
Abstract
Background
Falls and fall-related injuries are common in community-dwelling older persons. Longitudinal data on effective fall prevention programs are rare.
Objective
Therefore, we evaluated a 4-months multi-component exercise fall prevention program in a primary care setting on long-term effects over 24 months on falls and concomitant injuries in older community-dwelling persons with high risk of falling.
Design and Setting
In the Prevention of Falls (PreFalls) study, forty general practitioners in Germany were cluster-randomized (1:1) into an intervention group (IG) or control group (CG). Three hundred seventy-eight independently living people with high risk of falling (78.1 ± 5.9 years, 75% women) were assigned to IG (n = 222) or CG (n = 156).
Intervention and Measurements
Patients in IG took part in a 4-months multi-component exercise program comprising strength and balance exercises (28 sessions); patients in CG received no intervention. Primary outcome measure was number of falls over 24 months, analyzed by a patient-level, linear mixed Poisson model. Secondary endpoints were number of fall-related injuries, changes in physical function, fear of falling, and mortality.
Results
After 24 months, the IG demonstrated significantly fewer falls (IRR = 0.63, p = 0.021), injurious falls (IRR = 0.69, p = 0.034), and less fear of falling (p = 0.005). The mortality rate was 5.0% in IG and 10.3% in CG (HR = 0.51, 95% CI: 0.24 to 1.12; p = 0.094).
Conclusions
In older community-dwelling persons with high risk of falling, a short-term multi-component exercise intervention reduced falls and injurious falls, as well as fear of falling over 24 months.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
INTRODUCTION
Falls and fall-related injuries are common in community-dwelling older persons.1,2 Injurious falls pose an immense burden on the public health care system,3,4 as they are related to disability, admission to nursing homes, and even higher mortality.2,3,5
Risk factors for falls can be grouped into intrinsic (related to the individual, e.g., skills in balance or strength), extrinsic (related to the environment), and behavioral domains (individual beliefs, cognition decision-making).6,7 Fall-related psychological concerns (FrPCs) are reported up to 83% of community-dwelling older persons.8 Fear of falling (FoF) has been linked to cautious gait,9 reduced physical activity level due to activity avoidance, and social withdrawal.10,11
Multi-component exercise interventions are effective in reducing the risk of falls.6,12,13 They have included at least two of the risk domains (intrinsic, extrinsic, behavioral) and follow individualized intensity approaches based on risk assessment. Most effective multi-component exercise programs have included balance and strength exercise,1,12 demonstrating greater effects if the program lasts at least 3 months.12
However, the long-term effects of these programs are scarce as most follow-up time-periods have lasted for 6–12 months.2,6
General practitioners (GP) are in an ideal position to motivate their patients to participate in fall prevention programs,1415 though such opportunities are often missed.16 Therefore, we conducted a longitudinal, cluster-randomized controlled study (PreFalls; Prevention of Falls) in primary care settings. The primary hypothesis of the PreFalls trial was that a complex multi-component exercise intervention program (intervention group = IG) — consisting of a 4-months group exercise in combination with an individualized home-based training program — significantly reduces the number of falls per individual in older patients (≥65 years). After 4 months and 12 months, significant improvements were seen regarding physical function, reduction in FoF, and lower incidence of falls and fall-related injuries in older adults in IG compared to the control group (CG).17,18
We present results over a follow-up period of 24 months compared to those not receiving the intervention (CG). Secondary endpoints included the incidence of injurious falls, physical function, fear of falling, and mortality.
METHODS
Trial Design and Participants
The study protocol has been previously published including recruitment strategies.17,19 Briefly, we recruited 40 GPs and practice patients with risk factors for falls. Inclusion criteria were community-dwelling setting, age ≥ 65 years, and ≥1 fall risk criterion (≥1 fall in the past 12 months, Timed-up-and-Go-Test or Chair-Stand-Test >10 s, subjective or objective balance deficits or fear of falling). Exclusion criteria included dependence or suffering from physical or mental restrictions that did not allow the participation in an exercise program or the assessment of risk of falling.
Objectives, Outcomes
The primary endpoint of PreFalls was the difference in number of falls in community-dwelling older people between IG and CG over a period of 24 months.19 The number of falls over 24 months was documented by a daily falls calendar. Secondary outcomes were fall-related injuries, changes in physiological risk factors of falling (mainly balance, strength, and mobility), changes in fear of falling, and mortality over the period of 24 months.
The study protocol was approved by the ethics committee, School of Medicine, University Hospital “rechts der Isar,” Technical University of Munich, Munich, Germany (approval number 2386/09). The study design follows the fundamental principles of the Helsinki Declaration. Only data from people with written consent were included in the pseudonymized data analysis. No changes were made after ethics approval and trial commencement.
Intervention
Details of our 4-month intervention have been previously published.17,19 Briefly, participants in the IG were offered a combination of 28 supervised and unsupervised sessions. Sixteen sessions, once per week for 60 min, were supervised, and the participants were advised to add at least one unsupervised session starting at week five.17 The multi-component exercise intervention included progressive strength, challenging balance and gait training, behavioral aspects, self-management program, and perceptual and functional training conducted by a trained fall prevention instructor. The participants received brochures for home training including description of the different exercises and pictures. The CG received no intervention.
Sample Size Calculation and Randomization
The sample size and power calculation were based on the proportion of individuals with at least one fall during a 12-month follow-up period.20 An intra-cluster correlation coefficient of 0.02 was assumed and a cluster size of 10 was considered to be realistic. Based on 80% power, a two-sided significance of 5%, 40 clusters, and 382 individuals were felt sufficient to demonstrate a clinically meaningful reduction of about 20% .19,21,22
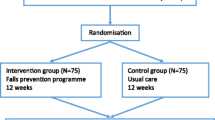
After recruitment by the study coordinators, the GPs were randomized by a biostatistician, not otherwise involved in the trial, using computer-generated random numbers to intervention or control groups (1:1). Then, the GP recruited patients according to the defined inclusion and exclusion criteria (Fig. 1).19 Masking of participants was not feasible as all patients knew whether or not they participated in an exercise intervention.
Clinical Assessment
All data were collected by the GP and their trained assistants, e.g., demographic data, comorbidities, and medication at the beginning, after the 4 months of active intervention, and after 12- and 24-months follow-up (final examination). Results were mailed to the regional coordination center.
Assessment of Falls and Fall-Related Injuries
A fall was defined as “an unexpected event, in which the participant comes to rest on the ground floor, or lower level”.23 A faller was defined as a person, who reported more than one fall per year or had at least one fall with a fall-related injury.
Falls were documented by patients in IG and CG into daily falls calendar over the full study period (24 months).18,19 Monthly, the falls calendars were sent to the study coordinators by the participants of the IG and CG. If a fall was reported, further information about fall-related injuries was collected by structured telephone interviews.
Fall Risk Assessment and Mortality
Physical Fall Risk Assessment
Physical fall risk was assessed by a standardized protocol. Function and mobility were measured by the “Timed-Up-and-Go-Test” (TUG) over the distance of 3 m, as fast but safely at possible.24,25 According to the “Short Physical Performance Battery” (SPPB),26 functional strength of the lower extremity was measured with the five time “Chair-Stand-Test” (CST, sit-to-stand-to-sit). The static balance was assessed by a modified Romberg test (mRomberg) with three measurements with feet positioned side by side, in semi-tandem, and in full tandem position. The participant was asked to stand in every position for 10 s. The total balance time in all three tests was used (0 to 30 s) as described previously.19
Fear of Falling
Fear of falling was assessed by the German version of the Falls Efficacy Scale-International (FES-I).27 This questionnaire contains 16 questions on demanding activities in daily living inside and outside the home and social activities (“not at all concerned” (1 point) to “very concerned” (4 points)). To obtain the total score, points were summed up.28,29
Mortality
The GP has informed the study coordinators about the death of patient by mail or telephone contact.
Statistical Analysis
The number of falls and fall-related injuries during the observation period was counted from the daily falls calendar and averaged per subject. Number of falls and fall-related injuries were compared between IG and CG in a Poisson model. All patients that returned at least one diary were included in the analysis as randomized (n(IG) = 212, n(CG) = 144). To account for the cluster structure of patients nested in GP and to consider possible over-dispersion in Poisson models with rare events like falls, a mixed effects Poisson model was fitted with MCMC (Monte Carlo Markov Chain) methods. The model also was adjusted to different number of returned diaries, included as a covariate. Additionally, the odds ratio (OR) of IG vs. CG for the number of patients, who had fallen two times or more often, was calculated by a generalized mixed linear logistic regression model. The resulting odds ratio was translated into a relative risk (RR) based on the estimated marginal distributions of patients.
For each secondary outcome measure (TUG, CST, modified Romberg, FES-I), the changes in the means over time were analyzed and compared between IG and CG. We determined a three-level linear mixed effects model for continuously normal distributed outcomes to account for the GP cluster structure and the cluster structure for measurement occasions within patients. Differences in the mean changes over time are represented by the group by time-interaction effect, which was the primary interest. For all considered outcome measures a random intercept and random slope model was deemed appropriate. However, none of the investigated outcome models for secondary outcomes showed the third level of GPs as relevant (only the first level (measurement occasion) and second level (patients)) in either explaining a notable amount of variance or accomplishing independent contribution to the residuals. Hence, two-level models were sufficient to represent the data structure while preserving parsimony. Mortality was compared between groups by using a cox proportional hazards model.
Data were analyzed with R environment for statistical computing (R Foundation for Statistical Computing, Vienna, Austria).
Role of the Funding Source
The funding source had no role in the study design, data analysis, data interpretation, or manuscript preparation.
RESULTS
Baseline Characteristics
Physicians and staff members of 40 GPs were recruited and trained. Seven GPs dropped out before recruiting patients for various reasons (e.g., lack of time). Thirty-three GPs participated in this study and recruited a total of 378 patients. These patients ranged in age from 65 to 94 years (mean age 78.1 ± 5.9 years). They were mostly women (Table 1). Baseline characteristics were evenly distributed. The physical performance at baseline was higher in IG compared to the CG for the TUG (13.0 s vs. 16.2 s, p < 0.001) and the CST (17.4 s vs. 19.4 s, p = 0.024) and comparable for the mRomberg (25.3 s vs. 24.0 s, p = 0.071) (Table 1).
After 24 months, 167 patients (75.2%) in the IG and 103 patients (66%) in the CG were re-assessed (Fig. 1).

Participant Recruitment, Enrolment, and Follow-up.
Dropouts
The dropout rate in the intervention group was 24.8% with 34% dropping out in the control group. The reasons for drop out included refused further participation (n = 14), death (n = 27), poor health (n = 36), dementia (n = 4), orthopedic problems (n = 5), admission to a residential care home for older persons (n = 8), family reasons/change of residence (n = 4), and unknown (n = 10).
24-Months Results
Falls, Fall-Related Injuries, and Fallers
All patients with at least one monthly falls calendar were included (n = 212 in IG and n = 144 in CG). On average, 19.1 falls calendar over the 24-months period were obtained in IG and 18.9 in CG.
Falls
During the 24 months of follow-up, 517 falls occurred in patients in IG compared to 588 falls in patients in CG. Intervention subjects averaged 1.89 falls per year, compared to 3.11 falls per year in the control group (IRR: 0.63; 95% confidence interval (CI): 0.44 to 0.94; p = 0.021) (Table 2).
Fall-Related Injuries
Fall-related injuries were reduced by 31% in IG compared to CG (IRR: 0.69; 95% CI: 0.47 to 0.97; p = 0.034) (Table 2).
Faller
Eighty out of 212 patients in IG were fallers compared to 96 out of 144 patients in CG. The proportion of fallers were comparable between IG and CG (Table 2).
Fall Risk Assessment
After 24 months, the results in the TUG showed a minor decline of function and mobility in IG compared to CG (IG: 13.0 to 14.0; CG: 16.2 to 18.8 s, p = 0.064) (Table 3).
Strength assessment by CST revealed no group difference, but only 52% of the older adults in CG were able to perform the CST after 24 months compared to 64% in IG. No significant differences were observed in adjusted mean time needed for the mRomberg test between both groups (p = 0.221). The percentage of older adults with full test time increased in the IC from 59 to 64%, while in the CG the percentage of participants with full test time decreased from 58 to 46%.
Fear of Falling
The fear of falling level was unchanged over 24 months in IG (25.1 vs. 25.2 points) while there was a distinct increase in CG subjects (27.6 vs. 30.3 points) (p = 0.005) (Table 3).
Mortality
In IG, 11 patients out of 222 patients (5.0%) died during 24 months in contrast to 16 out of 156 patients in CG (10.3%) (HR: 0.51, 95% CI: 0.24 to 1.12; p = 0.094).
Side Effects
No side effects in connection with the multimodal exercise intervention were observed. During the training sessions, no adverse events occurred.17
DISCUSSION
We found that our 4-months intervention had sustained improvement over 2 years, with a reduction in the number of falls, fall-related injuries, and death, compared to control participants. The reduction of injurious falls is particularly important, as these types of falls pose a significant burden for the older person, endangering independence and mobility as well as health.3,4
Few studies have assessed a long follow-up of 24 months continuously monitoring falls using daily falls calendars.30,30,32 In comparison to our study, Salminen30 and Uusi-Rasi31 used a different intervention, included only women and involved younger patients. In the study by Salminen,30 no reduction of incidence of falls could be found (IRR for IG vs. CG 0.92; 95% CI: 0.72 to 1.19). The study by Uusi-Rasi31 also found no significant difference in the rate of all falls or minor injurious falls. El-Khoury32 addressed injurious falls, but also only included women, though had a longer intervention period (24 months). They found a 19% higher reduction in injurious falls in the intervention group then in the control group (HR 0.81 for IG vs. CG; 95% CI 0.67–0.99). In addition, the reduction of all falls was 12% higher in the IG then in the CG. One recently reported cluster-randomized trial on injurious fall prevention in the GP setting33 — the STRIDE study — addressed also injurious falls and mortality but used different approaches in the statistical analyses (time-to-event analysis). Their participants were older and their multifactorial intervention was provided by a specialized nurse. In contrast to our study, no daily calendars were used but telephone calls at a 4-months period. One has to keep in mind that falls are mostly self-reported and the “golden standard” until now is the monthly daily falls calendar.
Congruent with the above cited studies, the STRIDE study also found no significant reduction in injurious falls. Concentrating only on injurious falls and not including falls as well seems challenging. In the STRIDE study, 86 primary care practices were included with 5451 community-dwelling participants but still they did not find a significant reduction in injurious falls. Nevertheless, injurious falls place a heavy burden on older persons and their carers as well as on the public health care system and should be addressed next to falls without injurious.
Interestingly, the clinical improvements in fall rates we found were congruent with the mobility measure (TUG) but did not reflect changes in functional tests, e.g., CST or mRomberg. This may be explained by the fact that in the CG only 52% of the older adults were able to perform the CST after 24 months compared to 64% in IG. For balance, the percentage of older adults with full test time was 28% in CG and 45% in IG indicating a larger proportion of older adults with good balance and better physical function after 24 months. An important behavioral finding was the significant difference in fear of falling. There was a significant increase in FoF among control group participants, compared to the IG. This is important because FoF can fuel a downward spiral by causing activity avoidance, resulting in reduced physical function and quality of life.34,35 Our findings suggest that it is important for GPs to address both physical functional and behavioral risk factors.
While not powered for mortality, we observed a mortality reduction of 49% in the IG compared to CG. This is greater than found in a previous trial.32 It may be assumed that an increase in physical function could act as a prevention against mortality. This would be congruent with the research by Landi et al.35 demonstrating that physical limitation are more relevant for mortality then comorbidities.
Limitation and Strengths
There are a number of potential limitations of our study. Because we randomized GPs, this could pose a bias on the GP’s recruitment for those to be included into the exercise intervention. However, using the GPs is more real-world. In practice, GPs select patients for interventions and have regular contact with their older patients.
The GPs are uniquely poised to observe fall risk factors and to intervene. Secondly, the dramatic decrease in mortality may suggest unmeasured confounders or there could be other factors that differentially affected our two groups after the intervention period ended.
Strengths of our study are the long follow-up time of 24 months, assessment of daily falls calendars obtaining falls, and injurious falls with a mean of 19-months return rate.
A short 4-months intervention integrating physical exercise and behavioral aspects in the multi-component exercise program provided significant results in falls and especially in injurious falls.
CONCLUSIONS
In conclusion, a 4-months multi-component exercise intervention demonstrated a significant reduction in falls and injurious falls, fear of falling, and mortality over a subsequent period of 24 months. Our study also demonstrated the need for “shared treatment” in future fall prevention including GPs and exercise instructors to offer effective fall preventions programs in the living environment of older adults.
References
Hopewell S, Adedire O, Copsey BJ, Boniface GJ, Sherrington C, Clemson L, et al. Multifactorial and multiple component interventions for preventing falls in older people living in the community. Cochrane Database Syst Rev. 2018;7:Cd012221.
Guirguis-Blake JM, Michael YL, Perdue LA, Coppola EL, Beil TL. Interventions to Prevent Falls in Older Adults: Updated Evidence Report and Systematic Review for the US Preventive Services Task Force. Jama. 2018;319(16):1705-16.
Stevens JA, Corso PS, Finkelstein EA, Miller TR. The costs of fatal and non- fatal falls among older adults. Injury Prevention. 2006;12(5):290–5.
Florence CS, Bergen G, Atherly A, Burns E, Stevens J, Drake C. Medical Costs of Fatal and Nonfatal Falls in Older Adults. J Am Geriatr Soc. 2018;66(4):693-8.
Peel NM, Kassulke DJ, McClure RJ. Population based study of hospitalised fall related injuries in older people. Inj Prev. 2002;8(4):280-3.
Ganz DA, Latham NK. Prevention of Falls in Community-Dwelling Older Adults. N Engl J Med. 2020;382(8):734-43.
Todd C, Skelton D. What are the main risk factors for falls among older people and what are the most effecxtive interventions to prevent these falls? Copenhagen: WHO REgional Office for Europe; 2004.
Zijlstra G, van Haastregt, JCM., van Eijk, JTM., van Rossum, E., Stalenhoef, PA., Kempen, GIJM. Prevalence and correlates of fear of falling, and associated avoidance of activity in the general population of community-living older people. Age Ageing. 2007;36(3):304-9.
Delbaere K, Sturnieks DL, Crombez G, Lord SR. Concern about falls elicits changes in gait parameters in conditions of postural threat in older people. J Gerontol A Biol Sci Med Sci. 2009;64(2):237-42.
Vellas B, Wayne, SJ., Romero, LJ., Baumgartner, RN., Garry, PJ. Fear of falling and restriction of mobility in elderly fallers. Age Ageing. 1997;26(3):189-93.
Bruce DG, Devine A, Prince RL. Recreational physical activity levels in healthy older women: the importance of fear of falling. J Am Geriatr Soc. 2002;50(1):84-9.
Sherrington C, Fairhall NJ, Wallbank GK, Tiedemann A, Michaleff ZA, Howard K, et al. Exercise for preventing falls in older people living in the community. Cochrane Database Syst Rev. 2019;1:Cd012424.
Gardner MM, Robertson MC, McGee R, Campbell AJ. Application of a Falls Prevention Program for Older People to Primary Health Care Practice. Prev Med. 2002;34(5):546-53.
Mackenzie L, McIntyre A. How Do General Practitioners (GPs) Engage in Falls Prevention With Older People? A Pilot Survey of GPs in NHS England Suggests a Gap in Routine Practice to Address Falls Prevention. Front Public Health. 2019;7:32.
Grossman DC, Curry SJ, Owens DK, Barry MJ, Caughey AB, Davidson KW, et al. Interventions to Prevent Falls in Community-Dwelling Older Adults: US Preventive Services Task Force Recommendation Statement. Jama. 2018;319(16):1696-704.
Freiberger E, Blank WA, Salb J, Geilhof B, Hentschke C, Landendoerfer P, et al. Effects of a complex intervention on fall risk in the general practitioner setting: a cluster randomized controlled trial. Clin Interv Aging. 2013;8:1079-88.
Siegrist M, Freiberger E, Geilhof B, Salb J, Hentschke C, Landendoerfer P, et al. Fall Prevention in a Primary Care Setting. Dtsch Arztebl International. 2016;113(21):365-72.
Blank WA, Freiberger E, Siegrist M, Landendoerfer P, Linde K, Schuster T, et al. An interdisciplinary intervention to prevent falls in community-dwelling elderly persons: protocol of a cluster-randomized trial [PreFalls]. BMC Geriatr. 2011;11:7.
Spice CL, Morotti W, George S, Dent TH, Rose J, Harris S, et al. The Winchester falls project: a randomised controlled trial of secondary prevention of falls in older people. Age Ageing. 2009;38(1):33-40.
Rubenstein LZ. Falls in older people: epidemiology, risk factors and strategies for prevention. Age Ageing. 2006;35 Suppl 2:ii37-ii41.
Elley C, Robertson, MC., Kerse, NMM. Garrett, McKinlay, ES., Lawton, B., Moriarty, H., Campbell, AJ. Fall Assessment clinical tiral (FACT): design, iunterventions, recruitment strategies and participant characterisistics. BMC Public Health 2007;7:185-95.
Lamb SE, Jorstad-Stein EC, Hauer K, Becker C. Development of a Common Outcome Data Set for Fall Injury Prevention Trials: The Prevention of Falls Network Europe Consensus. J Am Geriatr Soc. 2005;53(9):1618-22.
Podsiadlo D, Richardson, S. The timed “Up &Go”: a test of basic functional mobility for frail elderly persons. J Am Geriart Soc. 1991;39:142 - 8.
Shumway-Cook A, Brauer S, Woollacott M. Predicting the Probability for Falls in Community-Dwelling Older Adults Using the Timed Up & Go Test. Physical Therapy. 2000;80(9):896-903.
Guralnik JM, Ferrucci L, Simonsick EM, Salive ME, Wallace RB. Lower- extremity function in persons over the age of 70 years as a predictor of subsequent disability. N Engl J Med. 1995;332(9):556-61.
Dias N KG, Todd CJ, Beyer N, Freiberger E, Piot-Ziegler C,Yardley L., Hauer K. . [The German version of the Falls Efficacy Scale-International Version (FES-I)]. Z Gerontol Geriatr. 2006;39(4):297-300.
Hauer KA, Kempen GI, Schwenk M, Yardley L, Beyer N, Todd C, et al. Validity and sensitivity to change of the falls efficacy scales international to assess fear of falling in older adults with and without cognitive impairment. Gerontology. 2011;57(5):462-72.
Delbaere K, Close JC, Mikolaizak AS, Sachdev PS, Brodaty H, Lord SR. The Falls Efficacy Scale International (FES-I). A comprehensive longitudinal validation study. Age Ageing. 2010;39(2):210-6.
Salminen MJ, Vahlberg TJ, Salonoja MT, Aarnio PT, Kivela SL. Effect of a risk-based multifactorial fall prevention program on the incidence of falls. J Am Geriatr Soc. 2009;57(4):612-9.
Uusi-Rasi K, Patil R, Karinkanta S, Kannus P, Tokola K, Lamberg-Allardt C, et al. Exercise and vitamin D in fall prevention among older women: a randomized clinical trial. JAMA Intern Med. 2015;175(5):703-11.
El-Khoury F, Cassou B, Latouche A, Aegerter P, Charles MA, Dargent-Molina P. Effectiveness of two year balance training programme on prevention of fall induced injuries in at risk women aged 75-85 living in community: Ossebo randomised controlled trial. BMJ. 2015;351:h3830.
Bhasin S, Gill TM, Reuben DB, Latham NK, Ganz DA, Greene EJ, et al. A Randomized Trial of a Multifactorial Strategy to Prevent Serious Fall Injuries. New England Journal of Medicine. 2020;383(2):129-40.
Hughes CC, Kneebone, II, Jones F, Brady B. A theoretical and empirical review of psychological factors associated with falls-related psychological concerns in community-dwelling older people. Int Psychogeriatr. 2015;27(7):1071-87.
Schoene D, Heller C, Aung YN, Sieber CC, Kemmler W, Freiberger E. A systematic review on the influence of fear of falling on quality of life in older people: is there a role for falls? Clin Interv Aging. 2019;14:701-19.
Landi, F., Liperoti, R., Russo, A., Capoluongo, E., Barillaro, C., Pahor, M., . . . Onder, G. Disability, more than multimorbidity, was predictive of mortality among older persons aged 80 years and older. J Clin Epidemiol, 2010, 63(7), 752-759.
Acknowledgements
This paper is submitted in partial fulfilment of the requirements for obtaining the degree Dr. rer. biol. hum. (PhD in Human Biology) for the primary author.
We want to thank all our patients as well as our general practitioners for taking part in our study and giving us their time.
Funding
Open Access funding enabled and organized by Projekt DEAL. This work has been funded by a grant from the Bavarian State Ministry of the Environment and Public Health (Gesund.Leben.Bayern.) (LP 00110, Pr.Nr. 09–10).
Author information
Authors and Affiliations
Contributions
C. Hentschke: analysis and interpretation of data, manuscript preparation.
M. Halle: study concept and design, acquisition of subjects; interpretation of data, manuscript review.
B. Geilhof: acquisition of subjects and/or data, analysis and interpretation of data.
P. Landendörfer: study concept and design, acquisition of subjects and/or data.
C. Sieber: interpretation of data, manuscript review.
W. Blank: study concept and design, acquisition of subjects and/or data, analysis and interpretation of data.
E. Freiberger: study concept and design, acquisition of subjects and/or data, intervention development, analysis and interpretation of data, manuscript preparation.
M. Siegrist: study concept and design, acquisition of subjects and/or data, analysis and interpretation of data, manuscript preparation.
Corresponding author
Ethics declarations
Conflict of Interests
None of the authors have any conflict of interest to declare.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Ellen Freiberger and Monika Siegrist are equally contributed last authors
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Hentschke, C., Halle, M., Geilhof, B. et al. 24-Months Cluster-Randomized Intervention Trial of a Targeted Fall Prevention Program in a Primary Care Setting. J GEN INTERN MED (2021). https://doi.org/10.1007/s11606-021-06944-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s11606-021-06944-w