
Abstract
Background
Age-related cataracts are a significant global health issue due to population ageing. More than 70% of older Australians aged 80 or above have clinically significant age-related cataracts.
Aim
The study aimed to identify factors associated with age-related cataracts among older Australian women 79–90 years.
Method
A 6-year longitudinal analysis of the Australian Longitudinal Study on Women’s Health (ALSWH) was conducted on 7117 women from surveys four to six. The women were asked whether they had been diagnosed or treated for cataracts 3 years before each survey. We used generalised estimating equation (GEE) modelling to identify factors independently associated with age-related cataracts.
Results
At baseline (79–84 years), 44.8% lived in metropolitan Australia, 67.9% had good general health, 26.5% had private health insurance, 30.6% had cataracts, 28.8% had undergone cataract surgery, 12.0% had diabetes, 24.9% had skin cancer, 56.2% had hypertension, 24.0% had a history of falls, 63.0% had visited general practitioner (GP) frequently, and 48.8% were driving themselves as their main means of transport. In the final model, poor general health [adjusted odds ratio (AOR) = 1.23, 95% CI = 1.14, 1.33)], not driving (AOR = 1.09, 95% CI = 1.01, 1.18), having private health insurance (AOR = 1.13, 95% CI = 1.04, 1.23), frequent GP visits (AOR = 1.16, 95% CI = 1.07, 1.25), skin cancer (AOR = 1.26, 95% CI = 1.16, 1.37), hypertension (AOR = 1.13, 95% CI = 1.05, 1.21), and fall (AOR = 1.12, 95% CI = 1.04, 1.22) were significantly associated with the age-related cataracts.
Conclusions
Systemic diseases, poor quality of life, driving cessation, and health service use were significantly associated with age-related cataracts in older women.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
A cataract is the leading cause of blindness, responsible for approximately 51% of cases [1] and with 15·2 million cases among people aged 50 years and older in 2020 [2]. It is the preventable cause of blindness affecting 95 million people in the world [2, 3]. Cataract risk factors have hereditary and environmental components where the genetic factor plays a role in up to 70% of cases [4]. Age-related cataracts are the most common form of cataracts, generally occurring after 50 years [5]. The prevalence of cataracts increases with age, from around 4% among those aged 55–64 years to more than 90% among those aged 80 years and above [3]. As the population ages, the burden of cataracts will increase [6]. It is expected that age-related cataracts will continue to be an important global health issue due to increasing life expectancy [7], particularly among older women presenting huge financial burdens for both governments and individuals [6, 8]. At the age of 80, everyone either had a cataract or had undergone surgery [9, 10].
In Australia, cataracts are a common public health problem as a result of population ageing [11]. It is the second most common cause of bilateral vision impairment [11]. Clinically significant cataract was predicted to increase from 1.7 million people in 2001 to 2.7 million by 2021 in Australia [12]. Over 70% of older Australians aged 80 or above have clinically significant age-related cataracts, and the disease is more common among women than men [13]. The number of Australians with cataracts has grown by two-thirds during the past 20 years, indicating the impact of continued population ageing [12]. In 2016–2017, more than 700,000 Australians (3.9% of the whole population) were affected by cataracts [14]. According to the Medibank Better Health Index, there has been an increase in cataract incidence with 139,000 more Australians living with cataracts than in 2016–2017 compared to 2010–2011, with a steeper increase amongst older Australian women as the result of women’s greater longevity [14].
Previous studies have identified a number of factors associated with cataracts, including age [15], education [15], employment, socioeconomic factors, rural residence, smoking [15], excessive sunlight exposure [6, 16], diabetes [6, 15], and other systemic diseases [17].
Different studies examined smoking as a risk factor for cataracts, finding a consistently strong association [18,19,20]. Also, it has even been shown that there is a dose–response relationship between smoking and cataract that smoking cessation can decrease the risk of cataract [19]. Generally, smoking is one of the most constantly documented modifiable risk factors for cataract progression [6].
Diabetes has long been associated with cataracts, with evidence from different study designs and case observations [6, 15, 20, 21]. In addition, the high prevalence and early onset of cataracts and lens opacities in diabetic patients were also long-recognised by clinical studies [20, 22]. It has been suggested that around 4% of all cataracts can be attributed to diabetes [23].
An association of high prevalence of cataracts with hypertension was reported from the Barbados Eye Study [17] and a meta-analysis conducted on 25 studies in 2014. The pooled results showed that cataract risk in populations with hypertension significantly increased and concluded hypertension was strongly associated with cataract [24].
Many previous studies reported strong evidence for an increased association between falls and cataracts [25,26,27,28]. Fall is a public health problem and the main cause of an accident in older people as a result of frailty [29]. Even though cataract surgery is able to restore eyesight, lengthy waiting times for public patients, particularly those who have no private health insurance [30, 31] in many high-income countries, including Australia, is a common problem that results in falls while waiting for surgery [32, 33].
Several studies have reported driving cessation, reduced amount of driving, or decision to stop driving as a result of poor vision, often secondary to cataracts in old age [34, 35]. Driving depends heavily on vision. It is an almost well-established fact that eyesight is a very important organ required for driving activity [36]. Other research findings also revealed that eyesight problems, one of which is cataract, are among many commonly cited health issues mentioned as reasons for driving avoidance or cessation [35, 37].
In Australia, driving is a way of life and is common in older age groups [38]. The number of older road users Australians with a driver’s licence has been increasing at a rate greater than any other age group with a 44% increase for 65 years and above compared to what was only 17% growth across all age groups in 2014 [39]. This study hypothesizes as many Australians are driving across their life course; an age-related cataract will occur and may become a barrier in their way to continue driving at an advanced age.
In summary, previous studies identified sociodemographic factors like age, sex, education; lifestyle choices and health behaviours like smoking, alcohol drinking, obesity (BMI), and chronic conditions and injuries like diabetes, cardiac problem, hypertension, eye injury (surgery), falls, and UV-B exposure as factors associated with cataract. In turn, cataract has been associated with cessation or reduction in driving in older age.
However, what is less known is whether the same sociodemographic, lifestyle choices and chronic conditions are associated with age-related cataract at very old age and which factors are more important in relation to an ageing society and healthy ageing goals in older women. These factors have not been well explored in the very old age (80+) group. Previous studies of factors associated with cataracts have focused on middle-aged (40–54) and young-old (60–74) study populations. In this study, we question factors which are important in young, old and middle-aged people are the same for people over the age of 80 years [40, 41].
In addition, this study investigates the association between cataracts and driving in later life. Identifying the potential risk factors of age-related cataracts in this particular age group may help in targeting clinical interventions, early diagnosis, and prompt treatment that, in turn, reduces the economic, social and personal impact of cataract by improving the quality of life of older people in keeping with the goals of healthy ageing [42].
The specific objective of this study is to investigate factors associated with age-related cataracts among older Australian women from the age of 79–90 years. It is 6 years of follow-up using generalised estimating equation modelling (GEE) on the Australian Longitudinal Study on Women’s Health (ALSWH) data survey waves four to six.
Methods section
Study sample
The data for this study were from the 1921 to 1926 cohort of Australian Longitudinal Study on Women’s Health (ALSWH). ALSWH was established to examine the continuing health, medical condition, and health service utilisation of Australian women (www.alswh.org.au) [43]. The women were randomly sampled from the Australian Medicare database which includes all Australian citizens and permanent residents. They were first surveyed in 1996 when the women in the 1921–1926 cohort were 70–75 years. Since that time, the women have been surveyed every 3 years from 1996 to 2011, and then 6-monthly [43, 44]. This study uses survey four as a baseline when the cataract and eye surgery (including cataract) questions were incorporated into the ALSWH survey and include survey data from survey 4 (ages 79–84) to survey 6 (85–90) for longitudinal analysis.
In every survey, demographic factors; health and medical conditions including eye health, private health insurance, GP visit; well-being like general health; chronic medical conditions like skin cancer, diabetes, hypertension, and fall; environmental factors like state of residence (area); and lifestyle choices were inquired across the women’s life.
Outcome variable
Cataract (self-reported diagnosis for cataract)
To identify having a cataract we used the survey question, “In the last 3 years have you been diagnosed with or treated for Cataract?” with the response option “Yes” and” No”. This question was asked across all three surveys.
Independent variables
Independent variables in this study were chosen based on previous literature [6, 45] and modelled according to the sociodemographic factors, health behaviours, and chronic medical conditions. All independent variable measures were taken from ALSWH surveys 4 to 6, except education, country of birth, hormone replacement therapy (measured at survey 1 and 3), language spoken at home which were only measured at survey 1 in 1996, and whether the women eat fruit or vegetables most days and smoking status measured at survey 2, skin surgery due to cancer or sunspots removal (at measured at surveys 2 and 3) and different types of medication use measured at survey 3, and alcohol use status measured at survey 3 and 6.
Sociodemographic factors included age, highest educational qualification, state, country of birth, short-listed categorisation of language spoken at home, and area of residence.
Health behaviour variables included were self-rated health, which was dichotomized as good (excellent/very good/good) versus poor (fair/poor), having private health insurance, and frequency of general practitioner (GP) visits in the last 12 months of the survey. In addition, whether the women eat fruit or vegetables most days, smoking status, whether they drive a car themselves or not (means of transport), and alcohol use status were treated as health behaviour variables.
Chronic medical conditions and injury that could affect cataract development and progression included skin cancer, diabetes, hypertension, stroke, hormone replacement therapy, different types of medication use and fall.
Analysis
Data sets for surveys 4, 5, and 6 were merged and response patterns for the outcome variable (cataract) was performed to examine patterns of missing data. Independent variables were examined for correlation with each other, and bivariate association were assessed using chi-square test for categorical variables and t-tests for continuous variables with the outcome cataract.
The following variables, ARIA+, country of birth, education (also correlated with private insurance), language spoken at home, marital status, eating adequate amounts of fruit or vegetables most of the days, BMI, smoking, alcohol, were not statistically significantly associated with cataract on bivariate pre-regression screening (even though some of these variables seems to be well established risk factors in previous literature) and were excluded from the modelling process. Use of multiple medications was correlated with many variables including BMI, GP visit, and driving; skin surgery due to cancer or sunspots removal was correlated with skin cancer; physical function (PF) score and social function (SF) score were correlated with general health, GP visits and falls and were subsequently excluded from the modelling.
Generalised estimating equations (GEE) models were performed to account for the repeated measures of cataract over the three time points (6-year follow-up), and to adjust for multivariable relationships. Models were explored using time-invariant and time-varying independent variables, based on the Liang and Zeger approach [46]. GEE models were built applying binary distribution of the outcome variable, with a logit link function and autoregressive correlation structure as cataract was measured at equal time interval with 3 years between each survey from 2005 to 2011. Only independent variables with p < 0.25 were considered for the analyses using generalised estimating equations (GEE) model.
Four GEE models were constructed: model (1) a base model including time and baseline age. Driving was also added to examine the association between cataracts and driving, prior to adjusting for other variables; model (2) model 1 plus general health, smoking, GP use, and health insurance; model (3) model 2 plus health conditions. Lastly, in model 4, we looked at significant variables from model 3.
Results
Sample characteristics at baseline
The original cohort includes 12,432 women who joined the study in 1996. The response rate at this time was around 40%, but the women were broadly representative of the general population of women 70–75 in comparison with national data [47]. Survey 4 was completed by 7158 women, and 2289 women had died by that time. A further 19 women had no information for cataract for surveys 4–6, and 122 women had missing data for the outcome variable at baseline. At this point, 7117 women remained in the sample for subsequent longitudinal analysis.
Table 1 shows sociodemographic and health-related characteristics of the participants at baseline. Around two-thirds (63.1%) were non-partnered, 39.7% had school certificate, 13.2% had high school certificate, and 17.1% had trade/college or university degree, 44.8% live in metropolitan, 36.72% live in inner regional, 18.5% live in outer regional, remote, and very remote Australia, and 48.8% were driving themselves as their main means of transport.
Regarding health-related characteristics, 30.6% had cataract, 28.8% had underwent cataract surgery, 67.9% had excellent, very good or good general health, 26.5% had private health insurance, 12.0% had diabetes, 24.9% had skin cancer, 56.2% had hypertension, 24.0% had a history of fall, and 63.0% had visited GP 5 or more times in the past 12 months of the study (Table 1).
Three years later, at survey 5 (age 82–87 years), 23.3% of the women had cataracts, some deceased, and some did not complete the survey (Fig. 1, progression chart). A smaller proportion, 15.4%, had cataracts at survey six at age 85–90 years, with many women deceased or otherwise did not respond to the survey. However, among respondents, the prevalence of cataract remained at around 30% at each survey: 30.6% at survey four, 31.2% at survey five and 28.1% at survey six. It should be also noted that some of these women had undergone cataract surgery. For instance, at baseline (ages 79–84 years), 28.8% had already undergone cataract surgery (Table 1).

Proportion of women having cataract from 79 to 90 years surveys 4–6 (2005–2011)
Factors associated with age-related cataracts
Area of residence, alcohol consumption, and education have no association at bivariate screening. Time was significant between baseline and survey 6 but not with survey 5, and little change with addition of other variables.
Baseline age was not significant across the modelling process. However, we kept age in the model regardless of its statistical significance, as age is very important risk factor for cataracts.
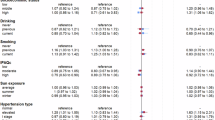
Not driving was significantly associated with having cataracts when added to baseline age. As the model building continues, not driving was significantly associated with having cataracts with little change in effect when lifestyle choice, health behaviour, and chronic condition variables added to the model across model 2 to model 4 (AOR = 1.09, 95% CI = 1.01, 1.18) (Table 2, model 4). From the lifestyle and health behaviour variables, smoking was not significantly associated with cataract (Table 2, model 2). From chronic conditions, diabetes, stroke, other eye surgeries, and hormone replacement therapy were not significant (Table 2, model 3).
In the final multivariable nested model, poor general health (AOR = 1.23, 95% CI = 1.14, 1.33), having private health insurance (AOR = 1.13, 95% CI = 1.04, 1.23), 5 or more GP visits in the past 12 months prior to the survey (AOR = 1.16, 95% CI = 1.07, 1.25), skin cancer (AOR = 1.26, 95% CI = 1.16, 1.37), hypertension (AOR = 1.13, 95% CI = 1.05, 1.21), and fall (AOR = 1.12, 95% CI = 1.04, 1.22) were significantly associated with the odds of having age-related cataracts (Table 2, model 4). The odd ratios indicated in this document is that of the parsimonious adjusted nested model 4.
Discussion
In this population-based longitudinal study of older Australian women, we found that poor general health, not driving, having private health insurance, frequent GP visits from health behaviour and lifestyle factors were significantly associated with age-related cataracts. There was also a strong significant association between hypertension, skin cancer, and fall and age-related cataracts from chronic conditions. In this study, previously reported associations between hypertension, driving cessation, fall and cataracts were confirmed. However, there was no association between smoking, alcohol intake, diabetes, hormone replacement therapy, and age-related cataracts in the current study.
Health behaviour, lifestyle choices, and age-related cataracts
In many studies, poor self-rated health has been associated with visual impairment, which is usually due to cataracts in older people [48, 49]. Our study also confirmed that women who rated their general health as poor were 23% more likely to have cataracts (Table 2 model 4). This might be due to its effect of cataract-related vision impairment on mental health, driving, social interaction, risk of falling and then fracture. As evidenced in previous studies, driving cessation due to cataract-related vision problems may affect older people’s independence, freedom of movement to fulfil their basic needs, essential services like shopping groceries and medical supplies [50,51,52]. It may also affect their mental health [53], risk of falls and then fracture, which hampers the quality of life in older individuals [25]. In general, this can be seen as indicative of the poor quality of life in older persons as a result of cataracts or change in vision and its consequences if timely intervention is not done [32, 54]. This finding has critical importance as the evaluation of healthcare in older people mainly focuses on quality of life.
In this study, women who were not driving were 9% more likely to have cataracts by the age of 79–90 years (Table 2 model 4). Numerous previous researchers reported driving cessation or decision to stop driving was mainly due to vision impairment as a result of cataracts in older age [34, 50, 52, 55]. Our study also confirmed this fact which is in line with many study findings as this could be due to the fact that driving a motor vehicle was strongly depends on the visual function of the eye above any other sense organs as receiving and processing information to operate a motor vehicle when driving is mainly received through eye [35, 36, 50, 56].
It is an almost well-established fact that eyesight is a very important organ required for driving activity [36]. Other research findings also revealed eyesight problems, one of which is due to cataracts, are among many commonly cited health issues mentioned as reasons for driving avoidance or cessation [35, 37]. A cataract is the main public health problem in older Australians; as well above 70% of older Australians had cataracts by the age of 80 years, and the problem is increasing with age and more common in women than men. It can affect the mental, physical, social-wellbeing, and more importantly, the functional ability of older people, which has paramount importance for healthy ageing [13].
This finding is very important as the number of older road user Australians have been increasing as a result of population ageing [39], as well as many Australians are driving across their life course. But age-related eye conditions, like cataracts, will occur in their way and become a barrier to driving which impacts older women not continuing to drive in old age, which needs early identification of risk factors, prioritizsing, and targeted intervention to promote healthy ageing of older Australians. The present study revealed that those women who have private health insurance were 23% more likely to be diagnosed or treated for cataracts compared to those who did not have private insurance, and those women with frequent GP (general practitioner) visits were also 16% more likely to be diagnosed or get treatment for cataract (Table 2 model 4). Recently published large population-based study of 257,237 participants of Australian population from the 45 and Up Study, having private health coverage, was independently associated with the treatment of cataract privately [57]. In another study in 4 European Countries, namely Germany, France, Italy, and Spain, having private health insurance coverage provided French patients with more and better access to the more effective and sophisticated eye lens [31].
The association between frequent GP use and cataract in the current study could be explained by the fact that when patients visit a family doctor or their own GP or health care intuition like a hospital for other comorbidity or ocular disease, they may get the opportunity to be diagnosed and referred early. A study conducted in Sweden also revealed this fact where more than 41% of patients who regularly visit their GP were diagnosed and referred by health care providers they frequently met compared to those who initiated and sought treatment by themselves [58].
Therefore, our findings and the limited previous studies suggest the importance of having private insurance as equity and accessibility to health services. The frequent GP visits also might show availability and accessibility of healthcare facilities, good health-seeking behaviour, or comorbidities needing frequent healthcare provider visits, especially in older women, which may also suggest socioeconomic inequalities. This could suggest the need for targeted intervention for those who have no private health cover in addition to Medicare cover.
Systemic diseases and chronic conditions associated with age-related cataracts
In our study, hypertension was associated with cataracts, where those women with hypertension were 1.13 times more likely to have cataracts compared to those without hypertension (Table 2 model 4) in the final adjusted model after controlling several confounding factors. In Australia’s ‘Blue Mountains Eye Study’, it was reported repeatedly that hypertension and other cardiovascular risk factors were associated with an incident of different forms of age-related cataract [59, 60] and many others studies, including a meta-analysis conducted on 25 studies in 2014 where the pooled results revealed that cataract risk in populations with hypertension was significantly increased, but in cataract subtype analysis hypertension has no association with nuclear cataract [24]. Finally, the study concluded that hypertension is associated with cataract development which might be either because of hypertension or anti-hypertension drugs utilisation [24, 60]. It also might be due to alteration of protein structure in the lens capsules, as suggested by Lee et al. [61]. In another study, the Barbados Eye Study, the association of high occurrence of cataracts with hypertension was reported [17]. Our study also revealed the association between hypertension and cataract, but the pathophysiology behind its formation and progression is unclear even though several suggestions have been forwarded [24]. Therefore, proper control of hypertension among older people is important, and further research is needed to identify the pathophysiology between hypertension and cataract in order to establish a causal pathway.
Only a few other studies have investigated the association between skin cancer and age-related cataracts. The current study has discovered that there was a strong positive association between skin cancer and cataract in which the odds of developing cataracts were 1.26 times more likely in older women with skin cancer compared to those who had no skin cancer (Table 2 model 4). This finding is relatively new of its kind as only two cross-sectional studies so far reported the positive association between skin cancer and age-related cataract as to the researchers’ knowledge [62, 63]. One of the studies was conducted on older Australian populations using historical Cohort of the Registry of Senior Australians (ROSA) that reported age-related cataract was positively associated with skin cancer and its different types among people aged ≥ 65 years (≥ 50 years in case of Aboriginal or Torres Strait Islander descent) who had an aged care eligibility assessment between 2005 and 2015 [63]. The other cross-sectional study conducted in Israel also examined the association of skin cancer with cataracts using a local health care services database among persons 40 years and over in which positive association between cancer skin lesion (cancer) from exposure to sunlight and cataract was identified [62]. Our study also revealed the same fact with a more sophisticated population-based longitudinal analysis among an older cohort of Australian women from age 79–84 to 85–90, which strengthened the previous studies.
The finding may be explained as exposure to sunlight may exacerbate the development and progression of age-related cataracts as ultraviolet radiation from sunlight exposure is the established environmental risk factor for both skin cancer and cataract [6, 16, 62, 64]. This effect was also demonstrated in the study of the Australian population that revealed a high level of climatic ultraviolet radiation was associated with the increasing prevalence of cataracts among indigenous Australians [65]. The finding supports the hypothesis previously suggested that both skin cancer and age-related cataract may share common causal pathways like ultraviolet radiation, particularly from sunlight exposure [63]. This finding can also be used as a proxy indicator of ultraviolet radiation from sunlight exposure as a risk factor for cataracts, as we do not have ultraviolet radiation (sunlight exposure) variable in our data, which would be advantageous to address the limitation of this study. This study can be used by clinicians to consider and manage multiple diseases (multimorbidity) such as ocular, dermatologic, and systemic diseases when patients visit for one health problem for early identification and referral. Future studies should focus on identifying the common causal pathway between skin cancer and cataract, testing the suggested hypothesis that cataracts and skin cancer share common pathophysiology, given that ultraviolet radiation from sunlight exposure is a common risk factor.
In our study, the odds of falls were 13% more likely associated with having cataracts among older women compared to those without a history of falls (Table 2 model 4). Similar to our finding, many previous studies also reported a significant association between falls and cataracts among older people in different settings, including Australia [30, 31]. As age increases, the risk of falls also considerably increases, and it becomes a public health problem [40, 73], resulting in fractures and other injury [66, 67], hospitalizations [68, 69], admission to aged care [68], and decline in quality of life, particularly in older people with cataracts [32, 68, 70, 71]. In the Melbourne visual impairment study, researchers have identified the risk of falls in older people with cataracts was almost three times more than for those without cataract [72]. In 2015–2016 alone, the treatment, functional loss, disability, and deaths due to falls were estimated to cost the Australian healthcare system $3.9 billion [73].
Against this cost of falls, cataract surgery is a high impact procedure that restores sight. However, lengthy waiting times for public patients, particularly those who have no private health insurance in many high-income countries such as Australia, are common. This supply side problem in accessing care can exacerbate the risks of falls while waiting for surgery [32, 33].
In Australia, cataract surgery waiting time can take up to 3 years from diagnosis to treatment, with 2 years spent in referral and pre-treatment ophthalmologic screening [74], and about 12 months on a surgical waiting list [75]. For instance, 90% of patients waited for 334 days for surgery in 2017–2018, and about 2.5% of these patients waited for over a year [75]. However, a randomised controlled trial study conducted in the UK by Harwood et al. [76] revealed decreasing the cataract surgery waiting times from 1 year to 1 month has resulted in a decrease in the rate of falls by 34% [76], revealing many cases of falls in older people with cataract can be prevented. Therefore, the issue of cataract surgery is not only just surgery but also the issue of preventing falls and fractures, promoting driving (mobility) and independence, and reducing admission to hospital and residential aged care. Thus, early cataract treatment by reducing surgical waiting time can help prevent falls and fractures and can promote healthy ageing. Training country tailored mid-level health practitioners like cataract surgeons may help to reduce the burden on ophthalmologists, rather than having patients waiting for specialist service all the time, specifically for those who have no private health insurance. This will help to ensure the right to sight and improve the quality of life.
This study has some limitations. Firstly, the cataracts and other variables are self-reported. This is a common limitation for large epidemiological surveys. We also do not have data for excessive sunlight (ultraviolet radiation) exposure from sunlight which is the established risk factor for age-related cataracts in several previous studies. But in our study, we identified a strong association between skin cancer and cataract, and we believe we addressed this through the association between skin cancer and cataract as ultraviolet sunlight exposure is a common risk factor for both skin cancer and cataract. In addition, we did not identify the three different subtypes of cataracts in this study, and it should be noted that the finding is for all three types of cataracts.
Conclusion
This finding supports our hypothesis that vision impairment due to age-related cataracts may be the barrier to continue driving in old age. The finding also supports our hypothesis that factors associated with age-related cataracts in young-old and middle-aged people may not be the same for people aged 80 years and above as demographic characteristics and lifestyle choices are different, and there have been competing risks over the course of their later lives. In our study, chronic conditions such as hypertension, skin cancer, and falls and health behaviours such as frequent GP visits, poor general health, and private health insurance were significantly associated with age-related cataracts in late life. However, sociodemographic and lifestyle factors like education, smoking, and alcohol intake were not associated with age-related cataracts in this age group. However, they have been shown to have an association in young-old and middle-aged individuals.
Policymakers should consider specific and targeted policy and practice for this oldest age group that addresses access to health service use like encouraging optimum GP visits, prioritising those with no private insurance, and reducing cataract surgery waiting times.
Also, integrating eye health into non-communicable chronic diseases will have importance. The findings can be used by policymakers and clinicians to consider managing multiple diseases (multimorbidity) such as ocular, dermatologic, and systemic diseases when patients visit for one health problem. This has paramount importance for early identification and referral in relation to an ageing society and healthy ageing goals.
References
Pascolini D, Mariotti SP (2012) Global estimates of visual impairment: 2010. Br J Ophthalmol 96(5):614–618
Steinmetz JD et al (2021) Causes of blindness and vision impairment in 2020 and trends over 30 years, and prevalence of avoidable blindness in relation to VISION 2020: the Right to Sight: an analysis for the Global Burden of Disease Study. Lancet Glob Health 9(2):e144–e160
Liu Y-C et al (2017) Cataracts. Lancet 390(10094):600–612
Heiba IM et al (1995) Evidence for a major gene for cortical cataract. Invest Ophthalmol Vis Sci 36(1):227–235
Shiels A, Hejtmancik JF (2017) Mutations and mechanisms in congenital and age-related cataracts. Exp Eye Res 156:95–102
Robman L, Taylor H (2005) External factors in the development of cataract. Eye 19(10):1074–1082
Rao GN, Khanna R, Payal A (2011) The global burden of cataract. Curr Opin Ophthalmol 22(1):4–9
Organization WH (1998) The World health report 1998: life in the 21st century a vision for all. In The world health report 1998: life in the 21st century A vision for all. p 241–241
NIH National Eye Institute (2021) Learn about eye health
Centre for Eye Research Australia (2021) How common is cataract? [cited 2021 21June 2021]; Available from: https://www.cera.org.au/conditions/cataract/
Foreman, J., et al. (2016) National eye health survey 2016
Rochtchina E et al (2003) Projected prevalence of age-related cataract and cataract surgery in Australia for the years 2001 and 2021: pooled data from two population-based surveys. Clin Experiment Ophthalmol 31(3):233–236
Australian Institute of Health Welfare (2005) Vision problems in older Australians. AIHW: Canberra
MediBank (2017) How common are cataracts in Australia? | Live Better. [cited 2018 19/06/2018]
Chang JR et al (2011) Risk factors associated with incident cataracts and cataract surgery in the Age-related Eye Disease Study (AREDS): AREDS report number 32. Ophthalmology 118(11):2113–2119
Neale RE et al (2003) Sun exposure as a risk factor for nuclear cataract. Epidemiology 14(6):707–712
Leske MC et al (1999) Diabetes, hypertension, and central obesity as cataract risk factors in a black population: the Barbados Eye Study. Ophthalmology 106(1):35–41
Seddon J et al (1995) Epidemiology of risk factors for age-related cataract. Surv Ophthalmol 39(4):323–334
Christen WG et al (1992) A prospective study of cigarette smoking and risk of cataract in men. JAMA 268(8):989–993
West S et al (1989) Cigarette smoking and risk of nuclear cataracts. Arch Ophthalmol 107(8):1166–1169
Obrosova IG, Chung SS, Kador PF (2010) Diabetic cataracts: mechanisms and management. Diabetes Metab Res Rev 26(3):172–180
Hodge WG, Whitcher JP, Satariano W (1995) Risk factors for age-related cataracts. Epidemiol Rev 17(2):336–346
Ederer F, Hiller R, Taylor HR (1981) Senile lens changes and diabetes in two population studies. Am J Ophthalmol 91(3):381–395
Yu X et al (2014) Hypertension and risk of cataract: a meta-analysis. PLoS ONE 9(12):e114012
Lord SR, Dayhew J (2001) Visual risk factors for falls in older people. J Am Geriatr Soc 49(5):508–515
Boptom RQI et al (1998) Visual impairment and falls in older adults: the Blue Mountains Eye Study. J Am Geriatr Soc 46(1):58–64
Lord SR et al (1994) Physiological factors associated with falls in older community-dwelling women. J Am Geriatr Soc 42(10):1110–1117
McCarty CA, Nanjan MB, Taylor HR (2000) Operated and unoperated cataract in Australia. Clin Experiment Ophthalmol 28(2):77–82
Davison J, Marrinan S (2007) Falls. Rev Clin Gerontol 17(2):93
Curbow B, Legro MW, Brenner MH (1993) The influence of patient-related variables in the timing of cataract extraction. Am J Ophthalmol 115(5):614–622
Cuq C et al (2008) A European survey of patient satisfaction with spectacles after cataract surgery and the associated costs in four European countries (France, Germany, Spain, and Italy). Ophthalmic Epidemiol 15(4):234–241
Palagyi A et al (2016) While we waited: incidence and predictors of falls in older adults with cataract. Invest Ophthalmol Vis Sci 57(14):6003–6010
Chan FW et al (2009) Waiting time for cataract surgery and its influence on patient attitudes. Invest Ophthalmol Vis Sci 50(8):3636–3642
Forrest KY et al (1997) Driving patterns and medical conditions in older women. J Am Geriatr Soc 45(10):1214–1218
Ragland DR, Satariano WA, MacLeod KE (2004) Reasons given by older people for limitation or avoidance of driving. Gerontologist 44(2):237–244
Bohensky M et al (2008) Implications of vision testing for older driver licensing. Traffic Inj Prev 9(4):304–313
Adler G, Rottunda S (2006) Older adults’ perspectives on driving cessation. J Aging Stud 20(3):227–235
Keay L et al (2016) Vision and driving status of older Australians with cataract: an investigation of public hospital waiting lists. Clin Exp Optom 99(5):449–455
Bureau of Infrastructure Transport and Regional Economics (BITRE) (2014) Road safety of older Australians - recent statistics. D.o.I.a. Regional and Development, Editors. Canberra
Lee SB et al (2018) Differences in youngest-old, middle-old, and oldest-old patients who visit the emergency department. Clin Exp Emerg Med 5(4):249
Alterovitz SS, Mendelsohn GA (2013) Relationship goals of middle-aged, young-old, and old-old internet daters: an analysis of online personal ads. J Aging Stud 27(2):159–165
World Health Organization (2015) World report on ageing and health. World Health Organization
University of Newcastle and University of Queensland (2020). Australian Longitudinal Study on Women’s Health (ALSWH). Available from: www.ALSWH.org.au. Accessed 24 September 2021
Lee C et al (2005) Cohort profile: the Australian longitudinal study on women’s health. Int J Epidemiol 34(5):987–991
Lee D-S et al (2015) The gender-dependent association between obesity and age-related cataracts in middle-aged Korean adults. PLoS ONE 10(5):e0124262
Liang K-Y, Zeger SL (1986) Longitudinal data analysis using generalized linear models. Biometrika 73(1):13–22
Brilleman SL, Pachana NA, Dobson AJ (2010) The impact of attrition on the representativeness of cohort studies of older people. BMC Med Res Methodol 10(1):1–9
Wang JJ, Mitchell P, Smith W (2000) Vision and low self-rated health: the Blue Mountains Eye Study. Invest Ophthalmol Vis Sci 41(1):49–54
Taylor HR, McCarty CA, Nanjan MB (2000) Vision impairment predicts five-year mortality. Trans Am Ophthalmol Soc 98:91
Gilhotra JS et al (2001) Impaired vision and other factors associated with driving cessation in the elderly: the Blue Mountains Eye Study. Clin Exp Ophthalmol 29(3):104–107
Owsley C et al (1999) Older drivers and cataract: driving habits and crash risk. J Gerontol A Biol Sci Med Sci 54(4):M203–M211
Owsley C, McGwin G Jr (1999) Vision impairment and driving. Surv Ophthalmol 43(6):535–550
Chandrasekaran S et al (2008) Change in health-related quality of life after cataract surgery in a population-based sample. Eye 22(4):479–484
Brenner MH et al (1993) Vision change and quality of life in the elderly: response to cataract surgery and treatment of other chronic ocular conditions. Arch Ophthalmol 111(5):680–685
Byles J, Gallienne L (2012) Driving in older age: a longitudinal study of women in urban, regional, and remote areas and the impact of caregiving. J Women Aging 24(2):113–125
Anstey KJ et al (2005) Cognitive, sensory and physical factors enabling driving safety in older adults. Clin Psychol Rev 25(1):45–65
Zhu Z et al (2021) Geographic variation in cumulative incidence of private cataract surgery in Australia and its influencing factors: Findings from the 45 and Up Study. Eye
Olofsson P, Lundström M, Stenevi U (2001) Gender and referral to cataract surgery in Sweden. Acta Ophthalmol Scand 79(4):350–353
Tan JSL, Wang JJ, Mitchell P (2008) Influence of diabetes and cardiovascular disease on the long-term incidence of cataract: the Blue Mountains eye study. Ophthalmic Epidemiol 15(5):317–327
Cumming RG, Mitchell P (1998) Medications and cataract: the blue mountains eye study. Ophthalmology 105(9):1751–1758
Lee SM et al (1997) Possible mechanism of exacerbating cataract formation in cataractous human lens capsules induced by systemic hypertension or glaucoma. Ophthalmic Res 29(2):83–90
Varssano D et al (2017) Association between cataract and keratinocytic skin cancers or melanoma: speculating on the common role of sun and ultraviolet radiation exposures. Ophthalmic Epidemiol 24(5):336–340
Sharma S et al (2020) Association of age-related cataract with skin cancer in an Australian population. Invest Ophthalmol Vis Sci 61(5):48–48
Dolezal JM, Perkins ES, Wallace RB (1989) Sunlight, skin sensitivity, and senile cataract. Am J Epidemiol 129(3):559–568
Hollows F, Moran D (1981) CAtaract-the ultraviolet risk factor. Lancet 318(8258):1249–1250
Van Helden S et al (2008) Bone and fall-related fracture risks in women and men with a recent clinical fracture. JBJS 90(2):241–248
Keay L, Palagyi A (2018) Preventing falls in older people with cataract–it is not just about surgery
Gill TM et al (2013) Association of injurious falls with disability outcomes and nursing home admissions in community-living older persons. Am J Epidemiol 178(3):418–425
Watson WL, Li Y, Mitchell RJ (2011) Projections of hospitalised fall-related injury in NSW, Australia: impacts on the hospital and aged care sectors. J Safety Res 42(6):487–492
Siracuse JJ et al (2012) Health care and socioeconomic impact of falls in the elderly. Am J Surg 203(3):335–338
Roe B et al (2009) Older people and falls: health status, quality of life, lifestyle, care networks, prevention and views on service use following a recent fall. J Clin Nurs 18(16):2261–2272
McCarty CA, Fu CL, Taylor HR (2002) Predictors of falls in the Melbourne visual impairment project. Aust N Z J Public Health 26(2):116–119
Australian Institute of Health Welfare (2020) Injury. AIHW: Canberra
Diviney E, Lillywhite S (2004) Victorian ophthalmology service planning framework
Australian Institute of Health Welfare (2018) Elective surgery waiting times 2017–18: Australian hospital statistics. AIHW: Canberra
Harwood RH et al (2005) Falls and health status in elderly women following first eye cataract surgery: a randomised controlled trial. Br J Ophthalmol 89(1):53–59
Acknowledgements
The research on which this article is based was conducted as part of the Australian Longitudinal Study on Women’s Health, led by The University of Newcastle and The University of Queensland jointly. The authors would like to thank the Australian Government Department of Health for funding and participants of the study. We also would like to thank Tara Tolhurst for English language editing service. Researchers in the School of Medicine and public Health at the University of Newcastle are also members of the Hunter Medical Research Institute. The finding, recommendations, conclusions, presented in this paper are those of the authors only and not an official position of the Government of Australia Department of Health.
Funding
Open Access funding enabled and organized by CAUL and its Member Institutions. This research was also supported by the Australian Research Council Centre of Excellence in Population Ageing Research (CEPAR) (project number CE170100005).
Author information
Authors and Affiliations
Contributions
MTH conceptualized the study, and contributed to design of the study, and performed data analysis, and drafted the manuscript and made final corrections. JB contributed to the conceptualisation of the study, contributed to analysis strategy, reviewed the manuscript critically for publication, and made final comments to the manuscript. XDG contributed conceptualisation of the study, reviewed the first and second draft of the manuscript. All authors approved the manuscript submission for publication.
Corresponding author
Ethics declarations
Ethics approval
The ALSWH study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Human Research Ethics Committees (HREC) of the University of Newcastle (reference H-076–0795) and the University of Queensland (reference 2004000224).
Competing interests
The authors have no relevant financial or non-financial interest to disclose related to this paper.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Hambisa, M.T., Dolja-Gore, X. & Byles, J.E. A longitudinal analysis of factors associated with age-related cataract among older Australian women: a cohort study of 7851 older Australian women 79–90 years. Ir J Med Sci 192, 1525–1536 (2023). https://doi.org/10.1007/s11845-022-03130-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11845-022-03130-7