
Abstract
Introduction
Lipoedema is a chronic disorder in which excessive fat distribution occurs predominantly from the waist down, resulting in a disproportion between the lower extremities and upper torso. Lipoedema is often not recognized, while patients experience pain and easy bruising. As a long-term condition, lipoedema has a massive effect on patients’ lives and mental health. The aim of this study is to explore patient characteristics, quality of life, physical complaints and comorbidities in patients with lipoedema.
Methods
A survey was conducted by email amongst lipoedema patients, consisting of informed consent and multiple questionnaires. The questionnaires included general patient characteristics, physical complaints, comorbidities, RAND-36 and EQ-5D-3L. Participants who responded to a message on the Dutch Lipoedema Association website were recruited.
Results
All lipoedema patients experience physical complaints, with pain (88.3 %) and easy bruising (85.9 %) as primary complaints. The diagnosis was mostly made by a dermatologist after visiting a mean of 2.8 doctors. Furthermore, mean time from onset until diagnosis was 18 years. Quality of life (59.3) was significantly lower than the Dutch female average (74.9; p < 0.001). Additionally, patients with comorbidities had significant lower quality of life (RAND 54.7, p < 0.001).
Conclusions
Lipoedema patients often have severe complaints and experience lower quality of life regarding physical, emotional and social functioning. Additionally, comorbidities have a large impact on quality of life.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Lipoedema is an adipose tissue disorder that was first described more than 75 years ago by Allen and Hines [1]. To date, there is little scientific evidence available on lipoedema. To gain better understanding of this frequently neglected and misdiagnosed disorder, it is particular important to collect further epidemiological, clinical and therapeutic evidence [2]. The goal of this study is to characterize lipoedema from the patient perspective.
The onset of lipoedema is usually at or soon after puberty up to the third decade of life [3, 4], with some cases reporting late onset after pregnancy or even menopause [4]. Although lipoedema is not currently recognized as a hereditary disease, the familial nature of the condition suggests that lipoedema can demonstrate heritability. Positive family history varies between 15 and 64 %, with no specific genes disclosed that explain inheritance [1, 4,5,6]. Clinical features such as easy bruising and pain upon pressure have been reported in 82 and 71 %, respectively [4]. Other complaints are a sensation of heaviness or discomfort in the legs that is worsened with pressure and mild pitting oedema [5]. Additionally, knee pain was described in 55 % of cases. Although knee pain can be found in “simple” obesity, it appears to be a phenotypic feature of lipoedema, even in patients with normal body mass index (BMI) [4].
Lipoedema has a massive effect on patients’ lives, and approximately 85 % say lipoedema affects their mental health and ability to cope with life [7]. In addition, altered body shape leads to low self-esteem, and many have lack of confidence, depression, self-harm thoughts and suicidal thoughts [8]. Furthermore, lipoedema restricts social life and relationships, including sexual activities [8]. Quality of life may be affected by decreased physical functioning and associated comorbid conditions such as obesity, venous varicosis and secondary lymphoedema [9].
Specific diagnostic tests for lipoedema are not available. Thus, diagnosis is based on examination and history, making it important for clinicians to understand the morphology of lipoedema and its unique features [3]. Characteristics are bilateral symmetrical fat deposition confined to the legs, thighs and buttocks, with sparing of the feet, which results in a “reverse shouldering” effect, also known as the “cuff sign” [3, 4, 10]. Due to this local fat deposition, a disproportionate ratio arises between the trunk and lower extremities [10]. The first manifestation of lipoedema may be filling of the retro-malleolar sulcus on both lower extremities [10].
The exact aetiology of lipoedema is still unclear, but multiple hypotheses have been proposed. Lipoedema is suspected to have a polygenetic susceptibility, which is affected by feminine hormonal changes [11]. These genes, coding for vasculo- or lymphangiogenesis under the influence of oestrogen, are suspected to cause the primary endothelial barrier dysfunction and lymphangiopathy [11]. Furthermore, oestrogen plays an important role in region-specific sympathetic innervation of subcutaneous adipose tissue. This might cover innervation abnormalities and concomitant inflammation of sensory nerves [11].
During the last decade, more evidence about surgical interventions has become available, while conservative treatment remains uncharted. Manual lymphatic drainage (MLD), intermittent pneumatic compression therapy, kinesio taping and multilayer bandaging are examples of conservative treatments [7]. Although there is a lack of clinical evidence, compression is perceived to reduce lipoedema symptoms and prevent progression of its lymphatic component, while enhancing mobility and function [7, 10]. Liposuction with tumescent local anaesthesia as surgical intervention demonstrated lower sensitivity to pressure, less bruising, less oedema, fewer restrictions of movement and less cosmetic impairment [6, 12]. Despite the fact that more data are available about surgical therapy, the clinical and epidemiological side remain unexposed.
The goal of this article is to evaluate patient characteristics, quality of life, physical complaints and comorbidities in patients with lipoedema. We report findings using surveys that provide lipoedema characteristics from the patient perspective.
Methods
A survey was carried out by email, consisting of informed consent, demographic details and multiple questionnaires. In 2011, the Department of Dermatology of Maastricht University Medical Centre posted a call on the Dutch Lipoedema Association website. Participants who responded received an email with the questionnaires. All patients aged 18 years and older, regardless of BMI and disease stage, were included. Participation in this study was voluntarily, and no incentives were offered. This study was approved by the Medical Ethics Committee of Maastricht University Medical Centre.
Patient Characteristics
The questionnaire started with general questions about patient characteristics based on clinical experience and literature and included the following: age, height, weight, comorbidities, medication, oral anti-conception usage, number of pregnancies and children, age at onset, age at diagnosis, how many doctors seen, who made the diagnosis and family members with lipoedema.
Physical Complaints
Because there are no validated questionnaires for assessment of lipoedema-related complaints, we made a new questionnaire based on available literature and clinical experience including: pain upon pressure, easy bruising, pain in the legs, cold legs, burning sensation of the skin, numbness and other complaints. Pain was evaluated using a numerical rating scale (NRS) ranging from 0 to 10 for minimum, maximum and current pain. In addition, patients were asked if the appearance of their lipoedema was less, equally, or more important than their physical complaints.
RAND-36
The RAND-36 is a questionnaire which determines health-related quality of life. It provides insight into how health impacts an individual’s ability to function and this person’s perceived well-being [13]. RAND-36 consists of 36 items that assess nine health dimensions: general health perceptions, physical functioning, mental health, pain, role limitations caused by physical health problems, role limitations caused by emotional problems, vitality, health change and social functioning. For each dimension, a sub-score is calculated, together forming a total score [14].
EQ-5D-3L
Quality of life was measured using the EuroQol-5D-3L, a standardized instrument used as a measure of health-related quality of life [15, 16]. It consists of five dimensions (mobility, self-care, usual activities, pain/discomfort, anxiety/depression). These dimensions were measured on a three-point scale: 0, no problems; 1, some or moderate problems; 2, extreme problems. We used the Dutch version and the matching value set to gain a more accurate outcome, taking the general population’s preferences into account [17].
Data Collection and Analysis
All questionnaires were manually added to a database. This database was then analysed by the first author. The independent T test was used to determine the effect of comorbidities on quality of life. Spearman correlation was used to assess correlation between different treatments and their effect on the shape of the legs. The significance level considered for all statistical tests was 0.05. Statistics were performed using SPSS 22.0 for Windows.
Results
In total, 414 patients responded to the message and received an email. A total of 163 questionnaires were returned. Almost all questionnaires were complete and filled out correctly. Frequency distributions corresponding to socio-demographic variables and clinical characteristics are presented in Table 1.
General Data
All questions regarding patient characteristics and physical complaints are available in Appendix 1. The mean age of patients was 44 years (21–76 years); the mean weight was 94.4 kg (57–160 kg); and the mean BMI was 33.2 kg/m2 (19.2–54.4 kg/m2). Oral anti-conception was used by 95.7 % of patients with mean duration of 13.3 years (0.5–48 years). One hundred thirteen women had been pregnant, with all of them having children while 15 (13.3 %) had one or two miscarriages. The diagnosis of lipoedema was made by a dermatologist (61.3 %), surgeon (6.1 %), general practitioner (3.7 %), physiotherapist (3.1 %), skin therapist (2.5 %), a combination of the foregoing options (11.70 %), or other professionals (11.7 %). The diagnosis was made after visiting a mean of 2.8 doctors, ranging from 1 to 20. Additionally, 11 patients filled in “many” instead of a number; these were not taken into account. Mean age at onset was 20.0 years, with mean age of 38.3 years at diagnosis. Familial involvement was reported in 57 cases (35 %), while 40 had no involvement (24.5 %) and 66 (40.5 %) did not know whether family members had lipoedema. Table 1 presents an extensive overview of the general data.
Physical Complaints
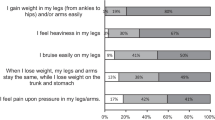
The following physical complaints were reported: pain upon pressure (143; 87.7 %), easy bruising (140; 85.9 %), pain (144; 88.3 %), cold (117; 71.8 %), burning sensation (58; 35.6 %), numbness (61; 37.4 %). Zero patients experienced no complaints. Additionally, 86 (52.8 %) patients reported other complaints. Examples of other complaints are: restless legs (16), heaviness in the legs (13), fatigue (12), cramps (7) and muscle weakness (7). The mean onset of complaints was 27 years. Five patients reported “always” and three “after pregnancy”; these were not taken into account. Pain was measured on a 10-point NRS, revealing mean current pain of 4.2, mean minimum pain of 3.1 and mean maximum pain of 6.1. Comparing complaints with appearance, 84 (51.5 %) patients reported complaints to be more important than appearance, 59 (36.2 %) weighted complaints equally important to appearance and 20 (12.3 %) considered appearance to be worse.
Quality of Life
The mean EQ-5D-3L score was 66.1 (N = 162; −20.4 to 100) in lipoedema patients, while the general Dutch population reports a mean EQ-5D-3L score of 85 [18]. Subdividing into different dimensions revealed that 63.0 % has some problems with mobility, although none reported being confined to bed. Only 9.9 % reported some problems with washing or dressing, and 1.2 % were unable to wash or dress themselves. Usual activities (e.g. work, study, housework, family or leisure activities) gave some problems in 64.8 %, and 3.1 % were unable to perform them. Pain or discomfort was reported in 74.1 % of cases, with 16.7% having extreme pain or discomfort. Lastly, anxiety or depression was mentioned in 42.0 %, with 1.2 % reporting to be extremely anxious or depressed. The mean RAND-36 score was 59.3 (N = 154; 0–100). Exploring the different dimensions, the results were as follows: physical functioning 63.5, social functioning 67.3, emotional limitations 71.6, mental health 69.9, vitality 49.1, pain 57.2, general health 51.6 and health change 51.4. Except for the ‘health change’ dimension, the scores for the study population are lower than the mean Dutch female population (Table 2) [10].
Comorbidities
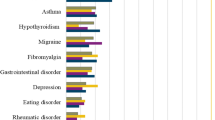
Comorbidities were reported in 92 cases (56.4 %), with a mean age of 46.8 years. Most common were cardiac disease (N = 35), thyroid disease (N = 19), fibromyalgia (N = 14), diabetes mellitus (N = 9), bowel disease (N = 8), asthma (N = 8) and lymphoedema (N = 5). Patients with comorbidities had significantly lower quality of life (RAND 54.7, p < 0.001; EQ-5D 60.5, p = 0.001) compared with those with no comorbidities (RAND 73.2; EQ-5D 65.0).
Discussion
In this study, we investigated disease characteristics and quality of life in patients with lipoedema using questionnaires. Our goal was to assess general health, frequent complaints and quality of life to gain better understanding of the lipoedema population. Furthermore, the relation between comorbidities and the effect on QOL was assessed. To our knowledge, this is the first article to put these items in order. Below we discuss our findings in the light of existing literature.
The age at diagnosis (38.3 years) is relatively high compared with the onset of complaints (20.0 years). With complaints starting at puberty, many women are not aware that they have developed lipoedema. Furthermore, lipoedema is not known or recognized by all clinicians, causing patients to visit multiple professionals. A previous study showed that lipoedema was only seen and recognized by 46.2 % of 251 consultants who were part of the Vascular Society of Great Britain and Ireland [19]. Moreover, lipoedema is frequently misdiagnosed as lymphoedema, chronic venous insufficiency or obesity [10, 20]. Literature showed that onset during puberty occurred in 55–78 % of cases [4, 8]. In agreement with this, our study showed 64.2 % of onset in the 10–19 years group. Child et al. showed that 27 out of 38 patients (71 %) experienced swollen legs which were painful upon pressure, quite a bit lower compared with the 87.7 % we found [4]. The relatively small sample size they used may, at least partly, account for this difference. However, there was only a small difference in easy bruising, which was 85.9 % in our study compared with 82 % in theirs [4].
To prevent disease progression in children of lipoedema patients, it is important to discuss inheritance. Familial involvement was reported in 35 %. Positive family history in other studies varied between 15 and 64 %, with no specific genes disclosed that explain inheritance [4, 20,21,22]. This outcome may be even higher, because 40.5 % did not know whether family members had lipoedema. It is not verified whether the diagnosis was accurate, since it is only based on questionnaires. On the other hand, the “unknown” option makes the outcome of familial involvement more reliable.
The overall RAND-36 score in this study (59.3) is considerably lower than the mean Dutch female RAND-36 score (74.9) [14]. Every subdomain except for health change was significantly lower in lipoedema patients, with physical parameters showing the greatest differences. An explanation might be that increased leg size causes mechanical hindrance and restricts mobility, resulting in physical limitations and reduced vitality [10]. Also, complaints such as pain, burning sensation and pain upon pressure have a negative effect on quality of life [10]. Ineffective treatments, stigmatization, contradictory advice and uncontrollable changes in body appearance can lead to learned helplessness, self-stigmatization, feelings of shame and guilt, and body dissatisfaction [3, 4, 23, 24]. Previous mentioned factors can influence emotional and social functioning. The quality of life of lipoedema patients, measured by the EQ-5D questionnaire, was also lower than the general Dutch female population (66.1 and 85, respectively) [18]. In particular, pain or discomfort was reported frequently. Some pain or discomfort was reported by 74.1 % of lipoedema patients compared with 31.1 % of the Dutch female population. Extreme pain or discomfort was reported in 16.7 and 2.1 %, respectively [25].
Cardiac and thyroid disease were reported frequently compared with a healthy population. Prevalence of hypothyroidism among Dutch females lies at around 25 per 1000 [26]. Although hypothyroidism (11.7 %) and hypertension (18.4 %) are more prevalent in our study group, both are associated with obesity [27, 28]. Patients with comorbidities reported lower QOL, which varies directly with the severity of obesity among individuals, with the most obese individuals reporting the poorest QOL [29]. The comorbidity group had BMI of 36.6 compared with 29.7 kg/m2 in patients without comorbidities, which might explain the difference in QOL.
Limitations
The response rate to our questionnaire was rather low (39 %). When questionnaires are used in scientific research, the response rate generally varies between 50 and 60 %, but there is a considerable grey area [30]. We believe that lipoedema patients often have little motivation, which in combination with the length of the questionnaires they received resulted in the lower response rate of 39 %.
As participation in this study was solely based on a reaction to our message, it is possible that patients with more complaints responded more often, creating a selection bias. However, this is inevitable with voluntary participation. Since, the Dutch Lipoedema Association has members throughout the country, we believe that our study population is geographically a representative selection of lipoedema patients in The Netherlands.
An advantage of the questionnaires is the possibility to use an index value, which makes it suitable for quantifying health outcomes [18]. The EQ-5D is very brief compared with other instruments. Although this instrument lacks detail, it has been proven to accurately describe the health status of the general population [25]. Also, it was specifically designed to complement other quality of life measures, such as the RAND-36 [31]. Two possible disadvantages are that the instrument contains no items that cover cognitive abilities and it is less sensitive at the milder end of the health distribution [32, 33]. The latter may cause patients to indicate problems faster. The RAND-36 has clear advantages over other instruments, as it covers all areas of health and is not targeted at specific diseases [14]. Furthermore, it is easily applicable but relatively long, consuming a lot of time to fill out the form [14, 34]. Nevertheless, almost all questionnaires were filled out completely.
Conclusions
This research provides information about complaints, quality of life and comorbidities in lipoedema patients. Patients experience significantly lower quality of life regarding physical, emotional and social functioning compared with the general Dutch female population. Physical complaints such as pain upon pressure, easy bruising and pain are very common, and comorbidities, such as cardiac and thyroid disease, are frequently seen. We recommend evaluating comorbidities and optimizing their therapy, as they have a large impact on QOL. Inheritance should be discussed to prevent disease progression after puberty. This study provides general information that can help identify the diagnosis by increasing awareness and knowledge. Further research should focus on how to optimize treatment for lipoedema patients, including special attention to patient quality of life.
References
Allen EV, Hines EA. Lipedema of the legs: a syndrome characterized by fat legs and orthostatic edema. Proc Staff Meet Mayo Clin. 1940;15:184–7.
Szolnoky G, Kemény L. Lipoedema: from clinical presentation to therapy. Further aspects. Br J Dermatol. 2010;162(4):889.
Fife CE, Maus EA, Carter MJ. Lipedema: a frequently misdiagnosed and misunderstood fatty deposition syndrome. Adv Skin Wound Care. 2010;23:81–92.
Child AH, Gordon KD, Sharpe P, et al. Lipedema: an inherited condition. Am J Med Genet A. 2010;152A:970–6.
Okhovat JP, Alavi A. Lipedema: a review of the literature. Int J Low Extrem Wounds. 2015;14(3):262–7.
Schmeller W, Hueppe M, Meier-Vollrath I. Tumescent liposuction in lipoedema yields good long-term results. Br J Dermatol. 2012;166:161–8.
Fetzer A. Specialist approaches to managing lipoedema. Chronic Oedema. 2016;21(Suppl 4):S30–5.
Fetzer A, Fetzer S. Early lipoedema diagnosis and the RCGP e-learning course. Br J Community Nurs. 2015;20(4 Suppl):S22–8.
Dudek JE, Białaszek W, Ostaszewski P. Quality of life in women with lipoedema: a contextual behavioral approach. Qual Life Res. 2016;25(2):401–8.
Langendoen SI, Habbema L, Nijsten TEC, Neumann HAM. Lipoedema: from clinical presentation to therapy. A review of the literature. Br J Dermatol. 2009;161(5):980–6.
Szél E, Kemény L, Groma G, et al. Pathophysiological dilemmas of lipedema. Med Hypotheses. 2014;83(5):599–606.
Baumgartner A, Hueppe M, Schmeller W. Long-term benefit of liposuction in patients with lipoedema: a follow-up study after an average of 4 and 8 years. Br J Dermatol. 2016;174(5):1061–7.
Hays RD, Morales LS. The RAND-36 measure of health-related quality of life. Ann Med. 2001;33(5):350–7.
van der Zee KL, Sanderman R. Het meten van de algemene gezondheidstoestand met de RAND-36. Een handleiding. 2nd ed. Groningen: Noordelijk Centrum voor Gezondheidsvraagstukken; 2012.
The EuroQol Group. EuroQol-a new facility for the measurement of health-related quality of life. Health Policy. 1990;16(3):199–208.
Brooks R. EuroQol: the current state of play. Health Policy. 1996;37(1):53–72.
Lamers LM, McDonnell J, Stalmeier PF, Krabbe PF, Busschbach JJ. The Dutch tariff: results and arguments for an effective design for national EQ-5D valuation studies. Health Econ. 2006;15(10):1121–32.
Hoeymans N, van Lindert H, Westert GP. The health status of the Dutch population as assessed by the EQ-6D. Qual Life Res. 2005;14:655–63.
Tiwari A, Myint F, Hamilton G. Management of lower limb lymphoedema in the United Kingdom. Eur J Vasc Endovasc Surg. 2006;31:311–5.
Rudkin GH, Miller TA. Lipedema: a clinical entity distinct from lymphedema. Plast Reconstr Surg. 1994;94:841–9.
Wold LE, Hines EA Jr, Allen EV. Lipedema of the legs: a syndrome characterized by fat legs and edema. Ann Intern Med. 1951;34:1243–50.
Harwood CA, Bull RH, Evans J, Mortimer PS. Lymphatic and venous function in lipoedema. Br J Dermatol. 1996;134:1–6.
Herbst KL. Rare adipose disorders (RADs) masquerading as obesity. Acta Pharmacol Sin. 2012;33(2):155–72.
Seo CA. You mean it’s not my fault: learning about lipedema, a fat disorder. Narrat Inq Bioeth. 2014;4(2):E6–9.
Szende A, Williams A. Measuring self-reported population health: an international perspective based on EQ-5D. 2004. The EuroQol Group’s International Task Force on Self-Reported Health.
Donker GA. Continue Morbiditeits Registratie Peilstations Nederland 2012. Utrecht: NIVEL; 2012.
Nyrnes A, Jorde R, Sundfjord J. Serum TSH is positively associated with BMI. Int J Obes (Lond). 2006;30:100–5.
Re RN. Obesity-related hypertension. Ochsner J. 2009;9(3):133–6.
Kolotkin RL, Meter K, Williams GR. Quality of life and obesity. The International Association for the Study of Obesity. Obes Rev. 2001;2:219–29.
Yammarino FJ, Skinner SJ, Childers TL. Understanding mail survey response behavior: a meta-analysis. Public Opin Q. 1991;55:613–39.
Elliott R, Payne K. Essentials of economic evaluation in healthcare. London: Pharmaceutical Press; 2005.
Macran S, Weatherly H, Kind P. Measuring population health: a comparison of three generic health status measures. Med Care. 2003;41:218–31.
Insinga RP, Fryback DG. Understanding differences between self-ratings and population ratings for health in the EuroQol. Qual Life Res. 2003;12:611–9.
Essink-Bot ML, Rutten-van Mölken MPMH. Het meten van de gezondheidstoestand: inventarisatie van meetinstrumenten voor medical technology assessment. Rotterdam: Instituut voor Maatschappelijke Gezondheidszorg/Instituut voor Medische Technology Assessment, Erasmus Universiteit Rotterdam/Rijksuniversiteit Limburg; 1991.
Acknowledgements
We would like to thank the participants of the study.
Funding
No funding or sponsorship was received for this study or publication of this article. The article processing charges were funded by the authors.
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Disclosures
J. R. M. Romeijn, M. J. M. de Rooij, L. Janssen and H. Martens have nothing to disclose.
Compliance with Ethics Guidelines
This study was approved by the local medical ethics committee of the Maastricht University Medical Centre, at Maastricht in The Netherlands. Written patient consent was obtained.
Data Availability
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Open Access
This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
Author information
Authors and Affiliations
Corresponding author
Additional information
Enhanced digital features
To view enhanced digital features for this article go to https://doi.org/10.6084/m9.figshare.6182141.
Electronic Supplementary Material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0), which permits use, duplication, adaptation, distribution, and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Romeijn, J.R.M., de Rooij, M.J.M., Janssen, L. et al. Exploration of Patient Characteristics and Quality of Life in Patients with Lipoedema Using a Survey. Dermatol Ther (Heidelb) 8, 303–311 (2018). https://doi.org/10.1007/s13555-018-0241-6
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13555-018-0241-6