
Abstract
Introduction
To evaluate the cost-effectiveness of the co-formulation insulin degludec/insulin aspart (IDegAsp) versus biphasic insulin aspart (BIAsp 30), both administered twice daily, in patients with type 2 diabetes mellitus (T2DM), using a short-term cost-effectiveness model.
Methods
Data from two phase 3a treat-to-target clinical trials were used to populate a simple and transparent short-term cost-effectiveness model. The costs and effects of treatment with IDegAsp versus BIAsp 30 were calculated over a 5-year period, from a Danish health-care cost perspective. One-way and probabilistic sensitivity analyses were conducted to assess the degree of uncertainty and robustness of the results.
Results
The base-case incremental cost-effectiveness ratio (ICER) of 81,507.91 Danish Kroner (DKK) per quality-adjusted life year (QALY) demonstrates that IDegAsp is a cost-effective treatment compared with BIAsp 30, over a 5-year time horizon. One-way sensitivity analyses show that the ICERs remain within an acceptable range when the rates of hypoglycemia, unit cost of hypoglycemia, disutilities of hypoglycemic events, and the time horizon are varied, ranging from 71,012 DKK to 209,446 DKK. The probabilistic sensitivity analysis demonstrates that the probability that IDegAsp is cost-effective relative to BIAsp 30 is 99.50%, assuming a cost-effectiveness threshold of 250,000 DKK per QALY.
Conclusion
This short-term cost-effectiveness model shows that IDegAsp is a cost-effective treatment compared with BIAsp 30 for patients with T2DM. This result is primarily driven by significant reductions in severe hypoglycemia and insulin dose observed with IDegAsp versus BIAsp 30. Sensitivity analyses demonstrate the robustness of these results.
Funding
Novo Nordisk A/S, Søborg, Denmark.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Due to the progressive nature of type 2 diabetes mellitus (T2DM), patients usually require treatment intensification to maintain glycemic control, eventually resulting in insulin therapy [1]. After treatment failure on basal insulin, guidelines recommend intensification with either a glucagon-like peptide-1 receptor agonist (GLP-1RA) or mealtime (bolus) insulin [1]. Premixed insulin can offer a convenient alternative to basal-bolus therapy, controlling both fasting and postprandial glucose with fewer injections. However, premixed insulin requires resuspension, and insufficient mixing can result in incorrect dosing [2].
Insulin degludec/insulin aspart (IDegAsp) is the first soluble co-formulation of a basal and a rapid-acting insulin analog in a single injection. The unique properties of insulin degludec (IDeg) enable combination with the rapid-acting insulin, insulin aspart [3]. IDeg has a long duration of action, with a longer half-life and less within-patient variability versus insulin glargine [4, 5]. The IDegAsp soluble co-formulation has the additional advantage that it does not require resuspension, eliminating the risk of incomplete mixing, which can lead to hypoglycemia [6].
The efficacy and safety of IDegAsp was investigated in a phase 3 clinical program (BOOST). A combined analysis of two trials [7, 8] comparing IDegAsp twice daily (BID) with biphasic insulin aspart (BIAsp 30) BID in insulin-experienced patients with T2DM showed that, at similar levels of glycemic control, IDegAsp resulted in a lower fasting plasma glucose (PG), lower rate of overall and nocturnal hypoglycemia and less weight gain compared with BIAsp 30, all at a lower insulin dose [9].
To optimize the use of health-care resources, the decision to prescribe a particular product is dependent on clinical and economic evidence. Therefore, it is important that the cost-effectiveness of diabetes interventions is investigated. The cost-effectiveness analyses of diabetes interventions have historically been conducted by estimating the long-term clinical consequences as a function of differences in HbA1c. However, according to the US Food and Drug Administration guidance, new insulins should be compared with a standard insulin (and not placebo or a non-insulin agent), aiming to achieve similar glycemic control, thus allowing the comparison of safety end points, such as hypoglycemia, body weight, and insulin dose [10, 11]. This approach is known as ‘treat-to-target’. It follows that there are no differences in long-term risk parameters related to HbA1c, and a short-term cost-effectiveness model is more appropriate for an economic evaluation of these secondary end points than a long-term model. Such a model has been used to compare treatment with IDeg versus insulin glargine in patients with type 1 diabetes mellitus (T1DM) and T2DM, from Swedish and UK health-care perspectives [12–14].
The objective of this study was to evaluate the cost-effectiveness of IDegAsp BID compared to BIAsp30 BID in patients with T2DM, from a Danish health-care cost perspective, using a short-term cost-effectiveness model.
Methods
Model Overview
Cost-effectiveness analyses combine the incremental cost of an intervention with the incremental health benefit it produces. A cost-effectiveness analysis of IDegAsp BID compared with BIAsp 30 BID in patients with T2DM was conducted, with the benefits measured in quality-adjusted life years (QALYs), a generic measure of health in terms of quantity and quality of life. The main outcome of the cost-effectiveness analysis was the incremental cost-effectiveness ratio (ICER), which is the most commonly used method by health technology assessment bodies across Europe [15–17].
The cost-effectiveness of IDegAsp was analyzed over a 5-year time horizon, a duration considered sufficient to capture the impact of titration and maintenance of treatment, and a discount rate of 3% for costs and effects was applied, as per the recommendations of the Danish Medicines Agency [17].
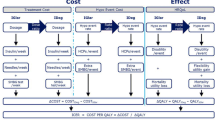
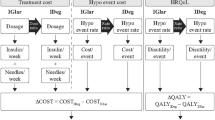
A simple and transparent short-term model was developed in Microsoft Excel 2010 (Fig. 1). Costs included insulin and the direct costs associated with hypoglycemic events. QALYs were calculated by applying a disutility per hypoglycemic event, per self-measured blood glucose (SMBG) test, and a disutility associated with weight gain.

Structure of the cost-effectiveness model. The model captured treatment costs (including insulin, needles, and costs associated with SMBG testing) and costs associated with hypoglycemic events (the resource used to treat the event multiplied by the hypoglycemic event rate) for both IDegAsp and comparator. QALYs were calculated by applying disutilities (reduction in HRQoL) per hypoglycemic event, SMBG test, and BMI gain. BIAsp 30 biphasic insulin aspart, BMI body mass index, HC health care, HRQoL health-related quality of life, ICER incremental cost-effectiveness ratio, IDegAsp insulin degludec/insulin aspart, QALY quality-adjusted life year, SMBG self-measured blood glucose
The cost-effectiveness analysis was based on a cohort approach to mimic the treatment of a patient starting on either IDegAsp BID or BIAsp 30 BID and continuing treatment for 5 years. Data from clinical trials of 26 weeks’ duration were used to predict the outcomes over the 5 years. The titration period is up to week 16 and the maintenance period is 16 weeks onward, when patients have usually reached a state of maintenance, with regard to insulin dose and glycemic control. The maintenance period was extended beyond the clinical trial duration, i.e., hypoglycemic rate ratios from the maintenance period were assumed to last for the remaining modeling period. Furthermore, end-of-trial doses and body mass index (BMI) were assumed to last for the remaining modeling period.
Patient Population
Data included in this model consisted of a combined analysis of two randomized, open label, treat-to-target, multinational, 26-week trials conducted in insulin-experienced patients with T2DM, both comparing IDegAsp BID with BIAsp 30 BID [9]. The trials were conducted in accordance with ethical guidelines [7, 8], and this study did not involve any new studies of human or animal subjects performed by any of the authors. The global trial (Intensify Premix 1; ClinicalTrials.gov identifier: NCT01009580) included patients from ten countries (including four European countries: Denmark, Finland, Poland, and Sweden) randomized 1:1 to IDegAsp or BIAsp 30, with T2DM for ≥6 months, ≥18 years of age, HbA1c of 7.0–10.0%, and BMI ≤40 kg/m2 who were previously treated with premixed insulin ± oral anti-diabetic drugs (OADs) for ≥3 months [7]. The second trial (Intensify All; ClinicalTrials.gov identifier: NCT01059812) was a pan-Asian study involving patients from five countries randomized 2:1 to IDegAsp or BIAsp 30, with T2DM for ≥6 months, ≥18 years of age (≥20 years for Japan and Taiwan), HbA1c of 7.0–10.0%, and BMI ≤35 kg/m2, who were previously treated with basal, premixed, or self-mixed insulin ± metformin for ≥3 months [8]. The trial designs were similar, and the patient characteristics are summarized in the primary publications [7, 8]. In total, 868 patients were included (IDegAsp n = 504; BIAsp 30 n = 364). Insulin was titrated weekly to a pre-meal SMBG target of 4.0–5.0 mmol/L. Patients with significant concomitant illness [e.g., history of cardiovascular disease (heart failure: New York Heart Association class III or IV, unstable angina pectoris, or a myocardial infarction) within 6 months preceding the trial and uncontrolled severe hypertension (systolic blood pressure ≥180 mmHg or sitting diastolic blood pressure ≥100 mmHg)] and those with recurrent severe hypoglycemia or hypoglycemic unawareness were excluded.
Data Used in the Model
Clinical Data
Insulin Dose
Daily insulin dose in units (U) was captured during the clinical trials. In this combined analysis, the BIAsp 30 dose was 45.7 U/day at baseline, 81.8 U/day at the end of titration, and 86.2 U/day at the end of the trial (Table 1a). The dose ratios (IDegAsp/IAsp 30) were 0.84 at both the end of titration and end of trial in the combined analysis and assumed to be 1 at baseline (Table 1a). The BIAsp 30 dose and the IDegAsp/BIAsp 30 dose ratio were applied to estimate the IDegAsp dose (Table 1a) to allow for adjustment of the covariates treatment, trial, anti-diabetic therapy at screening, sex, age, region, and baseline insulin dose.
Hypoglycemia Rates
Baseline values for severe and non-severe hypoglycemia were based on the UK Hypoglycaemia Study Group (UKHSG) observational study [18]. The rates represent a better estimation of real-life rates compared with data from clinical trials, where a bias in patient selection and treatment setting occurs, resulting in potentially lower rates of hypoglycemia due to the exclusion of patients with recurrent severe hypoglycemia or hypoglycemic unawareness [19–25]. The T2DM group which used insulin for more than 5 years was perceived as being representative of the population who would consider using IDegAsp. The rates of hypoglycemia reported were 10.2 and 0.7 events per patient year of exposure (PYE) for non-severe and severe hypoglycemia, respectively [18]. These estimates were taken as the base case for the comparator BIAsp 30 group (Table 1b). To estimate the corresponding hypoglycemic event rates for IDegAsp, the relative rate ratio of hypoglycemia derived from the combined analysis was applied (Table 1b). Hypoglycemic event rates were analyzed in mutually exclusive groups to avoid double counting of events: i.e., severe events, non-severe events occurring during the day (diurnal), and non-severe events occurring during the night (nocturnal). During the trials, hypoglycemia was classified as severe (requiring assistance from another person) or confirmed (PG measurement of <3.1 mmol/L or severe). Nocturnal confirmed hypoglycemia included confirmed episodes with time of onset from 00:01 h to 05:59 h.
BMI
In the combined analysis, there was less weight gain with IDegAsp versus BIAsp 30 [9]. A post hoc analysis calculated the change in BMI from baseline for BIAsp 30. Using the estimated difference (IDegAsp−BIAsp30) derived from the combined analysis, the corresponding change from baseline in BMI for IDegAsp was calculated, adjusting for the covariates treatment, trial, anti-diabetic therapy at screening, sex, age, region, and baseline BMI (Table 1c).
SMBG Testing
The titration schedule recommended for use of SMBG tests with BIAsp 30 (six SMBG tests per week) was applied in the cost-effectiveness model [26]. For IDegAsp, the once-weekly titration schedule for twice-daily administration was applied in the cost-effectiveness model (six SMBG tests per week) [7, 8].
Cost Data
All costs are calculated in Danish Kroner (DKK) (1 GBP = 9.4464 DKK,13 May 2016).
Cost of Insulin, Needles, and SMBG Tests
The cost of insulin was based on prices published by the Danish Medicines Agency [27] and the cost of needles, SMBG test strips, and lancets were based on prices published by the wholesaler Nomeco (Copenhagen, Denmark) [28] (Table 2).
Cost of Hypoglycemic Events
The direct costs associated with a single hypoglycemic event represent the sum of the cost of treating the hypoglycemic event itself plus the costs of additional SMBG tests in the week following the event (Table 3). The cost per event was multiplied by the annual rate of hypoglycemia to obtain an annual cost per insulin-treated patient.
The proportion of patients contacting a health-care professional (HCP) was obtained from the clinical trials, where patients completed a questionnaire regarding non-severe hypoglycemia events. To obtain information on the resource use associated with severe hypoglycemia, an analysis was conducted on all severe hypoglycemic events in the IDeg and IDegAsp clinical trial program. Of the 95 severe hypoglycemic events in patients with T2DM on multiple daily injection regimens, 25.3% required an ambulance or an on-site emergency team, 23.2% a hospital stay of ≤24 h, and 5.3% a hospital stay of >24 h (Table 3) [29].
The use of extra SMBG tests in the week following a non-severe event was also based on a questionnaire from the clinical trials. A mean of 2.15 additional SMBG tests were used following a non-severe event in the combined analysis. This appears conservative compared with an observational study across four countries (USA, UK, Germany, and France) with an average of 5.6 additional SMBG tests per non-severe hypoglycemic event [30], and a study that reported an increase of 3.7 SMBG tests per event in Denmark [31]. It was conservatively assumed that this testing pattern was similar for severe events as the extra SMBG tests following hypoglycemic events were collected for the non-severe events only in the clinical trials.
Utility Data
The effects that were incorporated in the model were the disutility (reduction in quality of life) associated with hypoglycemia [32], weight gain (measured as BMI) [33], and frequency of SMBG testing [34]. The multiplication of utilities and life years then provided QALYs.
Disutility per Hypoglycemic Event
Published disutility values, obtained using the well-established time trade-off (TTO) methodology, were used. Utility values were obtained using a Web-based survey asking respondents hypothetical questions to elicit the health-related quality of life impact of living with various frequencies of hypoglycemic events [32]. Disutility values were 0.057 for a severe event and 0.004 and 0.007 for non-severe daytime and non-severe nocturnal hypoglycemic events, respectively [32]. There was a significant difference in disutility associated with non-severe daytime and non-severe nocturnal hypoglycemia [32]. To investigate the incremental impact of IDegAsp, the disutility per hypoglycemic event was multiplied by the event rate per year. This was estimated separately for severe, non-severe daytime, and non-severe nocturnal hypoglycemic events.
Disutility of SMBG testing
The disutility (pain and discomfort) associated with SMBG testing was also investigated using a TTO survey, giving a disutility per additional SMBG of 0.0000221 [34], which was multiplied by the number of SMBG tests per year.
Disutility Associated with Higher BMI
A multinational survey utilizing the EQ-5D questionnaire to measure the impact of diabetes complications, including BMI, calculated a disutility value of 0.0061 per BMI unit above 25 kg/m2 [33].
Sensitivity Analyses
One-Way Sensitivity Analyses
To assess the robustness of these data and the impact of varying key assumptions and outcomes used in the base case on the cost-effectiveness results, several one-way sensitivity analyses were conducted (Table S1 in the supplementary material).
The base-case time horizon was 5 years, so the effects of time horizons of 1, 2, 3, and 10 years were investigated. Sensitivity analyses with discount rates of 0% and 5% were applied to investigate the effect of discounting.
Hypoglycemia event rates for Denmark from a recent multinational observational study were included as a sensitivity analysis, which reported severe, non-severe daytime, and nocturnal rates of 0.3, 13.6, and 8.3 events per PYE, respectively, for insulin-treated patients (classified as T2DM ‘other’ which included mixed insulins comparable to the present study) [35, 36].
The observed hypoglycemia clinical trial event rates per PYE from the combined analysis were also applied as a sensitivity analysis: 9.61 and 10.50 for non-severe daytime events during the titration and maintenance periods, respectively; 1.96 and 2.30 for non-severe nocturnal events during the titration and maintenance periods, respectively; and 0.13 and 0.23 for severe events during the titration and maintenance periods, respectively.
The costs of severe hypoglycemia were increased or decreased by 20% from the base case.
The estimated BMI difference (IDegAsp−BIAsp30) derived from the combined analysis was assumed to be zero in a sensitivity analysis.
Instead of the base-case TTO values [32], disutility values of 0.0036 and 0.0118 per non-severe and severe hypoglycemic event, respectively, were obtained from a UK-based study of patients with diabetes [37, 38].
Clinical results from the IDegAsp global trial, which included European patients [7], were used in a sensitivity analysis, as it could potentially be considered more representative for a Danish setting.
Instead of the SMBG disutility derived from the TTO study used for the base case, a disutility of zero associated with SMBG testing was assumed in a sensitivity analysis.
The disutility associated with BMI was assumed to be zero in a sensitivity analysis.
Probabilistic Sensitivity Analysis
A probabilistic sensitivity analysis (PSA) was conducted to capture the impact of statistical uncertainty accounting for the stochastic uncertainty in the input parameters used in the model. In a PSA, all stochastic input parameters can be varied simultaneously within a plausible range given statistical distributions for the input parameters in the model. Standard errors for the parameters were used and a log-normal distribution for rate ratios and normal distributions around continuous variables were used (Table S2 in the supplementary material). The PSA allows for an estimate of the certainty that a given intervention is cost-effective at different cost-effectiveness thresholds to be evaluated. The PSA were repeated with 10,000 iterations.
Compliance with Ethics Guidelines
This article is based on previously conducted studies and does not involve any new studies of human or animal subjects performed by any of the authors.
Results
This analysis shows that IDegAsp is a cost-effective treatment option compared with BIAsp 30 in patients with T2DM. The estimated ICER in the base-case analysis was 81,507.91 DKK (Table 4).
The total incremental discounted cost per patient over 5 years of IDegAsp compared to BIAsp 30 treatment was 18,125.94 DKK, mainly due to an increased insulin cost (Table 4). A lower incremental cost of treating non-severe and severe hypoglycemia was observed (Table 4), due primarily to the statistically significant reduction in hypoglycemic events in the maintenance period with IDegAsp versus BIAsp 30 in the combined analysis (Table 1).
One-Way Sensitivity Analyses
In all sensitivity analyses, ICERs were below normally accepted thresholds, with estimates ranging from 71,012 DKK to 209,446 DKK per QALY gained (Table S1). Varying the time horizon had a small impact on the ICER, with a lower cost per QALY gained with a 10 year time horizon. Similarly, changing the discount rate did not have a significant impact on the ICER. The rate of hypoglycemia applied to the model had a larger impact on the results, with the higher published rates from Denmark [35, 36] resulting in a lower ICER (71,012 DKK) compared to the base case.
Using the observed hypoglycemia event rates from the combined analysis, where fewer severe hypoglycemic events were observed than in the UKHSG study, IDegAsp was cost-effective with an ICER of 153,440 DKK per QALY gained. When the cost of hypoglycemia was increased or decreased by 20%, IDegAsp was still cost-effective versus BIAsp 30, with ICERs of 76,049 DKK and 86,968 DKK, respectively. Using the disutilities per hypoglycemic event published by Currie et al. [37] resulted in an ICER of 209,446 DKK. Using the clinical data from the global trial instead of the combined analysis resulted in an ICER of 100,289 DKK [7]. Assuming a disutility per SMBG test of 0 did not have a significant impact on the ICER, compared with the base case.
Probabilistic Sensitivity Analysis
The PSA input variables are outlined in Table S2 in the supplementary material. At a willingness-to-pay threshold of 250,000 DKK per QALY gained, the probability that IDegAsp was cost-effective relative to BIAsp 30 was 99.5% (Fig. S1 in the supplementary material).
Discussion
Due to limited health-care resources, demonstrating the value of new therapies is an essential part of clinical and economical decision making. This simple and transparent short-term cost-effectiveness model, conducted from a Danish health-care perspective, focuses on the impact of important aspects of insulin therapy, including hypoglycemia and dosing. For patients with T2DM, IDegAsp is a cost-effective treatment compared with BIAsp 30, with an ICER of 81,507.91 DKK, over a 5-year time horizon. Several one-way sensitivity analyses and a PSA also found that IDegAsp was cost-effective versus BIAsp 30, supporting the robustness of the analysis. The ICERs were stable when the rates of hypoglycemia, unit cost of hypoglycemia, and the disutility of a hypoglycemic event were varied, ranging from 71,012 DKK to 209,446 DKK, all cost-effective based on a threshold of 250,000 DKK. In Denmark, there is no official published cost-effectiveness threshold. However, two recent Danish cost-effectiveness studies have applied thresholds varying from 250,000 to 500,000 DKK per QALY, with the one in the field of diabetes applying a threshold of 250,000 DKK [39, 40].
The two-trial combined analysis was used in the base-case model to increase the sample size and thereby strengthen the certainty of the parameter estimates derived from individual trials. Previously, a pre-specified hypoglycemia meta-analysis using pooled data from seven trials in the IDeg clinical program was conducted [41]. The combined analysis used here was not pre-specified; however, it was conducted using the same methodology as the IDeg meta-analysis [41] the hypoglycemia classification described in a second IDeg meta-analysis [42].
The combined analysis showed that, at similar HbA1c levels, IDegAsp resulted in lower rates of overall and nocturnal confirmed hypoglycemia, particularly during the maintenance period, and less weight gain compared with BIAsp 30, while using a lower dose [9]. Although hypoglycemia is not a problem for all insulin-treated patients, its frequency tends to increase with longer disease duration and more intensive insulin regimens [23]. Additionally, treatment of hypoglycemia is associated with considerable resource use and cost and is a burden to patients [29, 43, 44]. In this analysis, the difference in the rates of hypoglycemia had a noticeable impact on the ICER. In this model, the mean population rates of hypoglycemia from published studies were used in the base case and sensitivity analysis [18, 35, 36] to more closely reflect the rates observed in routine clinical practice versus clinical trials (where patients at high risk of severe hypoglycemia are excluded). The UKHSG rates used in the base-case analysis [18] were a conservative estimate compared with the rates in a Danish population used for a sensitivity analysis, where the rates of non-severe daytime and nocturnal hypoglycemia were higher [35, 36]. Hypoglycemia disutilities from a global (US, UK, Germany, Sweden) TTO study were applied to the base-case model [32] and those from a UK setting in a sensitivity analysis [37]. Therefore, in subpopulations of patients, who experience recurrent hypoglycemia, hypoglycemia unawareness, or nocturnal hypoglycemia, a treatment such as IDegAsp might provide additional value for money as compared to the base case. The lower dose required for equivalent glycemic control for IDegAsp compared to BIAsp 30 in the combined analysis contributed to the cost-effectiveness of IDegAsp. The lower weight gain (measured by BMI) only had a limited impact on the cost-effectiveness results.
All modeling approaches are critically influenced by the quality of the input parameters. This model only used parameter estimates for which a statistically significant difference between the treatment arms was documented and assumed that all other differences were due to random variation. This cost-effectiveness model is limited by a variety of factors. The clinical data are derived from post hoc analyses of two clinical trials. The generalizability of clinical trials with high internal validity but usually low external validity, due to the highly selected population, which may not be representative of a real world clinical practice setting, is a common limitation inherent to economic modeling. The model assumed patients continued treatment with IDegAsp and BIAsp 30 for the 5-year period, without changing to another insulin regimen. As the data are based on treat-to-target clinical trials with no differences in HbA1c, any differences in mortality and morbidity are not expected and so not included in the model.
As with most models, the cost data for hypoglycemia were collected from a variety of publicly available sources, which measure parameters differently and may not accurately reflect the economic burden of hypoglycemia. The resources used following a hypoglycemia event were collected during the clinical trials for a selected population and may not represent the burden seen in clinical practice. The actual costs of hypoglycemia may be higher as the estimations did not take into consideration out-of-pocket expenses or lost work productivity. Finally, the model is based on comparable glycemic control between IDegAsp and BIAsp 30, with a potentially lower insulin dose requirement with IDegAsp. To address some of these limitations, more extensive clinical practice experience with IDegAsp would be useful for further health economic evaluations.
Conclusions
In conclusion, IDegAsp is a cost-effective alternative to BIAsp 30 for the treatment of T2DM in Denmark, based on the base case and sensitivity analyses with this short-term cost-effectiveness model.
References
Inzucchi SE, Bergenstal RM, Buse JB, et al. Management of hyperglycaemia in type 2 diabetes, 2015: a patient-centred approach. Update to a Position Statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetologia. 2015;58:429–42.
Brown A, Steel JM, Duncan C, Duncan A, McBain AM. An assessment of the adequacy of suspension of insulin in pen injectors. Diabet Med. 2004;21:604–8.
Havelund S, Ribel U, Hubalek F, Hoeg-Jensen T, Wahlund PO, Jonassen I. Investigation of the physico-chemical properties that enable co-formulation of basal insulin degludec with fast-acting insulin aspart. Pharm Res. 2015;32:2250–8.
Heise T, Hermanski L, Nosek L, Feldman A, Rasmussen S, Haahr H. Insulin degludec: four times lower pharmacodynamic variability than insulin glargine under steady-state conditions in type 1 diabetes. Diabetes Obes Metab. 2012;14:859–64.
Heise T, Nosek L, Bottcher SG, Hastrup H, Haahr H. Ultra-long-acting insulin degludec has a flat and stable glucose-lowering effect in type 2 diabetes. Diabetes Obes Metab. 2012;14:944–50.
Kaiser P, Maxeiner S, Weise A, et al. Assessment of the mixing efficiency of neutral protamine Hagedorn cartridges. J Diabetes Sci Technol. 2010;4:652–7.
Fulcher GR, Christiansen JS, Bantwal G, et al. Comparison of insulin degludec/insulin aspart and biphasic insulin aspart 30 in uncontrolled, insulin-treated type 2 diabetes: a phase 3a, randomized, treat-to-target trial. Diabetes Care. 2014;37:2084–90.
Kaneko S, Chow F, Choi DS, et al. Insulin degludec/insulin aspart versus biphasic insulin aspart 30 in Asian patients with type 2 diabetes inadequately controlled on basal or pre-/self-mixed insulin: a 26-week, randomised, treat-to-target trial. Diabetes Res Clin Pract. 2015;107:139–47.
Christiansen JS, Niskanen L, Rasmussen S, Johansen T, Fulcher G. Lower rates of hypoglycemia during maintenance treatment with IDegAsp versus BIAsp 30: a combined analysis of two phase 3a studies in type 2 diabetes. J Diabetes. 2016. doi:10.1111/1753-0407.12355 [epub ahead of print].
Garber AJ. Treat-to-target trials: uses, interpretation and review of concepts. Diabetes Obes Metab. 2014;16:193–205.
US Department of Health and Human Services, Food and Drug Administration, Center for Drug Evaluation and Research (CDER). Guidance for Industry: Diabetes Mellitus: Developing Drugs and Therapeutic Biologics for Treatment and Prevention (Draft guidance), 2008. 2008. http://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/ucm071624.pdf. Accessed Jan 6, 2016.
Evans M, Wolden M, Gundgaard J, Chubb B, Christensen T. Cost-effectiveness of insulin degludec compared with insulin glargine for patients with type 2 diabetes treated with basal insulin—from the UK health care cost perspective. Diabetes Obes Metab. 2014;16:366–75.
Evans M, Wolden M, Gundgaard J, Chubb B, Christensen T. Cost-effectiveness of insulin degludec compared with insulin glargine in a basal-bolus regimen in patients with type 1 diabetes mellitus in the UK. J Med Econ. 2015;18:56–68.
Ericsson A, Pollock RF, Hunt B, Valentine WJ. Evaluation of the cost-utility of insulin degludec vs insulin glargine in Sweden. J Med Econ. 2013;16:1442–52.
European Network for Health Technology Assessment. Methods for health economic evaluations. 2015. https://eunethta.fedimbo.belgium.be/sites/5026.fedimbo.belgium.be/files/2015-04-29-ECO-GL_Final%20version_0.pdf. Accessed Jan 6, 2016.
National Institute for Health and Clinical Excellence. Methods for the development of NICE public health guidance (third edition). 2012. http://www.nice.org.uk/article/pmg4/resources/non-guidance-methods-for-the-development-of-nice-public-health-guidance-third-edition-pdf. Accessed Jan 6, 2016.
Danish Medicines Agency. Experiences with health economic analyses in applications for general reimbursement for medicinal products. 2004. https://sundhedsstyrelsen.dk/da/medicin/tilskud/generelle-tilskud/ansoegning/sundhedsoekonomiske-analyser/erfaringer-med-sundhedsoekonomiske-analyser-i-ansoegninger-om-generelt-tilskud-til-laegemidler. Accessed Jan 6, 2016.
UK Hypoglycaemia Study Group. Risk of hypoglycaemia in types 1 and 2 diabetes: effects of treatment modalities and their duration. Diabetologia. 2007;50:1140–7.
Elliott L, Fidler C, Ditchfield A, Stissing T. Hypoglycemia event rates: a comparison between real-world data and randomized controlled trial populations in insulin-treated diabetes. Diabetes Ther. 2016;7:45–60.
Henderson JN, Allen KV, Deary IJ, Frier BM. Hypoglycaemia in insulin-treated type 2 diabetes: frequency, symptoms and impaired awareness. Diabet Med. 2003;20:1016–21.
Akram K, Pedersen-Bjergaard U, Borch-Johnsen K, Thorsteinsson B. Frequency and risk factors of severe hypoglycemia in insulin-treated type 2 diabetes: a literature survey. J Diabetes Complicat. 2006;20:402–8.
Gold AE, MacLeod KM, Frier BM. Frequency of severe hypoglycemia in patients with type I diabetes with impaired awareness of hypoglycemia. Diabetes Care. 1994;17:697–703.
Donnelly LA, Morris AD, Frier BM, et al. Frequency and predictors of hypoglycaemia in type 1 and insulin-treated type 2 diabetes: a population-based study. Diabet Med. 2005;22:749–55.
Smith CB, Choudhary P, Pernet A, Hopkins D, Amiel SA. Hypoglycemia unawareness is associated with reduced adherence to therapeutic decisions in patients with type 1 diabetes: evidence from a clinical audit. Diabetes Care. 2009;32:1196–8.
Heller SR. Hypoglycaemia: its pathophysiology in insulin treated diabetes and hypoglycaemia unawareness. Br J Diabetes Vasc Dis. 2011;11:6–9.
Novo Nordisk A/S. NovoMix European Summary of Product Characteristics. 2010. http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/000308/WC500029441.pdf. Accessed Jan 6, 2016.
Danish Medicines Agency. Pricing and Reimbursement. 2016. http://www.medicinpriser.dk. Accessed Feb 18, 2016.
Nomeco. Danish Pharmaceutical Wholesaler. 2016. http://www.nomeco.dk/en. Accessed Feb 18, 2016.
Heller SR, Frier BM, Herslov ML, Gundgaard J, Gough SC. Severe hypoglycaemia in adults with insulin-treated diabetes: impact on healthcare resources. Diabet Med. 2016;33:471–7.
Brod M, Christensen T, Thomsen TL, Bushnell DM. The impact of non-severe hypoglycemic events on work productivity and diabetes management. Value Health. 2011;14:665–71.
Geelhoed-Duijvestijn PH, Pedersen-Bjergaard U, Weitgasser R, Lahtela J, Jensen MM, Ostenson CG. Effects of patient-reported non-severe hypoglycemia on healthcare resource use, work-time loss, and wellbeing in insulin-treated patients with diabetes in seven European countries. J Med Econ. 2013;16:1453–61.
Evans M, Khunti K, Mamdani M, et al. Health-related quality of life associated with daytime and nocturnal hypoglycaemic events: a time trade-off survey in five countries. Health Qual Life Outcomes. 2013;11:90.
Bagust A, Beale S. Modelling EuroQol health-related utility values for diabetic complications from CODE-2 data. Health Econ. 2005;14:217–30.
Evans M, Jensen HH, Bogelund M, Gundgaard J, Chubb B, Khunti K. Flexible insulin dosing improves health-related quality-of-life (HRQoL): a time trade-off survey. J Med Econ. 2013;16:1357–65.
Östenson CG, Geelhoed-Duijvestijn P, Lahtela J, Weitgasser R, Markert JM, Pedersen-Bjergaard U. Self-reported non-severe hypoglycaemic events in Europe. Diabet Med. 2014;31:92–101.
Jensen MM, Pedersen-Bjergaard U. Self-reported frequency and impact of non-severe hypoglycemic events in insulin-treated diabetic patients in Denmark. Diabetes Manag. 2015;5:67–78.
Currie CJ, Morgan CL, Poole CD, Sharplin P, Lammert M, McEwan P. Multivariate models of health-related utility and the fear of hypoglycaemia in people with diabetes. Curr Med Res Opin. 2006;22:1523–34.
Fidler C, Elmelund Christensen T, Gillard S. Hypoglycemia: an overview of fear of hypoglycemia, quality-of-life, and impact on costs. J Med Econ. 2011;14:646–55.
Pedersen-Bjergaard U, Kristensen PL, Nørgaard K, et al. Short-term cost-effectiveness of insulin detemir and insulin aspart in people with type 1 diabetes who are prone to recurrent severe hypoglycemia. Curr Med Res Opin. 2016;20:13–7.
Jönsson L, Borgström F, Zethraeus N. Cost-effectiveness of alendronate in the treatment of osteoporosis in Denmark—an economic evaluation based on the fracture intervention trial. In: SSE/EFI working paper series in economics and finance, No. 501. Stockholm school of economics; 2002.
Ratner R, Gough SC, Mathieu C, et al. Hypoglycaemia risk with insulin degludec compared with insulin glargine in type 2 and type 1 diabetes: a pre-planned meta-analysis of phase 3 trials. Diabetes Obes Metab. 2013;15:175–84.
Vora J, Christensen T, Rana A, Bain SC. Insulin degludec versus insulin glargine in type 1 and type 2 diabetes mellitus: a meta-analysis of endpoints in phase 3a trials. Diabetes Ther. 2014;5:435–46.
Hammer M, Lammert M, Mejias SM, Kern W, Frier BM. Costs of managing severe hypoglycaemia in three European countries. J Med Econ. 2009;12:281–90.
Lundkvist J, Berne C, Bolinder B, Jonsson L. The economic and quality of life impact of hypoglycemia. Eur J Health Econ. 2005;6:197–202.
Dansk Sundhedsinstitut. International sammenligning af akut ambulancetjeneste—en foranalyse vedrørende finansieringsmæssige og økonomiske aspekter. DSI Institut for Sundhedsvæsen, 2003. http://docplayer.dk/1323732-International-sammenligning-af-akut-ambulancetjeneste.html. Accessed Mar 22, 2016.
Statistics Denmark. Consumer Price Index. 2015. http://dst.dk/da/Statistik/emner/forbrugerpriser/forbrugerprisindeks. Accessed Feb 18, 2016.
Danish Health Data Authority. Hospitalisation fees. 2016. http://sundhedsdatastyrelsen.dk/-/media/sds/filer/finansiering-og-afregning/takster/2016/stationaere-drgtakster-2016.xlsx. Accessed Feb 18, 2016.
Danish Health Data Authority. Outpatient services fees. 2016. http://sundhedsdatastyrelsen.dk/-/media/sds/filer/finansiering-og-afregning/takster/2016/ambulante-dags-takster-2016.xlsx. Accessed Feb 18, 2016.
Danish Medical Association. Fee table, daytime. 2016. http://www.laeger.dk/portal/page/portal/LAEGERDK/Laegerdk/P_L_O/Overenskomster/Honorartabel/Honorartabel%2001-10-2015/Honorartabel%2001-10-2015%20dagtid/%C2%A7%2050%20Grundydelser. Accessed Feb 18, 2016.
Acknowledgments
The sponsorship for this study was funded by Novo Nordisk A/S, Søborg, Denmark. Medical writing assistance and editorial/submission support were provided by Adele Buss and Beverly La Ferla of Watermeadow Medical, an Ashfield Company, a part of UDG Healthcare plc, funded by Novo Nordisk A/S. All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this manuscript, take responsibility for the integrity of the work as a whole, and have given final approval for the version to be published. Marc Evans contributed to the study design, interpretation of the results, and to the drafting, revising, and final approval of this manuscript. As corresponding author, Marc Evans agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. Brian Bekker Hansen contributed to the design, conduct/data collection, analysis, and interpretation of the results and to the drafting, revising, and final approval of this manuscript. Jens Gundgaard contributed to the design, conduct/data collection, analysis, and interpretation of the results and to the drafting, revising, and final approval of this manuscript.
Disclosures
Marc Evans has received honoraria as an advisory panel member and speaker for Novo Nordisk, Sanofi, Novartis, and Merck Sharp & Dohme. Brian Bekker Hansen and Jens Gundgaard are employees and shareholders of Novo Nordisk. This study was funded by Novo Nordisk.
Compliance with Ethics Guidelines
This article is based on previously conducted studies and does not involve any new studies of human or animal subjects performed by any of the authors.
Open Access
This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
Author information
Authors and Affiliations
Corresponding author
Additional information
Enhanced content
To view enhanced content for this article go to http://www.medengine.com/Redeem/E295F06048D26213.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0), which permits use, duplication, adaptation, distribution, and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Evans, M., Gundgaard, J. & Hansen, B.B. Cost-Effectiveness of Insulin Degludec/Insulin Aspart Versus Biphasic Insulin Aspart in Patients with Type 2 Diabetes from a Danish Health-Care Perspective. Diabetes Ther 7, 809–823 (2016). https://doi.org/10.1007/s13300-016-0195-6
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13300-016-0195-6