with different types in China. Biosci Trends 14:290–296. https://doi.org/10.5582/bst.2020.03197
Qeadan F, Tingey B, Gu LY et al (2021) Prognostic values of serum ferritin and D-dimer trajectory in patients with COVID-19. Viruses 13:419. https://doi.org/10.3390/v13030419
Laird E, Rhodes J, Kenny RA (2020) Vitamin D and inflammation: potential implications for severity of COVID-19. Ir Med J 113:81
Dofferhoff ASM, Piscaer I, Schurgers LJ et al (2021) Reduced vitamin K status as a potentially modifiable risk factor of severe coronavirus disease 2019. Clin Infect Dis 73:e4039–e4046. https://doi.org/10.1093/cid/ciaa1258
d’Alessandro M, Cameli P, Refini RM et al (2020) Serum KL-6 concentrations as a novel biomarker of severe COVID-19. J Med Virol 92:2216–2220. https://doi.org/10.1002/jmv.26087
Ishikawa N, Hattori N, Yokoyama A, Kohno N (2012) Utility of KL-6/MUC1 in the clinical management of interstitial lung diseases. Respir Investig 50:3–13. https://doi.org/10.1016/j.resinv.2012.02.001
Yokoyama A, Kondo K, Nakajima M et al (2006) Prognostic value of circulating KL-6 in idiopathic pulmonary fibrosis. Respirology 11:164–168. https://doi.org/10.1111/j.1440-1843.2006.00834.x
Awano N, Inomata M, Kuse N et al (2020) Serum KL-6 level is a useful biomarker for evaluating the severity of coronavirus disease 2019. Respir Investig 58:440–447. https://doi.org/10.1016/j.resinv.2020.07.004
Ai T, Yang Z, Hou H et al (2020) Correlation of chest CT and RT-PCR testing for coronavirus disease 2019 (COVID-19) in China: a report of 1014 cases. Radiology 296:E32–E40. https://doi.org/10.1148/radiol.2020200642
Francone M, Iafrate F, Masci GM et al (2020) Chest CT score in COVID-19 patients: correlation with disease severity and short-term prognosis. Eur Radiol 30:6808–6817. https://doi.org/10.1007/s00330-020-07033-y
Pan F, Ye T, Sun P et al (2020) Time course of lung changes at chest CT during recovery from coronavirus disease 2019 (COVID-19). Radiology 295:715–721. https://doi.org/10.1148/radiol.2020200370
Wu J, Wu X, Zeng W et al (2020) Chest CT findings in patients with coronavirus disease 2019 and its relationship with clinical features. Invest Radiol 55:257–261. https://doi.org/10.1097/RLI.0000000000000670
Franquet T (2011) Imaging of pulmonary viral pneumonia. Radiology 260:18–39. https://doi.org/10.1148/radiol.11092149
Koo HJ, Lim S, Choe J et al (2018) Radiographic and CT features of viral pneumonia. Radiographics 38:719–739. https://doi.org/10.1148/rg.2018170048
Hansell DM, Bankier AA, MacMahon H et al (2008) Fleischner society: glossary of terms for thoracic imaging. Radiology 246:697–722. https://doi.org/10.1148/radiol.2462070712
Nakamura H, Miyagi K, Otsuki M et al (2021) Serum KL-6 can distinguish between different phenotypes of severe COVID-19. J Med Virol 93:158–160. https://doi.org/10.1002/jmv.26268
Deng K, Fan Q, Yang Y et al (2021) Prognostic roles of KL-6 in disease severity and lung injury in COVID-19 patients: a longitudinal retrospective analysis. J Med Virol 93:2505–2512. https://doi.org/10.1002/jmv.26793
Varble N, Blain M, Kassin M et al (2021) CT and clinical assessment in asymptomatic and pre-symptomatic patients with early SARS-CoV-2 in outbreak settings. Eur Radiol 31:3165–3176. https://doi.org/10.1007/s00330-020-07401-8
Arnold DT, Donald C, Lyon M et al (2021) Krebs von den Lungen 6 (KL-6) as a marker for disease severity and persistent radiological abnormalities following COVID-19 infection at 12 weeks. PLoS ONE 16:e0249607. https://doi.org/10.1371/journal.pone.0249607
Kermali M, Khalsa RK, Pillai K et al (2020) The role of biomarkers in diagnosis of COVID-19: a systematic review. Life Sci 254:117788. https://doi.org/10.1016/j.lfs.2020.117788
Rostami M, Mansouritorghabeh H (2020) D-dimer level in COVID-19 infection: a systematic review. Expert Rev Hematol 13:1265–1275. https://doi.org/10.1080/17474086.2020.1831383
Tian S, Xiong Y, Liu H et al (2020) Pathological study of the 2019 novel coronavirus disease (COVID-19) through postmortem core biopsies. Mod Pathol 33:1007–1014. https://doi.org/10.1038/s41379-020-0536-x
Funding
Open access funding provided by Università degli Studi di Roma La Sapienza within the CRUI-CARE Agreement. No funding was received for conducting this study.
Author information
Authors and Affiliations
Contributions
Dr. Manganaro Lucia and Dr. Emanuela Anastasi contributed equally to the study as first authors.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethics approval
This single-center retrospective study was approved by the Ethics Committees of our Institute with protocol number CE 109/2020. The procedures used in this study adhere to tenets of the Declaration of Helsinki.
Consent to participate
Informed consent was waived because it is not required for images (CT).
Consent for publication
Informed consent was waived because of the use of anonymous clinical data.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Dr. Anastasi Emanuela and Dr. Manganaro Lucia are First co-authors.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Anastasi, E., Manganaro, L., Guiducci, E. et al. Association of serum Krebs von den Lungen-6 and chest CT as potential prognostic factors in severe acute respiratory syndrome SARS-CoV-2: a preliminary experience. Radiol med 127, 725–732 (2022). https://doi.org/10.1007/s11547-022-01504-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11547-022-01504-6