
Abstract
The Tandem t:slim X2 insulin pump is a second-generation automated insulin delivery system with Control-IQ technology. It consists of an X2 insulin pump, an integrated Dexcom sensor, and an embedded ‘Control-IQ’ algorithm, which predicts glucose levels 30 min in the future, adapting the programmed basal insulin rates to get glucose levels between 112.5 and 160 mg/dl (8.9 mmol/l). The system delivers automatic correction boluses of insulin when glucose levels are predicted to rise > 180 mg/dl (10 mmol/l). It has been commercially available since 2016. We reviewed the current evidence about the psychological, safety, and exercise-related outcomes of this device in children, adolescents, and young adults living with type 1 diabetes. We screened 552 papers, but only 21 manuscripts were included in this review. Fear of hypoglycemia is significantly reduced in young people with diabetes and their parents. Interestingly, diabetes-related distress is decreased; thus, the system is well accepted by the users. The sleeping quality of subjects living with diabetes and their caregivers is improved to a lesser extent as well. Despite the small number of data, this system is associated with a low rate of exercise-related hypoglycemia. Finally, evidence from the literature shows that this system is safe and effective in improving psychological personal outcomes. Even if further steps toward the fully closed loop are still mandatory, this second-generation automated insulin delivery system reduces the burden of diabetes. It properly addresses most psychological issues in children, adolescents, and young adults with type 1 diabetes mellitus; thus, it appears to be well accepted.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
The psychosocial needs of youth with diabetes and their families should be addressed appropriately by clinicians for the optimal use of automated insulin delivery systems |
Fear of hypoglycemia is a significant concern for individuals with diabetes and their caregivers |
The Tandem t:slim X2 insulin pump with Control-IQ technology is safe for children, adolescents, and young adults |
The literature shows that this system has beneficial effects on psychological issues, reducing the fear of hypoglycemia and diabetes-related distress and, finally, improving sleep quality to some extent |
Quality of life seems to be slightly improved in patients and caregivers, while the other psychological outcomes seem to be more improved |
Introduction
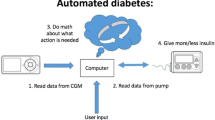
In recent years, technological advancements have provided individuals with type 1 diabetes (T1D) with increasingly high-performing systems that allow for personalized insulin delivery and/or continuous and minimally invasive continuous glucose monitoring (CGM), improving metabolic control and patients’ quality of life (QoL) [1,2,3,4,5,6,7,8]. The most sophisticated systems currently on the market, automated insulin delivery (AID) systems, can modulate basal insulin delivery and administer correction boluses through an insulin pump based on CGM readings without requiring user confirmation. Users are only responsible for reporting carbohydrate intake with meals and their willingness to engage in physical activity [9, 10]. These systems have demonstrated safety and efficacy in randomized controlled clinical trials (RCTs) and real-life studies, increasing time spent within optimal glucose ranges and reducing time spent in hypoglycemia [11, 12]. The Tandem T:slim X2 system with Control-IQ (CIQ) technology (Tandem Diabetes Care, San Diego, CA, USA) comprises the T:slim X2 insulin pump, Dexcom CGM sensor (Dexcom, San Diego, CA, USA), and predictive control algorithm CIQ, approved for use in patients ≥ 6 years old. This algorithm has a module to prevent hypoglycemia safely and automatically provide correction boluses and an overnight mode to intensify basal insulin delivery to reach near-normal glycemia each morning. It adjusts basal insulin by increasing, decreasing, or suspending programmed delivery and administers correction boluses as needed to maintain glucose levels within the 112.5–160 mg/dl (6.2–8.9 mmol/l) range.
A registrational study was conducted on 168 patients with T1D aged 14 to 71, randomized to use either the Tandem T:slim X2 system with CIQ or a Sensor-Augmented Pump (SAP) for 6 months [13]. Compared to SAP-treated patients, CIQ users spent 2.6 more hours per day in the desired glycemic range (71% vs. 59% of the time), less time in hyperglycemia, and less time in hypoglycemia. These results were achieved without severe hypoglycemia or diabetic ketoacidosis episodes [13].
The most recent International Society for Pediatric and Adolescent Diabetes (ISPAD) Clinical Practice Consensus Guidelines state that “When making treatment recommendations providers should consider the perceived treatment burden and self-efficacy, level of social and family support, and presence of significant mental health issues” in youth with diabetes [14]. Therefore, psychological investigation is important because technology may increase the burden of the care, which affects QoL and psychosocial issues. Psychological issue investigation is mandatory in the treatment of diabetes to set realistic patient and caregiver expectations, to reach appropriate results, and to provide appropriate training [15].
Prompted by these statements, the objective of this article was to summarize current evidence on psychological outcomes and related safety issues of the Tandem t:slim X2 insulin pump with CIQ technology in children, adolescents, and young adults living with T1D.
Methods
This review used the PRISMA statement for systematic reviews. The literature search was launched on 15 April 2024 in PubMed and Embase. The keywords used were “Tandem T:slim,” “Tandem t:slim,” “Tandem Tslim,” “Tandem tslim,” “Tandem tslim,” “Tslim X2,” “tslim X2,” “Control IQ,” and “Advanced Hybrid Closed Loop.”
Non-English language papers were excluded. We included randomized trials, retrospective studies, observational studies, and case reports regarding children, adolescents, and non-pregnant young adults up to 25 years of age with T1D and treated with the Tandem t:slim X2 with CIQ activated. Reviews, commentaries, editorials, and guidelines were excluded. Only one letter was included because it reported the original data. The studies were considered irrespective of study setting (real-life condition, experimental setting, diabetes camps), duration of intervention, and baseline treatment. Table 1 displays the population, intervention, professions, outcomes, and health care system (PIPOH) summary of the study.
Data Extraction
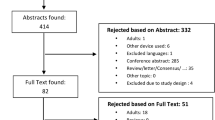
Two authors (CM and GMS) worked independently on the two online databases. The search retrieved 552 papers. They screened all records and excluded 132 duplicates. The remaining 420 records were screened by title and abstract, and 350 were excluded. Sixty-nine full texts of potentially eligible studies were retrieved for evaluation. Disagreements between authors were resolved by discussion and consensus, with the overview of the senior authors. At the end of the selection process, 22 manuscripts were selected for this review (Fig. 1). Eleven of 21 investigated psychological issues. Fourteen papers investigated safety issues.

PRISMA flowchart
This article is based on previously conducted studies and does not contain new studies with human participants or animals performed by any of the authors.
Outcomes
The main psychological outcomes were fear of hypoglycemia, QoL, sleep quality, safety during physical activity, and any person-related outcomes (PROs).
Information was extracted from each manuscript and summarized as (1) participants’ features (age, sex, diabetes duration, HbA1c before advanced hybrid closed loop-AHCL initiation); (2) inclusion and exclusion criteria in the case of clinical trials; (3) study design, outpatient setting, and follow-up duration; (4) psychological outcomes.
Diabetic ketoacidosis (DKA) and severe hypoglycemia (SH) were considered safety outcomes affecting psychological issues and thus evaluated.
Data Analysis
Data were extracted from the included papers and summarized using a narrative analysis. The results of each paper are displayed in Table 2. Data were synthesized thematically. Regarding data from cohorts with an age range different from our inclusion criteria, we evaluated only data about children, adolescents, and young adults < 25 years if available.
Results
Psychological and Sleep Quality Outcomes
Cobry et al. [16] compared health-related QoL and emotional distress between CIQ and SAP therapy in a 16-week + 12-week extension phase RCT involving 101 children (aged 6–13 years) and their caregivers. The study utilized the Problem Areas In Diabetes (PAID) scale, the Pediatric QoL (PedsQL) survey, and the Insulin Delivery Systems: Perceptions, Ideas, Reflections, and Expectations (INSPIRE) questionnaire. No statistically significant improvement was observed between groups for either parents or children.
However, Bisio et al. [17] documented a significant improvement in emotional distress and depressive symptoms for parents in a single-arm clinical trial after transitioning to CIQ therapy. The study involved the completion of the PAID scale and the Center for Epidemiologic Studies Depression Scale—Revised (CESDR) by parents and the PAID scale and the Children's Depression Inventory, second version, Self-Reported Short version (CDI-2:SR[S]) by children.
Similarly, Cobry et al. [18] reported an increase in parents PAID and PedsQL scores after switching from MDI or SAP to CIQ in a 6-month, single-arm, prospective observational study. However, there were no significant changes in scores for children and adolescents, except for an improvement in PedsQL scores for children aged 5–7 years (p = 0.042). There were no significant changes for either the parent or child INSPIRE surveys.
Zuijdwijk et al. [19] reported that only parents experienced an improved QoL after their children transitioned from Tandem t:slim X2 pump to CIQ technology. The WHO-5 Well-Being Index (p = 0.003) and INSPIRE questionnaire (p < 0.04) were used.
Improved QoL associated with CIQ technology was also reported in Hood et al. [20] 13-week RCT of CIQ vs SAP/MDI therapy. This study enrolled 102 young children (aged 2–6 yrs), data were collected based exclusively on the guardian’s perspective since this particular population relies primarily on a caregiver for diabetes management. The PedsQL survey and the Pediatric Inventory for Parents (PIP) questionnaire were used, and both showed improvement in child QoL and parenting stress (p = 0.02 and p = 0.05, respectively).
More recently, Marks et al. [21] investigated the PROs in a single-arm prospective pilot study on 13 insulin pump-naïve non-Hispanic Black youth (6–21 years old) with type 1 diabetes and HbA1c ≥ 10%. QoL significantly increased among parents and youth, and diabetes distress decreased in both groups. The improvements in blood glucose control parameters affected none of these outcomes.
Fear of hypoglycemia, a significant distress factor for patients and families, was addressed in various studies using the Hypoglycemia Fear Survey (HFS), with varying results. Ng et al. [22], Cobry et al. [18], and Zuijdwijk et al. [19] documented a substantial improvement in both patients and caregivers thanks to CIQ technology. Bisio et al. [17], on the other hand, found a significant improvement in parents alone; Hood et al. [20] documented an improvement in parents of very young children and Cobry et al. [16, 23] only in parents identified as “poor” sleepers and their children.
Different questionnaires were used to assess technology acceptance and treatment satisfaction across studies. Forlenza et al. [24] found that using the CIQ system was associated with reduced time spent thinking about diabetes and decreased burden in managing it. Renard et al. [25] noted a significant increase in Artificial Pancreas Acceptance Questionnaire scores (p = 0.036). In contrast, Diabetes Impact and Device Satisfaction (DIDS) questionnaire scores improved significantly for parents and children in a study by Zuijdwijk et al. [19].
In the prospective clinical study by Mingorance Delgado et al. [26], the same survey improved parents’ subjective feelings about diabetes control. Contrarily, Cobry et al. [18] experienced no significant changes in the parent and child Diabetes Technology Questionnaire scores after 6 months of CIQ usage, and Bisio et al. [17] reported no substantial differences in the benefits and burdens that parents experienced during the CIQ study phase.
Table 2 shows psychological outcomes in youth with T1D and their caregivers.
Sleep Quality Outcomes
Bisio et al. [17] conducted a single-arm clinical trial (4 weeks SAP + 4 weeks CIQ) using both questionnaires and an actigraphy watch to assess the sleep quality of parents and children. Parents reported a significant improvement in sleep quality and disturbances after switching to CIQ technology, as measured by the Pittsburgh Sleep Quality Index (PSQI). However, they did not observe a significant increase in their children's sleep quality and quantity, as measured by the Children's Sleep Habit Questionnaire-Abbreviated (CSHQ-A). Actigraphy data did not show any significant changes in sleep-related data for either parents or children, except for a decrease in parental awakenings lasting more than 5 min during the night (p = 0.036).
Cobry et al. [18], similarly, in their 6-month single-arm, prospective observational study, assessed sleep quality in children and adolescents and their parents. Participants' sleep was evaluated using questionnaires, wrist actigraphy, and sleep diaries. The Parent PSQI showed a significant improvement in subjective sleep quality after 3 months of AHCL use (p = 0.024), but this result was not confirmed at 6 months. The PROs Measurement Information System (PROMIS) scores showed significant improvements at 3 months only in the parent proxy for child sleep impairment subscale (p = 0.041); no improvement in PROMIS scores was seen at 6 months for either Child self-report (ages 8–17) or parent proxy for the child (children ages 5–17). Actigraphy watch measurements in children indicated no significant changes compared to baseline except for an increase in adolescents' sleep efficiency (ratio of the total sleep time and the time in bed) at 6 months (p = 0.03). Parents experienced a significant improvement in the total number of minutes awake after actigraphy sleep onset (WASO) at 3 (p = 0.004) and 6 months (p = 0.007).
Cobry et al. [16] also evaluated sleep quality in a RCT using the PSQI. Although there was no significant difference in PSQI scores between the two groups, parents in the CIQ group saw an improvement in sleep quality from “poor” (PSQI score > 5) to “adequate” over 16 weeks. A secondary analysis was conducted [23], focusing on parents identified as “poor” sleepers at baseline. At the end of the study, there was a significant improvement (p < 0.001) in PSQI scores, with 27 out of 49 poor sleepers becoming good sleepers. Hood et al. [20], in their RCT plus extension phase, reported improved PSQI scores in guardians of very young children on CIQ at 13 and 26 weeks compared to baseline.
Table 2 shows sleep quality outcomes in youth with T1D and their caregivers.
Safety: Diabetic Ketoacidosis and Severe Hypoglycemic Events
Data from different studies [22, 24, 25, 27,28,29,30,31,32,33,34,35,36,37] involving 1710 patients aged 0–18 were available regarding serious adverse events using the Tandem t:slim X2 insulin pump with CIQ technology. The follow-up duration varied considerably among the studies, ranging from 2 days to 12 months, with six studies lasting ≥ 6 months.
Messner et al. [27] conducted a prospective observational study in real-world conditions with 191 young people who began using the CIQ system for routine diabetes management. The follow-up period lasted for 6 months. At the 6-month mark, glycemic control improved compared to baseline. Additionally, two episodes of DKA were reported during the study period, one due to viral gastroenteritis and the other likely caused by an infusion set failure. There were no reports of severe hypoglycemic events in any of the participants.
Renard et al. [25] conducted a RCT with 122 free-living children with T1D aged between 6 and 12 years. The purpose of the study was to evaluate this system's safety over a 36-week period. During the initial phase of the study, which lasted 18 weeks, the authors compared the safety of using the CIQ technology only during the evening and night (E/N mode arm) when children were likely to be at home and under adult supervision with the safety of using it all day (24/7 arm). The study found that time in range (TIR) increased more in the 24/7 mode compared to the E/N mode (14.4% vs. 9.6%). Additionally, no severe adverse events such as SH or DKA were reported throughout the study when the CIQ software was activated. The authors concluded that this AHCL system is safe to use even when children are not under adult supervision, such as attending school, participating in physical activities, or eating without restrictions.
In a separate study conducted by Graham et al. [28], a single-arm, prospective, longitudinal study was carried out on individuals aged ≥ 6 years who started using the CIQ technology in a real-world setting. The trial enrolled 3157 participants with varying baseline HbA1c levels and previous therapy modalities. Participants were trained on the CIQ technology, and follow-up visits were conducted through their regular diabetes care provider without additional supervision. Data were collected over 12 months, and the rates of adverse events were compared to historical data from pediatrics [38]. It was found that the rates of SH and DKA were significantly lower in children compared to historical rates. The lower rates of adverse events were consistent regardless of baseline HbA1c levels, previous insulin delivery methods, or prior CGM experience.
Santova et al. [29] compared glycemic control and safety among Czech children with T1D using the 2022 annual report from the national pediatric diabetes registry, ČENDA. They collected data from all children < 19 years of age who had been using Medtronic MiniMed 780G (780G), Tandem t:slim X2 with CIQ, or do-it-yourself AndroidAPS (AAPS) HCL systems for > 12 months. The study included 512 patients, with 42.4% using 780G, 41.2% using CIQ, and 16.4% using AAPS. There were no statistically significant differences in the occurrence of DKA or SH events between the groups during the study period. In the CIQ group, DKA and SH events occurred at a rate of 2 per 100 patient-years.
All the other studies reported no serious adverse events [22, 24, 25, 30,31,32,33,34,35,36,37].
Exercise and Safety
The CIQ system has also been proven safe during intense exercise in youth. Mameli et al. [37] evaluated the safety and performance of CIQ technology during 2-h outdoor physical activity in 24 children and adolescents aged 9–18 years. All participants took part in both endurance activities (1000-m run and a jump circuit; 60 min duration) and power activities (80-m run and long jump; 60 min duration). Lunch and self-administration of an insulin bolus reduced by 50% compared to the usual calculated meal dose that occurred 90 min before starting exercise. The “Exercise activity” mode was set 90 min before starting physical activity and maintained until dinner time, while the “sleep mode” function was turned on at bedtime. No severe hypoglycemic episodes were recorded during physical activity or until 7 a.m.
Ekhlaspour et al. [31] and Schoelwer et al. [32] tested this AHCL system during winter ski camps. High altitude, low temperature, prolonged intense activity, increased carbohydrate intake, stress, and excitement could challenge glycemic control. The first study [31] included both adolescents (n = 24, aged 13–18 years) and children (n = 24, aged 6–12 years) who took part in a 48-h ski camp (~ 5 h skiing/day); the second study [32] only included adolescents (n = 18, aged 12–18 years), and the ski camp lasted 60 h. No serious adverse events were recorded in either of these studies.
Discussion
Different authors have evaluated the effectiveness of this AID system to assess its safety and effectiveness, metabolic outcomes, and psychological issues related to the Tandem t:slim X2 insulin pump with CIQ technology. This systematic review focuses on psychological issues to assess which outcomes are associated with its use.
Recent real-world data from the US report the effectiveness and safety of this AID system in children, adolescents, and young adults. In a cohort of 9010 CIQ users, TIR increased from 63.6% (IQR: 49.9–75.6%) to 73.6% (IQR: 64.4–81.8%), similar to MiniMed 780G™, 1 year after starting CIQ, with time < 70 mg/dl (3.0 mmol/l) consistently around 1% (IQR: 0.5–1.9%) [39]. Besides the evidence of improvement in metabolic outcomes, PROs are essential to evaluate satisfaction with the AID systems, and a relevant number of studies investigated these issues in both youth and their caregivers. Also, patients and their parents’ sleep quality and quantity are crucial because they impact physical and mental health.
Improvement in QoL has been inconstantly reported, as no changes in youth [16], no confirmed improvement for parents [18, 19], and large and significant improvement in historically minoritized youth and their parents [21] have been reported. Available data describe a considerable improvement in emotional distress and depressive symptoms in parents but not in children and adolescents [17, 18]. In contrast, a substantial improvement in fear of hypoglycemia has been widely reported both for patients and parents [17,18,19, 22]. One of the most critical concerns in diabetes treatment is the burden of blood glucose management, and treatment satisfaction and technology acceptance are essential aims for physicians. The papers investigating these issues and subjective feelings of diabetes control showed that Tandem t:slim X2 insulin pump with CIQ technology positively affects these outcomes [17,18,19, 24,25,26].
Despite the treatment satisfaction improvement and the positive effects on psychological issues, sleep quality is not significantly improved, at least in the short term [17], except for a not confirmed and mild positive effect on parents’ sleep quality, according to Cobry et al. [18]. However, this point could be biased by the shortness of the observation period, which includes the Tandem t:slim starts, when parents and individuals with T1D are not entirely confident about using the device. A more extended follow-up study could yield different results because of the different confidence levels with this device.
In this light, safety is paramount to engage parents and individuals with diabetes confidence. Several studies have investigated this point, and overall, serious adverse events in outpatient pediatric clinical trials using the CIQ system were very low. This could be attributed to the extra supervision provided to participants during the studies and the frequent visits to study centers, which may act as a barrier to enrollment and reduce diversity in the populations studied. However, real-world data also showed that the SH and DKA rates are meager and significantly lower than historic rates [38]. The data from the Czech pediatric diabetes registry clearly show that this system is safe, minimizing the occurrence of DKA and SH, and is as secure as the Medtronic MiniMed 780G and the do-it-yourself Android APS HCL systems. Also, data on safety and SH during exercise and sports show that this system is safe [31, 32, 37].
The first generation of the AID system, the MiniMed 670G, was effective in improving blood glucose control and safe for children and adolescents with T1D, increasing the time spent in the normoglycemic range while reducing the time spent in hypoglycemia and hyperglycemia. It does so without increasing the risk of severe hypoglycemic events and secondary DKA. Limited studies on psychological and sleep quality outcomes were available with conflicting results, without clarifying whether this first-generation device improved psychosocial outcomes [40]. However, this system had some burdens for the users,; thus, the drop-out rate was a concern. Prompted by this point, a second-generation AID system was launched for clinical use, further improving metabolic outcomes. In particular, the MiniMed 780G™ has been confirmed to be safe and effective in improving glucose control. It also addressed the burden of frequent user input and auto-exits, typical features of the MiniMed 670G. This AID enables the achievement of all recommended clinical targets for individuals with diabetes without excessive additional burden. Studies on psychological outcomes suggest that better metabolic control is strongly related to a reduced burden and improved psychosocial outcomes for people with diabetes and their caregivers [41].
This paper has some limitations. First, it is clear to the reader that papers are not homogeneous regarding age and methodology. Furthermore, there is a limited number of papers for each issue. We tried to present data in the best way for the purpose of clarity. Second, we cannot exclude that some papers could have been missed through our search strategy. We searched papers on two different available databases; the search was run by different authors, and we also checked any possible interesting paper in the reference list of each paper. We think that this bias has been reduced as much as possible.
Conclusion
This article systematically reviewed the literature on the safety and psychological outcomes of Tandem t:slim X2 insulin pump with CIQ. The system is safe and effective in improving the psychological outcomes of users and their parents. It significantly improved the PROs and treatment satisfaction but is less effective in improving sleep quality. Improvement in quality of life has been inconstantly reported. We are confident that this AID system is a significant technology in improving treatment for individuals with T1D. No RCTs are available to compare the effects of different second-generation AID systems.
Data Availability
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
Change history
14 August 2024
A Correction to this paper has been published: https://doi.org/10.1007/s13300-024-01636-0
References
Blackman SM, Raghinaru D, Adi S, et al. Insulin pump use in young children in the T1D Exchange clinic registry is associated with lower hemoglobin A1c levels than injection therapy. Pediatr Diabetes. 2014;15(8):564–72. https://doi.org/10.1111/pedi.12121.
DeSalvo DJ, Miller KM, Hermann JM, et al. Continuous glucose monitoring and glycemic control among youth with type 1 diabetes: International comparison from the T1D Exchange and DPV Initiative. Pediatr Diabetes. 2018;19(7):1271–5. https://doi.org/10.1111/pedi.12711.
Choudhary P, Ramasamy S, Green L, et al. Real-time continuous glucose monitoring significantly reduces severe hypoglycemia in hypoglycemia-unaware patients with type 1 diabetes. Diabetes Care. 2013;36(12):4160–2. https://doi.org/10.2337/dc13-0939.
Beato-Víbora P, Yeoh E, Rogers H, Hopkins D, Amiel SA, Choudhary P. Sustained benefit of continuous subcutaneous insulin infusion on glycaemic control and hypoglycaemia in adults with type 1 diabetes. Diabet Med. 2015;32(11):1453–9. https://doi.org/10.1111/dme.12869.
Heinemann L, Freckmann G, Ehrmann D, et al. Real-time continuous glucose monitoring in adults with type 1 diabetes and impaired hypoglycaemia awareness or severe hypoglycaemia treated with multiple daily insulin injections (HypoDE): a multicentre, randomised controlled trial. Lancet. 2018;391(10128):1367–77. https://doi.org/10.1016/S0140-6736(18)30297-6.
Pickup JC, Sutton AJ. Severe hypoglycaemia and glycaemic control in type 1 diabetes: meta-analysis of multiple daily insulin injections compared with continuous subcutaneous insulin infusion. Diabet Med. 2008;25(7):765–74. https://doi.org/10.1111/j.1464-5491.2008.02486.x.7.
Choudhary P, Campbell F, Joule N, Kar P, Diabetes UK. A type 1 diabetes technology pathway: consensus statement for the use of technology in Type 1 diabetes. Diabet Med. 2019;36(5):531–8. https://doi.org/10.1111/dme.13933.
Benioudakis E, Karlafti E, Kalaitzaki A, Kaiafa G, Savopoulos C, Didangelos T. Technological developments and quality of life in type 1 diabetes mellitus patients: a review of the modern insulin analogues, continuous glucose monitoring and insulin pump therapy. Curr Diabetes Rev. 2022;18(7): e031121197657. https://doi.org/10.2174/1573399818666211103163208.
Boughton CK, Hartnell S, Allen JM, Fuchs J, Hovorka R. Training and support for hybrid closed-loop therapy. J Diabetes Sci Technol. 2022;16(1):218–23. https://doi.org/10.1177/1932296820955168.
Leelarathna L, Choudhary P, Wilmot EG, et al. Hybrid closed-loop therapy: where are we in 2021? Diabetes Obes Metab. 2021;23(3):655–60. https://doi.org/10.1111/dom.14273.
Forlenza GP, Lal RA. Current status and emerging options for automated insulin delivery systems. Diabetes Technol Ther. 2022;24(5):362–71. https://doi.org/10.1089/dia.2021.0514.
Knoll C, Peacock S, Wäldchen M, et al. Real-world evidence on clinical outcomes of people with type 1 diabetes using open-source and commercial automated insulin dosing systems: a systematic review. Diabet Med. 2022;39(5): e14741. https://doi.org/10.1111/dme.14741.
Brown SA, Kovatchev BP, Raghinaru D, et al. Six-month randomized, multicenter trial of closed-loop control in type 1 diabetes. N Engl J Med. 2019;381(18):1707–17. https://doi.org/10.1056/NEJMoa1907863.
de Wit M, Gajewska KA, Goethals ER, et al. ISPAD clinical practice consensus guidelines 2022: psychological care of children, adolescents and young adults with diabetes. Pediatr Diabetes. 2022;23(8):1373–89. https://doi.org/10.1111/pedi.13428.
Sherr JL, Schoelwer M, Dos Santos TJ, et al. ISPAD clinical practice consensus guidelines 2022: diabetes technologies: insulin delivery. Pediatr Diabetes. 2022;23(8):1406–31. https://doi.org/10.1111/pedi.13421.
Cobry EC, Kanapka LG, Cengiz E, et al. Health-related quality of life and treatment satisfaction in parents and children with type 1 diabetes using closed-loop control. Diabetes Technol Ther. 2021;23(6):401–9. https://doi.org/10.1089/dia.2020.0532.
Bisio A, Brown SA, McFadden R, et al. Sleep and diabetes-specific psycho-behavioral outcomes of a new automated insulin delivery system in young children with type 1 diabetes and their parents. Pediatr Diabetes. 2021;22(3):495–502. https://doi.org/10.1111/pedi.13164.
Cobry EC, Pyle L, Karami AJ, et al. Impact of 6-months of an advanced hybrid closed-loop system on sleep and psychosocial outcomes in youth with type 1 diabetes and their parents. Diabetes Res Clin Pract. 2024;207: 111087. https://doi.org/10.1016/j.diabres.2023.111087.
Zuijdwijk C, Courtney J, Mitsakakis N, et al. Control-IQ technology positively impacts patient reported outcome measures and glycemic control in youth with type 1 diabetes in a real-world setting. Pediatr Diabetes. 2023. https://doi.org/10.1155/2023/5106107.
Hood KK, Schneider-Utaka AK, Reed ZW, et al. Patient reported outcomes (PROs) and user experiences of young children with type 1 diabetes using t:slim X2 insulin pump with control-IQ technology. Diabetes Res Clin Pract. 2024;208: 111114. https://doi.org/10.1016/j.diabres.2024.111114.
Marks BE, Grundman JB, Meighan S, Monaghan M, Streisand R, Perkins A. Hybrid closed loop systems improve glycemic control and quality of life in historically minoritized youth with diabetes. Diabetes Technol Ther. 2024;26(3):167–75. https://doi.org/10.1089/dia.2023.0450.
Ng SM, Katkat N, Day H, Hubbard R, Quinn M, Finnigan L. Real-world prospective observational single-centre study: hybrid closed loop improves HbA1c, time-in-range and quality of life for children, young people and their carers. Diabet Med. 2022;39(7): e14863. https://doi.org/10.1111/dme.14863.
Cobry EC, Bisio A, Wadwa RP, Breton MD. Improvements in parental sleep, fear of hypoglycemia, and diabetes distress with use of an advanced hybrid closed-loop system. Diabetes Care. 2022;45(5):1292–5. https://doi.org/10.2337/dc21-1778.
Forlenza GP, Ekhlaspour L, Breton M, et al. Successful at-home use of the tandem control-iq artificial pancreas system in young children during a randomized controlled trial. Diabetes Technol Ther. 2019;21(4):159–69. https://doi.org/10.1089/dia.2019.0011.
Renard E, Tubiana-Rufi N, Bonnemaison E, et al. outcomes of hybrid closed-loop insulin delivery activated 24/7 versus evening and night in free-living prepubertal children with type 1 diabetes: a multicentre, randomized clinical trial. Diabetes Obes Metab. 2022;24(3):511–21. https://doi.org/10.1111/dom.14605.
Mingorance Delgado A, Lucas F. The tandem control-iq advanced hybrid system improves glycemic control in children under 18 years of age with type 1 diabetes and night rest in caregivers. Endocrinol Diabetes Nutr (Engl Ed). 2023;70(Suppl 3):27–35. https://doi.org/10.1016/j.endien.2023.08.005.
Messer LH, Berget C, Pyle L, et al. Real-world use of a new hybrid closed loop improves glycemic control in youth with type 1 diabetes. Diabetes Technol Ther. 2021;23(12):837–43. https://doi.org/10.1089/dia.2021.0165.
Graham R, Mueller L, Manning M, et al. Real-world use of control-iq technology is associated with a lower rate of severe hypoglycemia and diabetic ketoacidosis than historical data: results of the control-IQ observational (CLIO) prospective study. Diabetes Technol Ther. 2024;26(1):24–32. https://doi.org/10.1089/dia.2023.0341.
Santova A, Plachy L, Neuman V, et al. Are all HCL systems the same? Long term outcomes of three HCL systems in children with type 1 diabetes: real-life registry-based study. Front Endocrinol (Lausanne). 2023;16(14):1283181. https://doi.org/10.3389/fendo.2023.1283181.
Kanapka LG, Wadwa RP, Breton MD, et al. Extended use of the control-iq closed-loop control system in children with type 1 diabetes. Diabetes Care. 2021;44(2):473–8. https://doi.org/10.2337/dc20-1729.
Ekhlaspour L, Forlenza GP, Chernavvsky D, et al. Closed loop control in adolescents and children during winter sports: use of the tandem control-IQ AP system. Pediatr Diabetes. 2019;20(6):759–68. https://doi.org/10.1111/pedi.12867.
Schoelwer MJ, Robic JL, Gautier T, et al. Safety and efficacy of initializing the control-iq artificial pancreas system based on total daily insulin in adolescents with type 1 diabetes. Diabetes Technol Ther. 2020;22(8):594–601. https://doi.org/10.1089/dia.2019.0471.
Cherubini V, Rabbone I, Berioli MG, et al. Effectiveness of a closed-loop control system and a virtual educational camp for children and adolescents with type 1 diabetes: a prospective, multicentre, real-life study. Diabetes Obes Metab. 2021;23(11):2484–91. https://doi.org/10.1111/dom.14491.
Scaramuzza AE, Bonfanti R, Cherubini V, Marigliano M, Schiaffini R, Toni S, Rabbone I, vEC Study Group. Comment on real-world use of a new hybrid closed loop improves glycemic control in youth with type 1 diabetes by Messer et al. Diabetes Technol Ther. 2022;24(6):455–7. https://doi.org/10.1089/dia.2022.0133.
Scaramuzza AE, Marigliano M, Bonfanti R, et al. Implementing control-IQ technology after a virtual educational camp in children and adolescents with type 1 diabetes: does time in range plateau over 1 year? Diabetes Obes Metab. 2024;26(2):763–6. https://doi.org/10.1111/dom.15343.
Rabbone I, Savastio S, Pigniatiello C, et al. Significant and persistent improvements in time in range and positive emotions in children and adolescents with type 1 diabetes using a closed-loop control system after attending a virtual educational camp. Acta Diabetol. 2022;59(6):837–42. https://doi.org/10.1007/s00592-022-01878-z.
Mameli C, Rigamonti A, Felappi B, et al. Performance of tandem control iq during outdoor physical activity in children and adolescents with type 1 diabetes. Diabetes Technol Ther. 2024;26(2):112–8. https://doi.org/10.1089/dia.2023.0324.
Foster NC, Beck RW, Miller KM, et al. State of type 1 diabetes management and outcomes from the T1D exchange in 2016–2018. Diabetes Technol Ther. 2019;21(2):66–72. https://doi.org/10.1089/dia.2018.0384.
Breton MD, Kovatchev BP. One year real-world use of the control-IQ advanced hybrid closed-loop technology. Diabetes Technol Ther. 2021;23(9):601–8. https://doi.org/10.1089/dia.2021.0097.
Mameli C, Smylie GM, Galati A, et al. Safety, metabolic and psychological outcomes of Medtronic MiniMed 670G in children, adolescents and young adults: a systematic review. Eur J Pediatr. 2023;182(5):1949–63. https://doi.org/10.1007/s00431-023-04833-4.
Passanisi S, Lombardo F, Mameli C, et al. Safety, metabolic and psychological outcomes of medtronic MiniMed 780G™ in children, adolescents and young adults: a systematic review. Diabetes Ther. 2024;15(2):343–65. https://doi.org/10.1007/s13300-023-01501-6.
Funding
No funding or sponsorship was received for the publication of this article.
Author information
Authors and Affiliations
Contributions
Chiara Mameli, Giulia Marie Smylie, Marco Marigliano, Luca Zagaroli, Valentina Mancioppi, Claudio Mafferis, Vincenzo Salpietro, Gianvincenzo Zuccotti, and Maurizio Delvecchio contributed to the study conception and design. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of Interest
Chiara Mameli, Giulia Marie Smylie, Marco Marigliano, Luca Zagaroli, Valentina Mancioppi, Claudio Mafferis, Vincenzo Salpietro, and Gianvincenzo Zuccotti do not declare any competing interests. Maurizio Delvecchio is an Editorial Board member of Diabetes Therapy and was not involved in the selection of peer reviewers for the manuscript nor any of the subsequent editorial decisions.
Ethical Approval
This article is based on previously conducted studies and does not contain new studies with human participants or animals performed by any of the authors.
Additional information
The original version was revised due to correction in second author name.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Mameli, C., Smylie, G.M., Marigliano, M. et al. Safety and Psychological Outcomes of Tandem t:Slim X2 Insulin Pump with Control-IQ Technology in Children, Adolescents, and Young Adults with Type 1 Diabetes: A Systematic Review. Diabetes Ther 15, 2133–2149 (2024). https://doi.org/10.1007/s13300-024-01618-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13300-024-01618-2