
Abstract
Colorectal cancer (CRC) stands as one of the most prevalent form of cancer globally, causing a significant number of deaths, surpassing 0.9 million in the year 2020. According to GLOBOCAN 2020, CRC ranks third in incidence and second in mortality in both males and females. Despite extensive studies over the years, there is still a need to establish novel therapeutic targets to enhance the patients’ survival rate in CRC. Nuclear receptors (NRs) are ligand-activated transcription factors (TFs) that regulate numerous essential biological processes such as differentiation, development, physiology, reproduction, and cellular metabolism. Dysregulation and anomalous expression of different NRs has led to multiple alterations, such as impaired signaling cascades, mutations, and epigenetic changes, leading to various diseases, including cancer. It has been observed that differential expression of various NRs might lead to the initiation and progression of CRC, and are correlated with poor survival outcomes in CRC patients. Despite numerous studies on the mechanism and role of NRs in this cancer, it remains of significant scientific interest primarily due to the diverse functions that various NRs exhibit in regulating key hallmarks of this cancer. Thus, modulating the expression of NRs with their agonists and antagonists, based on their expression levels, holds an immense prospect in the diagnosis, prognosis, and therapeutical modalities of CRC. In this review, we primarily focus on the role and mechanism of NRs in the pathogenesis of CRC and emphasized the significance of targeting these NRs using a variety of agents, which may represent a novel and effective strategy for the prevention and treatment of this cancer.
Graphical Abstract

Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
With more than 19.3 million new cases and 10 million fatalities recorded annually, cancer persists as one of the world’s most destructive diseases and causes of death [1]. Among these, colorectal cancer (CRC) ranks third in terms of incidence and second in fatality considering both sexes worldwide [1, 2]. Approximately 41% of all CRCs are believed to occur in the proximal colon, 22% in the distal colon, and 28% in the rectum [3]. Apparently, an increase in uptake of animal-source food, a sedentary lifestyle, less physical activity, excess body weight, and obesity are the major risk factors for the initiation, development, and progression of CRC [4]. In addition, heavy consumption of alcohol, excessive smoking, intake of red or processed meat, and various genetic and environmental aspects are also reported as key risk factors in CRC [3, 5, 6]. The detection of precancerous lesions or cancer at an early stage of CRC development has significantly risen due to the greater adoption of screening programmes [7, 8]. However, 20% of cases are identified when the illness has progressed to further organs like the liver or lung [7]. Although effective cancer screening programmes have reduced the incidence and mortality of CRC, GLOBOCAN 2020 projected 1,148,515 new cases and 576,858 deaths with respect to colon cancer and 732,210 new cases and 339,022 deaths in rectal cancer in the year 2020 [1, 9]. An approximate ninefold variation was observed in the incidence rate of colon cancer in different regions of the world, with the highest rates in New Zealand, Hungary, Europe, Norway, Australia, and Northern America [1]. Rectal cancer incidence rates are found to be the highest in the Eastern Asia region and the lowest in the regions like South-Central Asia and Africa [1]. However, the incidence rate of CRC has declined in some high-incidence countries mainly because of the healthier lifestyle choices, such as reduced consumption of tobacco, a proper dietary condition, the detection of CRC in the early stages by colonoscopy screening and the removal of precursor lesions [10, 11]. Though there are many advances made in the treatment, prevention of complications after post-operation remains a challenge in the clinical management of CRC [12, 13]. Moreover, the prognosis of CRC has never been effective, especially for patients with metastatic lesions [14]. Accumulating evidence over the past decades suggests that chemotherapy including natural compounds, have improved overall survival (OS) in cancer patients [15,16,17,18,19,20,21,22,23,24,25,26,27,28]. However, chemotherapy has been linked with a lot of drawbacks, such as systemic toxicity, unsatisfactory response rate, erratic innate and acquired resistance, and a dearth of tumor-specific selectivity [29, 30]. As a result, significant studies are required to develop innovative strategies to improve or possibly replace the current CRC chemotherapy regimen [13, 31,32,33,34]. Therefore, the exploration and identification of new therapeutic targets are imperative to enhance the management of CRC.
Nuclear receptors (NRs) are classically defined as ligand-activated transcription factors (TFs) and are divided into three groups based on their ligand-binding; orphan, adopted and the endocrine NRs [35, 36]. Currently, there are more than three hundred members in NR superfamily across the species, and forty-eight NRs are known to play a role in human physiology [35, 36]. Studies in the past have revealed the pivotal role of steroid hormones, such as androgens, in the progression of various cancers [37]. Later, numerous studies stated the critical role of NRs in cancer development and progression [38,39,40,41]. Thus, NRs have emerged as novel, highly efficacious therapeutic targets for various malignancies [35, 42,43,44]. It has also been observed that nuclear hormone receptors (NHRs) play a crucial role in interacting with hormonal factors in the nucleus and regulation of gene expression [36, 45]. Their varied biological and physiological properties are vast, and regulate numerous functions like differentiation, metabolism, reproduction, homeostasis, physiology, and development [36, 45]. It is well known that men are more predisposed towards colon cancer development compared to women. In line with this, accumulating evidence implicates the linkage of aberrant levels of sex hormones in the development of CRC [46]. It was shown that hormonal therapy such as dehydroepiandrosterone sulphate, an androgen precursor, improved the OS and was associated with a reduced risk in CRC patients [47]. Besides, the clinical trial by Women’s Health Initiative showed 40% decreased risk of CRC development when treated with estrogen plus progestin in the treatment cohort compared with the placebo group [48]. Further, it was reported that CAG repeats (> 25) in androgen gene in males increase their susceptibility to colon carcinogenesis, while females having CA repeats (≥ 25) in ERβ gene had six-fold higher risk for the development of colon cancer [49]. Preclinical studies have documented the protective role of both estradiol and testosterone in colon carcinogenesis. Treatment with testosterone resulted in apoptosis of colon cancer cells via phosphatidylinositol 3-kinase/Akt (PI3K/Akt) pathway, activation of Bad, and actin cytoskeleton dynamics [50]. Amos-Landgraf and colleagues studied the sex disparity in the development of colonic adenomas in Apc(Pirc/+) rat model. It was observed that ovariectomy in female rats resulted in the deprivation of endogenous hormones and had no effect on the prevalence of adenomas. However, it was reported that orchidectomy (castration) of male rats significantly protected the Apc(Pirc/+) rat from adenoma development, whereas treatment with testosterone reversed this effect [51]. Though various experiments have shown the differential role of sex hormones in CRC, prospective, multi-centered, interventional clinical trials are the need of hour to successfully establish the hormonal therapy as an adjuvant to conventional cancer treatments.
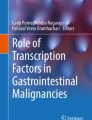
The NRs consists of intracellular TFs that serve as sensors for a variety of stimuli and translate the external signal into a transcriptional output [52]. All NR family members contain an N-terminal domain (NTD), a ligand binding domain (LBD), that can bind cell permeable agonists, a hinge region, a DNA-binding domain (DBD) that binds to upstream sequences of target genes, and a C-terminal domain (CTD) (Fig. 1) [52]. Dysregulation of NRs is often linked to various diseases in humans and controls complex regulatory signaling pathways in disease progression [36, 53]. The NRs REV-ERB and retinoic acid receptor-related orphan receptors (ROR) have been implicated in a wide range of physiological processes, including metabolic regulation, development, immunity, and the circadian rhythm [54]. Given that NRs govern a diverse array of biological processes that overlaps with the characteristics of cancer cells, their involvement in tumorigenesis and the advancement of cancer has been extensively studied over the decades [55]. NRs also possess a vital role in the tumor microenvironment by controlling inflammation and immune responses [56]. Furthermore, NRs also serve as biomarkers for tumor sub-classification and targets for hormone therapy which play a major role in cancer diagnosis and treatment [55, 57]. Since most NRs can be selectively activated or inactivated by small molecules, they act as prominent therapeutic targets [36]. There are several FDA-approved NR-targeted drugs for oncology use, such as flutamide, bexarotene, tamoxifen, etc. [58].

Nuclear receptor structural domains: N-terminal domain (NTD) (A/B), DNA binding domain (DBD) (C), hinge region (D), ligand/hormone binding domain (LBD) (E), and C-terminal domain (CTD) (F). NTD consists of a region, activation function-1 (AF-1), whose function is independent of the presence of a ligand. LBD consists of another region activation function-2 (AF-2), whose function is dependent on the presence of a bound ligand. Nuclear localization sequence or signal (NLS), is an amino acid sequence that tags a protein for import into the cell nucleus by nuclear transport
Extensive research conducted over the past decades has provided substantial insights into the role of NRs in the pathogenesis of CRC. Therefore, in this review, the influence of alterations in NRs of both normal and cancerous cellular processes in CRC is highlighted. We also demonstrate the prospect of targeting NRs as an alternate strategy for the prevention and treatment of CRC.
2 Nuclear receptor signaling
Activated NRs control numerous biological processes in the body through regulating the transcription of multiple genes [59]. Recent studies have highlighted the activation of orphan NRs by various endogenous ligands, which has increased the prospect for the development of various synthetic ligands for the modulation of the NRs in the management of different diseases, including cancer [54, 60]. NRs are majorly found as monomers, but they tend to form higher-order complexes when bound to their binding partners. For example, NRs when bound to RXR, can exist as either homo or heterodimeric complexes [59, 61].
Based on their modes of action, NRs signaling is divided into four types, ranging from Type I to Type IV (Fig. 2) [62]. Type I NRs: these receptors contain steroid receptors (SRs), which are activated by steroidal hormones generated from cholesterol, including androgens, estrogens, progesterone, and corticoids [61, 63]. These receptors are sequestered in the cytoplasm by chaperone proteins, but when the ligand activates, they dissociate from their chaperone proteins and translocate into the nucleus. In the nucleus, SRs often bind to DNA response elements (RE) composed of two inverted repeats as homodimers [61, 64]. Type II NRs: members of this class include RAR and LXR and are frequently found in the nucleus even without the presence of an activating ligand. Upon the binding of a ligand, the receptor undergoes a conformational change, resulting in its dissociation from a co-repressor complex. This event facilitates the subsequent recruitment of co-activators and the transcriptional machinery, initiating the process of gene transcription [61]. On direct repeat of DNA RE, these receptors typically form heterodimeric complexes with RXRs RE [59]. NRs of Type III generate homodimers on their direct repeat sequences, which are comparable to the REs of Type II NRs and have a similar mode of action [61]. Type IV NRs share a similar mode of action to that of Type II NRs, but it binds to DNA as a monomeric structure and recognizes extended half‐sites within RE [61]. NR crosstalk refers to the intricate interplay between various NRs or their intersecting signaling pathways. Some NRs, such as PPARs and RARs, participate in the formation of well-established "typical" heterodimers with RXR. Additionally, there is a distinct class of physical complexes known as the "atypical" heterodimers, wherein NRs like GR and PPARs or PPAR and ERR binds together, potentially exhibiting more transient characteristics [65]. In summary, these NRs represent viable targets for therapeutic intervention, and ligands designed to specifically target these receptors may be used as a possible strategy for the treatment of various diseases.

Nuclear receptor general mechanism: NRs exert their transcriptional stimulation of target genes by four different mechanisms (Type I–IV). (N Nucleus; C Cytoplasm)
3 Nuclear receptors in colorectal cancer
NRs have long been at the forefront of cancer research due to their ability to modulate various processes of tumorigenesis [36]. During tumor development, NRs remarkably control the growth of tumors in hormone-driven tissues [35]. Several NRs have been implicated in CRC development and progression, where they regulate multiple signaling pathways and TFs, thereby altering cellular behavior [66, 67]. The involvement of NRs in CRC has been the subject of an increasing amount of attention due to their ability to control a range of tumor-related processes, including cell proliferation, differentiation, homeostasis, migration, invasion, and cell death (Table 1 and 2). The significant role of several NRs such as Androgen Receptors (ARs), EAR2, Estrogen Receptors (ERs), Estrogen-related Receptors (ERRs), Farnesoid X Receptors (FXRs), Hepatocyte Nuclear Factor 4 alpha (HNF4α), Liver Receptor Homolog 1 (LRH-1), Liver X Receptors (LXRs), Nuclear Hormone Receptor 77 (Nur77), Progesterone Receptors (PRs), Peroxisome Proliferator-activated Receptors (PPARs), Pregnane X Receptors (PXR), Retinoid X Receptors (RXRs), Thyroid Hormone Receptors (THRs) and Vitamin D Receptors (VDRs) has been identified in CRC (Fig. 3). Through the regulation of various TFs and signaling cascades, these receptors help in the development and progression of CRC.

Nuclear receptors in colon cancer: Various NRs that are involved in colorectal cancer are Androgen receptors (ARs), EAR2, Estrogen receptors (ERs), Estrogen-related receptors (ERRs), Farnesoid X receptors (FXRs), Hepatocyte nuclear factor 4 alpha (HNF4α), Liver Receptor Homolog 1 (LRH-1), Liver X receptors (LXRs), Nuclear Hormone Receptor 77 (Nur77), Progesterone receptors (PRs), Peroxisome proliferator-activated receptors (PPARs), Pregnane X receptors (PXR), Retinoid X receptors (RXRs), Thyroid hormone receptors (THRs) and Vitamin D receptors (VDRs)
NRs also play a major role in the regulation of gut microbiota. Secondary bile acids (BAs) produced by the gut microbiota have a significant impact on human metabolism and energy balance via nuclear or G protein-coupled receptors. Recent research has demonstrated that BAs regulation by these receptors play an essential role in sustaining innate immune responses [68]. It is well known that the aberrant gut microbiome dysbiosis is associated with metabolic diseases including obesity, non-alcoholic fatty liver disease and insulin resistance [69]. For instance, mice models containing an intestine-specific deletion of ERβ when administered with AOM/DSS resulted in the reduction of gut microbiota diversity. This dysbiosis induced by the synergistic effects of AOM/DSS and ERβ deletion, further impacted cellular motility and carbohydrate metabolism, suggesting that intestinal ERβ contributes to microbiome homeostasis, potentially reducing the risk of developing CRC [70]. The following section describes the role of NRs and their mechanistic action in CRC (Fig. 4).

General overview of NR signaling mechanism on how various agonists, antagonist, and other ligands play a role in CRC
3.1 Androgen receptor (AR)
ARs, commonly referred as nuclear receptor subfamily 3, group C, gene 4 (NR3C4), belong to the NR superfamily that are ligand-dependent TFs [275, 276]. ARs consist of three major functional domains—DBD, NTD, and LBD [277]. They are primarily expressed in the kidney, testis, epididymis, seminal vesical, cervix, fallopian tube, endometrium, and breast tissues (The Human Protein Atlas: https://www.proteinatlas.org/ENSG00000169083-AR/tissue) [278]. Androgens are essential for the regulation of cell growth and differentiation in several CRC tissues. The majority of cancers, at the time of initial diagnosis, exhibit a dependence on androgens. Consequently, the primary therapeutic strategy typically involves androgen ablation therapy. This approach is designed to decrease serum androgen levels and inhibit the activity of the AR, targeting the primary drivers of tumor growth in these cases [279]. A plethora of studies have reported the pivotal role of AR in the initiation and advancement of various types of cancers [50, 280,281,282,283,284]. Moreover, studies in animal models suggest that androgens function as promoters in the development of colon cancer [142, 285]. Studies have elucidated the relation between AR and Wnt signaling pathway in prostate cancer. It has been evinced that AR activation is through various cofactors, such as β-catenin, glucocorticoid receptor interacting protein-1 (GRIP1), etc. [286, 287]. Yang and group studied the interaction and crosstalk between the AR and Wnt/β-catenin signaling in prostate cancer. It was reported that β-catenin exhibited strong and selective interaction with AR and not with other NRs like ERα, PR, and GR. Further, the armadillo repeats of β-catenin were found to directly interact with the LBD of AR [288]. Another study has reported that the translocation of β-catenin is facilitated by binding with AR, hence activating the Wnt signaling [289]. In another study, it was shown that limiting levels of β-catenin leads to AR-mediated suppression of β-catenin/TCF-related transcription and had no effect on AR target gene expression [290]. Also, various studies have linked the co-activation of Src and AR to be crucial in prostate tumorigenesis [291,292,293]. Another study reported that the Src mutant (Y527F), which displayed constitutive activity, promoted the nuclear translocation of AR and enhanced AR activity even in the absence of androgens. Conversely, the Src mutant with inactive kinase activity demonstrated a downregulation of AR transcriptional activity [291]. Hence the interplay between the AR, Src and β-catenin orchestrates the transcriptional activation of AR.
It was noted that the genes encoding the AR consists of 2 polymorphic trinucleotide repeat segments, which are polyglutamine (CAG) and polyglycine (GGC). These CAG repeats are inversely related to numerous cancers [294]. Since AR is expressed in colon tissues, alterations in the length of the CAG repeat of the AR gene can also be associated with colon cancer [294]. Further, it was observed that AR and VDR signaling are interlinked, and they work mutually in CRC [295]. For example, individuals with 23 or more CAG repeats of the AR gene, less exposure to sunlight, and low intake of vitamin D tend to show an increased rate of rectal carcinoma development, mainly amongst men when compared to women [295]. Multiple studies have reported the downregulation of AR in CRC tissues when compared to adjacent normal tissues [71, 73, 74, 296]. However, its expression was also reported to be upregulated in CRC tissues implicating the differential role of AR in CRC development and progression [72].
Several studies suggested the drugs that modulate the expression of AR have remarkable potential in the prevention and treatment of CRC. For example, FCX, an arylidene derivative, suppressed the cell growth of AR-selective HCT-8 and HT-29 colon cancer cell lines in higher FCX concentrations [139]. In another study, it was observed that dehydroepiandrosterone (DHEA) and nerve growth factor (NGF) decreased, serum deprivation-induced apoptosis, but the treatment with testosterone led to increased apoptosis in colon cancer cell line (Caco2), suggesting the interplay between steroid hormones and neurotrophins signaling in hormone-dependent tumors [50]. Xia et al., elucidated the role of AR gene methylation in the modulation of CRC (Fig. 5) [297]. Another study revealed that enzalutamide, an AR antagonist, enhanced the myeloid cell-mediated immune suppression and progression in both in vitro and in vivo [140]. Further, treatment of SW480 cells with DHT in combination with casodex effectively disrupted the androgen-sensitive interaction between AR and β-catenin, and concurrently alleviated the transcriptional repression of the TOPFLASH reporter. Furthermore, an increase in the accumulation of cells at the G1 phase of the cell cycle was observed. Concurrently, in vitro growth assays demonstrated a 35% decrease in the viability of cells treated with the AR+DHT [141]. In another study, the combination of selective androgen receptor modulator (SARM), GTx-024, with histone deacetylase inhibitor (HDACi), AR-42, was found to improve anabolic response in the cachectic condition in CRC by mediating the regulation of β-catenin in C-26 cachectic mice model [142]. Therefore, AR and its modulators play a key role in regulating different processes involved in CRC and hence could be an important target in the treatment and clinical management of CRC.

Activity of AR in DNA methylation- A Nonmutant, inactive androgen receptor binds to testosterone resulting in receptor activation. Androgen receptor response elements are bound with the activated androgen receptor causing DNA-inducing gene expression and preventing DNA methylation. Additionally, suppressor complexes (S; dotted arrow) that repress specific gene sets (“Gene 2”) are affected by either the active AR itself or AR-induced genes, which ultimately results in the DNA methylation of suppressed genes. B In Androgen insensitivity syndrome, the absence of AR activity leads to the inhibition of AR target genes, which may cause (stochastic de novo) DNA methylation of the affected genes. On the other hand, genes that AR typically silences (directly or through additional AR-dependent pathways) are activated, which prevents DNA methylation. Grey lollipops: unmethylated DNA, Greens lollipops: methylated DNA
3.2 EAR 2
EAR 2, also known as nuclear receptor subfamily 2, group F, gene 6 (NR2F6), is an orphan NR belonging to the member of the chick ovalbumin upstream promoter-transcription factors (COUP-TFs) that regulate various biological processes like migration, adhesion, apoptosis, etc. [75, 298]. The expression of EAR 2 is highly upregulated in human primary colorectal tumors when compared to normal colon tissues. It was observed that the knockdown of EAR 2 in CRC cell lines HCT-116, RKO, and HT-29 resulted in the inhibition of X-linked inhibitor of apoptosis protein (XIAP) expression and induction of apoptosis. Further, in the same study, the EAR 2-inactivated RKO xenograft model showed suppression of tumor growth, thus suggesting the role of EAR 2 in regulating cell survival in colon cancer [75]. However, more studies are needed to establish the potential of EAR 2 as a therapeutic target for CRC.
3.3 Estrogen receptors (ERs)
The ER, a steroid hormone NR, acts as a TF and governs the expression of target genes implicated in diverse processes, including cellular proliferation and survival [299]. Following the activation of the receptor, ER dimerizes when they are in contact with a ligand [300]. The ligand estradiol (E2) activates ER resulting in the dimerization, nuclear translocation and biding to the RE of the target gene that is located in or adjacent to the promoter regions [301]. The ER is categorized into two groups, namely estrogen receptors alpha (ERα) and beta (ERβ), which are mainly involved in regulating multiple physiological processes in the human body [302]. This receptor has been reported to play a significant role in modulating a variety of pathological disorders, including cancer [303, 304].
A plethora of studies have shown the association of ER with CRC, and it is variably expressed in this cancer [76,77,78,79,80, 82,83,84,85,86,87,88,89,90,91,92, 94, 100]. Moreover, both isoforms are reported to have different functions in CRC. For instance, ERβ was reported to exhibit a protective effect in CRC through its activation by estrogen [305]. It was observed that ERβ exhibited contrasting results of p65 chromatin binding in HT-29 and SW480 cells. In HT-29 cells, ERβ diminished a significant portion of p65 chromatin binding, whereas in SW480 cells, it augmented p65 binding. This could be due to the appearance of new p65 binding sites in SW480 cells in the presence of ERβ, resulting in distinct modulation of the p65 cistrome in both cell lines [305].
Hartman et al., demonstrated that ERβ has the ability to impede cell proliferation and suppress tumor growth in both in vitro and in vivo, likely due to the inhibitory effects of ERβ on cell-cycle pathways. Moreover, this repression of the cell cycle by ERβ relies on the functional binding with estrogen response elements (EREs) [86]. Studies have shown that low expression of ER induces colon carcinogenesis and its progression; however, overexpression of this receptor inhibited cell viability and induced apoptosis by upregulating Bax, p53, and cleaved caspase -3 and -9 [81, 149]. Moreover, the differential expression of ERα and ERβ was found to regulate numerous miRNAs, signaling pathways like Wnt/β catenin, p38/MAPK, etc., and induce apoptosis [81, 149, 154, 155, 157,158,159]. An intriguing study reported that over-expression of ERα inhibited cell proliferation and induced apoptosis by upregulating the expression of the hTNF-α gene and downregulating β-catenin signaling in LoVo cells. The same study has also shown the overexpression of hERα and E2 treatment enhanced the promoter activity of TNF-α in these cells [148]. Moreover, it was shown that the deficiency of ERβ increased small intestine tumorigenesis in murine models and was correlated with the modulation of genes implicated in TGFβ signaling with or without estrogen treatment [154]. Another study suggested that the treatment of cisplatin with SW480 ERβ cells resulted in the increased cell viability [163]. In addition, ERβ knockout mouse model was found to develop higher colitis-associated colon carcinogenesis [93]. The downregulated ERβ expression also led to higher inflammatory damage caused by upregulating TNF-α and nuclear factor-κB (NF-κB) target molecules [93]. Furthermore, the upregulation of ERβ was found to increase miRNA-205 levels in both normal and cancerous colon epithelial cells, subsequently reducing PROX1 expression, leading to decreased proliferative and metastatic potential of the cells [95]. Contrastingly, ERβ was also shown to exhibit tumor-promoting effect. For instance, it was shown that ERβ was positively correlated with colon carcinogenesis in a rat model; however, the treatment with ERβ antagonist, raloxifene, inhibited aberrant crypt foci (ACF) formation in this model [146].
A plethora of studies have also identified the potential of ER agonists and antagonists modulating the activity of ER. For example, activation of ERβ with agonist ERB-041 in HCT-116, Caco2, and SW480 cell lines decreased cell survival, colonosphere formation, and migration while increasing the expression of ESR2, HPGD, CCND1, CTNNB1, CSLTR1, etc., suggesting the anti-tumor role of ERβ in CRC and the possible use of its agonist in the treatment of this disease [147]. Moreover, 17-β estradiol and progesterone increased the expression of ERβ, which led to elevated apoptosis by decreasing proliferating cell nuclear antigen (PCNA) and upregulating the expression of caspase -3 and -8 with enhanced cleavage of Poly (ADP-ribose) polymerases (PARP) in the experimental model [160]. The modulators of ER, such as tamoxifen and raloxifene, were also shown to reduce cell growth, and proliferation in HCT-116 and HCT-8 cell lines [143]. In another study, tamoxifen and 5-Flurouracil (5-FU) alone, or in combination inhibited cell migration, proliferation and induced apoptosis and cell cycle arrest with downregulation of ERβ and matrix metalloproteinase 7 (MMP-7) in HT-29 colon cancer cells [156]. In addition, the agents like celecoxib and difluoromethylornithine (DFMO) was found to exhibit chemopreventive effect by modulating ERα expression and DNA methylation [80]. Further, it was shown that various natural compounds and other agents like 5-Aza-CdR, quercetin, curcumin, ginseng, raloxifene, soy isoflavones, folic acid, genistein, resveratrol, and silymarin exhibit anti-cancer activity by modulating the expression of ER [146, 153, 162, 306, 307]. With regard to this, the induction of ERβ by dietary soy isoflavones demonstrated an anti-cancer effect by suppressing cell growth and tumor dysplasia in both in vitro experiments using DLD-1 cells and in a rat model [153]. In another study, the activation of ERβ with apigenin and naringenin showed cancer-preventive effects in young adult mouse colonocytes (YAMC) cells [144]. Moreover, 5-Aza-CdR induced the expression of ERα and ERβ via the downregulation of DNMT1, which resulted in apoptosis and inhibition of cell growth in HT-29 CRC cells [162]. Thus, ER could be a potential target, and modulating this NR with various agonists/antagonists and other agents holds immense prospects for the management of CRC.
3.4 Estrogen related receptor (ERR)
The ERR, also known as nuclear receptor subfamily 3, group B (NR3B), is one of the orphan receptors belonging to the NR superfamily of ligand-regulated TFs, which significantly regulates the cellular metabolism of the body [308]. It is structurally more related to the canonical ER and can modulate estrogen signaling in most types of cancers [308]. The presence of ERR mainly in the metabolically active tissue regions helps in regulating the transcription of metabolic genes, consisting of the ones involved in mitochondrial turnover and autophagy [309]. ERRs are classified into three isoforms, among which ERRα and ERRβ were first cloned in 1988 by using the DBD of ERα as the probe to screen recombinant DNA libraries [310]. Later, the third isoform ERRγ was identified [310]. Vernier et al., reported a direct molecular connection between the activity of two isoforms of ERR and the regulation of glutamine utilization as well as the production of the antioxidant glutathione. The downregulation of ERRα limits the entry of glutamine into the TCA cycle, whereas the upregulation of ERRγ enhances the production of glutathione driven by glutamine. Significantly, it was also observed that elevated expression of ERRγ serves as a notable indicator of oxidative stress induced by mitochondrial dysfunction or chemotherapy [310]. Recent evidence have reported the critical role of ERR in various metabolic diseases and cancer [309, 311]. In line with this, studies have also evaluated the role of ERR in regulating various molecules and processes involved in CRC [96, 97, 99, 312].
The expression of ERRα was found to be upregulated in CRC cells and tissues [96, 97, 99, 312]. In addition, ERRα overexpression was associated with shorter OS and progression-free survival (PFS) and correlated with advanced stage and higher tumor grade [99]. Additionally, the overexpression of ERRα was found to increase the proliferation and migration of CRC cells via elevating the expression of IL-8 [312]. However, numerous studies suggested that inhibiting ERRα significantly impaired cell proliferation, migration, colony formation, cell cycle arrest, and induced apoptosis by downregulating several metabolic pathways and associated molecules [164]. For example, inhibition of ERRα induced cell cycle arrest, apoptosis, and increased mitochondrial metabolic stresses, ROS generation, and mitochondrial membrane permeabilization [98]. Moreover, the inhibition of ERRα decreased the expression of peroxisome proliferator-activated receptor gamma coactivator 1-alpha (PGC-1α), cytochrome c oxidase subunit IV, and voltage-dependent anion channel 1 (VDAC1) and reduced mitochondrial oxidative phosphorylation (mtOxPhos), mitochondrial DNA (mtDNA) copy number and intracellular ATP levels in HCT-116 p53+/+ cells [98]. In addition, the knockdown of ERRα and inhibition of its expression with agents like XCT790 significantly inhibited cell growth and colony formation by reducing c-Myc and cyclin D1 expression in HCT-116 and SW480 CRC cell lines [97]. Further treatment with trametinib, a specific MEK inhibitor, suppressed cell growth by reducing the expression of ERRα and its downstream molecule IDH3A. Furthermore, the combined treatment of trametinib and simvastatin, resulted in the suppression of ERRα transcriptional activity, culminating in a synergistic impact on the inhibition of proliferation and survival of colon cancer cells in pre-clinical settings [97]. Additionally, it was shown that osteopontin (OPN), an oncogene involved in tumor progression, is a direct target of ERRα and thus, silencing of ERRα resulted in a marked reduction of OPN at both protein and RNA levels in HT-29 cells, suggesting the significance of targeting ERRα in CRC [96]. Collectively, these studies suggest that ERRα is a potential target for the treatment and management of CRC.
3.5 Farnesoid X-receptor (FXR)
FXR also known as nuclear receptor subfamily 1, group H, gene 4 (NR1H4) is a well-characterized member of the metabolic subfamily of NRs [276, 313]. It is mainly expressed in the liver and intestine, and due to its pivotal role in regulating BA homeostasis, it is also referred to as BA receptor [314]. Upon binding of ligands, the FXR regulates the function of essential genes that are implicated in the metabolism of lipids and carbohydrates. Therefore, due to these important functions, it is considered one of the most promising drug targets for the treatment of BA-related liver diseases [315, 316]. Obeticholic acid (OCA) is approved as the first small molecule to target FXR, and various other small molecules are being evaluated in clinical trials [317, 318]. As ligands for FXR, bile acids, oxysterols, and cholestanoic acid take part in the complex web of interactions that ultimately control the lipid, steroid, and cholesterol homeostasis [313]. It has been shown that FXR has been linked to distinct roles specific to certain tissues and cells within different cancer types. Further, FXR has exhibited its ability to modulate a multitude of cellular signaling pathways, encompassing NF-κB, EGFR/ERK, JAK/STAT PI3K/Akt, Wnt/β-catenin, and p38/MAPK, along with their respective targets. These targets consists of a diverse array of molecules, such as EMT markers, MMPs, caspases, tumor suppressor proteins (such as C/EBPβ, p-Rb, and p53), cyclins, various cytokines, and numerous other entities. As a result, FXR exhibits potential as a cutting-edge target for the identification, prognosis, and treatment of cancer [43, 166, 168, 174]. According to several studies, the rate of cancer cell proliferation and tumor aggressiveness were linked with the overexpression of FXR in different cancers of breast, esophageal, lung, pancreas, and thyroid [43, 319,320,321].
Many studies have revealed both tumor-suppressive and oncogenic roles of FXR in CRC [35, 42, 43, 100, 322]. The FXR expression increased with the degree of differentiation in HT-29 and Caco2 cells, and it was also demonstrated that the FXR was downregulated in colon carcinomas and adenomas [101]. Further, FXR and PPARγ expression was inversely correlated in CRC [101]. Mao et al., demonstrated that silencing of FXR by small interfering RNAs (siRNAs) resulted in the Wnt/β-catenin signaling activation and formation of β-catenin/TCF4 complex in HT-29, Caco2 and HCT-116 cells [166]. FXR activation with agonists, like CDCA and GW4064, resulted in the dose-dependent suppression of MMP-7 in HT-29 cells. Additionally, it was observed that there was an increase in protein and mRNA levels of MMP-7 in the intestinal tissues and liver homogenates in the FXR knockout mice (B6.129X1 (FVB)-Nr1h4tm1Goz/J) [174]. In the same study, FXR overexpression was also shown to suppress MMP-7 expression and cell invasion in MC38 cells [174]. Another study showed that FXR overexpression and treatment with the agonist GW4064 suppressed CRC cell proliferation by inhibiting p-EGFR (Tyr845), p-ERK, and p-Src. On the other hand, inhibition of FXR by siRNA or guggulsterone induced p-EGFR (Tyr845) and p-ERK leading to increased cell proliferation in CRC. Moreover, the upregulation of FXR suppressed CRC tumor growth in nude mice, implying the role of Src, FXR, and EGFR in intestinal cell proliferation and tumorigenesis [168]. Selmin et al., observed the impairment of APC function favors the knockdown of FXR expression via CpG hypermethylation in both murine colonic mucosa and human colon cells. This downregulation led to a decreased expression of downstream targets such as SHP and IBABP, which are critical for BA homeostasis. Concurrently, there was an upregulation of pro-inflammatory and oncogenic factors like COX-2 and c-Myc, contributing to the pathogenesis of colon carcinogenesis [171]. Moreover, it was shown that FXR deficiency increased CRC cell proliferation by upregulating the expression level of cyclin D1, IL-6 and increased size and multiplicity of small intestine adenocarcinomas in CRC mouse models [167]. In addition, it was shown that chenodeoxycholic acid binds to FXR and upregulates the miR-22 expression, inhibiting cyclin A2 (CCNA2) and inducing G0/G1 cell cycle arrest in HCT-116 cells. Additionally, FXR knockout mice exhibited downregulation of miR-22, upregulation of ileal CCNA2 and increased Ki67-positive cells in the colon [169]. In another study, it was observed that activation of FXR by GW4064 led to the upregulation of death receptor 5 (DR5), and reduced cell proliferation upon treatment with TRAIL and GW4064 in CRC cell lines (HCT-116, SW480, DLD-1) [170]. In addition, it was found that FXR activation by GW4064 in colon cancer cell lines, SW620 and HCT-116 upregulated the expression of cyclin G2 (CCNG2) by suppressing miR-135A1, which leads to reduced cell proliferation and induction of cell cycle arrest. However, the knockdown of FXR reversed this effect by upregulating the expression of miR-135A1 and suppressing CCNG2 [172]. Another study revealed that FXR knockout mice (FXR−/−Apc Min/+) showed a reduction in survival rate and an increase in size and number of AOM/DSS-induced colon tumors revealing the significant potential of FXR in suppressing colorectal carcinogenesis [173]. Therefore, understanding the tumor suppressive role of FXR in CRC and thus modulating its expression by agonists and antagonists might be helpful in the management of colon tumorigenesis.
3.6 Hepatocyte nuclear factor 4 alpha (HNF4α)
The ligand-dependent TF HNF4α, is also known as nuclear receptor subfamily 2, group A, gene 1 (NR2A1) [276]. It is a highly conserved member of the NR superfamily and is expressed in both liver and gastrointestinal tract. In the liver, HNF4α is mainly known for its role as the master regulator of liver-specific gene expression and is vital for both fetal and adult liver functioning [276, 323]. The dysregulation of HNF4α expression has been linked with various human diseases like colon cancer, hepatocellular carcinoma, liver cirrhosis, ulcerative colitis, and maturity-onset diabetes of the young [323, 324]. HNF4α is linked to numerous signaling pathways that significantly contribute to tumor transformation, metastasis, inhibition of apoptosis, and promotion of proliferation. Lv et al., demonstrated that HNF4α participates in the aberrant activation of various signaling pathways, including the NF-κB pathway, Wnt/β-catenin pathway, and STAT3 pathway. Its involvement in these pathways plays an essential role in the initiation and advancement of cancer, including CRC [325]. The dysregulation of the Wnt/β-catenin signaling pathway plays a role in several cancer types. Wu et al., reported that the upregulation of HNF4α can inhibit tumor progression by suppressing the Wnt/β-catenin signaling pathway [326]. HNF4α plays a key role in the modulation of NF-κB signaling during cancer development. It promotes the expression of interleukin 1 receptor type 1 (IL1R1) and subsequently enhances the inflammatory response triggered by its ligand, interleukin 1β (IL1β). The activation of NF-κB signaling by IL1β/IL1R1 leads to the upregulation of HNF4α, establishing a feedback loop that sustains NF-κB pathway activation and propels inflammation towards cancer development [327]. The association between STAT family proteins and human carcinoma has been extensively established, and the constitutive activation of STAT3 plays a pivotal role in the process of carcinogenesis [328]. Further, HNF4α can disrupt the regulation of miR-122, leading to the upregulation of c-Met and subsequent activation of STAT3 [329]. Therefore, HNF4α has the ability to reverse tumor lesions by inhibiting the activation of the STAT3 signaling pathway and suppressing the invasion and metastasis of cancer cells. It has been observed that loss of HNF4α affects ion transport and induces chronic inflammation like inflammatory bowel disease in mice [330]. Moreover, it was shown that the inactivation of HNF4α in colon cancer cells and conditionally knockout mice decreased the expression of the gut-specific homeotic TF Cdx2, suggesting their positive correlation and tumor suppressive activity of HNF4α in colon cancer [331]. In addition, it was shown that ectopic overexpression of HNF4α suppressed proliferation, migration, invasion, and promoted G2/M phase arrest and apoptosis in HT-29, SW480, and LoVo cells. Besides, overexpression of HNF4α inhibited EMT via modulating Wnt/β-catenin signaling and suppressing the expression of Snail, Slug, Twist, and Vimentin while inducing E-cadherin expression in colon cancer cells. The same study also showed that the overexpression of HNF4α suppressed tumor growth and liver metastasis in SW480 xenograft model [102]. Contrastingly, studies have also identified the tumor-promoting activity of HNF4α. For example, a study by Xu et al., showed that the increased expression of HNF4α induced by the overexpression of tumor-promoting lncRNA LINC00858, resulted in suppression of WNK lysine deficient protein kinase 2 (WNK2) and progression of carcinogenesis in colon cancer cells [175]. In addition, lectins such as lens culinaris agglutinin (LCA) was shown to promote CRC by inducing the gene expression of HNF4α along with other genes like glucose-6-phosphatase (G6Pase) and phosphoenolpyruvate carboxykinase (PEPCK) in Caco2 cells [332]. Additionally, it was found that the inactivation of HNF4α inhibited cell proliferation and differentiation by blocking the gene expression of MUC4 and PCNA in HM7 cells [177]. Further, studies reported the divergent roles of HNF4α isoforms in tumorigenesis. Specifically, the HNF4α8 isoform was shown to promote tumor progression by enhancing cellular proliferation, invasion, and migration. In contrast, the HNF4α2 isoform exhibited tumor-suppressive properties, as evidenced in both in vitro and in vivo experimental models [176, 333]. Thus, these studies suggest the differential function of HNF4α in CRC. However, more studies are required to have a better understanding of its role in this cancer.
3.7 Liver receptor homolog 1 (LRH-1)
LRH-1, a member of the nuclear receptor 5, group A, gene 2 (NR5A2) subfamily is expressed in the tissue regions derived from the endodermal origin, including the exocrine pancreas, intestine, liver, ovary, placental region, and pre-adipocytes [334, 335]. They are predominantly regulated by cofactor interactions [336]. They modulate various functions like tissue-specific cell proliferation, cholesterol homeostasis, steroidogenesis, and stem cell pluripotency [334]. LRH-1 plays a major role in various biological processes such as gastrulation, differentiation, development, maintaining reverse cholesterol transport, BA, and glucose homeostasis [334,335,336]. It was reported that LRH-1 was involved in etiology of various tumor types, encompassing breast, gastric, pancreatic and colon cancer [334]. Several studies showed that LRH-1 is highly upregulated in colon cancer patients and is associated with poor OS, which might suggest LRH-1 as a beneficial prognostic molecular marker for the treatment of CRC [103,104,105]. For example, in a clinical study, the expression of LRH-1 was investigated in 128 cases of colon cancer, alongside their adjacent normal tissues using immunohistochemistry. The results revealed positive LRH-1 expression in 108 out of 128 colon cancer samples, while only 17 out of 128 adjacent normal tissues showed LRH-1 expression. The statistical analysis demonstrated a significant association between positive LRH-1 expression and various clinical pathological factors, including stage, depth of invasion, and lymph node metastasis. Patients with high LRH-1 expression had a notably lower OS rate compared to those with low expression. Furthermore, the multivariate analysis indicated that LRH-1 expression could serve as an independent predictor of OS. Overall, the observations of this study signify that LRH-1 likely plays a crucial role in the onset and advancement of CRC. It has the potential to serve as a valuable prognostic molecular marker, offering assistance in the diagnosis of colon cancer [103]. Moreover, it was shown that LRH-1 plays a significant role in intestinal tumorigenesis by regulating cell cycle and inflammatory proteins such as cyclin D1, cyclin E1, c-Myc, and TNF-α in animal model [184, 334]. A study by Lai et al., has shown the association of LRH-1 in promoting cancer stemness by acting as a direct target of GATA6 and elevating the levels of stem cell markers such as ALDH‐1, Ascl2, CD133, CD44, and LGR5 in CRC cells. Overexpression of LRH-1 also leads to the induction of HIF‐1α and its target genes, resulting in stronger glycolysis and lactate accumulation in HCT-116 and HT-29 clones [178]. Moreover, overexpression of LRH-1 was shown to increase the expression of steroidogenic enzymes and cortisol synthesis while its downregulation inhibited these processes implying the novel mechanism of tumor immune escape via glucocorticoids synthesis in colon cancer [337, 338]. In addition, it was shown that LRH-1 modulates the expression of PPARγ by maintaining the synthesis of cortisol in Caco2 cells [185]. Additionally, the knockdown of LRH-1 leads to cell cycle arrest and suppression of cell proliferation via Wnt signaling cascade in Caco2 and HT-29 cells [179]. LRH-1 was also shown to promote CRC cell growth by suppressing the CDKN1A gene expression mediated through p53 pathway [186]. Further, the downregulated expression of miR-381 and miR-30d led to the modulation of its direct target, LRH-1 resulting in the induction of proliferation and invasion in CRC cells [104, 181]. Furthermore, miR-136 and miR-374b was found to suppress the proliferation and invasion of CRC cells by targeting LRH-1 and Wnt signaling [105, 180]. Thus, these studies highlight the importance of targeting LRH-1 as a potential target for combating CRC.
3.8 Liver X receptors (LXRs)
LXRs, an oxysterols receptor, have two isoforms: LXRα and LXRβ, which belongs to the NR superfamily and play crucial roles in the transcriptional regulation of lipid metabolism [339, 340]. LXRs bind to the genes and regulate their expression that encode proteins involved in cholesterol efflux, absorption, excretion, transport, and conversion of BA in the liver [341]. As LXRs are involved in controlling membrane structures and functions, they also provide novel therapeutic insights into the pathophysiology of diseases like diabetes mellitus, atherosclerosis, and cancer that are linked to dysregulated lipid metabolism [339]. Studies have revealed that LXRs are involved in the progression of inflammatory diseases of the nervous, cardiovascular, and respiratory systems, and therefore targeting this receptor could result in the inhibition of these diseases including cancer [340, 341].
Interestingly, LXRs activation has been reported to affect cell survival and cell proliferation of various types of cancers that distort the metabolic pathways resulting in the accumulation of cholesterol [342]. Lin et al., stated the potential efficacy of LXRs’ ligands in the management of cancer [343]. In line with this, the role of LXR in CRC was reported by many studies and revealed that LXR was diversely expressed in this disease [106, 191]. However, Tang et al., found that the expression level of LXR was downregulated in CRC patients [189]. Moreover, the inactivation of LXR in mice model showed increased tumorigenesis by inducing the expression of proliferation markers, while treatment with its agonist GW3965 inhibited this effect. Furthermore, the activation of LXR was shown to induce cell cycle arrest by modulating the expression of genes such as, Skp2, c-Myc, CDKs, cyclins, SCD1, p15 and hypo-phosphorylation of the retinoblastoma (Rb) tumor suppressor protein [191]. Additionally in another study, the activation of LXR was found to induce G1 phase arrest and caspase-dependent apoptosis in vitro and also suppressed colon cancer tumor growth in a mouse model [106].
Further, activation of LXRβ was shown to induce cell death by modulating the expression of NLRP3, caspase-1, -3, -7, -8, and -9 as confirmed by preclinical studies [190, 344]. In another study, it was shown that cytoplasmic localization of LXRβ promoted the ligand induced pyroptosis in colon cancer cells, while this process was not observed in normal colon epithelial cells [188]. It was also demonstrated that mice treated with LXR agonist T0901317 induced immunogenic cell death by modulating the levels of calreticulin, HMGB1, and ATP in CT26 cells [194]. The activation of LXR by its agonist, T0901317, was found to suppress the proliferation, clonogenicity, and migration by upregulating ABC transporters, ABCA1, ABCG5, and ABCG8, in HT-29 CD133+ cells. Similarly, its antagonist, SR9243, also showed inhibition in the proliferation and clonogenic potential of these cells by increasing ROS generation and suppressing metabolic enzymes such as PFKFB3, GSK3β, FASN, and SCD-1, thus suggesting the role of LXR in regulating cancer stem cells, colon tumorigenesis, and metastasis [187]. Moreover, treatment of HCT-116 cells with LXR agonists LXR623 and GW3965 along with ABT263 and BH3 mimetics induced the expression of LXRβ, which subsequently led to elevated levels of apoptosis and inhibition of cell viability, thus proposing the potential of LXR agonists and BH3 mimetics to be plausible agents for the treatment of solid malignancies [193]. Further, a clinical study with 37 patients have elucidated that the expression of LXR was downregulated in tumor tissues. Another clinical study with 707 patients has revealed that positive expression of LXR and COUP-TFII were observed in 50.9% (360/707) and 32.7% (231/707) of the CRC tissues, respectively. However, it was noted that the presence of LXR and COUP-TFII expression exhibited an association with improved OS rates. Therefore, the expression of LXR and COUP-TFII, in combination, may serve as biomarkers indicating positive prognosis in patients diagnosed with CRC [346]. Overall, preclinical studies have demonstrated that LXR agonists have shown promise for the treatment of CRC. Further clinical investigation is needed to assess the safety and efficacy of LXR agonists as plausible therapeutic agents in this disease. Therefore, clinical trials involving LXR agonists as part of combination treatment regimens for CRC are ongoing, suggesting the promising efficacy of LXR and its agonists/antagonists for the treatment and management of CRC.
3.9 Nuclear hormone receptor 77 (Nur77)
Nur77, commonly known as nerve growth factor-induced B alpha (NGFI-B α), NR4A1, NGFIB, TR3, TIS1, NAK-1, or N10, is an orphan NR, which is known for its endogenous ligands [107, 347]. The Nur77 act as an immediate early response gene that is initiated through multiple signal transduction mechanisms [348]. It plays a vital role in cell differentiation, proliferation, and apoptosis [348]. Nur77 has been found to function as both tumor and anti-tumor gene in CRC depending on its cellular context [349, 350]. Studies have also evaluated the expression and role of Nur77 in different cancers, including CRC. For instance, the NR Nur77 was found to be highly expressed in colon tumors and was found to induce survival in CRC cells [107, 108]. Moreover, induction of Nur77 by its agonist, deoxycholic acid (DCA), was found to induce cell growth, colony formation, and migration by modulating Wnt/β-catenin and AP-1 pathways and upregulating BRE and VEGF in CRC cells [108]. In addition, it was observed that hypoxia induced the expression of Nur77, which subsequently increased β-catenin via PI3K/Akt signaling and was found to augment cell migration, invasion, and EMT in CRC cells [198]. Additionally, the activation of Nur77 with BA was found to regulate genes involved in cell survival and apoptosis, such as CDK4, CCND2, MAP4K5, STAT5A, RBBP8, and Bid in colon cancer cells [202]. On the other hand, studies have also reported the anti-tumorigenic role of Nur77 in CRC. For instance, Nur77 was shown to promote the proteasomal degradation of an oncogenic protein, β-catenin, in SW620 colon cancer cells, thereby suggesting the tumor-repressive property of this NR in CRC [351]. Niu et al., revealed that Nur77’s role in colon cancer is specifically defined by its effects on inhibitor of differentiation 1 (ID1), a target gene of TGFβ, expression and is modulated by the potency of the TGFβ signal. Nur77 suppresses ID1 expression to function as a tumor suppressor in a low TGFβ-signal environment, whereas, Nur77 promotes the growth of tumors by enhancing the effect of TGFβ on the induction of ID1 under situations of strong TGFβ signal [350]. Further, agents like indomethacin, sulindac, and 5-FU were found to activate Nur77, which led to apoptosis in CRC cells [200, 352]. In addition, miR-22 was found to upregulate the expression of Nur77 and RARβ and suppress HDAC, leading to increased apoptosis in CRC cells. In the same study, the activation of miR-22, Nur77, and RARβ and reduction of HDACs were found to supress tumor growth in CRC xenograft [196]. Furthermore, multiple studies have demonstrated the anti-cancer efficacy of Nur77 agonist, 1,1-bis(3′-indolyl)-1-(phenyl)methane(DIM-C-Ph), 1,1-bis(3′-indolyl)-1-(p-anisyl)methane (DIM-C-pPhOCH3), in CRC cells. It was found to inhibit cell growth, survival, migration, and invasion while inducing apoptosis by elevating the expression of TRAIL, PARP, PDCD1, CSE, ATF3, and CSE and activating caspases -3, -8, and -9 [107, 197, 199, 201].
Moreover, another orphan NR, Nurr1, also known as nuclear receptor 4 group A, gene 2 (NR4A2), belongs to the same NR subfamily of Nur77 [276]. Nurr1 is expressed ubiquitously throughout the body and grouped under gene 2 (NR4A2). It is a transcriptional regulator that is crucial for the formation, maintenance, and differentiation of meso-diencephalic dopaminergic (mdDA) neurons [278, 348, 353]. It is necessary for the transcription of a group of genes, including SLC6A3, SLC18A2, tyrosine hydroxylase, and DRD2, whose expression is required for the growth of mdDA neurons [353]. NR4A2 further serves as a significant and critical junction linking the eicosanoid and fatty acid metabolic pathways through its transcriptional integration. Moreover, it was also observed that induction of NR4A2 by PGE2 resulted in binding to the Nur77-binding response element located within the peroxisome proliferator response element, activating the fatty acid oxidation genes, including FABP2, FABP4, ACOX, and CPT1M. Thus, PGE2 can be used to regulate the shift toward fatty acid oxidation, which is observed in several types of cancer, to control energy utilization [204]. Nurr1 was also reported to play a pivotal role in the development and progression of CRC [348]. Another study by Holla et al., reported that activation of Nurr1 by PGE2 promoted cell survival by inducing fatty acid oxidation and its associated proteins in LS-174 T and HCT-116 CRC cells. Thus, this study suggests the role of Nurr1 in regulating the process of ATP generation in CRC cells [204]. The precise mechanism by which Nur77 acts as an oncogene and tumor suppressor gene in CRC is still not well understood. Further investigation is warranted to better understand the intricate roles of Nur77 and Nurr1 in the development of colorectal tumors, and to develop therapeutic strategies that can be used to target these genes in order to improve the clinical outcomes of CRC patients.
3.10 Progesterone receptor (PR)
PR, identified as nuclear receptor subfamily 3, group C, gene 3 (NR3C3), is a ligand-dependent transcription factor belonging to the NR family. Its primary function involves the regulation of target gene expression through binding with its specific steroid hormone ligand, progesterone (P4). Further, PR serves as a central controller in processes such as proliferation, differentiation, and development, particularly during the reproductive cycle and pregnancy in female reproductive tissues [354, 355]. Studies have implicated a potential association between the PR levels and the risk of CRC. For instance, various studies have indicated an upregulation of PR expression in CRC tissues compared to normal mucosa [76, 122]. In another study, Zhang et al., proposed that decreased expression of PR and its ligand, P4, correlates with an unfavorable prognosis in CRC patients. Treatment of P4 inhibited cell proliferation, induced cell cycle arrest, and promoted apoptosis. These effects were mediated through the activation of the JNK pathway via DNA damage-inducible protein α (GADD45α), leading to the suppression of malignant progression in CRC. Additionally, P4 treatment resulted in reduced tumor volume and weight in CRC xenografts, suggesting a potential inhibitory role for P4 and PR in improving the prognosis of CRC patients [123]. Further, treatment with E2 and P4 induced apoptosis by enhancing the expression of PCNA and upregulating cleaved PARP, caspase-3, and cleaved caspase-8 levels in vivo [160]. Furthermore, folic acid (FA) treatment significantly attenuated the proliferation rate of PR-positive COLO-205, HT-29, and LoVo cells by activating c-Src and inducing the expression of cell cycle regulators p21, p27, and p53. However, this effect was nullified by pre-treatment with a PR-specific antagonist, Org 31710, highlighting the involvement of PR in FA-mediated inhibition of proliferation [247]. Taken together, PR emerges as a pivotal NR in regulating mechanisms associated with cell growth, proliferation, and apoptosis in the context of CRC.
3.11 Peroxisome proliferator-activated receptors (PPARs)
The PPARs belong to the NR superfamily, which plays a crucial function in lipid and glucose metabolism and acts as a ligand-inducible TF [356]. PPARs are present in 3 isoforms—PPARα, PPARβ/δ, and PPARγ and are classified as nuclear receptor subfamily 1, group C (PPARα-NR1C1; PPARβ/δ-NR1C2; PPARγ-NR1C3) in the current nomenclature system [356, 357]. The three PPARs are variably expressed in various tissues [358]. PPARβ/δ is more widespread; however, it is mostly found in skin, skeletal muscle, heart, adipose tissue, liver, and inflammatory cells. PPARγ comprises three distinct variant isoforms (γ1, γ2, and γ3) with different tissue localization [358]. All the isoforms of the PPARs form heterodimers with RXR to either activate or repress the downstream target genes. They are known to regulate multiple conditions, such as hypertension, inflammation, and atherosclerosis [356]. Further, due to the special role of PPARβ/δ, this receptor is known as an important therapeutic target for various disorders, including cancer [359]. Furthermore, it has also been observed that designing agonists of PPARs, might improve its therapeutic values in cancer [356]. Studies have reported the activation/suppression of PPARβ and PPARδ expression in various cancer cell models have resulted in the modulation of CRC [111, 117, 360]. In several studies, it was exhibited that PPARs were highly upregulated in CRC models [111,112,113,114, 116,117,118]. Contrastingly, few studies have also reported the downregulation of PPARs in CRC [109, 110, 115]. PPAR activation has been shown to decrease cell growth as well as trigger differentiation and apoptosis in a range of cancer cell types [361,362,363]. With regard to this, combined treatment of indomethacin with 5-FU significantly reduced tumor growth by activating PPARγ and suppressing the expression of PROM 1, CD44, PTGS2, and HES1 in SW620 xenograft mice [212]. The treatment of PPAR ligand, rosiglitazone, was found to suppress tumor growth in HCT-116-XIAP(−/−) xenograft model via the upregulation of PTEN [227]. Moreover, PPARγ ligand thiazolidinedione (TZD) was demonstrated to suppress cell growth, metastasis and induce G1 phase arrest by upregulating the expression of p21Waf-1, Drg-1, and E-cadherin and reducing tyrosine phosphorylation of β-catenin in HT-29 cells. Further, TZD treatment was also found to block lymph nodes and lung metastasis in xenograft mice [223]. In addition, the treatment of pioglitazone and 15-deoxy-delta (12,14)-prostaglandin J2 (15-d Δ PGJ2) blocked the proliferation, invasion and initiated G1 phase cell cycle arrest by suppressing MMP-7 and elevating TIMP-1 level in SW480 and LS174T cell lines [225]. Another study demonstrated that the overexpression of miR-506 in an HCPT-resistant colorectal carcinoma cell line contributed to the resistance against HCPT by suppressing PPARα expression. These findings offer a scientific basis for formulating miRNA-centered therapeutic approaches to counter drug resistance in HCPT-resistant CRC [218]. The induction of PPARγ by bitter melon oil (BMO) (Momordica charantia) was also found to suppress tumor growth in a rat model [213]. Another PPAR agonist, troglitazone, was found to induce apoptosis and G0/G1 cell cycle arrest by attenuating the expression of NF-κB, and GSK-3β in SW620 and HCT-116 cells [215]. Additionally, amorfrutin C, a PPARγ agonist having low affinity for PPARγ, was shown to inhibit cell proliferation and induce apoptosis by disrupting mitochondrial integrity and inducing caspases, DNA fragmentation, PARP cleavage, externalization of phosphatidylserine, and ROS generation in HT-29 cells [234]. Further, the activation of PPARγ with 6-shogaol initiated apoptotic cell death by suppressing the activity of NF-κB in HT-29 cells [118]. Furthermore, Mielczarek-Puta et al., showed that linoleic acid (LA), a PPARγ agonist, decreased the cell viability and proliferation in SW480 and SW620 cells in a concentration-dependent manner [235]. It was also found that silencing of PPARδ increased cell proliferation by enhancing the expression of VEGF in KM12C cells while this effect was reversed by bevacizumab, a specific VEGF inhibitor [216]. Moreover, troglitazone treatment was found to repress cell growth in various colon cancer cells in vitro [364]. Additionally, the treatment of several agonists such as troglitazone, pioglitazone, and rosiglitazone, suppresses tumor growth and ACF formation in mice, suggesting a possible involvement of PPAR at the initial phase of CRC development [233]. Further, the treatment with GW0742, Wy-14,643, and troglitazone induced markers involved in colonocyte differentiation, along with other markers such as ADRP, FABP, keratin 20, and KLF4 in PPARβ+/+ mouse model [109]. Contrastingly, it was reported that the low dosage of PPARγ ligand 15-d Δ PGJ2 and pioglitazone promoted cell growth and tumor growth in APC-mutated HT-29 cells and its xenograft mouse model, respectively, by elevating the expression of c-Myc, and β-catenin [226]. Moreover, Zou et al., has reported that GW501516, a PPARδ agonist, increased the expression of Glut1 and SLC1A5 in SW480 cells and enhanced the colitis-associated CRC by inducing pro-inflammatory genes, such as COX-2, IL-6, IL-8, and MCP-1 in AOM/DSS-exposed mice [220].
Several clinical trials targeting PPARα and PPARγ receptors are currently ongoing for the treatment of different cancers [http://clinicaltrials.gov/]. In a Phase I, multicenter clinical trial, combinatorial treatment of efatutazone, a selective PPAR-γ agonist and paclitaxel was found to be safe and well tolerable in 15 patients of anaplastic thyroid cancer. Moreover, it was found that angiopoietin-like 4 was induced by the treatment of efatutazone in the biopsy samples of patients [365]. Another dose escalated clinical study determined the effectiveness of efatutazone in solid malignancies patients. It was observed that 0.5 mg twice daily was safe and induced a sustained partial response in a patient with myxoid liposarcoma. Moreover, the treatment also showed stable disease (SD) response for more than 60 days in 10 patients [366]. Komatsu and group evaluated the efficacy of efatutazone in conjunction with FOLFIRI treatment against metastatic CRC. Combinatorial treatment had significant safety profile and stable disease progression with increased levels of adiponectin in plasma [367]. Recently, a Phase I interventional clinical trial (ClinicalTrials.gov ID NCT03829436) is ongoing to explore the tolerability, safety and tumor inhibiting activity of TPST-1120, selective antagonist of PPARα as monotherapy and with nivolumab, an anti-PD1 antibody against solid tumors including CRC. It is now well known that targeting PPARs could be an important approach in the battle against CRC, although, it is a long road ahead for successfully establishing PPARs in clinical settings. The major drawback for PPAR based therapy is the differential expression of the PPARs in various cancers and its context dependent response, thereby impeding the development of a universal and common PPAR agonist or antagonist for all cancers. Moreover, the off targets effects induce side effects which could be detrimental in the treatments. With the advent of advanced omics and technologies, it is prudent to develop reliable biomarkers which could help in predicting the therapy response in CRC that could pave the way for integrating personalized medicine approach in NRs based treatments. Hence these findings suggest the role of PPARs in CRC, and targeting this group of NRs with its ligands is of significant importance for the management of CRC.
3.12 Pregnane X receptor (PXR)
PXR, also known as nuclear receptor subfamily 1, group I, gene 2 (NR1I2), is a prototypical member of the NR superfamily, which is known to be stimulated by the endobiotics and xenobiotics [368]. PXR being a key xenobiotic receptor generally binds to the regulatory gene sequences in a ligand-dependent manner [369]. Detoxification, metabolism, and inflammation are some of the common downstream targets of PXR in xenobiotic responses [368]. It was also reported that PXR signaling was involved in various biological process like proliferation, apoptosis, cell cycle arrest, angiogenesis, and oxidative stress [368]. PXR is widely expressed in both normal and malignant tissues [370]. Moreover, it was also reported that PXR has a crucial role in cancer stem cells (CSC)-mediated tumor recurrence. In addition, it was also observed that its expression in CSCs plays an important role in modulating gene expressions that are involved in chemoresistance and self-renewal [238].
Several studies have reported that PXR is variably expressed in various CRC cell lines and tissues which might regulate different processes of colon carcinogenesis [119,120,121]. Overexpression of miR-148a was found to suppress the expression of PXR along with DNMT1, FGF-19, ALDH1A1, ABCG2, CYP3A4, and CD44, which subsequently inhibited tumorsphere formation in HT-29 cells. Moreover, the overexpression of miR-148a also led to decreased CSC chemoresistance in HT-29 xenograft mice [237]. However, in another study, it was shown that PXR was downregulated in colon tumors and the ectopic upregulation of PXR inhibited cell proliferation and elevated G0/G1 cell cycle arrest by upregulating p21(WAF1/CIP1) and reducing E2F1 expression in HT-29 cells. Moreover, the ectopic expression of PXR was found to reduce tumor size and weight in HT-29 xenograft mice [119]. Moreover, the overexpression of PXR was associated with poor recurrence-free survival in CRC patients [238]. However, in an in vivo study, it was found that the knockdown of PXR induced the chemosensitivity and ameliorated the self-renewal property of CSCs and slowed down the process of tumor recurrence in a mouse model exposed to chemotherapeutic drug [238]. In addition, several preclinical studies have demonstrated the efficacy of the chemotherapeutic drug rifaximin in inhibiting proliferation and inducing apoptosis in CRC experimental models by upregulating hPXR and suppressing the expression of various molecules such as VEGF, MMP-2, MMP-9, VEGFR-2, iNOS, p-Akt, p-mTOR, p-p70S6K, HIF-1α, p-p38MAPK, TNF-α, iNOS, IL-6, IL-10, and NF-κB [239, 241, 244]. Further, the treatment of CRC cells with rifampicin enhanced the expression of PXR, SP1, and MRP3, which suggests the role of PXR in inducing resistance to chemotherapeutic agents in CRC cells [121]. Furthermore, baicalein, a herbal flavonoid was found to activate PXR in a Cdx2-dependent manner, suggesting the potential involvement of PXR in inducing anti-inflammatory and anti-cancer activities in CRC. Baicalein treatment was also shown to reduce MDR1 and CYP3A11 expressions in PXR+/+ in vivo model [242]. In another study, the treatment of LS174T cells with fucoxanthin attenuated the drug resistance by suppressing rifampin-induced multiple drug resistance 1 (MDR1) and cytochrome CYP3A4 mRNA expression via PXR-mediated pathways [243]. However, a study by Zimmermann et al., showed that glucocorticoids like budesonide induced the expression of molecules involved in drug metabolisms like CYP3A4 and CYP3A11 via modulation of PXR [240]. Moreover, in a study, it was reported that methylation of the PXR promoter modulated the mRNA expression of PXR and CYP3A4 in CRC cell lines, suggesting the involvement of PXR/CYP3A4 axis during colon carcinogenesis and drug responses. However, the treatment of CRC cells, Caco2, HT-29, HCT-116, and SW480, with 5-Aza-dC, reversed the process of DNA methylation [246]. Therefore, PXR plays an important role in several processes of drug response and metabolism and could be an important target to overcome drug resistance in CRC.
3.13 Retinoid X receptors (RXR)
RXRs, also known as nuclear receptor subfamily 2 group B (NR2B), a member of the NR superfamily, which mainly consists of three isoforms, i.e., α, β, and γ, are found in every cell type in humans [276, 371, 372]. It plays an important role in nutrient metabolism through heterodimerization with other NRs such as CAR, FXR, LXR, PPAR, PXR, etc. [372]. RXR was also reported to suppress cell proliferation and induce apoptosis in various cancers by its homodimerization with selective agonists or rexinoids [124, 372, 373]. Studies have shown that RXRα was downregulated in CRC tumorigenesis, as confirmed in CRC tissues and in vivo mouse models [126, 127]. However, some studies have also reported the upregulation of RXR in CRC and its association with the induction of other molecules involved in the RA pathway, such as ALDH1, RAR, CYP26A1, and CtBP1 [124, 125]. The different findings on the expression of RXRs in CRC can be influenced by a wide pleotropic factors including tumor stage differences, genetic backgrounds, and experimental procedures used in the investigations. These variables may contribute to the disparities and variabilites observed in RXR expression levels and functional roles in CRC. For instance, tumor stage is an important factor to consider when evaluating RXR expression in CRC. RXR expression levels may differ at different phases of CRC development and progression [126]. Some studies, for example, have found decreased RXR expression in advanced CRC stages, implying that RXRs may play a role in early tumorigenesis [126, 127]. However, few findings have showed elevated RXR expression in certain CRC cases, revealing a possible connection with tumor growth or resistance to therapeutic interventions [124, 125]. As a result, changes in tumor stage distribution between study cohorts can alter the overall conclusions about RXR expression in CRC. As it is well known that CRC being the heterogeneous disease has varied genetic alterations, RXR expression and function can be influenced by genetic factors such as mutations in important signaling pathways or transcriptional regulators. These genetic variances across patients can result in changes in RXR expression profiles [126]. The heterogeneity in experimental methodologies used to determine RXR expression may also contribute to the contradictory results. Discrepancies in the expression could occur due to differences in sample collection, RNA extraction, and quantitative methodologies for detecting RXR expression levels. Furthermore, changes in antibody specificity and sensitivity in immunohistochemistry or immunofluorescence assays can impact RXR protein expression detection and interpretation. Janakiram et al., revealed that induction of RXR with its agonist, β-ionone, inhibited cell proliferation and induced G1/S-phase cell cycle arrest and apoptosis in HCT-116 cells. Further, activation of RXRα also inhibited AOM-induced ACF in colon carcinogenesis in a rat model [126]. Similarly, a study by the same group showed that treatment with bexarotene, an RXRα agonist, suppressed colon tumorigenesis by inhibiting cyclin D1, COX-2, and PCNA in Apc (Min/+) mouse model. In addition, dose-dependent treatment of bexarotene also suppressed serum triglycerides and inflammatory cytokines in a mouse model [251]. Studies have also reported that berberine and its analog 3,9-dimethoxy-5,6-dihydroisoquinolino [3,2-a] isoquinolin-7-ium chloride (B-12) activate RXRα, which further leads to the reduction of cell growth by downregulating the Wnt/β-catenin pathway in CRC cells. Subsequently, it was observed that the shRXRα KM12C cell xenograft model treated with berberine resulted in the suppression of tumor growth [252, 253].
The phosphorylation of RXRα was associated with colon carcinogenesis; however, inhibition of this phosphorylation and inducing the heterodimerization of unphosphorylated RXR–PPARγ in the presence of their ligands, 9-cisRA, and ciglitazone, synergistically suppressed cell growth and induced apoptosis by reducing COX-2 and c-Jun at both protein and RNA level [124]. Moreover, the combination of RXR and PPARγ agonists, bexarotene and rosiglitazone respectively, inhibited cell growth by suppressing COX-2 and PGE2 while increasing carcinoembryonic antigen (CEA) in Moser CRC cells. The combination treatment was also found to suppress tumor growth in Moser cells xenograft mouse model [248]. In addition, the treatment of ATRA-resistant HCT-116, WiDr, and SW620 cells with retinol suppressed cancer cell growth by augmenting the proteasomal degradation of β-catenin via the RXR-mediated pathway [249]. Further, it was shown that DHA induced a chemopreventive effect against colon carcinogenesis by modulating RXR-PPAR axis in YAMC and NCM460 cells [250]. A bioactive component of green tea, epigallocatechin-3-gallate (EGCG), was also found to inhibit cell proliferation and induced G1/S phase cell cycle arrest by upregulating the expression of RXRα and suppressing β-catenin, cyclin D1, and DNA methyltransferase activity in CRC cell lines [127]. Moreover, the combined treatment of sodium valproate (VPA), an HDAC inhibitor, with a RXR ligand, 6-OH-11-O-hydroxyphenanthrene (IIF), was found to induce apoptosis and reduce cell viability and invasion by increasing the expression of RXRγ and apoptotic proteins such as Bax and cleaved caspase-3 and -9, tissue inhibitor matrix metalloproteinase 1 (TIMP1) and TIMP2 while reducing Bcl-2, MMP-2, and MMP-9 in HT-29 cells [254]. Further, the combination of IIF with ciglitazone was demonstrated to enhance apoptosis and attenuate cell growth and migration by elevating RXRγ, PPARγ, TIMP1, and TIMP2 and inhibited the expression of COX-2, MMP-2, MMP-9 and PGE2 in HCA-7 and HCT-116 cells [236]. Hence, RXRs play a crucial role in cell proliferation and survival, thereby modulating RXRs with specific agonists or antagonists might be beneficial in the treatment and management of CRC.
3.14 Thyroid hormone receptors (THR)
The THRs along with their isotypes THRα1, and THRβ1 belong to the NR superfamily that regulates thyroid hormone signaling in various tissues to mediate numerous important developmental and physiological processes [374]. They are mainly known for their role as ligand-dependent TFs, and the THRs bind to the thyroid hormone RE irrespective of the presence or absence of thyroid hormone to modulate the expression of target genes [374]. It was observed that the expression of THR was upregulated in thyroid cancer patients [375]. In addition, the levels of THRα1 was also highly upregulated in human CRC patients and was found to modulate the Wnt pathway [128]. However, Horkko et al., reported that the expression of THRβ1 was higher in normal human mucosa when compared to CRC samples. This expression study suggests that the downregulation of this NR at an advanced stage suggests its tumor-suppressive function [129]. THRs expression patterns in CRC have revealed inconsistent results in several studies, and multiple variables could contribute to these variations. Tumor stage, genetic background, and experimental procedures used in the investigations are all potential variables impacting the reported THR expression differences. For instance, THRs subtypes expression levels could differ at different stages of CRC development and progression. Some studies, for example, have found lower THRβ1 expression in advanced CRC stages, implying that THRβ1 may play a tumor-suppressive function in early carcinogenesis. THRs might have potential therapeutic implications in CRC treatment, particularly in terms of cell viability, cell cycle arrest, and reduction in tumor growth [128, 129]. Preclinical investigations have shown that activating THRs with thyroid hormone analogues or synthetic ligands reduces CRC cell survival. These ligands bind to THR and regulate gene expression as well as signaling pathways involved in cell proliferation, survival, and apoptosis. The downstream effects include cell cycle arrest at several checkpoints, such as the G1 and G2/M phases, as well as the stimulation of apoptosis in CRC cells. Moreover, THR activation has been shown to increase the susceptibility of cancer including CRC to conventional chemotherapeutic drugs, resulting in better treatment outcomes [376, 377]. THR agonists have also been studied as prospective combination therapy with other targeted medicines, such as EGFR inhibitors, to alleviate efficacy and overcome resistance mechanisms [376]. In this context, a study by Natsume and group demonstrated that the inhibition of endogenous wild type β-catenin with triiodothyronine (T3)/THRβ1 in SW480 cells with mutation of the APC gene resulted in the inhibition of cyclin D1 through the Tcf/Lef-1 site [255]. Moreover, activation of THRβ1 by its agonist, GC-1, was found to induce an anti-proliferative effect by decreasing cell viability and increasing G1 phase arrest in CT26 and SW480 cells. In the same study, treatment of GC-1 showed a tremendous reduction in tumor growth in CT26 xenograft mouse model [256]. Thus, these studies suggest the significant importance of THR in the management of CRC; however, more studies are warranted to explore the potential mechanism behind the role of this NR in CRC.
3.15 Vitamin D receptor (VDR)
VDRs belong to the NHR superfamily, which acts as ligand-inducible TFs [378]. VDR is expressed in all tissues of the bone, breast, colon, kidney, lung, ovary, pancreas, etc. [379]. Several co-activator complexes are essential for the ligand-mediated transactivation of VDR [378]. Most of the biological processes involving vitamin D are known to be exerted through VDR and mediate processes like cell proliferation, differentiation, and calcium homeostasis [378, 379]. Studies have also shown the role of vitamin D and its receptor in cancer [379,380,381]. In CRC, VDR has anti-cancer properties and was found to be downregulated in CRC cells and tissues [130,131,132,133, 135, 137, 138]. However, few studies have also reported that the expression of VDR was upregulated in CRC tissues compared to normal adjacent tissues [134, 136]. Moreover, it was shown that the expression of VDR was sequentially upregulated from normal to a well-differentiated tumor while decreasing in poorly differentiated tumor [379].
VDR was first identified as a biomarker for vitamin D-mediated suppression of cell proliferation in human colon cancer [382]. VDR and its ligands play an important role in the regulation of several genes and signaling pathways linked to CRC. The activation of VDR by its ligands, such as 1,25-dihydroxyvitamin D3 (calcitriol), impacts gene expression and many cellular processes in colon cancer cells. In the colon, VDR activation has been demonstrated to decrease cell proliferation, promote differentiation, induce apoptosis, and suppress inflammation [383]. VDR signaling also interacts with critical pathways involved in colon cancer, such as Wnt/β-catenin, PI3K/Akt, and MAPK signaling. Further, several types of immune cells express VDR and are controlled by calcitriol, which may contribute to its anti-CRC activity. Given the relevance of the intestinal microbiota in CRC and the discovery that it is affected by vitamin D deficiency, an indirect antitumoral action of calcitriol at this level could be vital in CRC progression [384]. For instance, it was shown that 25(OH)D3, a VDR ligand, exhibited an anti-proliferative effect and induced apoptosis by regulating the expression of VDR in SW480 cells [379]. Additionally, 1,25(OH)2D3, a high-affinity VDR ligand, was known to regulate the transcription of various genes in CRC by activating VDR and modulating its binding to the target genes such as β-catenin [385]. Further, the AOM/DSS-induced colon carcinogenesis was associated with the inhibition of VDR and upregulation of Snail1, Snail2, COX-2 and iNOS in a murine model [132]. Furthermore, many studies have demonstrated the role of 1,25-(OH)2D3 in regulating VDR and various other genes such as TNF-α, CYP3A4, c-FOS, c-Jun, CCND1, Snail1, Snail2, CDH1, AXIN2, TCF-4, TCF7L2, etc. to exhibit anti-cancer property by suppressing the CRC hallmarks [259, 261, 262, 270, 274]. In another study, it was shown that the treatment of SW480 and HCT-116 cells with ZnCl2 induced the expression of MT1A, MT2A, and 1,25(OH) 2D3-induced cadherin 1, thus suggesting the linkage of VDR with zinc signaling in CRC [269]. Thus, VDR and its ligand play a pivotal role in regulating different signaling and molecules associated with CRC.
4 Conclusion
Despite the advancement in recent research, colon cancer remains one of the most common malignancies globally. The diagnosis of CRC at an advanced stage is linked to poor prognosis and diminished survival outcomes among patients. Thus, it is necessary for the identification of biomarkers that could be a target for the management of CRC. Regarding this, NRs were known to be deregulated and differentially expressed in CRC and were shown to modulate different processes associated with this cancer. The different NRs, such as AR, EAR 2, ER, ERR, FXR, HNF4α, LRH-1, LXR, Nur77, PPAR, PXR, PR, RXR, THR, and VDR, were found to modulate different signaling pathways such as NF-κB, Wnt/β-catenin, MAPK, etc. These NRs and their modulators (agonists/antagonists) were found to regulate various proteins and genes associated with major pathways involved in CRC progression, which subsequently led to the suppression of cell survival, proliferation, migration, invasion, and induction of apoptosis in CRC. Further, several agonists and antagonists of NRs have been shown to enhance the anti-tumor efficacy through a combinatorial approach with other anti-cancer compounds, such as bexarotene and raloxifene in CRC [94, 126]. Growing lines of evidence have established that NRs targeting could be a viable treatment intervention in CRC, although this treatment modality has its own set of limitations and challenges. The intricacy of NRs signaling pathways is the major limitation in treatment, as NRs can have varied and context-dependent consequences on tumor progression and therapy response. Further, the differential expression levels and transcriptional activity of NRs amongst various cancer types, makes it improbable to develop a universal NR-targeted therapy. Furthermore, the off-target effects and acquisition of drug resistance against NR agonists and antagonists can have unanticipated results and debilitating side effects. Further research in exploring the intricate cross talk and mechanistic action of NRs is vital in developing putative targets that can be exploited for diagnosis, prognosis and therapeutic approaches for CRC. Moreover, randomized, double blind, multicentered clinical trials are necessary for establishing the safety and efficacy of these agonists and antagonists. Overall, while NRs show potential as cancer therapeutic targets, addressing these limits and obstacles are crucial for their effective and safe implementation in clinical settings for CRC. Due to this, several clinical trials are currently being carried out to investigate the potential of NR-targeting small molecules as CRC therapeutics.
Data availability
Not applicable.
Abbreviations
- 5-oxo-ETE:
-
5-Oxoeicosatretraenoic acid
- 15-d Δ PGJ2:
-
15-Deoxy-delta (12,14)-prostaglandin J2
- ACF:
-
Aberrant crypt foci
- Akt:
-
Protein kinase B
- ALP:
-
Alkaline phosphatase;
- AOM:
-
Azoxymethane
- AP1:
-
Activator protein 1
- APC:
-
Adenomatous polyposis coli
- AR:
-
Androgen receptor
- B-12:
-
3,9-Dimethoxy-5,6-dihydroisoquinolino [3,2-a] isoquinolin-7-ium chloride
- BAR:
-
Bile activated receptor
- Ber:
-
Berberine
- THR:
-
Thyroid hormone receptor
- CAF:
-
Cancer-associated fibroblasts
- CAR:
-
Constitutive androstane receptor
- CDH 1:
-
Cadherin 1
- ChIP:
-
Chromatin immunoprecipitation
- CRC:
-
Colorectal cancer
- CSC:
-
Cancer stem cells
- DBD:
-
DNA-binding domain
- DHA:
-
Docosahexaenoic acid
- DKK 1:
-
Dickkopf Wnt signaling pathway inhibitor 1
- DSS:
-
Dextran sulfate sodium
- EAR2:
-
v-Erb A related-2
- ECGC:
-
Epigallocatechin- 3-gallate
- EGFR:
-
Epidermal growth factor receptor
- ER:
-
Estrogen receptor
- EREs:
-
Estrogen-responsive elements
- ERR α :
-
Estrogen related receptor alpha
- ERRγ :
-
Estrogen related receptor gamma
- ERα :
-
Estrogen receptor alpha
- ERβ :
-
Estrogen receptor beta
- Ex4:
-
Exendin 4
- FGF 2:
-
Fibroblast growth factor 2
- FXR:
-
Farnesoid X receptor
- GA:
-
Glycyrrhetinic acid
- GL:
-
Glycyrrhizin
- GLP1R:
-
Glucagon-like peptide-1 receptor
- Glut1:
-
Glucose transporter 1
- HDI:
-
Human development index
- HIF-1α :
-
Hypoxia-inducible factor 1-alpha
- HMGB1:
-
High mobility group box 1
- HNF4α :
-
Hepatocyte nuclear factor 4 alpha
- HRT:
-
Hormone-replacement therapy
- JNK:
-
C-Jun N-terminal kinases
- LA:
-
Linoleic acid
- LCA:
-
Lens culinaris agglutinin
- LDHA:
-
Lactate dehydrogenase A
- lncRNAs:
-
Long non-coding RNAs
- LRH1:
-
Liver receptor homolog 1
- LXR:
-
Liver X receptors
- MCT4:
-
Monocarboxylate transporter 4
- mdDA:
-
Meso-diencephalic dopaminergic
- MEK:
-
Mitogen-activated protein kinase kinase
- miRNA:
-
MicroRNA
- MMP 7:
-
Matrix metalloproteinase 7
- mRNA:
-
Messenger RNA
- mtDNA:
-
Mitochondrial DNA
- NF:
-
Normal fibroblasts
- NF-κB:
-
Nuclear factor kappa B
- NGFI-B alpha:
-
Nerve growth factor-induced B alpha
- NR:
-
Nuclear receptor
- Nur77:
-
Nuclear hormone receptor 77
- OCA:
-
Obeticholic acid
- OPN:
-
Osteopontin
- OS:
-
Overall survival
- PCNA:
-
Proliferating cell nuclear antigen
- PDK1:
-
3-Phosphoinositide-dependent kinase 1
- PEPCK:
-
Phosphoenolpyruvate carboxykinase
- PGC-1α :
-
Peroxisome proliferator-activated receptor gamma coactivator 1-alpha
- PGRMC1:
-
Progesterone receptor membrane component 1
- PI3K:
-
Phosphoinositide 3-kinase
- PPAR:
-
Peroxisome proliferator-activated receptors
- PR:
-
Progesterone receptor
- PSF:
-
PTB-associated splicing factor
- PXR:
-
Pregnane X receptor
- RAR:
-
Retinoic acid receptor
- ROS:
-
Reactive oxygen species
- RXR:
-
Retinoid X receptors
- SF 1:
-
Steroidogenic factor-1
- shRNA:
-
Short hairpin RNA
- siFXR:
-
Fxr-small interfering RNA
- TIMP:
-
Tissue inhibitor metalloproteinase
- OXER1:
-
Oxoeicosanoid receptor 1
- TCA:
-
Tricarboxylic acid cycle
- TF:
-
Transcription factor
- TGFβ :
-
Transforming growth factor β
- TNF-α :
-
Tumor necrosis factor alpha
- THR:
-
Thyroid Hormone Receptor
- TRPM8:
-
Transient receptor potential melastatin 8
- TZD:
-
Thiazolidinedione
- UTR:
-
Untranslated region
- VDAC1:
-
Voltage-dependent anion channel 1
- VDR:
-
Vitamin D receptor
- VEGF:
-
Vascular endothelial growth factor
References
Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, Bray F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71:209–49. https://doi.org/10.3322/caac.21660.
Cheng L, Eng C, Nieman LZ, Kapadia AS, Du XL. Trends in colorectal cancer incidence by anatomic site and disease stage in the United States from 1976 to 2005. Am J Clin Oncol. 2011;34:573–80. https://doi.org/10.1097/COC.0b013e3181fe41ed.
Thanikachalam K, Khan G. Colorectal cancer and nutrition. Nutrients. 2019. https://doi.org/10.3390/nu11010164.
Siegel RL, Miller KD, Goding Sauer A, Fedewa SA, Butterly LF, Anderson JC, Cercek A, Smith RA, Jemal A. Colorectal cancer statistics, 2020. CA Cancer J Clin. 2020;70:145–64. https://doi.org/10.3322/caac.21601.
Clinton SK, Giovannucci EL, Hursting SD. The world cancer research fund/American institute for cancer research third expert report on diet, nutrition, physical activity, and cancer: impact and future directions. J Nutr. 2020;150:663–71.
Harsha C, Banik K, Bordoloi D, Kunnumakkara AB. Antiulcer properties of fruits and vegetables: a mechanism based perspective. Food Chem Toxicol. 2017;108:104–19. https://doi.org/10.1016/j.fct.2017.07.023.
Grassadonia A, Di Marino P, Ficorella C, Cortellini A, Cannita K, Parisi A, Gamucci T, Zoratto F, Vici P, Barba M, et al. Impact of primary tumor location in patients with RAS wild-type metastatic colon cancer treated with first-line chemotherapy plus anti-EGFR or anti-VEGF monoclonal antibodies: a retrospective multicenter study. J Cancer. 2019;10:5926–34. https://doi.org/10.7150/jca.34550.
Siegel RL, Miller KD, Fedewa SA, Ahnen DJ, Meester RGS, Barzi A, Jemal A. Colorectal cancer statistics, 2017. CA Cancer J Clin. 2017;67:177–93. https://doi.org/10.3322/caac.21395.
Siegel RL, Wagle NS, Cercek A, Smith RA, Jemal A. Colorectal cancer statistics, 2023. CA Cancer J Clin. 2023;73:233–54. https://doi.org/10.3322/caac.21772.
Schreuders EH, Ruco A, Rabeneck L, Schoen RE, Sung JJ, Young GP, Kuipers EJ. Colorectal cancer screening: a global overview of existing programmes. Gut. 2015;64:1637–49. https://doi.org/10.1136/gutjnl-2014-309086.
Siegel RL, Ward EM, Jemal A. Trends in colorectal cancer incidence rates in the United States by tumor location and stage, 1992–2008. Cancer Epidemiol Biomarkers Prev. 2012;21:411–6. https://doi.org/10.1158/1055-9965.EPI-11-1020.
Sanchez-Guillen L, Arroyo A. Immunonutrition in patients with colon cancer. Immunotherapy. 2020;12:5–8. https://doi.org/10.2217/imt-2019-0179.
Kumar A, Singam A, Swaminathan G, Killi N, Tangudu NK, Jose J, Gundloori Vn R, Dinesh Kumar L. Combinatorial therapy using RNAi and curcumin nano-architectures regresses tumors in breast and colon cancer models. Nanoscale. 2022;14:492–505. https://doi.org/10.1039/d1nr04411g.
Filip S, Vymetalkova V, Petera J, Vodickova L, Kubecek O, John S, Cecka F, Krupova M, Manethova M, Cervena K, et al. Distant metastasis in colorectal cancer patients-do we have new predicting clinicopathological and molecular biomarkers? A comprehensive review. Int J Mol Sci. 2020. https://doi.org/10.3390/ijms21155255.
Muralimanoharan SB, Kunnumakkara AB, Shylesh B, Kulkarni KH, Haiyan X, Ming H, Aggarwal BB, Rita G, Kumar AP. Butanol fraction containing berberine or related compound from nexrutine inhibits NFkappaB signaling and induces apoptosis in prostate cancer cells. Prostate. 2009;69:494–504. https://doi.org/10.1002/pros.20899.
Sajeev A, Hegde M, Daimary UD, Kumar A, Girisa S, Sethi G, Kunnumakkara AB. Modulation of diverse oncogenic signaling pathways by oroxylin A: an important strategy for both cancer prevention and treatment. Phytomedicine. 2022;105:154369. https://doi.org/10.1016/j.phymed.2022.154369.
Sajeev A, Hegde M, Girisa S, Devanarayanan TN, Alqahtani MS, Abbas M, Sil SK, Sethi G, Chen JT, Kunnumakkara AB. Oroxylin A: a promising flavonoid for prevention and treatment of chronic diseases. Biomolecules. 2022. https://doi.org/10.3390/biom12091185.
Kunnumakkara AB, Sung B, Ravindran J, Diagaradjane P, Deorukhkar A, Dey S, Koca C, Tong Z, Gelovani JG, Guha S, et al. Zyflamend suppresses growth and sensitizes human pancreatic tumors to gemcitabine in an orthotopic mouse model through modulation of multiple targets. Int J Cancer. 2012;131:E292-303. https://doi.org/10.1002/ijc.26442.
Padmavathi G, Rathnakaram SR, Monisha J, Bordoloi D, Roy NK, Kunnumakkara AB. Potential of butein, a tetrahydroxychalcone to obliterate cancer. Phytomedicine. 2015;22:1163–71.
Henamayee S, Banik K, Sailo BL, Shabnam B, Harsha C, Srilakshmi S, Vgm N, Baek SH, Ahn KS, Kunnumakkara AB. Therapeutic emergence of rhein as a potential anticancer drug: a review of its molecular targets and anticancer properties. Molecules. 2020;25:2278.
Nair A, Amalraj A, Jacob J, Kunnumakkara AB, Gopi S. Non-curcuminoids from turmeric and their potential in cancer therapy and anticancer drug delivery formulations. Biomolecules. 2019;9:13.
Singh YP, Girisa S, Banik K, Ghosh S, Swathi P, Deka M, Padmavathi G, Kotoky J, Sethi G, Fan L. Potential application of zerumbone in the prevention and therapy of chronic human diseases. J Funct Foods. 2019;53:248–58.
Devi Daimary U, Girisa S, Parama D, Verma E, Kumar A, Kunnumakkara AB. Embelin: A novel XIAP inhibitor for the prevention and treatment of chronic diseases. J Biochem Mol Toxicol. 2022;36:e22950.
Verma E, Kumar A, Devi Daimary U, Parama D, Girisa S, Sethi G, Kunnumakkara AB. Potential of baicalein in the prevention and treatment of cancer: a scientometric analyses based review. J Funct Foods. 2021;86:104660. https://doi.org/10.1016/j.jff.2021.104660.
Girisa S, Shabnam B, Monisha J, Fan L, Halim CE, Arfuso F, Ahn KS, Sethi G, Kunnumakkara AB. Potential of zerumbone as an anti-cancer agent. Molecules. 2019. https://doi.org/10.3390/molecules24040734.
Cassidy J, Tabernero J, Twelves C, Brunet R, Butts C, Conroy T, Debraud F, Figer A, Grossmann J, Sawada N. XELOX (capecitabine plus oxaliplatin): active first-line therapy for patients with metastatic colorectal cancer. J Clin Oncol. 2004;22:2084–91.
Colucci G, Gebbia V, Paoletti G, Giuliani F, Caruso M, Gebbia N, Cartenì G, Agostara B, Pezzella G, Manzione L. Phase III randomized trial of FOLFIRI versus FOLFOX4 in the treatment of advanced colorectal cancer: a multicenter study of the Gruppo Oncologico Dell’Italia Meridionale. J Clin Oncol. 2005;23:4866–75.
Goldberg RM, Sargent DJ, Morton RF, Fuchs CS, Ramanathan RK, Williamson SK, Findlay BP, Pitot HC, Alberts SR. A randomized controlled trial of fluorouracil plus leucovorin, irinotecan, and oxaliplatin combinations in patients with previously untreated metastatic colorectal cancer. J Clin Oncol. 2004;22:23–30.
Nurgali K, Jagoe RT, Abalo R. Editorial: adverse effects of cancer chemotherapy: anything new to improve tolerance and reduce sequelae? Front Pharmacol. 2018;9:245. https://doi.org/10.3389/fphar.2018.00245.
Monisha J, Roy NK, Padmavathi G, Banik K, Bordoloi D, Khwairakpam AD, Arfuso F, Chinnathambi A, Alahmadi TA, Alharbi SA, et al. NGAL is downregulated in oral squamous cell carcinoma and leads to increased survival, proliferation, migration and chemoresistance. Cancers (Basel). 2018. https://doi.org/10.3390/cancers10070228.
Kunnumakkara AB, Bordoloi D, Sailo BL, Roy NK, Thakur KK, Banik K, Shakibaei M, Gupta SC, Aggarwal BB. Cancer drug development: The missing links. Exp Biol Med. 2019;244:663–89.
Xie YH, Chen YX, Fang JY. Comprehensive review of targeted therapy for colorectal cancer. Signal Transduct Target Ther. 2020;5:22. https://doi.org/10.1038/s41392-020-0116-z.
Quinn BJ, Dallos M, Kitagawa H, Kunnumakkara AB, Memmott RM, Hollander MC, Gills JJ, Dennis PA. Inhibition of lung tumorigenesis by metformin is associated with decreased plasma IGF-I and diminished receptor tyrosine kinase signaling. Cancer Prev Res (Phila). 2013;6:801–10. https://doi.org/10.1158/1940-6207.CAPR-13-0058-T.
Buhrmann C, Kunnumakkara AB, Kumar A, Samec M, Kubatka P, Aggarwal BB, Shakibaei M. Multitargeting effects of calebin A on malignancy of CRC cells in multicellular tumor microenvironment. Front Oncol. 2021;11: 650603. https://doi.org/10.3389/fonc.2021.650603.
Gangwar SK, Kumar A, Jose S, Alqahtani MS, Abbas M, Sethi G, Kunnumakkara AB. Nuclear receptors in oral cancer-Emerging players in tumorigenesis. Cancer Lett. 2022;536: 215666. https://doi.org/10.1016/j.canlet.2022.215666.
Frigo DE, Bondesson M, Williams C. Nuclear receptors: from molecular mechanisms to therapeutics. Essays Biochem. 2021;65:847–56. https://doi.org/10.1042/EBC20210020.
Huggins C, Hodges CV. Studies on prostatic cancer: I. The effect of castration, of estrogen and of androgen injection on serum phosphatases in metastatic carcinoma of the prostate. CA Cancer J Clin. 1972;22:232–40.
Bluemn E, Nelson PS. The androgen/androgen receptor axis in prostate cancer. Curr Opin Oncol. 2012;24:251.
Long MD, Campbell MJ. Pan-cancer analyses of the nuclear receptor superfamily. Nucl Receptor Res. 2015. https://doi.org/10.11131/2015/101182.
Thomas C, Gustafsson J-Å. Estrogen receptor mutations and functional consequences for breast cancer. Trends Endocrinol Metab. 2015;26:467–76.
Zhang Y, Hagedorn CH, Wang L. Role of nuclear receptor SHP in metabolism and cancer. Biochim Biophys Acta. 2011;1812:893–908.
Gangwar SK, Kumar A, Yap KC, Jose S, Parama D, Sethi G, Kumar AP, Kunnumakkara AB. Targeting nuclear receptors in lung cancer-novel therapeutic prospects. Pharmaceuticals. 2022. https://doi.org/10.3390/ph15050624.
Girisa S, Henamayee S, Parama D, Rana V, Dutta U, Kunnumakkara AB. Targeting farnesoid X receptor (FXR) for developing novel therapeutics against cancer. Mol Biomed. 2021;2:21. https://doi.org/10.1186/s43556-021-00035-2.
Girisa S, Rana V, Parama D, Dutta U, Kunnumakkara AB. Differential roles of farnesoid X receptor (FXR) in modulating apoptosis in cancer cells. Adv Protein Chem Struct Biol. 2021;126:63–90.
Yen PM. Classical nuclear hormone receptor activity as a mediator of complex biological responses: a look at health and disease. Best Pract Res Clin Endocrinol Metab. 2015;29:517–28. https://doi.org/10.1016/j.beem.2015.07.005.
Lin JH, Giovannucci E. Sex hormones and colorectal cancer: what have we learned so far? J Natl Cancer Inst. 2010;102:1746–7.
Alberg AJ, Gordon GB, Hoffman SC, Comstock GW, Helzlsouer KJ. Serum dehydroepiandrosterone and dehydroepiandrosterone sulfate and the subsequent risk of developing colon cancer. Cancer Epidemiol Biomark Prev. 2000;9:517–21.
Chlebowski RT, Wactawski-Wende J, Ritenbaugh C, Hubbell FA, Ascensao J, Rodabough RJ, Rosenberg CA, Taylor VM, Harris R, Chen C. Estrogen plus progestin and colorectal cancer in postmenopausal women. N Engl J Med. 2004;350:991–1004.
Slattery ML, Sweeney C, Murtaugh M, Ma KN, Wolff RK, Potter JD, Caan BJ, Samowitz W. Associations between ERα, ERβ, and AR genotypes and colon and rectal cancer. Cancer Epidemiol Biomark Prev. 2005;14:2936–42.
Anagnostopoulou V, Pediaditakis I, Alkahtani S, Alarifi SA, Schmidt EM, Lang F, Gravanis A, Charalampopoulos I, Stournaras C. Differential effects of dehydroepiandrosterone and testosterone in prostate and colon cancer cell apoptosis: the role of nerve growth factor (NGF) receptors. Endocrinology. 2013;154:2446–56. https://doi.org/10.1210/en.2012-2249.
Amos-Landgraf JM, Heijmans J, Wielenga MC, Dunkin E, Krentz KJ, Clipson L, Ederveen AG, Groothuis PG, Mosselman S, Muncan V. Sex disparity in colonic adenomagenesis involves promotion by male hormones, not protection by female hormones. Proc Natl Acad Sci. 2014;111:16514–9.
Flanagan JJ, Neklesa TK. Targeting Nuclear Receptors with PROTAC degraders. Mol Cell Endocrinol. 2019;493: 110452. https://doi.org/10.1016/j.mce.2019.110452.
Cathcart P, Lucchesi W, Ottaviani S, De Giorgio A, Krell J, Stebbing J, Castellano L. Noncoding RNAs and the control of signalling via nuclear receptor regulation in health and disease. Best Pract Res Clin Endocrinol Metab. 2015;29:529–43. https://doi.org/10.1016/j.beem.2015.07.003.
Kojetin DJ, Burris TP. REV-ERB and ROR nuclear receptors as drug targets. Nat Rev Drug Discov. 2014;13:197–216. https://doi.org/10.1038/nrd4100.
Yang Z, Gimple RC, Zhou N, Zhao L, Gustafsson JA, Zhou S. Targeting Nuclear Receptors for Cancer Therapy: Premises, Promises, and Challenges. Trends Cancer. 2021;7:541–56. https://doi.org/10.1016/j.trecan.2020.11.007.
Zhao L, Hu H, Gustafsson JA, Zhou S. Nuclear Receptors in Cancer Inflammation and Immunity. Trends Immunol. 2020;41:172–85. https://doi.org/10.1016/j.it.2019.12.006.
Dhiman VK, Bolt MJ, White KP. Nuclear receptors in cancer - uncovering new and evolving roles through genomic analysis. Nat Rev Genet. 2018;19:160–74. https://doi.org/10.1038/nrg.2017.102.
Zhao L, Zhou S, Gustafsson JA. Nuclear Receptors: Recent Drug Discovery for Cancer Therapies. Endocr Rev. 2019;40:1207–49. https://doi.org/10.1210/er.2018-00222.
Mangelsdorf DJ, Thummel C, Beato M, Herrlich P, Schütz G, Umesono K, Blumberg B, Kastner P, Mark M, Chambon P. The nuclear receptor superfamily: the second decade. Cell. 1995;83:835.
Kipps TJ. ROR1: an orphan becomes apparent. Blood. 2022;140:1583–91. https://doi.org/10.1182/blood.2021014760.
Weikum ER, Liu X, Ortlund EA. The nuclear receptor superfamily: a structural perspective. Protein Sci. 2018;27:1876–92.
Jayaprakash S, Hegde M, Girisa S, Alqahtani MS, Abbas M, Lee EHC, Yap KC-H, Sethi G, Kumar AP, Kunnumakkara AB. Demystifying the functional role of nuclear receptors in esophageal cancer. Int J Mol Sci. 2022;23:10952.
Fuller PJ. The steroid receptor superfamily: mechanisms of diversity. FASEB J. 1991;5:3092–9.
O’Malley BW, Tsai M-J. Molecular pathways of steroid receptor action. Biol Reprod. 1992;46:163–7.
De Bosscher K, Desmet SJ, Clarisse D, Estébanez-Perpiña E, Brunsveld L. Nuclear receptor crosstalk—defining the mechanisms for therapeutic innovation. Nat Rev Endocrinol. 2020;16:363–77.
Degirolamo C, Modica S, Palasciano G, Moschetta A. Bile acids and colon cancer: Solving the puzzle with nuclear receptors. Trends Mol Med. 2011;17:564–72. https://doi.org/10.1016/j.molmed.2011.05.010.
Mulholland DJ, Dedhar S, Coetzee GA, Nelson CC. Interaction of nuclear receptors with the Wnt/beta-catenin/Tcf signaling axis: Wnt you like to know? Endocr Rev. 2005;26:898–915. https://doi.org/10.1210/er.2003-0034.
Hu J, Wang C, Huang X, Yi S, Pan S, Zhang Y, Yuan G, Cao Q, Ye X, Li H. Gut microbiota-mediated secondary bile acids regulate dendritic cells to attenuate autoimmune uveitis through TGR5 signaling. Cell Rep. 2021;36: 109726. https://doi.org/10.1016/j.celrep.2021.109726.
Gonzalez FJ, Jiang C, Patterson AD. An Intestinal Microbiota-Farnesoid X Receptor Axis Modulates Metabolic Disease. Gastroenterology. 2016;151:845–59. https://doi.org/10.1053/j.gastro.2016.08.057.
Ibrahim A, Hugerth LW, Hases L, Saxena A, Seifert M, Thomas Q, Gustafsson JA, Engstrand L, Williams C. Colitis-induced colorectal cancer and intestinal epithelial estrogen receptor beta impact gut microbiota diversity. Int J Cancer. 2019;144:3086–98. https://doi.org/10.1002/ijc.32037.
Catalano MG, Pfeffer U, Raineri M, Ferro P, Curto A, Capuzzi P, Corno F, Berta L, Fortunati N. Altered expression of androgen-receptor isoforms in human colon-cancer tissues. Int J Cancer. 2000;86:325–30. https://doi.org/10.1002/(sici)1097-0215(20000501)86:3%3c325::aid-ijc4%3e3.0.co;2-g.
Albasri AM, Elkablawy MA. Clinicopathological and prognostic significance of androgen receptor overexpression in colorectal cancer. Experience from Al-Madinah Al-Munawarah. Saudi Arabia Saudi Med J. 2019;40:893–900. https://doi.org/10.15537/smj.2019.9.24204.
Castagnetta L, Traina A, Campisi I, Calabro M, Maratta A, Saetta A, Agostara B, Mezzatesta N. Androgen receptor status in nontumoral and malignant human colorectal tissues. Ann N Y Acad Sci. 2002;963:322–5. https://doi.org/10.1111/j.1749-6632.2002.tb04124.x.
Stebbings WS, Farthing MJ, Vinson GP, Northover JM, Wood RF. Androgen receptors in rectal and colonic cancer. Dis Colon Rectum. 1986;29:95–8. https://doi.org/10.1007/BF02555385.
Li XB, Jiao S, Sun H, Xue J, Zhao WT, Fan L, Wu GH, Fang J. The orphan nuclear receptor EAR2 is overexpressed in colorectal cancer and it regulates survivability of colon cancer cells. Cancer Lett. 2011;309:137–44. https://doi.org/10.1016/j.canlet.2011.05.025.
Zhou ZW, Wan DS, Wang GQ, Pan ZZ, Lu HP, Gao JH, Ding PR. Expression of estrogen receptor and progesterone receptor in colorectal cancer: a quantitative study. Ai Zheng. 2004;23:851–4.
Nüssler NC, Reinbacher K, Shanny N, Schirmeier A, Glanemann M, Neuhaus P, Nussler AK, Kirschner M. Sex-specific differences in the expression levels of estrogen receptor subtypes in colorectal cancer. Gend Med. 2008;5:209–17.
Jiang HP, Teng RY, Wang Q, Zhang X, Wang HH, Cao J, Teng LS. Estrogen receptor alpha variant ERalpha46 mediates growth inhibition and apoptosis of human HT-29 colon adenocarcinoma cells in the presence of 17beta-oestradiol. Chin Med J (Engl). 2008;121:1025–31.
Jiang L, Fei H, Yang A, Zhu J, Sun J, Liu X, Xu W, Yang J, Zhang S. Estrogen inhibits the growth of colon cancer in mice through reversing extracellular vesicle-mediated immunosuppressive tumor microenvironment. Cancer Lett. 2021;520:332–43.
Pereira MA, Tao L, Wang W, Li Y, Umar A, Steele VE, Lubet RA. Modulation by celecoxib and difluoromethylornithine of the methylation of DNA and the estrogen receptor-α gene in rat colon tumors. Carcinogenesis. 2004;25:1917–23.
Armstrong CM, Billimek AR, Allred KF, Sturino JM, Weeks BR, Allred CD. A novel shift in estrogen receptor expression occurs as estradiol suppresses inflammation-associated colon tumor formation. Endocr Relat Cancer. 2013;20:515–25.
Topi G, Ghatak S, Satapathy SR, Ehrnström R, Lydrup M-L, Sjölander A. Combined estrogen alpha and beta receptor expression has a prognostic significance for colorectal cancer patients. Front Med. 2022;9:739620.
Castiglione F, Taddei A, Degl’Innocenti DR, Buccoliero AM, Bechi P, Garbini F, Chiara FG, Moncini D, Cavallina G, Marascio L. Expression of estrogen receptor β in colon cancer progression. Diagn Mol Pathol. 2008;17:231–6.
Edvardsson K, Nguyen-Vu T, Kalasekar SM, Pontén F, Gustafsson J-Å, Williams C. Estrogen receptor β expression induces changes in the microRNA pool in human colon cancer cells. Carcinogenesis. 2013;34:1431–41.
Peng J, Ou Q, Wu X, Zhang R, Zhao Q, Jiang W, Lu Z, Wan D, Pan Z, Fang Y. Expression of voltage-gated sodium channel Nav1.5 in non-metastatic colon cancer and its associations with estrogen receptor (ER)-beta expression and clinical outcomes. Chin J Cancer. 2017. https://doi.org/10.1186/s40880-017-0253-0.
Hartman J, Edvardsson K, Lindberg K, Zhao C, Williams C, Ström A, Gustafsson J-A. Tumor repressive functions of estrogen receptor β in SW480 colon cancer cells. Can Res. 2009;69:6100–6.
López-Calderero I, Carnero A, Astudillo A, Palacios J, Chaves M, Benavent M, Limón ML, Garcia-Carbonero R. Prognostic relevance of estrogen receptor-α Ser167 phosphorylation in stage II-III colon cancer patients. Hum Pathol. 2014;45:2437–46.
Motylewska E, Stasikowska O, Mełeń-Mucha G. The inhibitory effect of diarylpropionitrile, a selective agonist of estrogen receptor beta, on the growth of MC38 colon cancer line. Cancer Lett. 2009;276:68–73.
Ya G, Wang H, Ma Y, Hu A, Ma Y, Hu J, Yu Y. Serum miR-129 functions as a biomarker for colorectal cancer by targeting estrogen receptor (ER) β. Die Pharmazie Intl J Pharm Sci. 2017;72:107–12.
Mostafaie N, Kállay E, Sauerzapf E, Bonner E, Kriwanek S, Cross HS, Huber KR, Krugluger W. Correlated downregulation of estrogen receptor beta and the circadian clock gene Per1 in human colorectal cancer. Mol Carcinog. 2009;48:642–7.
Topi G, Ehrnström R, Jirström K, Palmquist I, Lydrup M-L, Sjölander A. Association of the oestrogen receptor beta with hormone status and prognosis in a cohort of female patients with colorectal cancer. Eur J Cancer. 2017;83:279–89.
Konstantinopoulos P, Kominea A, Vandoros G, Sykiotis G, Andricopoulos P, Varakis I, Sotiropoulou-Bonikou G, Papavassiliou A. Oestrogen receptor beta (ERβ) is abundantly expressed in normal colonic mucosa, but declines in colon adenocarcinoma paralleling the tumour’s dedifferentiation. Eur J Cancer. 2003;39:1251–8.
Hases L, Indukuri R, Birgersson M, Nguyen-Vu T, Lozano R, Saxena A, Hartman J, Frasor J, Gustafsson J-Å, Katajisto P. Intestinal estrogen receptor beta suppresses colon inflammation and tumorigenesis in both sexes. Cancer Lett. 2020;492:54–62.
Janakiram NB, Mohammed A, Zhang Y, Brewer M, Bryant T, Lightfoot S, Steele VE, Rao CV. Chemopreventive efficacy of raloxifene, bexarotene, and their combination on the progression of chemically induced colon adenomas to adenocarcinomas in rats. Cancer Prev Res. 2013;6:1251–61.
Nguyen-Vu T, Wang J, Mesmar F, Mukhopadhyay S, Saxena A, McCollum CW, Gustafsson JA, Bondesson M, Williams C. Estrogen receptor beta reduces colon cancer metastasis through a novel miR-205—PROX1 mechanism. Oncotarget. 2016;7:42159–71. https://doi.org/10.18632/oncotarget.9895.
Boudjadi S, Bernatchez G, Beaulieu JF, Carrier JC. Control of the human osteopontin promoter by ERRalpha in colorectal cancer. Am J Pathol. 2013;183:266–76. https://doi.org/10.1016/j.ajpath.2013.03.021.
Zhou S, Xia H, Xu H, Tang Q, Nie Y, Gong QY, Bi F. ERRalpha suppression enhances the cytotoxicity of the MEK inhibitor trametinib against colon cancer cells. J Exp Clin Cancer Res. 2018;37:218. https://doi.org/10.1186/s13046-018-0862-8.
De Vitto H, Ryu J, Calderon-Aparicio A, Monts J, Dey R, Chakraborty A, Lee MH, Bode AM, Dong Z. Estrogen-related receptor alpha directly binds to p53 and cooperatively controls colon cancer growth through the regulation of mitochondrial biogenesis and function. Cancer Metab. 2020;8:28. https://doi.org/10.1186/s40170-020-00234-5.
Abou Gabal H, Ahmed N, Meckawy G, Yassin R, Hakim S. Evaluation of EZH2 and ERRalpha in colorectal carcinoma: an immunohistochemical study. Pol J Pathol. 2021;72:200–10. https://doi.org/10.5114/pjp.2021.111770.
Lax S, Schauer G, Prein K, Kapitan M, Silbert D, Berghold A, Berger A, Trauner M. Expression of the nuclear bile acid receptor/farnesoid X receptor is reduced in human colon carcinoma compared to nonneoplastic mucosa independent from site and may be associated with adverse prognosis. Int J Cancer. 2012;130:2232–9.
De Gottardi A, Touri F, Maurer CA, Perez A, Maurhofer O, Ventre G, Bentzen CL, Bentzen EJ, Dufour J-F. The bile acid nuclear receptor FXR and the bile acid binding protein IBABP are differently expressed in colon cancer. Dig Dis Sci. 2004;49:982–9.
Yao HS, Wang J, Zhang XP, Wang LZ, Wang Y, Li XX, Jin KZ, Hu ZQ, Wang WJ. Hepatocyte nuclear factor 4alpha suppresses the aggravation of colon carcinoma. Mol Carcinog. 2016;55:458–72. https://doi.org/10.1002/mc.22294.
Wu C, Feng J, Li L, Wu Y, Xie H, Yin Y, Ye J, Li Z. Liver receptor homologue 1, a novel prognostic marker in colon cancer patients. Oncol Lett. 2018;16:2833–8. https://doi.org/10.3892/ol.2018.8988.
Yan L, Qiu J, Yao J. Downregulation of microRNA-30d promotes cell proliferation and invasion by targeting LRH-1 in colorectal carcinoma. Int J Mol Med. 2017;39:1371–80. https://doi.org/10.3892/ijmm.2017.2958.
Qu R, Hao S, Jin X, Shi G, Yu Q, Tong X, Guo D. MicroRNA-374b reduces the proliferation and invasion of colon cancer cells by regulation of LRH-1/Wnt signaling. Gene. 2018;642:354–61. https://doi.org/10.1016/j.gene.2017.11.019.
Lo Sasso G, Bovenga F, Murzilli S, Salvatore L, Di Tullio G, Martelli N, D’Orazio A, Rainaldi S, Vacca M, Mangia A, et al. Liver X receptors inhibit proliferation of human colorectal cancer cells and growth of intestinal tumors in mice. Gastroenterology. 2013. https://doi.org/10.1053/j.gastro.2013.02.005.
Cho SD, Yoon K, Chintharlapalli S, Abdelrahim M, Lei P, Hamilton S, Khan S, Ramaiah SK, Safe S. Nur77 agonists induce proapoptotic genes and responses in colon cancer cells through nuclear receptor-dependent and nuclear receptor-independent pathways. Cancer Res. 2007;67:674–83. https://doi.org/10.1158/0008-5472.CAN-06-2907.
Wu H, Lin Y, Li W, Sun Z, Gao W, Zhang H, Xie L, Jiang F, Qin B, Yan T, et al. Regulation of Nur77 expression by beta-catenin and its mitogenic effect in colon cancer cells. FASEB J. 2011;25:192–205. https://doi.org/10.1096/fj.10-166462.
Marin HE, Peraza MA, Billin AN, Willson TM, Ward JM, Kennett MJ, Gonzalez FJ, Peters JM. Ligand activation of peroxisome proliferator-activated receptor beta inhibits colon carcinogenesis. Cancer Res. 2006;66:4394–401. https://doi.org/10.1158/0008-5472.Can-05-4277.
Luo Y, Xie C, Brocker CN, Fan J, Wu X, Feng L, Wang Q, Zhao J, Lu D, Tandon M, et al. Intestinal PPARalpha protects against colon carcinogenesis via regulation of methyltransferases DNMT1 and PRMT6. Gastroenterology. 2019;157(744–759): e744. https://doi.org/10.1053/j.gastro.2019.05.057.
Martinasso G, Oraldi M, Trombetta A, Maggiora M, Bertetto O, Canuto RA, Muzio G. Involvement of PPARs in cell proliferation and apoptosis in human colon cancer specimens and in normal and cancer cell lines. PPAR Res. 2007;2007:93416. https://doi.org/10.1155/2007/93416.
Ouyang N, Williams JL, Rigas B. NO-donating aspirin isomers downregulate peroxisome proliferator-activated receptor (PPAR) δ expression in APC min/+ mice proportionally to their tumor inhibitory effect: implications for the role of PPARδ in carcinogenesis. Carcinogenesis. 2006;27:232–9.
Gupta RA, Tan J, Krause WF, Geraci MW, Willson TM, Dey SK, DuBois RN. Prostacyclin-mediated activation of peroxisome proliferator-activated receptor delta in colorectal cancer. Proc Natl Acad Sci U S A. 2000;97:13275–80. https://doi.org/10.1073/pnas.97.24.13275.
Zuo X, Xu M, Yu J, Wu Y, Moussalli MJ, Manyam GC, Lee SI, Liang S, Gagea M, Morris JS. Potentiation of colon cancer susceptibility in mice by colonic epithelial PPAR-δ/β overexpression. J Natl Cancer Inst. 2014;106:052.
Konstantinopoulos PA, Vandoros GP, Sotiropoulou-Bonikou G, Kominea A, Papavassiliou AG. NF-kappaB/PPAR gamma and/or AP-1/PPAR gamma “on/off” switches and induction of CBP in colon adenocarcinomas: correlation with COX-2 expression. Int J Colorectal Dis. 2007;22:57–68. https://doi.org/10.1007/s00384-006-0112-y.
Qiao L, Dai Y, Gu Q, Chan KW, Ma J, Lan HY, Zou B, Rocken C, Ebert MP, Wong BC. Loss of XIAP sensitizes colon cancer cells to PPARgamma independent antitumor effects of troglitazone and 15-PGJ2. Cancer Lett. 2008;268:260–71. https://doi.org/10.1016/j.canlet.2008.04.003.
DuBois RN, Gupta R, Brockman J, Reddy BS, Krakow SL, Lazar MA. The nuclear eicosanoid receptor, PPARgamma, is aberrantly expressed in colonic cancers. Carcinogenesis. 1998;19:49–53. https://doi.org/10.1093/carcin/19.1.49.
Tan BS, Kang O, Mai CW, Tiong KH, Khoo AS, Pichika MR, Bradshaw TD, Leong CO. 6-Shogaol inhibits breast and colon cancer cell proliferation through activation of peroxisomal proliferator activated receptor gamma (PPARgamma). Cancer Lett. 2013;336:127–39. https://doi.org/10.1016/j.canlet.2013.04.014.
Ouyang N, Ke S, Eagleton N, Xie Y, Chen G, Laffins B, Yao H, Zhou B, Tian Y. Pregnane X receptor suppresses proliferation and tumourigenicity of colon cancer cells. Br J Cancer. 2010;102:1753–61.
Raynal C, Pascussi J-M, Leguelinel G, Breuker C, Kantar J, Lallemant B, Poujol S, Bonnans C, Joubert D, Hollande F. Pregnane× Receptor (PXR) expression in colorectal cancer cells restricts irinotecan chemosensitivity through enhanced SN-38 glucuronidation. Mol Cancer. 2010;9:1–13.
Jiang H, Chen K, He J, Pan F, Li J, Chen J, Chen W, Liang H. Association of pregnane X receptor with multidrug resistance-related protein 3 and its role in human colon cancer chemoresistance. J Gastrointest Surg. 2009;13:1831–8.
Singh S, Sheppard MC, Langman MJ. Sex differences in the incidence of colorectal cancer: an exploration of oestrogen and progesterone receptors. Gut. 1993;34:611–5. https://doi.org/10.1136/gut.34.5.611.
Zhang YL, Wen XD, Guo X, Huang SQ, Wang TT, Zhou PT, Li W, Zhou LF, Hu YH. Progesterone suppresses the progression of colonic carcinoma by increasing the activity of the GADD45alpha/JNK/cJun signalling pathway. Oncol Rep. 2021. https://doi.org/10.3892/or.2021.8046.
Yamazaki K, Shimizu M, Okuno M, Matsushima-Nishiwaki R, Kanemura N, Araki H, Tsurumi H, Kojima S, Weinstein IB, Moriwaki H. Synergistic effects of RXRα and PPARγ ligands to inhibit growth in human colon cancer cells—phosphorylated RXRα is a critical target for colon cancer management. Gut. 2007;56:1557–63.
Modarai SR, Gupta A, Opdenaker LM, Kowash R, Masters G, Viswanathan V, Zhang T, Fields JZ, Boman BM. The anti-cancer effect of retinoic acid signaling in CRC occurs via decreased growth of ALDH+ colon cancer stem cells and increased differentiation of stem cells. Oncotarget. 2018;9:34658.
Janakiram NB, Cooma I, Mohammed A, Steele VE, Rao CV. Beta-ionone inhibits colonic aberrant crypt foci formation in rats, suppresses cell growth, and induces retinoid X receptor-alpha in human colon cancer cells. Mol Cancer Ther. 2008;7:181–90. https://doi.org/10.1158/1535-7163.MCT-07-0529.
Morris J, Moseley VR, Cabang AB, Coleman K, Wei W, Garrett-Mayer E, Wargovich MJ. Reduction in promotor methylation utilizing EGCG (epigallocatechin-3-gallate) restores RXRalpha expression in human colon cancer cells. Oncotarget. 2016;7:35313–26. https://doi.org/10.18632/oncotarget.9204.
Uchuya-Castillo J, Aznar N, Frau C, Martinez P, Le Nevé C, Marisa L, Penalva LO, Laurent-Puig P, Puisieux A, Scoazec J-Y. Increased expression of the thyroid hormone nuclear receptor TRα1 characterizes intestinal tumors with high Wnt activity. Oncotarget. 2018;9:30979.
Horkko TT, Tuppurainen K, George SM, Jernvall P, Karttunen TJ, Makinen MJ. Thyroid hormone receptor beta1 in normal colon and colorectal cancer-association with differentiation, polypoid growth type and K-ras mutations. Int J Cancer. 2006;118:1653–9. https://doi.org/10.1002/ijc.21556.
Giardina C, Nakanishi M, Khan A, Kuratnik A, Xu W, Brenner B, Rosenberg DW. Regulation of VDR expression in Apc-mutant mice, human colon cancers and adenomas. Cancer Prev Res (Phila). 2015;8:387–99. https://doi.org/10.1158/1940-6207.CAPR-14-0371.
Zhang YG, Lu R, Wu S, Chatterjee I, Zhou D, Xia Y, Sun J. Vitamin D receptor protects against dysbiosis and tumorigenesis via the JAK/STAT pathway in intestine. Cell Mol Gastroenterol Hepatol. 2020;10:729–46. https://doi.org/10.1016/j.jcmgh.2020.05.010.
Knackstedt RW, Moseley VR, Sun S, Wargovich MJ. Vitamin D receptor and retinoid X receptor alpha status and vitamin D insufficiency in models of murine colitis. Cancer Prev Res (Phila). 2013;6:585–93. https://doi.org/10.1158/1940-6207.CAPR-12-0488.
Long MD, Campbell MJ. Integrative genomic approaches to dissect clinically-significant relationships between the VDR cistrome and gene expression in primary colon cancer. J Steroid Biochem Mol Biol. 2017;173:130–8.
Pena C, Garcia J, Larriba M, Barderas R, Gomez I, Herrera M, García V, Silva J, Domínguez G, Rodríguez R. SNAI1 expression in colon cancer related with CDH1 and VDR downregulation in normal adjacent tissue. Oncogene. 2009;28:4375–85.
Wada K, Tanaka H, Maeda K, Inoue T, Noda E, Amano R, Kubo N, Muguruma K, Yamada N, Yashiro M. Vitamin D receptor expression is associated with colon cancer in ulcerative colitis. Oncol Rep. 2009;22:1021–5.
Murillo G, Matusiak D, Benya RV, Mehta RG. Chemopreventive efficacy of 25-hydroxyvitamin D3 in colon cancer. J Steroid Biochem Mol Biol. 2007;103:763–7.
Larriba MJ, Martín-Villar E, García JM, Pereira F, Pena C, de Garcia Herreros A, Bonilla F, Munoz A. Snail2 cooperates with Snail1 in the repression of vitamin D receptor in colon cancer. Carcinogenesis. 2009;30:1459–68.
Anderson MG, Nakane M, Ruan X, Kroeger PE, Wu-Wong JR. Expression of VDR and CYP24A1 mRNA in human tumors. Cancer Chemother Pharmacol. 2006;57:234–40.
Prasanna R, Elbessoumy AA, Chandramoorthy HC, Dera A, Al Fayi M. FCX, an arylidene derivative, induces apoptosis in androgen receptor-selective prostate cancer cells. J Cancer Res Ther. 2021;17:401–7. https://doi.org/10.4103/jcrt.JCRT_228_17.
Consiglio CR, Udartseva O, Ramsey KD, Bush C, Gollnick SO. Enzalutamide, an androgen receptor antagonist, enhances myeloid cell-mediated immune suppression and tumor progression. Cancer Immunol Res. 2020;8:1215–27. https://doi.org/10.1158/2326-6066.CIR-19-0371.
Mulholland DJ, Read JT, Rennie PS, Cox ME, Nelson CC. Functional localization and competition between the androgen receptor and T-cell factor for nuclear beta-catenin: a means for inhibition of the Tcf signaling axis. Oncogene. 2003;22:5602–13. https://doi.org/10.1038/sj.onc.1206802.
Liva SG, Tseng YC, Dauki AM, Sovic MG, Vu T, Henderson SE, Kuo YC, Benedict JA, Zhang X, Remaily BC, et al. Overcoming resistance to anabolic SARM therapy in experimental cancer cachexia with an HDAC inhibitor. EMBO Mol Med. 2020;12:e9910. https://doi.org/10.15252/emmm.201809910.
Picariello L, Fiorelli G, Martineti V, Tognarini I, Pampaloni B, Tonelli F, Brandi ML. Growth response of colon cancer cell lines to selective estrogen receptor modulators. Anticancer Res. 2003;23:2419–24.
Yang L, Allred KF, Dykes L, Allred CD, Awika JM. Enhanced action of apigenin and naringenin combination on estrogen receptor activation in non-malignant colonocytes: implications on sorghum-derived phytoestrogens. Food Funct. 2015;6:749–55.
Fiorelli G, Picariello L, Martineti V, Tonelli F, Brandi ML. Functional estrogen receptor β in colon cancer cells. Biochem Biophys Res Commun. 1999;261:521–7.
Janakiram NB, Steele VE, Rao CV. Estrogen receptor-β as a potential target for colon cancer prevention: chemoprevention of azoxymethane-induced colon carcinogenesis by raloxifene in F344 rats. Cancer Prev Res. 2009;2:52–9.
Topi G, Satapathy SR, Dash P, Fred Mehrabi S, Ehrnström R, Olsson R, Lydrup ML, Sjölander A. Tumour-suppressive effect of oestrogen receptor β in colorectal cancer patients, colon cancer cells, and a zebrafish model. J Pathol. 2020;251:297–309.
Hsu H-H, Cheng S-F, Chen L-M, Liu J-Y, Chu C-H, Weng Y-J, Li Z-Y, Lin C-S, Lee S-D, Kuo W-W. Over-expressed estrogen receptor-α up-regulates hTNF-α gene expression and down-regulates β-catenin signaling activity to induce the apoptosis and inhibit proliferation of LoVo colon cancer cells. Mol Cell Biochem. 2006;289:101–9.
Jin P, Wang D-z, Lyu C-x, Wang Y-t, He Y-q, Sheng J-q, Li X. Mismatch repair protein hMLH1, but not hMSH2, enhances estrogen-induced apoptosis of colon cancer cells. J Cancer. 2017;8:3232.
Wei Y, Huang C, Wu H, Huang J. Estrogen receptor beta (ERβ) mediated-CyclinD1 degradation via autophagy plays an anti-proliferation role in colon cells. Int J Biol Sci. 2019;15:942–52.
Nakayama Y, Sakamoto H, Satoh K, Yamamoto T. Tamoxifen and gonadal steroids inhibit colon cancer growth in association with inhibition of thymidylate synthase, survivin and telomerase expression through estrogen receptor beta mediated system. Cancer Lett. 2000;161:63–71.
Bustos V, Nolan ÁM, Nijhuis A, Harvey H, Parker A, Poulsom R, McBryan J, Thomas W, Silver A, Harvey BJ. GPER mediates differential effects of estrogen on colon cancer cell proliferation and migration under normoxic and hypoxic conditions. Oncotarget. 2017;8:84258.
Raju J, Bielecki A, Caldwell D, Lok E, Taylor M, Kapal K, Curran I, Cooke GM, Bird RP, Mehta R. Soy isoflavones modulate azoxymethane-induced rat colon carcinogenesis exposed pre-and postnatally and inhibit growth of DLD-1 human colon adenocarcinoma cells by increasing the expression of estrogen receptor-β. J Nutr. 2009;139:474–81.
Giroux V, Lemay F, Bernatchez G, Robitaille Y, Carrier JC. Estrogen receptor β deficiency enhances small intestinal tumorigenesis in ApcMin/+ mice. Int J Cancer. 2008;123:303–11.
He Y-q, Sheng J-q, Ling X-l, Fu L, Jin P, Yen L, Rao J. Estradiol regulates miR-135b and mismatch repair gene expressions via estrogen receptor-β in colorectal cells. Exp Mol Med. 2012;44:723–32.
Fang Y-J, Pan Z-Z, Li L-R, Lu Z-H, Zhang L-Y, Wan D-S. MMP7 expression regulated by endocrine therapy in ERβ-positive colon cancer cells. J Exp Clin Cancer Res. 2009;28:1–8.
Caiazza F, Galluzzo P, Lorenzetti S, Marino M. 17β-estradiol induces ERβ up-regulation via p38/MAPK activation in colon cancer cells. Biochem Biophys Res Commun. 2007;359:102–7.
Qiu Y, Waters C, Lewis A, Langman M, Eggo M. Oestrogen-induced apoptosis in colonocytes expressing oestrogen receptor beta. J Endocrinol. 2002;174:369–77.
Fiocchetti M, Camilli G, Acconcia F, Leone S, Ascenzi P, Marino M. ERβ-dependent neuroglobin up-regulation impairs 17β-estradiol-induced apoptosis in DLD-1 colon cancer cells upon oxidative stress injury. J Steroid Biochem Mol Biol. 2015;149:128–37.
Sasso CV, Santiano FE, Arboccó FCV, Zyla LE, Semino SN, Guerrero-Gimenez ME, Creydt VP, Fontana CML, Carón RW. Estradiol and progesterone regulate proliferation and apoptosis in colon cancer. Endocr Connect. 2019;8:217–29.
Bulzomi P, Galluzzo P, Bolli A, Leone S, Acconcia F, Marino M. The pro-apoptotic effect of quercetin in cancer cell lines requires ERbeta-dependent signals. J Cell Physiol. 2012;227:1891–8. https://doi.org/10.1002/jcp.22917.
Sanaei M, Kavoosi F. Effect of 5-aza-2′-deoxycytidine on estrogen receptor alpha/beta and DNA methyltransferase 1 genes expression, apoptosis induction, and cell growth prevention of the colon cancer HT 29 cell line. Int J Prev Med. 2020;11:147. https://doi.org/10.4103/ijpvm.IJPVM_140_19.
Edvardsson K, Strom A, Jonsson P, Gustafsson JA, Williams C. Estrogen receptor beta induces antiinflammatory and antitumorigenic networks in colon cancer cells. Mol Endocrinol. 2011;25:969–79. https://doi.org/10.1210/me.2010-0452.
Bernatchez G, Giroux V, Lassalle T, Carpentier AC, Rivard N, Carrier JC. ERRα metabolic nuclear receptor controls growth of colon cancer cells. Carcinogenesis. 2013;34:2253–61.
Mencarelli A, Distrutti E, Renga B, D’Amore C, Cipriani S, Palladino G, Donini A, Ricci P, Fiorucci S. Probiotics modulate intestinal expression of nuclear receptor and provide counter-regulatory signals to inflammation-driven adipose tissue activation. PLoS ONE. 2011;6:e22978. https://doi.org/10.1371/journal.pone.0022978.
Mao J, Chen X, Wang C, Li W, Li J. Effects and mechanism of the bile acid (farnesoid X) receptor on the Wnt/beta-catenin signaling pathway in colon cancer. Oncol Lett. 2020;20:337–45. https://doi.org/10.3892/ol.2020.11545.
Maran RR, Thomas A, Roth M, Sheng Z, Esterly N, Pinson D, Gao X, Zhang Y, Ganapathy V, Gonzalez FJ. Farnesoid X receptor deficiency in mice leads to increased intestinal epithelial cell proliferation and tumor development. J Pharmacol Exp Ther. 2009;328:469–77.
Peng Z, Raufman J-P, Xie G. Src-mediated cross-talk between farnesoid X and epidermal growth factor receptors inhibits human intestinal cell proliferation and tumorigenesis. PLoS ONE. 2012;7:e48461.
Yang F, Hu Y, Liu H-X, Wan Y-JY. MiR-22-silenced cyclin A expression in colon and liver cancer cells is regulated by bile acid receptor. J Biol Chem. 2015;290:6507–15.
Hotta M, Sakatani T, Ishino K, Wada R, Kudo M, Yokoyama Y, Yamada T, Yoshida H, Naito Z. Farnesoid X receptor induces cell death and sensitizes to TRAIL-induced inhibition of growth in colorectal cancer cells through the up-regulation of death receptor 5. Biochem Biophys Res Commun. 2019;519:824–31.
Selmin OI, Fang C, Lyon AM, Doetschman TC, Thompson PA, Martinez JD, Smith JW, Lance PM, Romagnolo DF. Inactivation of adenomatous polyposis coli reduces bile acid/farnesoid X receptor expression through Fxr gene CpG methylation in mouse colon tumors and human colon cancer cells. J Nutr. 2016;146:236–42.
Qiao P, Li S, Zhang H, Yao L, Wang F. Farnesoid X receptor inhibits proliferation of human colorectal cancer cells via the miR-135A1/CCNG2 signaling pathway. Oncol Rep. 2018;40:2067–78.
Modica S, Murzilli S, Salvatore L, Schmidt DR, Moschetta A. Nuclear bile acid receptor FXR protects against intestinal tumorigenesis. Can Res. 2008;68:9589–94.
Peng Z, Chen J, Drachenberg CB, Raufman J-P, Xie G. Farnesoid X receptor represses matrix metalloproteinase 7 expression, revealing this regulatory axis as a promising therapeutic target in colon cancer. J Biol Chem. 2019;294:8529–42.
Xu T, Wu K, Zhang L, Zheng S, Wang X, Zuo H, Wu X, Tao G, Jiang B, Zhang L. Long non-coding RNA LINC00858 exerts a tumor-promoting role in colon cancer via HNF4alpha and WNK2 regulation. Cell Oncol (Dordr). 2020;43:297–310. https://doi.org/10.1007/s13402-019-00490-8.
Vuong LM, Chellappa K, Dhahbi JM, Deans JR, Fang B, Bolotin E, Titova NV, Hoverter NP, Spindler SR, Waterman ML, et al. Differential effects of hepatocyte nuclear factor 4alpha Isoforms on tumor growth and T-cell factor 4/AP-1 interactions in human colorectal cancer cells. Mol Cell Biol. 2015;35:3471–90. https://doi.org/10.1128/MCB.00030-15.
Algamas-Dimantov A, Yehuda-Shnaidman E, Peri I, Schwartz B. Epigenetic control of HNF-4α in colon carcinoma cells affects MUC4 expression and malignancy. Cell Oncol. 2013;36:155–67.
Lai HT, Chiang CT, Tseng WK, Chao TC, Su Y. GATA6 enhances the stemness of human colon cancer cells by creating a metabolic symbiosis through upregulating LRH-1 expression. Mol Oncol. 2020;14:1327–47. https://doi.org/10.1002/1878-0261.12647.
Bayrer JR, Mukkamala S, Sablin EP, Webb P, Fletterick RJ. Silencing LRH-1 in colon cancer cell lines impairs proliferation and alters gene expression programs. Proc Natl Acad Sci U S A. 2015;112:2467–72. https://doi.org/10.1073/pnas.1500978112.
Yuan Q, Cao G, Li J, Zhang Y, Yang W. MicroRNA-136 inhibits colon cancer cell proliferation and invasion through targeting liver receptor homolog-1/Wnt signaling. Gene. 2017;628:48–55. https://doi.org/10.1016/j.gene.2017.07.031.
Liang Y, Zhao Q, Fan L, Zhang Z, Tan B, Liu Y, Li Y. Down-regulation of MicroRNA-381 promotes cell proliferation and invasion in colon cancer through up-regulation of LRH-1. Biomed Pharmacother. 2015;75:137–41. https://doi.org/10.1016/j.biopha.2015.07.020.
Benod C, Carlsson J, Uthayaruban R, Hwang P, Irwin JJ, Doak AK, Shoichet BK, Sablin EP, Fletterick RJ. Structure-based discovery of antagonists of nuclear receptor LRH-1. J Biol Chem. 2013;288:19830–44. https://doi.org/10.1074/jbc.M112.411686.
Lai HT, Tseng WK, Huang SW, Chao TC, Su Y. MicroRNA-203 diminishes the stemness of human colon cancer cells by suppressing GATA6 expression. J Cell Physiol. 2020;235:2866–80. https://doi.org/10.1002/jcp.29192.
Schoonjans K, Dubuquoy L, Mebis J, Fayard E, Wendling O, Haby C, Geboes K, Auwerx J. Liver receptor homolog 1 contributes to intestinal tumor formation through effects on cell cycle and inflammation. Proc Natl Acad Sci U S A. 2005;102:2058–62. https://doi.org/10.1073/pnas.0409756102.
Bouguen G, Langlois A, Djouina M, Branche J, Koriche D, Dewaeles E, Mongy A, Auwerx J, Colombel JF, Desreumaux P, et al. Intestinal steroidogenesis controls PPARgamma expression in the colon and is impaired during ulcerative colitis. Gut. 2015;64:901–10. https://doi.org/10.1136/gutjnl-2014-307618.
Kramer HB, Lai CF, Patel H, Periyasamy M, Lin ML, Feller SM, Fuller-Pace FV, Meek DW, Ali S, Buluwela L. LRH-1 drives colon cancer cell growth by repressing the expression of the CDKN1A gene in a p53-dependent manner. Nucleic Acids Res. 2016;44:582–94. https://doi.org/10.1093/nar/gkv948.
Dianat-Moghadam H, Khalili M, Keshavarz M, Azizi M, Hamishehkar H, Rahbarghazi R, Nouri M. Modulation of LXR signaling altered the dynamic activity of human colon adenocarcinoma cancer stem cells in vitro. Cancer Cell Int. 2021;21:100. https://doi.org/10.1186/s12935-021-01803-4.
Courtaut F, Derangere V, Chevriaux A, Ladoire S, Cotte AK, Arnould L, Boidot R, Rialland M, Ghiringhelli F, Rebe C. Liver X receptor ligand cytotoxicity in colon cancer cells and not in normal colon epithelial cells depends on LXRbeta subcellular localization. Oncotarget. 2015;6:26651–62. https://doi.org/10.18632/oncotarget.5791.
Tang H, Mirshahidi S, Senthil M, Kazanjian K, Chen CS, Zhang K. Down-regulation of LXR/RXR activation and negative acute phase response pathways in colon adenocarcinoma revealed by proteomics and bioinformatics analysis. Cancer Biomark. 2014;14:313–24. https://doi.org/10.3233/CBM-140409.
Derangere V, Chevriaux A, Courtaut F, Bruchard M, Berger H, Chalmin F, Causse SZ, Limagne E, Vegran F, Ladoire S, et al. Liver X receptor beta activation induces pyroptosis of human and murine colon cancer cells. Cell Death Differ. 2014;21:1914–24. https://doi.org/10.1038/cdd.2014.117.
Vedin LL, Gustafsson JA, Steffensen KR. The oxysterol receptors LXRalpha and LXRbeta suppress proliferation in the colon. Mol Carcinog. 2013;52:835–44. https://doi.org/10.1002/mc.21924.
Uno S, Endo K, Jeong Y, Kawana K, Miyachi H, Hashimoto Y, Makishima M. Suppression of beta-catenin signaling by liver X receptor ligands. Biochem Pharmacol. 2009;77:186–95. https://doi.org/10.1016/j.bcp.2008.10.007.
Nguyen TTT, Ishida CT, Shang E, Shu C, Torrini C, Zhang Y, Bianchetti E, Sanchez-Quintero MJ, Kleiner G, Quinzii CM, et al. Activation of LXRbeta inhibits tumor respiration and is synthetically lethal with Bcl-xL inhibition. EMBO Mol Med. 2019;11: e10769. https://doi.org/10.15252/emmm.201910769.
Wang Q, Ren M, Feng F, Chen K, Ju X. Treatment of colon cancer with liver X receptor agonists induces immunogenic cell death. Mol Carcinog. 2018;57:903–10. https://doi.org/10.1002/mc.22811.
Warns J, Marwarha G, Freking N, Ghribi O. 27-hydroxycholesterol decreases cell proliferation in colon cancer cell lines. Biochimie. 2018;153:171–80. https://doi.org/10.1016/j.biochi.2018.07.006.
Hu Y, French SW, Chau T, Liu HX, Sheng L, Wei F, Stondell J, Garcia JC, Du Y, Bowlus CL, et al. RARbeta acts as both an upstream regulator and downstream effector of miR-22, which epigenetically regulates NUR77 to induce apoptosis of colon cancer cells. FASEB J. 2019;33:2314–26. https://doi.org/10.1096/fj.201801390R.
Cho SD, Lei P, Abdelrahim M, Yoon K, Liu S, Guo J, Papineni S, Chintharlapalli S, Safe S. 1,1-bis(3′-indolyl)-1-(p-methoxyphenyl)methane activates Nur77-independent proapoptotic responses in colon cancer cells. Mol Carcinog. 2008;47:252–63. https://doi.org/10.1002/mc.20378.
To SK, Zeng WJ, Zeng JZ, Wong AS. Hypoxia triggers a Nur77-beta-catenin feed-forward loop to promote the invasive growth of colon cancer cells. Br J Cancer. 2014;110:935–45. https://doi.org/10.1038/bjc.2013.816.
Lee SO, Li X, Hedrick E, Jin UH, Tjalkens RB, Backos DS, Li L, Zhang Y, Wu Q, Safe S. Diindolylmethane analogs bind NR4A1 and are NR4A1 antagonists in colon cancer cells. Mol Endocrinol. 2014;28:1729–39. https://doi.org/10.1210/me.2014-1102.
Kang HJ, Song MJ, Choung SY, Kim SJ, Le MO. Transcriptional induction of Nur77 by indomethacin that results in apoptosis of colon cancer cells. Biol Pharm Bull. 2000;23:815–9. https://doi.org/10.1248/bpb.23.815.
Hedrick E, Lee SO, Safe S. The nuclear orphan receptor NR4A1 regulates beta1-integrin expression in pancreatic and colon cancer cells and can be targeted by NR4A1 antagonists. Mol Carcinog. 2017;56:2066–75. https://doi.org/10.1002/mc.22662.
Hu Y, Chau T, Liu H-X, Liao D, Keane R, Nie Y, Yang H, Wan Y-JY. Bile acids regulate nuclear receptor (Nur77) expression and intracellular location to control proliferation and apoptosis. Mol Cancer Res. 2015;13:281–92.
Lei P, Abdelrahim M, Cho SD, Liu S, Chintharlapalli S, Safe S. 1,1-Bis(3′-indolyl)-1-(p-substituted phenyl)methanes inhibit colon cancer cell and tumor growth through activation of c-jun N-terminal kinase. Carcinogenesis. 2008;29:1139–47. https://doi.org/10.1093/carcin/bgn103.
Holla VR, Wu H, Shi Q, Menter DG, DuBois RN. Nuclear orphan receptor NR4A2 modulates fatty acid oxidation pathways in colorectal cancer. J Biol Chem. 2011;286:30003–9. https://doi.org/10.1074/jbc.M110.184697.
Abdel-Latif RT, Wadie W, Abdel-Mottaleb Y, Abdallah DM, El-Maraghy NN, El-Abhar HS. Reposition of the anti-inflammatory drug diacerein in an in-vivo colorectal cancer model. Saudi Pharm J. 2022;30:72–90. https://doi.org/10.1016/j.jsps.2021.12.009.
Lachal S, Ford J, Shulkes A, Baldwin GS. PPARα agonists stimulate progastrin production in human colorectal carcinoma cells. Regul Pept. 2004;120:243–51.
Grau R, Iñiguez MA, Fresno M. Inhibition of activator protein 1 activation, vascular endothelial growth factor, and cyclooxygenase-2 expression by 15-deoxy-Δ12, 14-prostaglandin J2 in colon carcinoma cells: evidence for a redox-sensitive peroxisome proliferator-activated receptor-γ-independent mechanism. Can Res. 2004;64:5162–71.
Kohno H, Yoshitani Si, Takashima S, Okumura A, Hosokawa M, Yamaguchi N, Tanaka T. Troglitazone, a Ligand for Peroxisome Proliferator-activated Receptor γ Inhibits Chemically-induced Aberrant Crypt Foci in Rats. Jpn J Cancer Res. 2001;92:396–403.
Gupta RA, Brockman JA, Sarraf P, Willson TM, DuBois RN. Target genes of peroxisome proliferator-activated receptor γ in colorectal cancer cells. J Biol Chem. 2001;276:29681–7.
Su W, Necela BM, Fujiwara K, Kurakata S, Murray NR, Fields AP, Thompson EA. The high affinity peroxisome proliferator-activated receptor-gamma agonist RS5444 inhibits both initiation and progression of colon tumors in azoxymethane-treated mice. Int J Cancer. 2008;123:991–7. https://doi.org/10.1002/ijc.23640.
Lin MS, Chen WC, Bai X, Wang YD. Activation of peroxisome proliferator-activated receptor γ inhibits cell growth via apoptosis and arrest of the cell cycle in human colorectal cancer. J Dig Dis. 2007;8:82–8.
Moon CM, Kwon JH, Kim JS, Oh SH, Jin Lee K, Park JJ, Pil Hong S, Cheon JH, Kim TI, Kim WH. Nonsteroidal anti-inflammatory drugs suppress cancer stem cells via inhibiting PTGS2 (cyclooxygenase 2) and NOTCH/HES1 and activating PPARG in colorectal cancer. Int J Cancer. 2014;134:519–29.
Kohno H, Yasui Y, Suzuki R, Hosokawa M, Miyashita K, Tanaka T. Dietary seed oil rich in conjugated linolenic acid from bitter melon inhibits azoxymethane-induced rat colon carcinogenesis through elevation of colonic PPARγ expression and alteration of lipid composition. Int J Cancer. 2004;110:896–901.
Wang J-B, Qi L-L, Zheng S-D, Wang H-Z, Wu T-X. Curcumin suppresses PPARδ expression and related genes in HT-29 cells. World J Gastroenterol: WJG. 2009;15:1346.
Ban JO, Kwak DH, Oh JH, Park EJ, Cho MC, Song HS, Song MJ, Han SB, Moon DC, Kang KW, et al. Suppression of NF-kappaB and GSK-3beta is involved in colon cancer cell growth inhibition by the PPAR agonist troglitazone. Chem Biol Interact. 2010;188:75–85. https://doi.org/10.1016/j.cbi.2010.06.001.
Yang L, Zhou J, Ma Q, Wang C, Chen K, Meng W, Yu Y, Zhou Z, Sun X. Knockdown of PPAR delta gene promotes the growth of colon cancer and reduces the sensitivity to bevacizumab in nude mice model. PLoS ONE. 2013;8: e60715. https://doi.org/10.1371/journal.pone.0060715.
Jackson L, Wahli W, Michalik L, Watson SA, Morris T, Anderton K, Bell DR, Smith JA, Hawkey CJ, Bennett AJ. Potential role for peroxisome proliferator activated receptor (PPAR) in preventing colon cancer. Gut. 2003;52:1317–22. https://doi.org/10.1136/gut.52.9.1317.
Tong JL, Zhang CP, Nie F, Xu XT, Zhu MM, Xiao SD, Ran ZH. MicroRNA 506 regulates expression of PPAR alpha in hydroxycamptothecin-resistant human colon cancer cells. FEBS Lett. 2011;585:3560–8. https://doi.org/10.1016/j.febslet.2011.10.021.
Aung CS, Faddy HM, Lister EJ, Monteith GR, Roberts-Thomson SJ. Isoform specific changes in PPAR alpha and beta in colon and breast cancer with differentiation. Biochem Biophys Res Commun. 2006;340:656–60. https://doi.org/10.1016/j.bbrc.2005.12.061.
Zhou D, Jin J, Liu Q, Shi J, Hou Y. PPARδ agonist enhances colitis-associated colorectal cancer. Eur J Pharmacol. 2019;842:248–54. https://doi.org/10.1016/j.ejphar.2018.10.050.
Yang W-L, Frucht H. Activation of the PPAR pathway induces apoptosis and COX-2 inhibition in HT-29 human colon cancer cells. Carcinogenesis. 2001;22:1379–83.
Campbell SE, Stone WL, Whaley SG, Qui M, Krishnan K. Gamma (gamma) tocopherol upregulates peroxisome proliferator activated receptor (PPAR) gamma (gamma) expression in SW 480 human colon cancer cell lines. BMC Cancer. 2003;3:25. https://doi.org/10.1186/1471-2407-3-25.
Yoshizumi T, Ohta T, Ninomiya I, Terada I, Fushida S, Fujimura T, Nishimura G, Shimizu K, Yi S, Miwa K. Thiazolidinedione, a peroxisome proliferator-activated receptor-gamma ligand, inhibits growth and metastasis of HT-29 human colon cancer cells through differentiation-promoting effects. Int J Oncol. 2004;25:631–9.
Chintharlapalli S, Papineni S, Liu S, Jutooru I, Chadalapaka G, Cho S-d, Murthy RS, You Y, Safe S. 2-Cyano-lup-1-en-3-oxo-20-oic acid, a cyano derivative of betulinic acid, activates peroxisome proliferator-activated receptor γ in colon and pancreatic cancer cells. Carcinogenesis. 2007;28:2337–46.
Shen D, Deng C, Zhang M. Peroxisome proliferator-activated receptor gamma agonists inhibit the proliferation and invasion of human colon cancer cells. Postgrad Med J. 2007;83:414–9. https://doi.org/10.1136/pmj.2006.052761.
Choi IK, Kim YH, Kim JS, Seo JH. PPAR-gamma ligand promotes the growth of APC-mutated HT-29 human colon cancer cells in vitro and in vivo. Invest New Drugs. 2008;26:283–8. https://doi.org/10.1007/s10637-007-9108-x.
Dai Y, Qiao L, Chan KW, Zou B, Ma J, Lan HY, Gu Q, Li Z, Wang Y, Wong BL, et al. Loss of XIAP sensitizes rosiglitazone-induced growth inhibition of colon cancer in vivo. Int J Cancer. 2008;122:2858–63. https://doi.org/10.1002/ijc.23443.
Rageul J, Mottier S, Jarry A, Shah Y, Théoleyre S, Masson D, Gonzalez FJ, Laboisse CL, Denis MG. KLF4-dependent, PPARgamma-induced expression of GPA33 in colon cancer cell lines. Int J Cancer. 2009;125:2802–9. https://doi.org/10.1002/ijc.24683.
Tsukahara T, Haniu H, Matsuda Y. PTB-associated splicing factor (PSF) is a PPARγ-binding protein and growth regulator of colon cancer cells. PLoS ONE. 2013;8: e58749.
Tylichová Z, Straková N, Vondráček J, Vaculová AH, Kozubík A, Hofmanová J. Activation of autophagy and PPARγ protect colon cancer cells against apoptosis induced by interactive effects of butyrate and DHA in a cell type-dependent manner: The role of cell differentiation. J Nutr Biochem. 2017;39:145–55. https://doi.org/10.1016/j.jnutbio.2016.09.006.
Yaacob NS, Darus HM, Norazmi MN. Modulation of cell growth and PPARγ expression in human colorectal cancer cell lines by ciglitazone. Exp Toxicol Pathol. 2008;60:505–12.
Lee JY, Hwang DH. Docosahexaenoic acid suppresses the activity of peroxisome proliferator-activated receptors in a colon tumor cell line. Biochem Biophys Res Commun. 2002;298:667–74. https://doi.org/10.1016/s0006-291x(02)02530-5.
Osawa E, Nakajima A, Wada K, Ishimine S, Fujisawa N, Kawamori T, Matsuhashi N, Kadowaki T, Ochiai M, Sekihara H, et al. Peroxisome proliferator-activated receptor gamma ligands suppress colon carcinogenesis induced by azoxymethane in mice. Gastroenterology. 2003;124:361–7. https://doi.org/10.1053/gast.2003.50067.
Weidner C, Rousseau M, Micikas RJ, Fischer C, Plauth A, Wowro SJ, Siems K, Hetterling G, Kliem M, Schroeder FC. Amorfrutin C induces apoptosis and inhibits proliferation in colon cancer cells through targeting mitochondria. J Nat Prod. 2016;79:2–12.
Mielczarek-Puta M, Otto-Slusarczyk D, Chrzanowska A, Filipek A, Grabon W. Telmisartan influences the antiproliferative activity of linoleic acid in human colon cancer cells. Nutr Cancer. 2020;72:98–109. https://doi.org/10.1080/01635581.2019.1613552.
Papi A, Rocchi P, Ferreri AM, Orlandi M. RXRγ and PPARγ ligands in combination to inhibit proliferation and invasiveness in colon cancer cells. Cancer Lett. 2010;297:65–74.
Bansard L, Bouvet O, Moutin E, Le Gall G, Giammona A, Pothin E, Bacou M, Hassen-Khodja C, Bordignon B, Bourgaux JF. Niclosamide induces miR-148a to inhibit PXR and sensitize colon cancer stem cells to chemotherapy. Stem Cell Reports. 2022;17:835–48.
Planque C, Rajabi F, Grillet F, Finetti P, Bertucci F, Gironella M, Lozano JJ, Beucher B, Giraud J, Garambois V. Pregnane X-receptor promotes stem cell-mediated colon cancer relapse. Oncotarget. 2016;7:56558.
Cheng J, Fang Z-Z, Nagaoka K, Okamoto M, Qu A, Tanaka N, Kimura S, Gonzalez FJ. Activation of intestinal human pregnane X receptor protects against azoxymethane/dextran sulfate sodium-induced colon cancer. J Pharmacol Exp Ther. 2014;351:559–67.
Zimmermann C, van Waterschoot RA, Harmsen S, Maier A, Gutmann H, Schinkel AH. PXR-mediated induction of human CYP3A4 and mouse Cyp3a11 by the glucocorticoid budesonide. Eur J Pharm Sci. 2009;36:565–71.
Cheng J, Shah YM, Ma X, Pang X, Tanaka T, Kodama T, Krausz KW, Gonzalez FJ. Therapeutic role of rifaximin in inflammatory bowel disease: clinical implication of human pregnane X receptor activation. J Pharmacol Exp Ther. 2010;335:32–41.
Dou W, Mukherjee S, Li H, Venkatesh M, Wang H, Kortagere S, Peleg A, Chilimuri SS, Wang Z-T, Feng Y. Alleviation of gut inflammation by Cdx2/Pxr pathway in a mouse model of chemical colitis. PLoS ONE. 2012;7:e36075.
Liu C-L, Lim Y-P, Hu M-L. Fucoxanthin attenuates rifampin-induced cytochrome P450 3A4 (CYP3A4) and multiple drug resistance 1 (MDR1) gene expression through pregnane X receptor (PXR)-mediated pathways in human hepatoma HepG2 and colon adenocarcinoma LS174T cells. Mar Drugs. 2012;10:242–57.
Esposito G, Gigli S, Seguella L, Nobile N, D’alessandro A, Pesce M, Capoccia E, Steardo L, Cirillo C, Cuomo R. Rifaximin, a non-absorbable antibiotic, inhibits the release of pro-angiogenic mediators in colon cancer cells through a pregnane X receptor-dependent pathway. Int J Oncol. 2016;49:639–45.
Harmsen S, Meijerman I, Febus C, Maas-Bakker R, Beijnen J, Schellens J. PXR-mediated induction of P-glycoprotein by anticancer drugs in a human colon adenocarcinoma-derived cell line. Cancer Chemother Pharmacol. 2010;66:765–71.
Habano W, Gamo T, Terashima J, Sugai T, Otsuka K, Wakabayashi G, Ozawa S. Involvement of promoter methylation in the regulation of Pregnane X receptor in colon cancer cells. BMC Cancer. 2011;11:1–10.
Kuo CT, Lee WS. Progesterone receptor activation is required for folic acid-induced anti-proliferation in colorectal cancer cell lines. Cancer Lett. 2016;378:104–10. https://doi.org/10.1016/j.canlet.2016.05.019.
Cesario RM, Stone J, Yen W-C, Bissonnette RP, Lamph WW. Differentiation and growth inhibition mediated via the RXR: PPARγ heterodimer in colon cancer. Cancer Lett. 2006;240:225–33.
Dillard AC, Lane MA. Retinol decreases β-catenin protein levels in retinoic acid-resistant colon cancer cell lines. Mol Carcinog. 2007;46:315–29.
Fan YY, Spencer TE, Wang N, Moyer MP, Chapkin RS. Chemopreventive n-3 fatty acids activate RXRalpha in colonocytes. Carcinogenesis. 2003;24:1541–8. https://doi.org/10.1093/carcin/bgg110.
Janakiram NB, Mohammed A, Qian L, Choi C-I, Steele VE, Rao CV. Chemopreventive effects of RXR-selective rexinoid bexarotene on intestinal neoplasia of ApcMin/+ mice. Neoplasia. 2012;14:159–68.
Ruan H, Zhan Y, Hou J, Xu B, Chen B, Tian Y, Wu D, Zhao Y, Zhang Y, Chen X. Berberine binds RXRα to suppress β-catenin signaling in colon cancer cells. Oncogene. 2017;36:6906–18.
Xu B, Jiang X, Xiong J, Lan J, Tian Y, Zhong L, Wang X, Xu N, Cao H, Zhang W. Structure–activity relationship study enables the discovery of a novel berberine analogue as the RXRα activator to inhibit colon cancer. J Med Chem. 2020;63:5841–55.
Papi A, Ferreri A, Guerra F, Orlandi M. Anti-invasive effects and proapoptotic activity induction by the rexinoid IIF and valproic acid in combination on colon cancer cell lines. Anticancer Res. 2012;32:2855–62.
Natsume H, Sasaki S, Kitagawa M, Kashiwabara Y, Matsushita A, Nakano K, Nishiyama K, Nagayama K, Misawa H, Masuda H, et al. Beta-catenin/Tcf-1-mediated transactivation of cyclin D1 promoter is negatively regulated by thyroid hormone. Biochem Biophys Res Commun. 2003;309:408–13. https://doi.org/10.1016/j.bbrc.2003.08.019.
Pourvali K, Shimi G, Ghorbani A, Shakery A, Shirazi FH, Zand H. Selective thyroid hormone receptor beta agonist, GC-1, is capable to reduce growth of colorectal tumor in syngeneic mouse models. J Recept Signal Transduct Res. 2022;42:495–502. https://doi.org/10.1080/10799893.2022.2032748.
Ben-Shoshan M, Amir S, Dang DT, Dang LH, Weisman Y, Mabjeesh NJ. 1alpha,25-dihydroxyvitamin D3 (Calcitriol) inhibits hypoxia-inducible factor-1/vascular endothelial growth factor pathway in human cancer cells. Mol Cancer Ther. 2007;6:1433–9. https://doi.org/10.1158/1535-7163.MCT-06-0677.
Fernandez-Garcia NI, Palmer HG, Garcia M, Gonzalez-Martin A, del Rio M, Barettino D, Volpert O, Munoz A, Jimenez B. 1alpha,25-Dihydroxyvitamin D3 regulates the expression of Id1 and Id2 genes and the angiogenic phenotype of human colon carcinoma cells. Oncogene. 2005;24:6533–44. https://doi.org/10.1038/sj.onc.1208801.
Meyer MB, Goetsch PD, Pike JW. VDR/RXR and TCF4/beta-catenin cistromes in colonic cells of colorectal tumor origin: impact on c-FOS and c-MYC gene expression. Mol Endocrinol. 2012;26:37–51. https://doi.org/10.1210/me.2011-1109.
Ranji P, Agah S, Heydari Z, Rahmati-Yamchi M, Mohammad Alizadeh A. Effects of Lactobacillus acidophilus and Bifidobacterium bifidum probiotics on the serum biochemical parameters, and the vitamin D and leptin receptor genes on mice colon cancer. Iran J Basic Med Sci. 2019;22:631–6. https://doi.org/10.22038/ijbms.2019.32624.7806.
Palmer HG, Gonzalez-Sancho JM, Espada J, Berciano MT, Puig I, Baulida J, Quintanilla M, Cano A, de Herreros AG, Lafarga M, et al. Vitamin D(3) promotes the differentiation of colon carcinoma cells by the induction of E-cadherin and the inhibition of beta-catenin signaling. J Cell Biol. 2001;154:369–87. https://doi.org/10.1083/jcb.200102028.
Donohue MM, Demay MB. Rickets in VDR null mice is secondary to decreased apoptosis of hypertrophic chondrocytes. Endocrinology. 2002;143:3691–4. https://doi.org/10.1210/en.2002-220454.
Kallay E, Pietschmann P, Toyokuni S, Bajna E, Hahn P, Mazzucco K, Bieglmayer C, Kato S, Cross HS. Characterization of a vitamin D receptor knockout mouse as a model of colorectal hyperproliferation and DNA damage. Carcinogenesis. 2001;22:1429–35. https://doi.org/10.1093/carcin/22.9.1429.
Zhu Y, Mahon BD, Froicu M, Cantorna MT. Calcium and 1 alpha,25-dihydroxyvitamin D3 target the TNF-alpha pathway to suppress experimental inflammatory bowel disease. Eur J Immunol. 2005;35:217–24. https://doi.org/10.1002/eji.200425491.
Iseki K, Tatsuta M, Uehara H, Iishi H, Yano H, Sakai N, Ishiguro S. Inhibition of angiogenesis as a mechanism for inhibition by 1alpha-hydroxyvitamin D3 and 1,25-dihydroxyvitamin D3 of colon carcinogenesis induced by azoxymethane in Wistar rats. Int J Cancer. 1999;81:730–3. https://doi.org/10.1002/(sici)1097-0215(19990531)81:5%3c730::aid-ijc11%3e3.0.co;2-q.
Chen S, Bu D, Ma Y, Zhu J, Chen G, Sun L, Zuo S, Li T, Pan Y, Wang X, et al. H19 Overexpression Induces Resistance to 1,25(OH)2D3 by Targeting VDR Through miR-675-5p in Colon Cancer Cells. Neoplasia. 2017;19:226–36. https://doi.org/10.1016/j.neo.2016.10.007.
Zhang Y, Garrett S, Carroll RE, Xia Y, Sun J. Vitamin D receptor upregulates tight junction protein claudin-5 against colitis-associated tumorigenesis. Mucosal Immunol. 2022;15:683–97. https://doi.org/10.1038/s41385-022-00502-1.
Larriba MJ, Ordonez-Moran P, Chicote I, Martin-Fernandez G, Puig I, Munoz A, Palmer HG. Vitamin D receptor deficiency enhances Wnt/beta-catenin signaling and tumor burden in colon cancer. PLoS ONE. 2011;6: e23524. https://doi.org/10.1371/journal.pone.0023524.
Ishizawa M, Hirayu A, Makishima M. Zinc Inhibits Cadherin 1 Expression Induced by 1α, 25-Dihydroxyvitamin D3 in Colon Cancer Cells. Anticancer Res. 2021;41:5453–9.
Thompson PD, Jurutka PW, Whitfield GK, Myskowski SM, Eichhorst KR, Dominguez CE, Haussler CA, Haussler MR. Liganded VDR induces CYP3A4 in small intestinal and colon cancer cells via DR3 and ER6 vitamin D responsive elements. Biochem Biophys Res Commun. 2002;299:730–8.
Egan JB, Thompson PA, Vitanov MV, Bartik L, Jacobs ET, Haussler MR, Gerner EW, Jurutka PW. Vitamin D receptor ligands, adenomatous polyposis coli, and the vitamin D receptor FokI polymorphism collectively modulate β-catenin activity in colon cancer cells. Mol Carcinog. 2010;49:337–52.
Bartik L, Whitfield GK, Kaczmarska M, Lowmiller CL, Moffet EW, Furmick JK, Hernandez Z, Haussler CA, Haussler MR, Jurutka PW. Curcumin: a novel nutritionally derived ligand of the vitamin D receptor with implications for colon cancer chemoprevention. J Nutr Biochem. 2010;21:1153–61.
Qi X, Tang J, Pramanik R, Schultz RM, Shirasawa S, Sasazuki T, Han J, Chen G. p38 MAPK activation selectively induces cell death in K-ras-mutated human colon cancer cells through regulation of vitamin D receptor. J Biol Chem. 2004;279:22138–44.
Beildeck ME, Islam M, Shah S, Welsh J, Byers SW. Control of TCF-4 expression by VDR and vitamin D in the mouse mammary gland and colorectal cancer cell lines. PLoS ONE. 2009;4: e7872.
Chua FY, Adams BD. Androgen receptor and miR-206 regulation in prostate cancer. Transcription. 2017;8:313–27. https://doi.org/10.1080/21541264.2017.1322668.
Burris TP, Solt LA, Wang Y, Crumbley C, Banerjee S, Griffett K, Lundasen T, Hughes T, Kojetin DJ. Nuclear receptors and their selective pharmacologic modulators. Pharmacol Rev. 2013;65:710–78. https://doi.org/10.1124/pr.112.006833.
Davey RA, Grossmann M. Androgen Receptor Structure, Function and Biology: From Bench to Bedside. Clin Biochem Rev. 2016;37:3–15.
Uhlen M, Fagerberg L, Hallstrom BM, Lindskog C, Oksvold P, Mardinoglu A, Sivertsson A, Kampf C, Sjostedt E, Asplund A. Proteomics. Tissue-based map of the human proteome. Science. 2015;347:1260419. https://doi.org/10.1126/science.1260419.
Aurilio G, Cimadamore A, Mazzucchelli R, Lopez-Beltran A, Verri E, Scarpelli M, Massari F, Cheng L, Santoni M, Montironi R. Androgen receptor signaling pathway in prostate cancer: from genetics to clinical applications. Cells. 2020. https://doi.org/10.3390/cells9122653.
Buchanan G, Birrell SN, Peters AA, Bianco-Miotto T, Ramsay K, Cops EJ, Yang M, Harris JM, Simila HA, Moore NL. Decreased androgen receptor levels and receptor function in breast cancer contribute to the failure of response to medroxyprogesterone acetate. Can Res. 2005;65:8487–96.
Castellano I, Allia E, Accortanzo V, Vandone AM, Chiusa L, Arisio R, Durando A, Donadio M, Bussolati G, Coates AS. Androgen receptor expression is a significant prognostic factor in estrogen receptor positive breast cancers. Breast Cancer Res Treat. 2010;124:607–17.
Gucalp A, Traina TA. Triple-negative breast cancer: role of the androgen receptor. Cancer J. 2010;16:62–5.
Lønning PE. Additive endocrine therapy for advanced breast cancer–back to the future. Acta Oncol. 2009;48:1092–101.
Peters AA, Buchanan G, Ricciardelli C, Bianco-Miotto T, Centenera MM, Harris JM, Jindal S, Segara D, Jia L, Moore NL. Androgen receptor inhibits estrogen receptor-α activity and is prognostic in breast cancer. Can Res. 2009;69:6131–40.
Izbicki JR, Wambach G, Hamilton SR, Harnisch E, Hogenschurz R, Izbicki W, Kusche J. Androgen receptors in experimentally induced colon carcinogenesis. J Cancer Res Clin Oncol. 1986;112:39–46. https://doi.org/10.1007/BF00394937.
Li H, Kim JH, Koh SS, Stallcup MR. Synergistic effects of coactivators GRIP1 and beta-catenin on gene activation: cross-talk between androgen receptor and Wnt signaling pathways. J Biol Chem. 2004;279:4212–20. https://doi.org/10.1074/jbc.M311374200.
Song LN, Gelmann EP. Interaction of beta-catenin and TIF2/GRIP1 in transcriptional activation by the androgen receptor. J Biol Chem. 2005;280:37853–67. https://doi.org/10.1074/jbc.M503850200.
Yang F, Li X, Sharma M, Sasaki CY, Longo DL, Lim B, Sun Z. Linking beta-catenin to androgen-signaling pathway. J Biol Chem. 2002;277:11336–44. https://doi.org/10.1074/jbc.M111962200.
Mulholland DJ, Cheng H, Reid K, Rennie PS, Nelson CC. The androgen receptor can promote beta-catenin nuclear translocation independently of adenomatous polyposis coli. J Biol Chem. 2002;277:17933–43. https://doi.org/10.1074/jbc.M200135200.
Chesire DR, Isaacs WB. Ligand-dependent inhibition of beta-catenin/TCF signaling by androgen receptor. Oncogene. 2002;21:8453–69. https://doi.org/10.1038/sj.onc.1206049.
Asim M, Siddiqui IA, Hafeez BB, Baniahmad A, Mukhtar H. Src kinase potentiates androgen receptor transactivation function and invasion of androgen-independent prostate cancer C4–2 cells. Oncogene. 2008;27:3596–604. https://doi.org/10.1038/sj.onc.1211016.
Cai H, Babic I, Wei X, Huang J, Witte ON. Invasive prostate carcinoma driven by c-Src and androgen receptor synergy. Cancer Res. 2011;71:862–72. https://doi.org/10.1158/0008-5472.CAN-10-1605.
Migliaccio A, Castoria G, Di Domenico M, de Falco A, Bilancio A, Lombardi M, Barone MV, Ametrano D, Zannini MS, Abbondanza C, et al. Steroid-induced androgen receptor-oestradiol receptor beta-Src complex triggers prostate cancer cell proliferation. EMBO J. 2000;19:5406–17. https://doi.org/10.1093/emboj/19.20.5406.
Ferro P, Catalano MG, Raineri M, Reato G, dell’Eva R, Risio M, Foa R, Fortunati N, Pfeffer U. Somatic alterations of the androgen receptor CAG repeat in human colon cancer delineate a novel mutation pathway independent of microsatellite instability. Cancer Genet Cytogenet. 2000;123:35–40. https://doi.org/10.1016/s0165-4608(00)00296-x.
Slattery ML, Sweeney C, Murtaugh M, Ma KN, Caan BJ, Potter JD, Wolff R. Associations between vitamin D, vitamin D receptor gene and the androgen receptor gene with colon and rectal cancer. Int J Cancer. 2006;118:3140–6. https://doi.org/10.1002/ijc.21791.
Kim K, Kumagai J, Eishi Y, Ishige I, Ishige Y, Koike M. Clonality analysis for normal and cancerous colon tissues with human androgen receptor gene polymerase chain reaction. J Med Dent Sci. 2005;52:163–70.
Xia T, Sun H, Huang H, Bi H, Pu R, Zhang L, Zhang Y, Liu Y, Xu J, Onwuka JU, et al. Androgen receptor gene methylation related to colorectal cancer risk. Endocr Connect. 2019;8:979–87. https://doi.org/10.1530/EC-19-0122.
Klepsch V, Siegmund K, Baier G. Emerging next-generation target for cancer immunotherapy research: the orphan nuclear receptor NR2F6. Cancers (Basel). 2021. https://doi.org/10.3390/cancers13112600.
Yu K, Huang ZY, Xu XL, Li J, Fu XW, Deng SL. Estrogen receptor function: impact on the human endometrium. Front Endocrinol (Lausanne). 2022;13: 827724. https://doi.org/10.3389/fendo.2022.827724.
Bharathkumar H, Mohan CD, Ananda H, Fuchs JE, Li F, Rangappa S, Surender M, Bulusu KC, Girish KS, Sethi G. Microwave-assisted synthesis, characterization and cytotoxic studies of novel estrogen receptor α ligands towards human breast cancer cells. Bioorg Med Chem Lett. 2015;25:1804–7.
Marino M, Galluzzo P, Ascenzi P. Estrogen signaling multiple pathways to impact gene transcription. Curr Genomics. 2006;7:497–508. https://doi.org/10.2174/138920206779315737.
Jia M, Dahlman-Wright K, Gustafsson JA. Estrogen receptor alpha and beta in health and disease. Best Pract Res Clin Endocrinol Metab. 2015;29:557–68. https://doi.org/10.1016/j.beem.2015.04.008.
Paterni I, Granchi C, Katzenellenbogen JA, Minutolo F. Estrogen receptors alpha (ERalpha) and beta (ERbeta): subtype-selective ligands and clinical potential. Steroids. 2014;90:13–29. https://doi.org/10.1016/j.steroids.2014.06.012.
Chang EC, Frasor J, Komm B, Katzenellenbogen BS. Impact of estrogen receptor beta on gene networks regulated by estrogen receptor alpha in breast cancer cells. Endocrinology. 2006;147:4831–42. https://doi.org/10.1210/en.2006-0563.
Indukuri R, Hases L, Archer A, Williams C. Estrogen receptor beta influences the inflammatory p65 cistrome in colon cancer cells. Front Endocrinol (Lausanne). 2021;12: 650625. https://doi.org/10.3389/fendo.2021.650625.
Macdonald RS, Wagner K. Influence of dietary phytochemicals and microbiota on colon cancer risk. J Agric Food Chem. 2012;60:6728–35. https://doi.org/10.1021/jf204230r.
Berner C, Aumüller E, Gnauck A, Nestelberger M, Just A, Haslberger AG. Epigenetic control of estrogen receptor expression and tumor suppressor genes is modulated by bioactive food compounds. Ann Nutr Metab. 2010;57:183–9.
Stein RA, McDonnell DP. Estrogen-related receptor alpha as a therapeutic target in cancer. Endocr Relat Cancer. 2006;13(Suppl 1):S25-32. https://doi.org/10.1677/erc.1.01292.
Tripathi M, Yen PM, Singh BK. Estrogen-related receptor alpha: an under-appreciated potential target for the treatment of metabolic diseases. Int J Mol Sci. 2020. https://doi.org/10.3390/ijms21051645.
Vernier M, Dufour CR, McGuirk S, Scholtes C, Li X, Bourmeau G, Kuasne H, Park M, St-Pierre J, Audet-Walsh E, et al. Estrogen-related receptors are targetable ROS sensors. Genes Dev. 2020;34:544–59. https://doi.org/10.1101/gad.330746.119.
Ranhotra HS. Estrogen-related receptor alpha and cancer: axis of evil. J Recept Signal Transduct Res. 2015;35:505–8. https://doi.org/10.3109/10799893.2015.1049362.
Ding S, Tang Z, Jiang Y, Huang H, Luo P, Qing B, Zhang S, Tang R. IL-8 is involved in estrogen-related receptor alpha-regulated proliferation and migration of colorectal cancer cells. Dig Dis Sci. 2017;62:3438–46. https://doi.org/10.1007/s10620-017-4779-4.
Pellicciari R, Costantino G, Fiorucci S. Farnesoid X receptor: from structure to potential clinical applications. J Med Chem. 2005;48:5383–403. https://doi.org/10.1021/jm0582221.
Wang YD, Chen WD, Wang M, Yu D, Forman BM, Huang W. Farnesoid X receptor antagonizes nuclear factor kappaB in hepatic inflammatory response. Hepatology. 2008;48:1632–43. https://doi.org/10.1002/hep.22519.
Sayin SI, Wahlstrom A, Felin J, Jantti S, Marschall HU, Bamberg K, Angelin B, Hyotylainen T, Oresic M, Backhed F. Gut microbiota regulates bile acid metabolism by reducing the levels of tauro-beta-muricholic acid, a naturally occurring FXR antagonist. Cell Metab. 2013;17:225–35. https://doi.org/10.1016/j.cmet.2013.01.003.
Trauner M, Gulamhusein A, Hameed B, Caldwell S, Shiffman ML, Landis C, Eksteen B, Agarwal K, Muir A, Rushbrook S, et al. The nonsteroidal farnesoid X receptor agonist cilofexor (GS-9674) improves markers of cholestasis and liver injury in patients with primary sclerosing cholangitis. Hepatology. 2019;70:788–801. https://doi.org/10.1002/hep.30509.
Jiang L, Zhang H, Xiao D, Wei H, Chen Y. Farnesoid X receptor (FXR): structures and ligands. Comput Struct Biotechnol J. 2021;19:2148–59. https://doi.org/10.1016/j.csbj.2021.04.029.
Markham A, Keam SJ. Obeticholic acid: first global approval. Drugs. 2016;76:1221–6. https://doi.org/10.1007/s40265-016-0616-x.
You W, Chen B, Liu X, Xue S, Qin H, Jiang H. Farnesoid X receptor, a novel proto-oncogene in non-small cell lung cancer, promotes tumor growth via directly transactivating CCND1. Sci Rep. 2017;7:591. https://doi.org/10.1038/s41598-017-00698-4.
Giaginis C, Tsoukalas N, Alexandrou P, Tsourouflis G, Dana E, Delladetsima I, Patsouris E, Theocharis S. Clinical significance of farnesoid X receptor expression in thyroid neoplasia. Future Oncol. 2017;13:1785–92. https://doi.org/10.2217/fon-2017-0090.
Giaginis C, Karandrea D, Alexandrou P, Giannopoulou I, Tsourouflis G, Troungos C, Danas E, Keramopoulos A, Patsouris E, Nakopoulou L, et al. High Farnesoid X Receptor (FXR) expression is a strong and independent prognosticator in invasive breast carcinoma. Neoplasma. 2017;64:633–9. https://doi.org/10.4149/neo_2017_420.
Girisa S, Parama D, Harsha C, Banik K, Kunnumakkara AB. Potential of guggulsterone, a farnesoid X receptor antagonist, in the prevention and treatment of cancer. Explor Target Antitumor Ther. 2020;1:313–42.
Yeh MM, Bosch DE, Daoud SS. Role of hepatocyte nuclear factor 4-alpha in gastrointestinal and liver diseases. World J Gastroenterol. 2019;25:4074–91. https://doi.org/10.3748/wjg.v25.i30.4074.
Sun Q, Xu W, Ji S, Qin Y, Liu W, Hu Q, Zhang Z, Liu M, Yu X, Xu X. Role of hepatocyte nuclear factor 4 alpha in cell proliferation and gemcitabine resistance in pancreatic adenocarcinoma. Cancer Cell Int. 2019;19:49. https://doi.org/10.1186/s12935-019-0767-4.
Lv DD, Zhou LY, Tang H. Hepatocyte nuclear factor 4alpha and cancer-related cell signaling pathways: a promising insight into cancer treatment. Exp Mol Med. 2021;53:8–18. https://doi.org/10.1038/s12276-020-00551-1.
Wu N, Zhang YL, Wang HT, Li DW, Dai HJ, Zhang QQ, Zhang J, Ma Y, Xia Q, Bian JM, et al. Overexpression of hepatocyte nuclear factor 4alpha in human mesenchymal stem cells suppresses hepatocellular carcinoma development through Wnt/beta-catenin signaling pathway downregulation. Cancer Biol Ther. 2016;17:558–65. https://doi.org/10.1080/15384047.2016.1177675.
Ma L, Zeng J, Guo Q, Liang X, Shen L, Li S, Sun Y, Li W, Liu S, Yu H, et al. Mutual amplification of HNF4alpha and IL-1R1 composes an inflammatory circuit in Helicobacter pylori associated gastric carcinogenesis. Oncotarget. 2016;7:11349–63. https://doi.org/10.18632/oncotarget.7239.
Grandis JR, Drenning SD, Chakraborty A, Zhou MY, Zeng Q, Pitt AS, Tweardy DJ. Requirement of Stat3 but not Stat1 activation for epidermal growth factor receptor- mediated cell growth In vitro. J Clin Invest. 1998;102:1385–92. https://doi.org/10.1172/JCI3785.
Yang YM, Lee CG, Koo JH, Kim TH, Lee JM, An J, Kim KM, Kim SG. Galpha12 overexpressed in hepatocellular carcinoma reduces microRNA-122 expression via HNF4alpha inactivation, which causes c-Met induction. Oncotarget. 2015;6:19055–69. https://doi.org/10.18632/oncotarget.3957.
Darsigny M, Babeu JP, Dupuis AA, Furth EE, Seidman EG, Levy E, Verdu EF, Gendron FP, Boudreau F. Loss of hepatocyte-nuclear-factor-4alpha affects colonic ion transport and causes chronic inflammation resembling inflammatory bowel disease in mice. PLoS ONE. 2009;4:e7609. https://doi.org/10.1371/journal.pone.0007609.
Saandi T, Baraille F, Derbal-Wolfrom L, Cattin AL, Benahmed F, Martin E, Cardot P, Duclos B, Ribeiro A, Freund JN, et al. Regulation of the tumor suppressor homeogene Cdx2 by HNF4alpha in intestinal cancer. Oncogene. 2013;32:3782–8. https://doi.org/10.1038/onc.2012.401.
Pervin M, Paeng N, Yasui K, Imai S, Isemura M, Yokogoshi H, Nakayama T. Effects of Lens culinaris agglutinin on gene expression of gluconeogenic enzymes in the mouse intestine. J Sci Food Agric. 2012;92:857–61. https://doi.org/10.1002/jsfa.4658.
Chellappa K, Deol P, Evans JR, Vuong LM, Chen G, Briancon N, Bolotin E, Lytle C, Nair MG, Sladek FM. Opposing roles of nuclear receptor HNF4alpha isoforms in colitis and colitis-associated colon cancer. Elife. 2016. https://doi.org/10.7554/eLife.10903.
Nadolny C, Dong X. Liver receptor homolog-1 (LRH-1): a potential therapeutic target for cancer. Cancer Biol Ther. 2015;16:997–1004. https://doi.org/10.1080/15384047.2015.1045693.
Mays SG, Okafor CD, Tuntland ML, Whitby RJ, Dharmarajan V, Stec J, Griffin PR, Ortlund EA. Structure and Dynamics of the Liver Receptor Homolog 1-PGC1alpha Complex. Mol Pharmacol. 2017;92:1–11. https://doi.org/10.1124/mol.117.108514.
Meinsohn MC, Smith OE, Bertolin K, Murphy BD. The orphan nuclear receptors steroidogenic factor-1 and liver receptor homolog-1: structure, regulation, and essential roles in mammalian reproduction. Physiol Rev. 2019;99:1249–79. https://doi.org/10.1152/physrev.00019.2018.
Sidler D, Renzulli P, Schnoz C, Berger B, Schneider-Jakob S, Fluck C, Inderbitzin D, Corazza N, Candinas D, Brunner T. Colon cancer cells produce immunoregulatory glucocorticoids. Oncogene. 2011;30:2411–9. https://doi.org/10.1038/onc.2010.629.
Sidler D, Renzulli P, Schnoz C, Berger B, Schneider-Jakob S, Fluck C, Inderbitzin D, Corazza N, Candinas D, Brunner T. Colon cancer cells produce immunoregulatory glucocorticoids. Oncoimmunology. 2012;1:529–30. https://doi.org/10.4161/onci.19459.
Wang B, Tontonoz P. Liver X receptors in lipid signalling and membrane homeostasis. Nat Rev Endocrinol. 2018;14:452–63. https://doi.org/10.1038/s41574-018-0037-x.
Gao BC, Chen Q, Sun T, Wang DM, Xiao J. Research progress of the relationship between liver X receptor and inflammatory-related diseases. Sheng Li Xue Bao. 2018;70:335–41.
Zhu R, Ou Z, Ruan X, Gong J. Role of liver X receptors in cholesterol efflux and inflammatory signaling (review). Mol Med Rep. 2012;5:895–900. https://doi.org/10.3892/mmr.2012.758.
Bilotta MT, Petillo S, Santoni A, Cippitelli M. Liver X receptors: regulators of cholesterol metabolism, inflammation, autoimmunity, and cancer. Front Immunol. 2020;11:584303. https://doi.org/10.3389/fimmu.2020.584303.
Lin CY, Gustafsson JA. Targeting liver X receptors in cancer therapeutics. Nat Rev Cancer. 2015;15:216–24. https://doi.org/10.1038/nrc3912.
Rebe C, Derangere V, Ghiringhelli F. Induction of pyroptosis in colon cancer cells by LXRbeta. Mol Cell Oncol. 2015;2:e970094. https://doi.org/10.4161/23723548.2014.970094.
Sharma B, Gupta V, Dahiya D, Kumar H, Vaiphei K, Agnihotri N. Clinical relevance of cholesterol homeostasis genes in colorectal cancer. Biochim Biophys Acta Mol Cell Biol Lipids. 2019;1864:1314–27. https://doi.org/10.1016/j.bbalip.2019.06.008.
Yun SH, Park MG, Kim YM, Roh MS, Park JI. Expression of chicken ovalbumin upstream promoter-transcription factor II and liver X receptor as prognostic indicators for human colorectal cancer. Oncol Lett. 2017;14:4011–20. https://doi.org/10.3892/ol.2017.6659.
To SK, Zeng JZ, Wong AS. Nur77: a potential therapeutic target in cancer. Expert Opin Ther Targets. 2012;16:573–85. https://doi.org/10.1517/14728222.2012.680958.
Wansa KD, Harris JM, Muscat GE. The activation function-1 domain of Nur77/NR4A1 mediates trans-activation, cell specificity, and coactivator recruitment. J Biol Chem. 2002;277:33001–11. https://doi.org/10.1074/jbc.M203572200.
Chen HZ, Liu QF, Li L, Wang WJ, Yao LM, Yang M, Liu B, Chen W, Zhan YY, Zhang MQ, et al. The orphan receptor TR3 suppresses intestinal tumorigenesis in mice by downregulating Wnt signalling. Gut. 2012;61:714–24. https://doi.org/10.1136/gutjnl-2011-300783.
Niu B, Liu J, Lv B, Lin J, Li X, Wu C, Jiang X, Zeng Z, Zhang XK, Zhou H. Interplay between transforming growth factor-beta and Nur77 in dual regulations of inhibitor of differentiation 1 for colonic tumorigenesis. Nat Commun. 2021;12:2809. https://doi.org/10.1038/s41467-021-23048-5.
Sun Z, Cao X, Jiang MM, Qiu Y, Zhou H, Chen L, Qin B, Wu H, Jiang F, Chen J, et al. Inhibition of beta-catenin signaling by nongenomic action of orphan nuclear receptor Nur77. Oncogene. 2012;31:2653–67. https://doi.org/10.1038/onc.2011.448.
Wilson AJ, Arango D, Mariadason JM, Heerdt BG, Augenlicht LH. TR3/Nur77 in colon cancer cell apoptosis. Cancer Res. 2003;63:5401–7.
Messmer K, Remington MP, Skidmore F, Fishman PS. Induction of tyrosine hydroxylase expression by the transcription factor Pitx3. Int J Dev Neurosci. 2007;25:29–37. https://doi.org/10.1016/j.ijdevneu.2006.11.003.
Grimm SL, Hartig SM, Edwards DP. Progesterone Receptor Signaling Mechanisms. J Mol Biol. 2016;428:3831–49. https://doi.org/10.1016/j.jmb.2016.06.020.
Sriraman V, Rudd MD, Lohmann SM, Mulders SM, Richards JS. Cyclic guanosine 5′-monophosphate-dependent protein kinase II is induced by luteinizing hormone and progesterone receptor-dependent mechanisms in granulosa cells and cumulus oocyte complexes of ovulating follicles. Mol Endocrinol. 2006;20:348–61. https://doi.org/10.1210/me.2005-0317.
Mirza AZ, Althagafi II, Shamshad H. Role of PPAR receptor in different diseases and their ligands: physiological importance and clinical implications. Eur J Med Chem. 2019;166:502–13.
Wagner N, Wagner KD. The role of PPARs in disease. Cells. 2020. https://doi.org/10.3390/cells9112367.
Wang Y, Nakajima T, Gonzalez FJ, Tanaka N. PPARs as metabolic regulators in the liver: lessons from liver-specific PPAR-null mice. Int J Mol Sci. 2020. https://doi.org/10.3390/ijms21062061.
Strosznajder AK, Wójtowicz S, Jeżyna MJ, Sun GY, Strosznajder JB. Recent insights on the role of PPAR-β/δ in neuroinflammation and neurodegeneration, and its potential target for therapy. NeuroMol Med. 2021;23:86–98.
Wagner N, Wagner K-D. PPAR beta/delta and the hallmarks of cancer. Cells. 2020;9:1133.
Bonofiglio D, Cione E, Qi H, Pingitore A, Perri M, Catalano S, Vizza D, Panno ML, Genchi G, Fuqua SA, et al. Combined low doses of PPARgamma and RXR ligands trigger an intrinsic apoptotic pathway in human breast cancer cells. Am J Pathol. 2009;175:1270–80. https://doi.org/10.2353/ajpath.2009.081078.
Garcia-Bates TM, Bernstein SH, Phipps RP. Peroxisome proliferator-activated receptor gamma overexpression suppresses growth and induces apoptosis in human multiple myeloma cells. Clin Cancer Res. 2008;14:6414–25. https://doi.org/10.1158/1078-0432.CCR-08-0457.
Youssef J, Badr M. Peroxisome proliferator-activated receptors and cancer: challenges and opportunities. Br J Pharmacol. 2011;164:68–82. https://doi.org/10.1111/j.1476-5381.2011.01383.x.
Sarraf P, Mueller E, Jones D, King FJ, DeAngelo DJ, Partridge JB, Holden SA, Chen LB, Singer S, Fletcher C. Differentiation and reversal of malignant changes in colon cancer through PPARγ. Nat Med. 1998;4:1046–52.
Smallridge RC, Copland JA, Brose MS, Wadsworth JT, Houvras Y, Menefee ME, Bible KC, Shah MH, Gramza AW, Klopper JP, et al. Efatutazone, an oral PPAR-gamma agonist, in combination with paclitaxel in anaplastic thyroid cancer: results of a multicenter phase 1 trial. J Clin Endocrinol Metab. 2013;98:2392–400. https://doi.org/10.1210/jc.2013-1106.
Pishvaian MJ, Marshall JL, Wagner AJ, Hwang JJ, Malik S, Cotarla I, Deeken JF, He AR, Daniel H, Halim AB, et al. A phase 1 study of efatutazone, an oral peroxisome proliferator-activated receptor gamma agonist, administered to patients with advanced malignancies. Cancer. 2012;118:5403–13. https://doi.org/10.1002/cncr.27526.
Komatsu Y, Yoshino T, Yamazaki K, Yuki S, Machida N, Sasaki T, Hyodo I, Yachi Y, Onuma H, Ohtsu A. Phase 1 study of efatutazone, a novel oral peroxisome proliferator-activated receptor gamma agonist, in combination with FOLFIRI as second-line therapy in patients with metastatic colorectal cancer. Invest New Drugs. 2014;32:473–80. https://doi.org/10.1007/s10637-013-0056-3.
Xing Y, Yan J, Niu Y. PXR: a center of transcriptional regulation in cancer. Acta Pharmaceutica Sinica B. 2020;10:197–206.
Chen Y, Tang Y, Guo C, Wang J, Boral D, Nie D. Nuclear receptors in the multidrug resistance through the regulation of drug-metabolizing enzymes and drug transporters. Biochem Pharmacol. 2012;83:1112–26. https://doi.org/10.1016/j.bcp.2012.01.030.
Skandalaki A, Sarantis P, Theocharis S. Pregnane X receptor (PXR) polymorphisms and cancer treatment. Biomolecules. 2021;11:1142.
Garcia P, Lorenzo P, de Lera AR. Natural ligands of RXR receptors. Methods Enzymol. 2020;637:209–34. https://doi.org/10.1016/bs.mie.2020.02.006.
Wagner CE, Jurutka PW, Marshall PA, Heck MC. Retinoid X receptor selective agonists and their synthetic methods. Curr Top Med Chem. 2017;17:742–67. https://doi.org/10.2174/1568026616666160617091559.
Wang W, Zhao M, Cui L, Ren Y, Zhang J, Chen J, Jia L, Zhang J, Yang J, Chen G, et al. Characterization of a novel HDAC/RXR/HtrA1 signaling axis as a novel target to overcome cisplatin resistance in human non-small cell lung cancer. Mol Cancer. 2020;19:134. https://doi.org/10.1186/s12943-020-01256-9.
Anyetei-Anum CS, Roggero VR, Allison LA. Thyroid hormone receptor localization in target tissues. J Endocrinol. 2018;237:R19–34. https://doi.org/10.1530/JOE-17-0708.
Zhang ZZ, Chen Q, Kong CY, Li ZM, Wang LS. Circulating thyroid stimulating hormone receptor messenger RNA and differentiated thyroid cancer: a diagnostic meta-analysis. Oncotarget. 2017;8:6623–9. https://doi.org/10.18632/oncotarget.14251.
Yang YSH, Ko PJ, Pan YS, Lin HY, Whang-Peng J, Davis PJ, Wang K. Role of thyroid hormone-integrin alphavbeta3-signal and therapeutic strategies in colorectal cancers. J Biomed Sci. 2021;28:24. https://doi.org/10.1186/s12929-021-00719-5.
Diaz Flaque MC, Cayrol MF, Sterle HA, Del Rosario Aschero M, Diaz Albuja JA, Isse B, Farias RN, Cerchietti L, Rosemblit C, Cremaschi GA. Thyroid hormones induce doxorubicin chemosensitivity through enzymes involved in chemotherapy metabolism in lymphoma T cells. Oncotarget. 2019;10:3051–65. https://doi.org/10.18632/oncotarget.26890.
Kato S. The function of vitamin D receptor in vitamin D action. J Biochem. 2000;127:717–22. https://doi.org/10.1093/oxfordjournals.jbchem.a022662.
Gnagnarella P, Raimondi S, Aristarco V, Johansson HA, Bellerba F, Corso F, Gandini S. Vitamin D receptor polymorphisms and cancer. Adv Exp Med Biol. 2020;1268:53–114. https://doi.org/10.1007/978-3-030-46227-7_4.
Fathi N, Ahmadian E, Shahi S, Roshangar L, Khan H, Kouhsoltani M, Dizaj SM, Sharifi S. Role of vitamin D and vitamin D receptor (VDR) in oral cancer. Biomed Pharmacother. 2019;109:391–401.
Jeon S-M, Shin E. Exploring vitamin D metabolism and function in cancer. Exp Mol Med. 2018;50:1–14.
Dou R, Ng K, Giovannucci EL, Manson JE, Qian ZR, Ogino S. Vitamin D and colorectal cancer: molecular, epidemiological and clinical evidence. Br J Nutr. 2016;115:1643–60. https://doi.org/10.1017/S0007114516000696.
Wang H, Wang X, Xu L, Zhang J, Cao H. A molecular sub-cluster of colon cancer cells with low VDR expression is sensitive to chemotherapy, BRAF inhibitors and PI3K-mTOR inhibitors treatment. Aging (Albany NY). 2019;11:8587–603. https://doi.org/10.18632/aging.102349.
Ferrer-Mayorga G, Larriba MJ, Crespo P, Munoz A. Mechanisms of action of vitamin D in colon cancer. J Steroid Biochem Mol Biol. 2019;185:1–6. https://doi.org/10.1016/j.jsbmb.2018.07.002.
Carlberg C, Munoz A. An update on vitamin D signaling and cancer. Semin Cancer Biol. 2022;79:217–30. https://doi.org/10.1016/j.semcancer.2020.05.018.
Acknowledgements
The figures were created in BioRender.com. The authors acknowledgement the use of AI for improving language and readablity.
Funding
This work was supported by the BT/556/NE/U-Excel/2016 grant awarded to Prof. Ajaikumar B. Kunnumakkara by Department of Biotechnology (DBT), Government of India. Alan Prem Kumar was supported by grant from the Singapore Ministry of Education (MOE-T2EP30120-0016). The authors extend their appreciation to the Deanship of Scientific Research at King Khalid University (KKU) for funding this work through the Research Group Program Under the Grant Number:(R.G.P.2/555/44). Aviral Kumar acknowledges Prime Minister’s Research Fellowship (PMRF) program, Ministry of Education (MOE), Govt. of India for providing him the fellowship. Elena Okina is supported by the Singapore Ministry of Education Postdoctoral Fellowship. Huiyan Eng is supported by the Singapore National Research Foundation Resilience & Growth Postdoctoral Fellowship.
Author information
Authors and Affiliations
Contributions
MKM: Writing—original draft preparation, investigation, visualization, figure and table preparation; SJ: Writing—review & editing, figure preparation; SG: Writing—review & editing, figure preparation; AK: Writing—review & editing; figure preparation; HYL: Writing-review & editing; EO: Writing-review & editing; HE: Editing; MSA: Writing review & editing; MA: Writing review & editing; GS: Overall editing; APK: Contributed to the conceptualization, funding, overall supervision, supported review development and overall editing; ABK: Contributed to the conceptualization, funding, overall supervision, supported review development and overall editing.
Corresponding authors
Ethics declarations
Competing interests
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Manickasamy, M.K., Jayaprakash, S., Girisa, S. et al. Delineating the role of nuclear receptors in colorectal cancer, a focused review. Discov Onc 15, 41 (2024). https://doi.org/10.1007/s12672-023-00808-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s12672-023-00808-x